
Abstract
Context:
Patellofemoral pain syndrome (PFPS) is a common orthopaedic condition for which operative and nonoperative treatments have been used. Therapeutic modalities have been recommended for the treatment of patients with PFPS—including cold, ultrasound, phonophoresis, iontophoresis, neuromuscular electrical stimulation, electrical stimulation for pain control, electromyographic biofeedback, and laser.
Objective:
To determine the effectiveness of therapeutic modalities for the treatment of patients with PFPS.
Data Sources:
In May and August 2010, Medline was searched using the following databases: PubMed, CINAHL, Web of Science Citation Index, Science Direct, ProQuest Nursing & Allied Health, and Your Journals@OVID.
Study Selection:
Selected studies were randomized controlled trials that used a therapeutic modality to treat patients with PFPS. The review included articles with all outcome measures relevant for the PFPS patient: knee extension and flexion strength (isokinetic and isometric), patellofemoral pain assessment during activities of daily life, functional tests (eg, squats), Kujala patellofemoral score, and electromyographic recording from knee flexors and extensors and quadriceps femoris cross-sectional areas.
Data Extraction:
Authors conducted independent quality appraisals of studies using the PEDro Scale and a system designed for analysis of studies on interventions for patellofemoral pain.
Results:
Twelve studies met criteria: 1 on the effects of cold and ultrasound together, ice alone, iontophoresis, and phonophoresis; 3, neuromuscular electrical stimulation; 4, electromyographic biofeedback; 3, electrical stimulation for control of pain; and 1, laser.
Discussion:
Most studies were of low to moderate quality. Some reported that therapeutic modalities, when combined with other treatments, may be of some benefit for pain management or other symptoms. There was no consistent evidence of any beneficial effect when a therapeutic modality was used alone. Studies did not consistently provide added benefit to conventional physical therapy in the treatment of PFPS.
Conclusions:
None of the therapeutic modalities reviewed has sound scientific justification for the treatment of PFPS when used alone.
Patellofemoral pain syndrome (PFPS) is one of the most common orthopaedic conditions in adolescents and young adults. 26 It is the most common overuse injury in adolescent girls. 26 It affects approximately 26% of young athletes 14 and 7% of young active adults.14,29 PFPS is so common in runners and other endurance athletes that it is often referred to as runner’s knee. 15 PFPS is generally characterized by diffuse anterior knee pain, aggravated with specific activities that heighten the compressive loading forces across the patellofemoral joint,6,9,24,28 including ascending and descending stairs, squatting, and prolonged sitting.6,24,28 Altered lower extremity kinematics 28 and knee and hip muscle weakness 29 contribute to the pain and dysfunction associated with PFPS.
Both operative and nonoperative approaches are used in the treatment of PFPS, and many patients improve with nonoperative rehabilitation care.17,26 The principal goals of a rehabilitation program for PFPS are to decrease pain and edema, correct biomechanical deficiencies, increase strength and endurance, and restore motion and function.10,23 Among the nonoperative treatment approaches that are recommended in a rehabilitation program for PFPS are the therapeutic modalities.3,4,10,15,16,20,27 In addition, the American Physical Therapy Association’s Guide for Physical Therapist Practice 2 recommends the use of therapeutic modalities for a variety of musculoskeletal conditions, including PFPS.
Recommended modalities for use in patients with PFPS include
thermotherapy (therapeutic heat) for local vasodilation to reduce pain and stimulate healing, in the forms of ultrasound,20,27 moist hot packs, 20 and warm whirlpool 27 ;
phonophoresis20,27 and iontophoresis 20 to reduce inflammation and pain;
transcutaneous electrical nerve stimulation (TENS) for pain20,27;
neuromuscular electrical stimulation (NMES) to facilitate quadriceps muscle activity, which may be helpful in muscle reeducation in those who have acute pain, edema, or significant weakness and are unable to properly activate their vastus medialis9,10,20,27; and
electromyographic (EMG) biofeedback to promote selective activation of the vastus medialis for selective strengthening or to restore muscle balance in knee extension.3,16,21,31
Despite the incorporation of these therapeutic modalities into the recommended treatment of PFPS patients, there has not been a systematic review of evidence for such practice. The purpose of this review is to examine the evidence basis for the use of therapeutic modalities in the rehabilitation of the PFPS patient.
Methods
Search
In May and August 2010, the literature was searched using the following databases for the years 1970 to 2010: PubMed, CINAHL, Web of Science Citation Index, Science Direct, ProQuest Nursing & Allied Health, and Your Journals@OVID. The database review began with a general search using the term patellofemoral pain syndrome treatment, followed by searches using the term patellofemoral pain syndrome paired with therapeutic modality, cryotherapy, cold, Cryocuff, thermotherapy, heat, diathermy, ultrasound, moist hot pack, whirlpool, electrical stimulation, TENS, NMES, biofeedback, EMG biofeedback, and laser.
