
Abstract
Context:
Both spondylolysis and spondylolisthesis can be diagnosed across the life span of sports-participating individuals. Determining which treatments are effective for these conditions is imperative to the rehabilitation professional.
Data Sources:
A computer-assisted literature search was completed in MEDLINE, CINAHL, and EMBASE databases (1966-April 2012) utilizing keywords related to nonoperative treatment of spondylolysis and/or spondylolisthesis. Reference lists were also searched to find all relevant articles that fit our inclusion criteria: English language, human, lumbar pain with diagnosed spondylolysis and/or spondylolisthesis, inclusion of at least 1 nonoperative treatment method, and use of a comparative study design.
Data Extraction:
Data were independently extracted from the selected studies by 2 authors and cross-referenced. Any disagreement on relevant data was discussed and resolved by a third author.
Results:
Ten studies meeting the criteria were rated for quality using the GRADE scale. Four studies found surgical intervention more successful than nonoperative treatment for treating pain and functional limitation. One study found no difference between surgery and nonoperative treatment with regard to future low back pain. Improvement was found in bracing, bracing and exercises emphasizing lumbar extension, range of motion and strengthening exercises focusing on lumbar flexion, and strengthening specific abdominal and lumbar muscles.
Conclusion:
No consensus can be reached on the role of nonoperative versus surgical care because of limited investigation and heterogeneity of studies reported. Studies of nonoperative care options suffered from lack of blinding assessors and control groups and decreased patient compliance with exercise programs.
Instability of the lumbar spine is one of multiple pathologic causes of low back pain (LBP).19,20 It can be defined as a loss of motion stiffness such that forces applied to a given segment produce greater displacement than would occur normally. 22 Spondylolysis and spondylolisthesis can cause LBP because of instability. Spondylolysis is a bony defect, possibly a stress fracture, of one or both pars interarticularis and most commonly occurs in the lower lumbar spine (Figure 1). 3 Prevalence of spondylolysis ranges from approximately 6% to 11.5% in the general population 9 and approximately 7% to 8% in elite athletes; this percentage is grossly underreported.12,26,27 Nearly 50% of LBP cases in adolescent athletes have been attributed to spondylolysis. 21
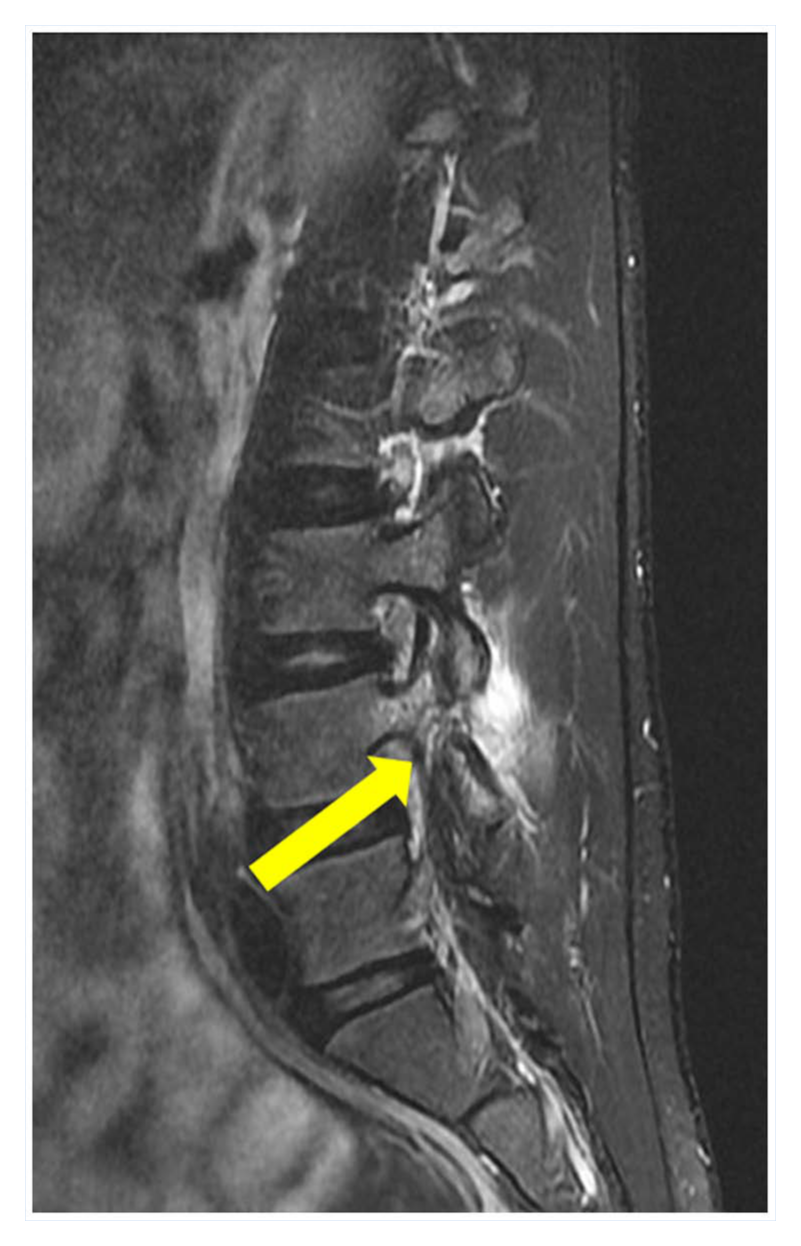
Sagittal fat-saturated T2-weighted image showing a defect of the right pars interarticularis at L4. Adjacent high signal in the marrow and soft tissues on the image reflects acute or subacute fracture.
