
Abstract
Marathon running has evolved considerably over the past several decades. What was once a sport of elite athletes has now become a goal for many average and inexperienced runners. A comparison of race entrants and finishing times at the New York City marathon in 1978 and 2001 showed that the number of participants had almost tripled and that a large portion of the runners required substantially more time to complete the marathon, suggesting that the overall fitness level had decreased. 11 The USA Track and Field Road Running Information Center confirms this trend: 25 000 US marathon finishers in 1976 compared to 425 000 in 2008. 14 The median finishing time in the United States increased from 3:32:17 in 1980 to 4:20:04 in 2008. 14 As the number of participants has grown and the experience level has become more varied, medical teams are likely to experience a larger need for care on race day.
Endurance running challenges the human body in several ways. The annual incidence of injury for runners training for a marathon may be as high as 90%. 4 Experienced runners are less injury prone than less experienced runners. 4 On the day of the marathon, 2% to 8% of the participants seek medical assistance; fortunately, serious health issues are rare. 12
Running generates significant heat. Sweating dissipates that heat, resulting in a loss of body water, with urine and respiratory losses contributing to a small extent. 13 Sweat rates are variable and attributed to environmental conditions, physical conditioning, exercise intensity, clothing, genetic design, and level of acclimatization. 13 Fluid intake during exercise replenishes body water losses, but care should be taken not to overhydrate. Exercise-associated hyponatremia is potentially fatal and primarily caused by fluid intake in excess of sweat and urine losses. 5 Exercise duration, running pace, and inexperience are among the several known risk factors for exercise-associated hyponatremia. 5
The goal of this study was to examine the experience of the typical marathon participant regarding the potential complications of running a marathon and hydration status.
Methods
Participants
Institutional review board approval was obtained by the authors. Runners of the 2007 LaSalle Bank Chicago Marathon were recruited for a survey while attending the Marathon Expo 2 days before the marathon. The researchers were available for questions. Participants were informed that their participation was optional, and verbal consent was obtained.
Survey Details
The survey asked for age, sex, number of years running, number of completed marathons, and number of months training for the marathon (specifics of training type or frequency were not defined on the survey).
Runners were asked to recall injuries suffered during the current and previous running seasons. The definition of injury was left to the interpretation of the participant. They were also asked if they had ever been treated in the medical tent during or after a marathon and, if so, for what reason. The 8 reasons provided were musculoskeletal (sprains/strains), dehydration, vomiting, cramping, bleeding, dizziness/passed out, over- or underheated, and low sodium. Additionally, the runners qualified their concern for musculoskeletal injury and hyponatremia during the race on a 5-point scale.
Runners were questioned regarding their preference for water or sports beverage during training and the race. The participants were asked to estimate (in ounces) the expected volume of water and sports beverage that they planned to consume during the race. They were asked whether they supplement their fluids with additional electrolytes (salt tablets), carbohydrates, caffeine, or other supplements. They were also asked if they weigh themselves before and after runs, if they knew their sweat rate, or if other methods to assess hydration status were used.
Statistics
Frequency distributions, means ± SD, correlations, χ2, and 1-way analysis of variance were calculated for the responses as appropriate. Relationships were examined among sex, age, running experience, marathon experience, treatment in the medical tent for dehydration versus other reasons, concern for musculoskeletal injury, concern for hyponatremia, choice of beverage, and hydration assessment strategies. A probability level of 0.05 was selected for statistical significance. 3 Calculations were made using SPSS 15.0.1 software.
Results
Demographics
In sum, 419 runners completed the survey (211 women, 38.3 ± 9.1 years old; 208 men, 41.6 ± 11.0 years old).
Runners in our sample had trained for the marathon for 6.8 ± 4.3 months and had been running for 9.8 ± 9.1 years. Of the 419 runners completing the survey, 135 (33.5%) had never run a marathon before and 70 (16.9%) had run 1 previous marathon. Out of the 48 463 registrants for the marathon, 35% had never run a marathon before.