Only studies in peer-reviewed journals were considered. No abstracts, dissertations, theses or articles from meeting proceedings were reviewed.
Study Selection
Studies had to meet the following criteria:
Population: principal diagnosis of PFPS; no additional knee pain diagnoses; both sexes and all age ranges included
Study design: randomized controlled trial—either direct comparison to control or 2-group (or more) comparison
Interventions: one of the therapeutic modalities as the intervention; no limitations placed on the use of concurrent treatments or the nature of control groups
Outcome measures: knee extension and flexion strength (isokinetic and isometric), patellofemoral pain assessment during activities of daily life, functional tests (eg, squats, step-up/step-down), Kujala patellofemoral score, 19 and EMG recording from knee flexors and extensors (specifically comparing vastus medialis and vastus lateralis) and quadriceps femoris cross-sectional area.
Language: non-English-language studies excluded
Quality Assessment
Quality was independently assessed by both authors using the PEDro Scale 22 and a second system, 8 specifically designed for interventions for patellofemoral pain.
This system uses 4 main criteria: population, interventions, effect size, and data presentation and analysis. Each criterion is composed of 3 or 4 scored items for a total of 100 points. This scale has a high interrater reliability, with intraclass correlation coefficients for items ranging from 0.64 (for intervention standardization and description) to 0.99 (for the blinding of outcome assessors). The intraclass correlation coefficient for the total quality score was 0.97.
Results
Study Selection
Twelve studies were identified that met the criteria: 1 investigated the effects of cold and ultrasound, ice alone, iontophoresis, and phonophoresis 4 ; 3 studied the effects of NMES7,11,12; 4 investigated the effects of EMG biofeedback16,18,21,31; 3 evaluated the effects of electroanalgesia (electrical stimulation for management of pain)1,5,13; and 1 studied the effects of low-intensity laser therapy 25 (Table 1).
Study Characteristics. a
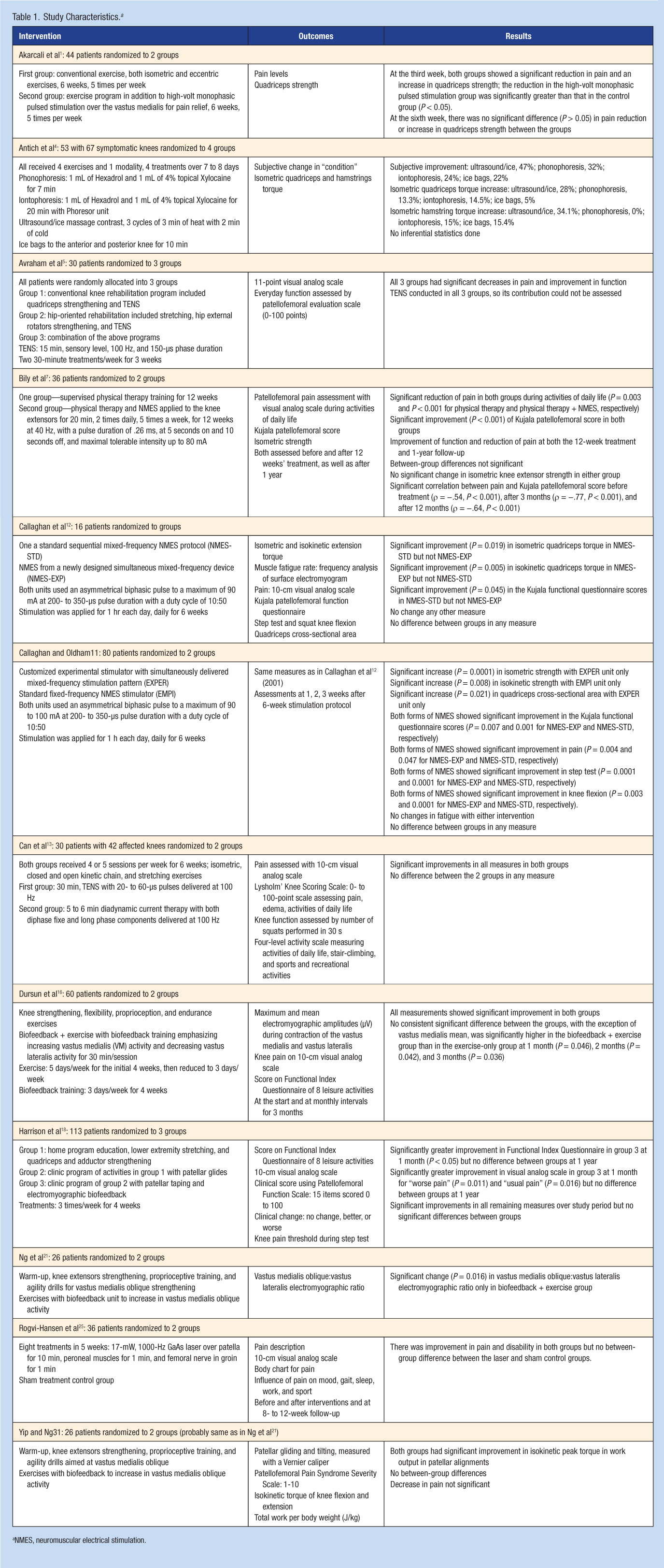
NMES, neuromuscular electrical stimulation.