Repetitive microtrauma leading to spondylolysis has been attributed to lumbar hyperextension combined with rotation and loading.11,26,27 These injuries occur in dancers, gymnasts, figure skaters, weight lifters, and football players26,27; active spondylolysis has been reported in almost every sport. 11
Spondylolisthesis is displacement of a vertebra due to a defect in the pars (Figure 2). 14 Spondylolysis is a precipitating factor and can be classified as isthmic, dysplastic, degenerative, traumatic, and pathologic.7,31,32 Spondylolisthesis severity can be graded I through IV. Grade I is displacement of 0% to 25%; grade II, 26% to 50%; and grade III, up to 75%. Displacement of 75% to 100% is grade IV. 16
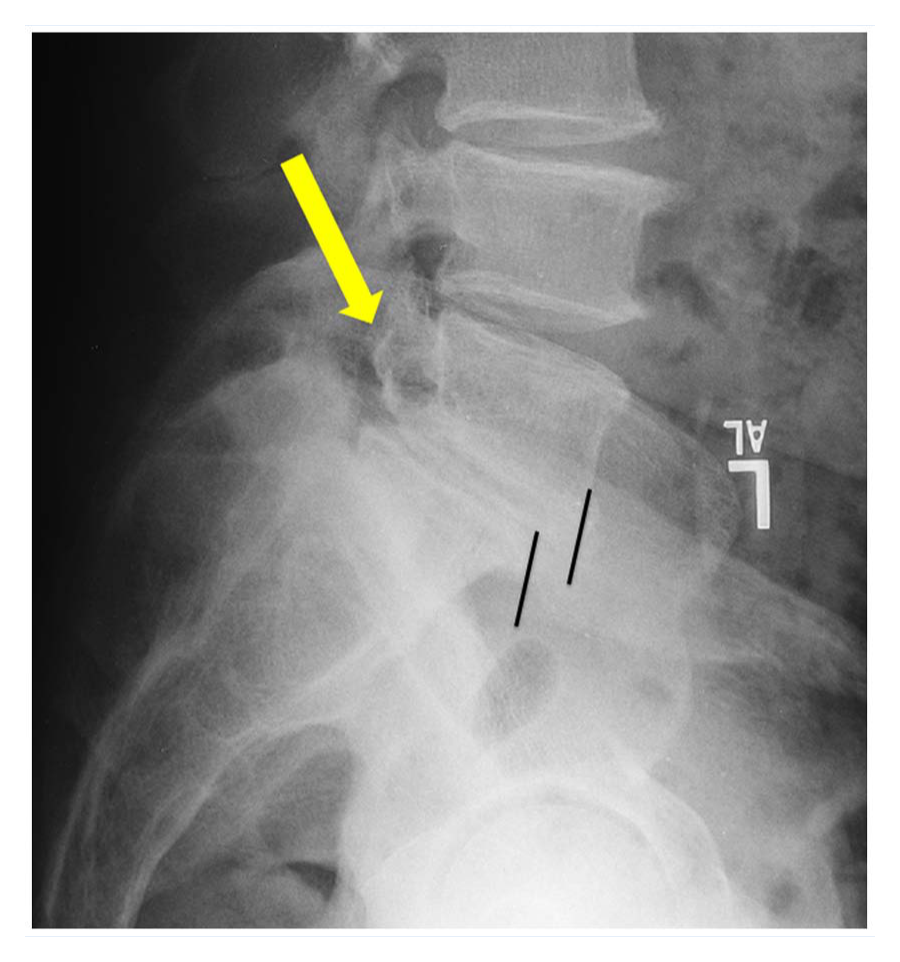
Radiograph of fracture of pars interarticularis (yellow arrow) with grade II spondylolisthesis demonstrating slippage (black lines).