Injuries
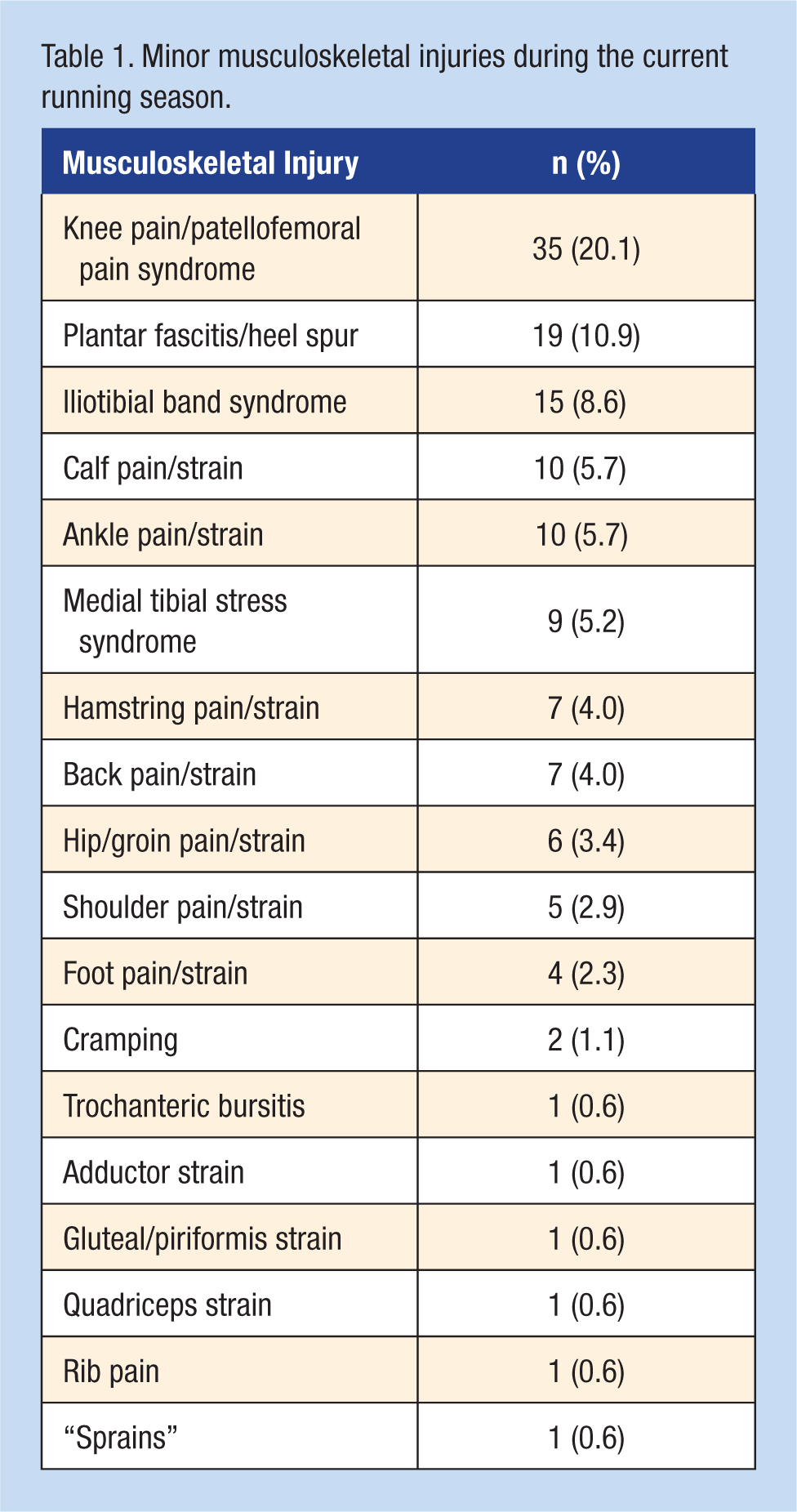
Overall, 129 (30.8%) participants reported suffering 1 injury during the current running season; 21 (5.0%) reported 2; and 1 (0.2%) reported 3. Of those, 135 (77.6%) were minor musculoskeletal injuries (Table 1).
Minor musculoskeletal injuries during the current running season.