Quality Assessment
Quality scores were based on the analysis of 2 independent reviewers (D.A.L., N.H.W.). Reviewers’ scores on the patellofemoral-specific scale 8 ranged from 19 to 79 (maximum score, 100). Average quality scores based on the use of the PEDro Scale ranged from 4 to 8 (maximum score, 10).
Discussion
Ultrasound and Ice Massage, Ice Bags, Phonophoresis, and Iontophoresis
The single study 4 of the ultrasound and ice massage, ice bags, phonophoresis, and iontophoresis modalities reported improvement in subjective symptoms and hamstring and quadriceps strength. However, there was no control group, and no inferential statistics were performed; so, the significance of these changes cannot be determined. The quality of this study was the lowest of all articles reviewed, with a 19 of 100 on the patellofemoral-specific scale 8 and 4 of 10 on the PEDro Scale. 22 Because of the poor quality of the study and the use of an exercise program with the modalities, there is no evidence that any of these modalities are effective in treating PFPS.
Neuromuscular Electrical Stimulation
Each study postulated that selective strengthening of the vastus medialis using NMES could enhance a standard exercise protocol in reducing the symptoms of PFPS. Studies varied in quality, with a range of 57 to 79 of 100 on the patellofemoral-specific scale 8 and 5 to 6 of 10 on the PEDro Scale.
Three studies showed improvements in several measures of pain and function.7,11,12 Because the exercise protocol was part of the intervention in these groups, it is not possible to separate the effects of NMES from the known positive effects of exercise on PFPS. 6 The results of these 3 studies suggest that there is no added benefit of NMES when combined with standard physical therapy.
EMG Biofeedback
Studies on EMG biofeedback varied widely in quality, with a range of 50 to 76 of 100 on the patellofemoral-specific scale of Bizzini et al 8 and 6 to 8 of 10 on the PEDro scale.
Significantly greater short-term improvements in pain and functional measures were reported when exercise was combined with EMG biofeedback and patellar taping, compared with exercise alone. 18 However, at 1 year following the intervention, there were no significant differences between the 2 groups. The decreased number of patients at the 1-year follow-up may have contributed to this lack of significance difference. Unfortunately, the effect of patellar taping cannot be separated from EMG biofeedback.
Differences in pain or functional measures between exercise and exercise combined with EMG biofeedback were not found, whereas increased recruitment of the vastus medialis/vastus medialis oblique was seen. 16 EMG biofeedback may be useful in activation of the vastus medialis oblique, but this may have little impact on pain and function. Similarly, no differences in pain or functional scores were reported for an exercise program as compared with exercise combined with EMG biofeedback.21,31 Significant improvement in the vastus medialis oblique:vastus lateralis EMG ratio was seen with the EMG biofeedback. 21 EMG biofeedback may be able to affect the relative activation of the vastus medialis/vastus medialis oblique when compared with the vastus lateralis, but when combined with an exercise program, EMG biofeedback has no additional effect in reducing the symptoms of PFPS.
Electrical Stimulation for Pain Control
One study 5 included TENS in all 3 experimental groups, so the effect of TENS in isolation of other treatments could not be assessed. A second study 13 compared TENS with diadynamic current therapy, both used in combination with an exercise program, and it found no difference between the 2 pain-reducing electrical modalities. The third of these 3 studies 1 reported that when high-volt monophasic pulsed stimulation was used in combination with an exercise program, compared with the exercise program alone, there was a significant difference between the 2 groups after 3 weeks of treatment, but after 6 weeks of treatment, there were no between-group differences. Conclusions cannot be drawn about the efficacy of electrotherapy for pain control on treating the symptoms of PFPS, because in these studies, electrical stimulation was used with exercise in all groups 13 or included in each intervention. 5 The one study 1 that had an exercise control suggested a short-term advantage to high volt monophasic pulsed stimulation, but at the end of treatment, there was no additive effect in reducing the symptoms of PFPS.
Low-Intensity Therapeutic Laser
There was no significant difference in any measure for the laser when compared with a sham laser control in the treatment of patients with PFPS. 25 There was a range of variables in the treatments with laser therapy, including wavelength, power, power density, energy, energy density, treatment duration, treatment intervention time postinjury, and method of application (contact mode versus noncontact mode). 30 The effectiveness of laser therapy may be related to these parameters. No conclusions can be reached from this study.
Conclusions
None of the therapeutic modalities reviewed has sound scientific justification for the treatment of PFPS.
Footnotes
No potential conflict of interest declared.