Etiologic factors, 6 degree of slippage, 16 and pathology type7,31,32 reflect the heterogeneous nature of both spondylolysis and spondylolisthesis. Computed tomography, single-photon computed tomography, and magnetic resonance imaging techniques assist in the accurate diagnosis of spondylolysis and spondylolisthesis. Guidelines for these conditions remain elusive.11,26,27
Development of guidelines requires a systematic review of the current level of evidence. Consequently, the purpose of this review is to systematically review nonoperative methods of intervention as related to spondylolysis and spondylolisthesis.
Methods
Data Sources
An electronic literature search of MEDLINE, CINAHL, and EMBASE databases was performed for articles published between 1966 and April 2012. The MESH search terms for MEDLINE included: (spondylolysis OR spondylolisthesis) AND (lumbar vertebrae OR lumbar spine) AND (physical therapy OR rehabilitation OR stabilization OR strengthening OR motor control OR massage OR joint mobilization OR joint manipulation OR manual therapy OR stretching OR conservative treatment OR therapy OR athletic OR training OR bracing), limited to the English language and human subjects. The reference lists were also checked to retrieve relevant publications. Gray literature (textbooks, abstracts presented at conferences, web information, etc) was also hand searched.
Study Selection
Full-text articles were retrieved if the abstract provided insufficient information to establish eligibility or if the article had passed the first eligibility screening. All articles examining nonoperative treatment of spondylolysis and/or spondylolisthesis were eligible if they met all of the following criteria: (1) patients presenting with lumbar spine pain with primary diagnosis of spondylolysis and/or spondylolisthesis; (2) cohort, case control, and/or cross-sectional design; (3) inclusion of at least 1 nonoperative therapy for spondylolysis/listhesis (relevant to physical therapy or athletic training); and (4) article was in English.
An article was excluded if (1) other pathologies were present, (2) nonoperative treatment was omitted, and (3) subjects were infants or toddlers. Criteria were independently applied by 2 reviewers (MG, JS). A third author (MR) was consulted to resolve disagreements. This screening resulted in 10 full-text articles for data extraction (Table 1 and Figure 3).
Description of included studies
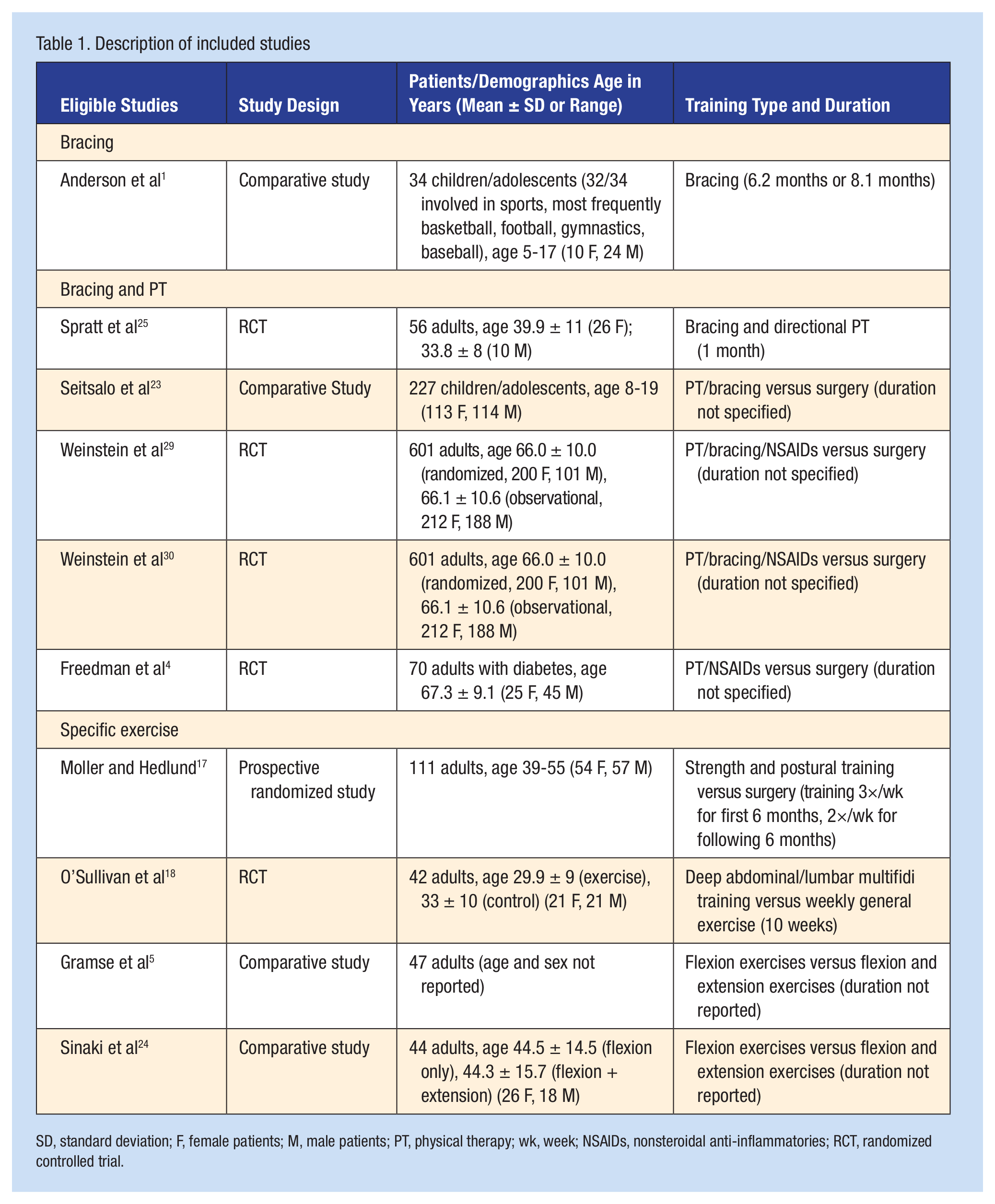
SD, standard deviation; F, female patients; M, male patients; PT, physical therapy; wk, week; NSAIDs, nonsteroidal anti-inflammatories; RCT, randomized controlled trial.
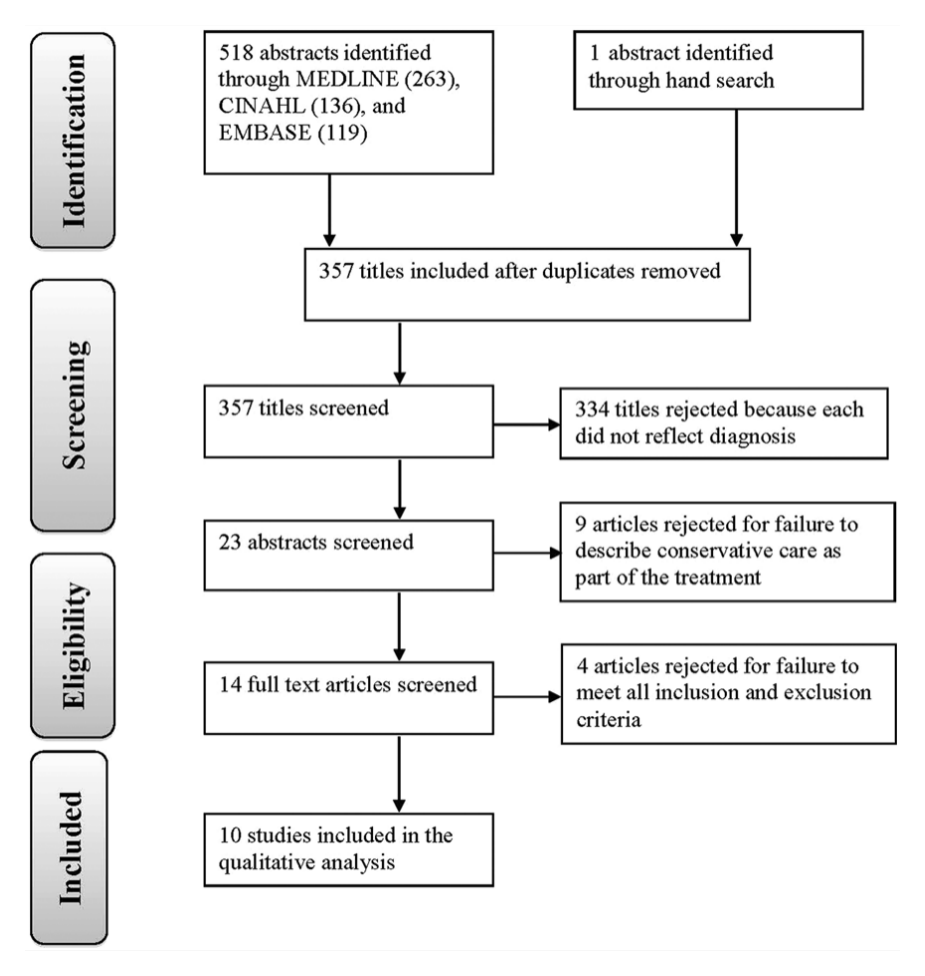
Flow diagram of study.