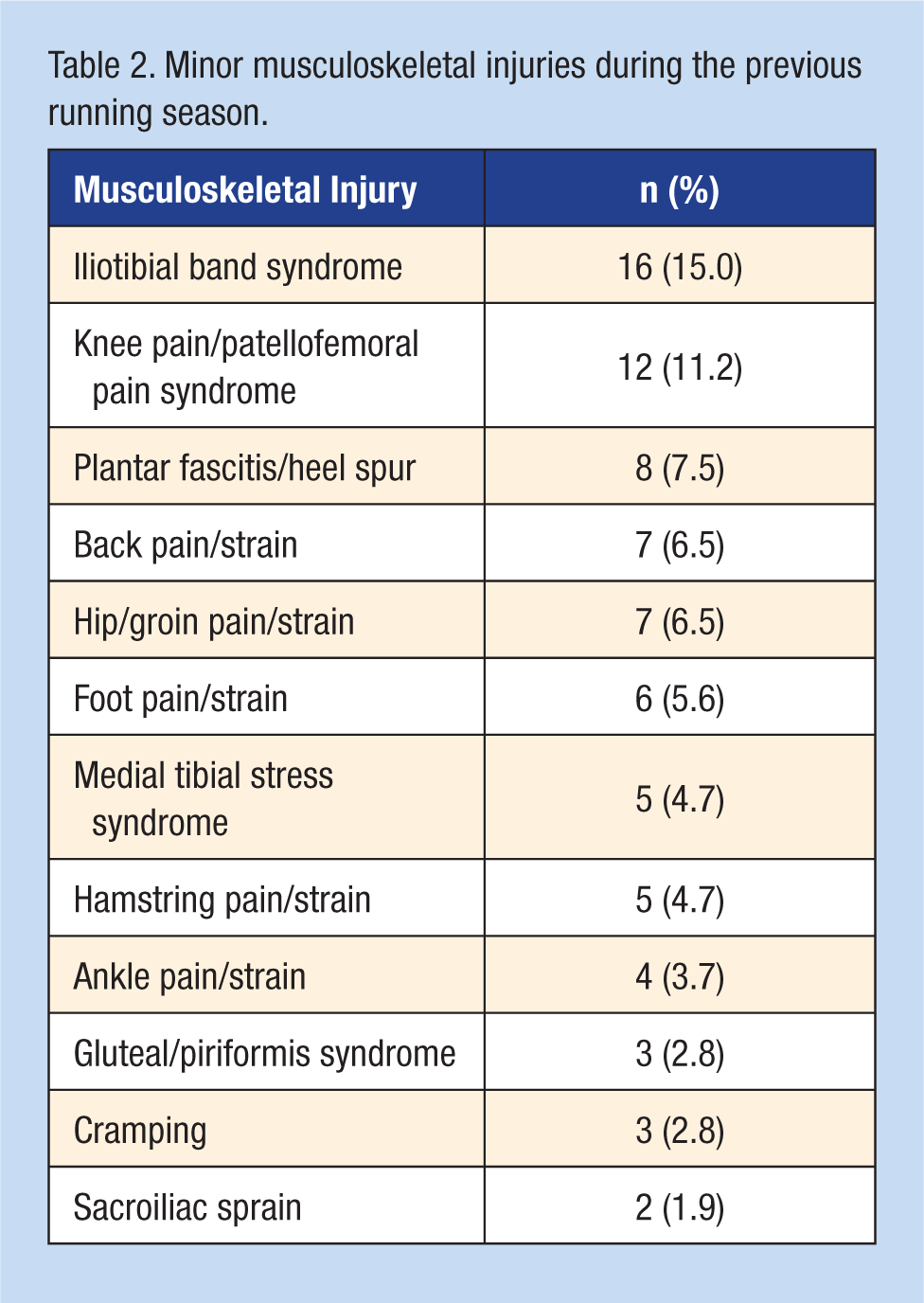
A total of 91 runners (21.7%) reported suffering 1 injury during the previous running season, and 8 (1.9%) reported 2. The 107 total injuries in the previous running season included 78 (72.9%) minor musculoskeletal injuries (Table 2).
Minor musculoskeletal injuries during the previous running season.
Of the 278 survey participants who had completed a marathon, 54 (19.0%) had been a patient in a medical tent: 17 (31.5%) for dehydration, 10 (18.5%) for cramping, 9 (16.7%) for dizziness or passing out, 6 (11.1%) for musculoskeletal issues, 5 (9.3%) for vomiting, 3 (5.6%) for bleeding, 3 (5.6%) for heat or cold related illnesses, and 1 (1.9%) for hyponatremia.
Of the survey respondents, 223 (54.9%) and 257 (64.3%) stated that they were “not at all” concerned with musculoskeletal injury and hyponatremia, respectively; 67 (16.5%) and 61 (15.4%) stated that they were “moderately,” “very much,” or “extremely” concerned about musculoskeletal injury or hyponatremia, respectively.
Fluid Strategies
In sum, 271 participants (65.3%) reported drinking both water and sports beverage during training and 298 (71.0%) on race day; 106 (25.5%) drank only water during their training and 74 (17.7%) planned to drink only water on race day; and 38 (9.2%) drank only sports drink during training and 46 (11.0%) planned to drink only sports drink on race day.
The average estimate of planned beverage consumption during the race was 55.8 oz (1.65 L) for water and 42.2 oz (1.25 L) for sports drink. The average total amount of planned beverage consumption was 81.2 oz (2.40 L).
Most runners reported no knowledge of their sweat rate (n = 370, 88.7%), and the majority did not weigh themselves to assess hydration status (n = 284, 67.8%). Furthermore, 335 (81.3%) did not address hydration status; 77 (18.7%) used other methods; and 38 (49.3%) used urine color. The other methods of hydration assessment were thirst (n = 9, 11.7%), distance (n = 3, 3.9%), past experience (n = 3, 3.9%), “scale” (n = 2, 2.6%), general feeling (n = 2, 2.6%), and frequency of urination (n = 2, 2.6%); pulse, cramping, amount drank, “sweat,” and “pinch test” were all listed once (1.3%). Finally, 265 runners (60.1%) supplemented their fluids with carbohydrate, 86 (19.5%) with electrolytes or salt tablets, 68 (15.4%) with caffeine, and 22 (5.0%) with supplements.
Discussion
The sample of runners who completed the survey was a relatively good representation of the entire group of people who ran the marathon. Most participants were inexperienced marathon runners. The majority of runners in the sample were not concerned about musculoskeletal injury or hyponatremia. Only 1.4% of the survey participants received medical attention on race day, which is lower than the previously reported 2% to 8% seeking medical attention the day of the marathon. 12 A minority of runners in our sample used methods to assess their hydration status. Roughly one-third of the total number of survey participants weighed themselves before and after running, compared with almost one-half of those who had been treated in a medical tent for any reason who reported self-weighing.
In its position stand on exercise and fluid replacement, the American College of Sports Medicine recommends monitoring hydration status with body weight changes, urine-specific gravity, and/or osmolality. 13 Not many have access to urine testing materials; however, self-weighing is accessible. Self-weighing is the “simplest and most accurate index of hydration status” for athletes in the field. 1 A study surveying college athletes found that only 15% were weighing themselves, even though 66% stated that they understood that weight changes evaluate hydration status. 10
A position statement by the International Marathon Medical Directors Association stated that weight changes may not be the most accurate indicator of hydration status, because the body defends plasma osmolality and not weight. 6 Cyclists participating in an ultramarathon event avoided dehydration despite significant body weight change. 9 Weight changes in ultramarathon runners have been good measures of hydration status. 7
An athlete should replace 50% to 80% of their sweat losses to maintain an adequate blood volume and appropriate core temperature during endurance exercise. 2 On average, marathon runners complete the race with 3% to 4% dehydration and replace less than 50% of their sweat losses.2,8 Self-weighing may be most useful in determining when individuals have hydrated too much. It is a worrisome sign to maintain or gain weight during a marathon, owing to the potential for exercise-associated hyponatremia.5-7,13
Performance deficits and cardiovascular strain can occur with body water losses of greater than 2%.6,8,10 The ultramarathon runner can lose approximately 6% of his or her body weight. 7 Thirst is activated when body water is decreased 1.7% to 3.5%.6,8 Runners who drink according to thirst consistently dehydrate. 6
Limitations
The potential limitations of this study include language, terminology, and sampling bias. Survey participants may not have understood the meaning of questions despite attempts to clarify the terms.
Conclusions
The majority of runners were inexperienced marathoners, lacked concern about musculoskeletal injury or hyponatremia, and did not use methods to assess their hydration status.