Data Extraction
Data on the study population, description, intervention, outcome measures, and results were independently extracted and cross-referenced (Tables 1-5; see appendix, available at http://sph.sagepub.com/content/suppl).
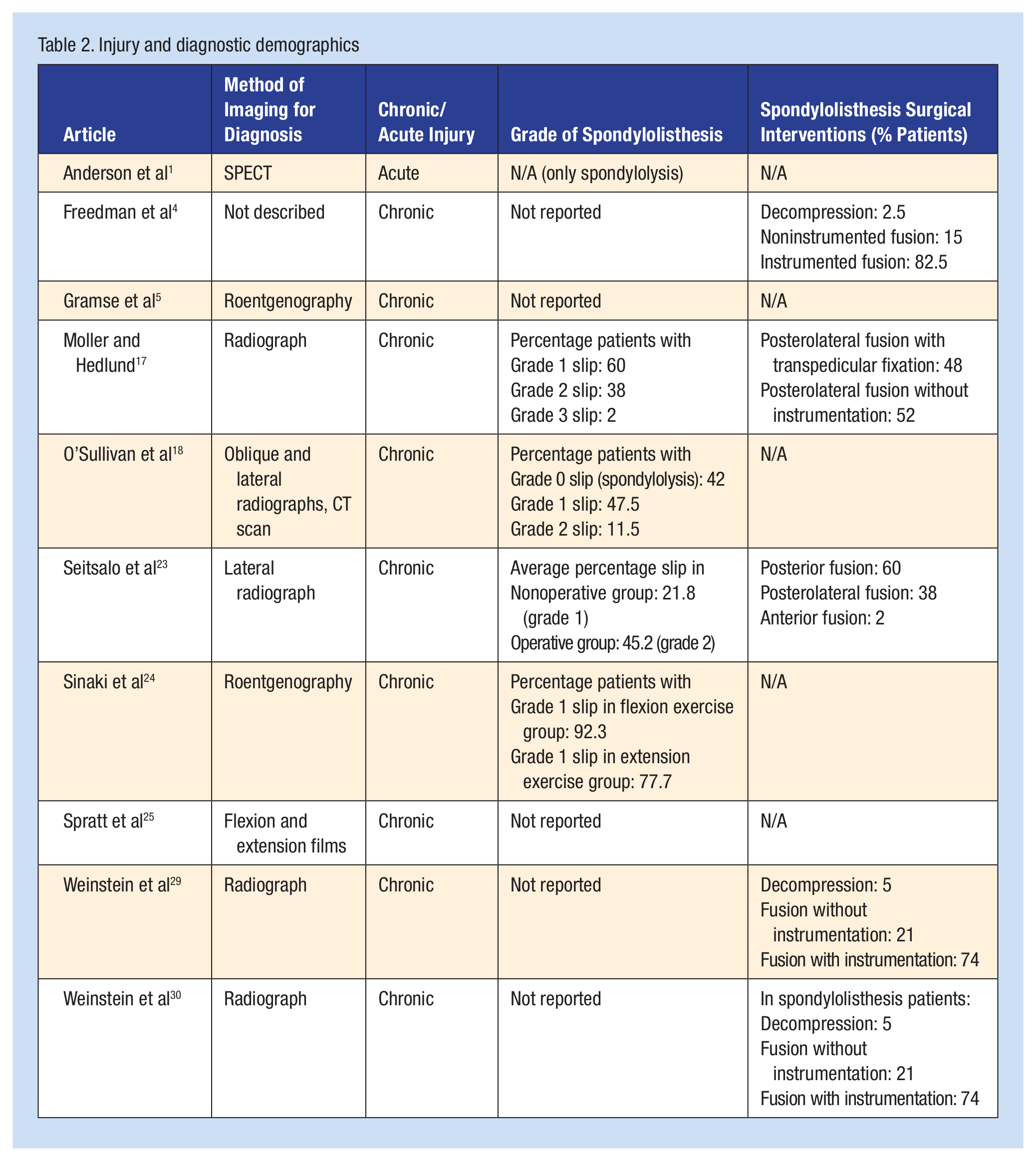
Injury and diagnostic demographics
Bracing versus activity restriction: interventions, outcomes, and results
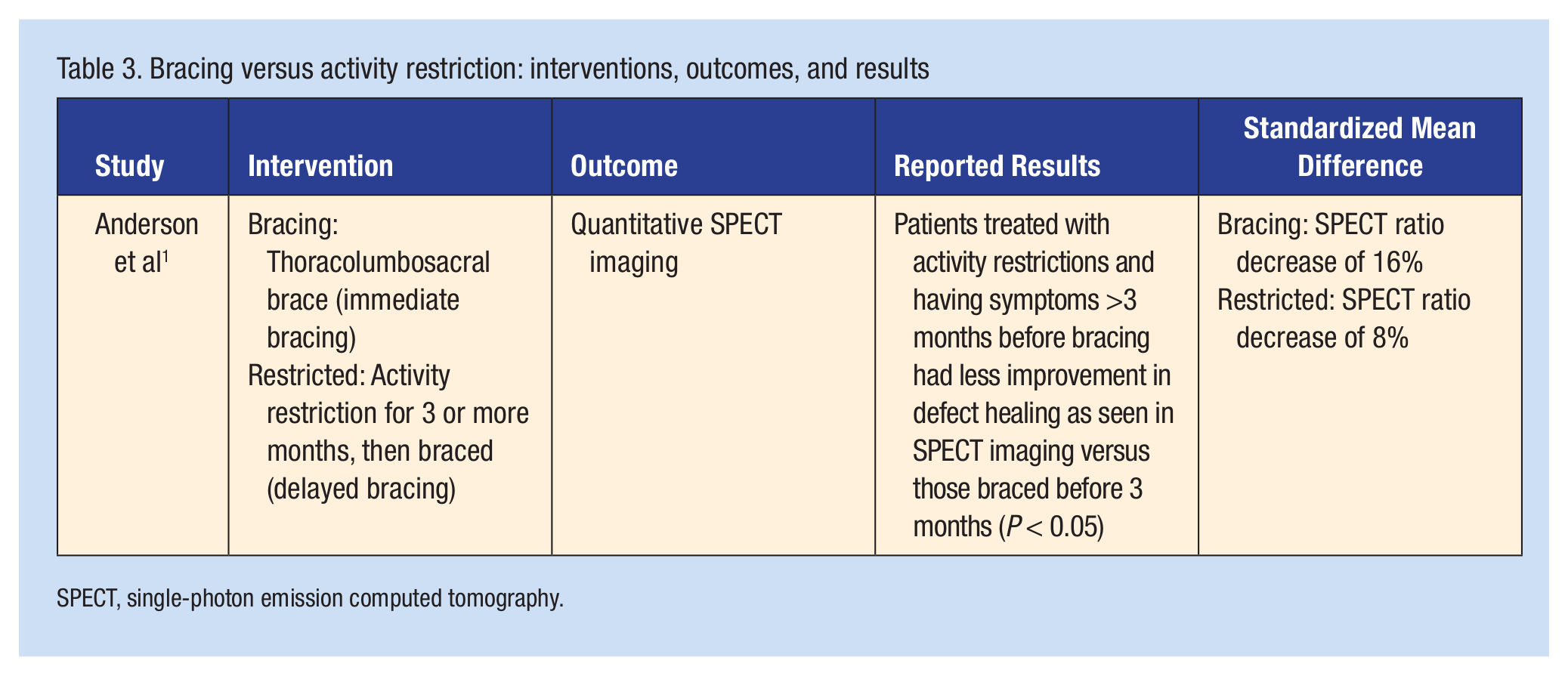
SPECT, single-photon emission computed tomography.
Bracing and direction-based PT versus placebo control
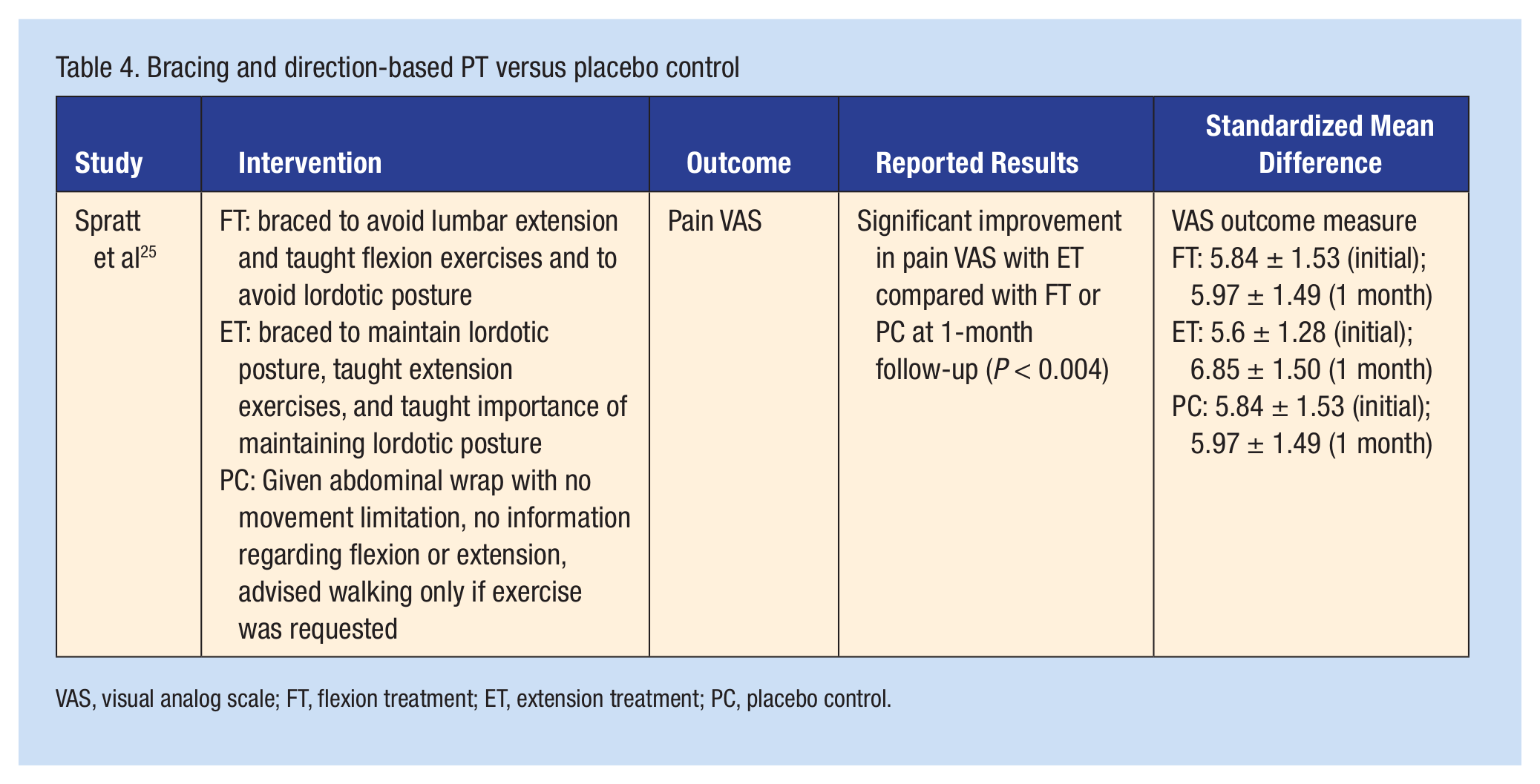
VAS, visual analog scale; FT, flexion treatment; ET, extension treatment; PC, placebo control.
Exercise interventions
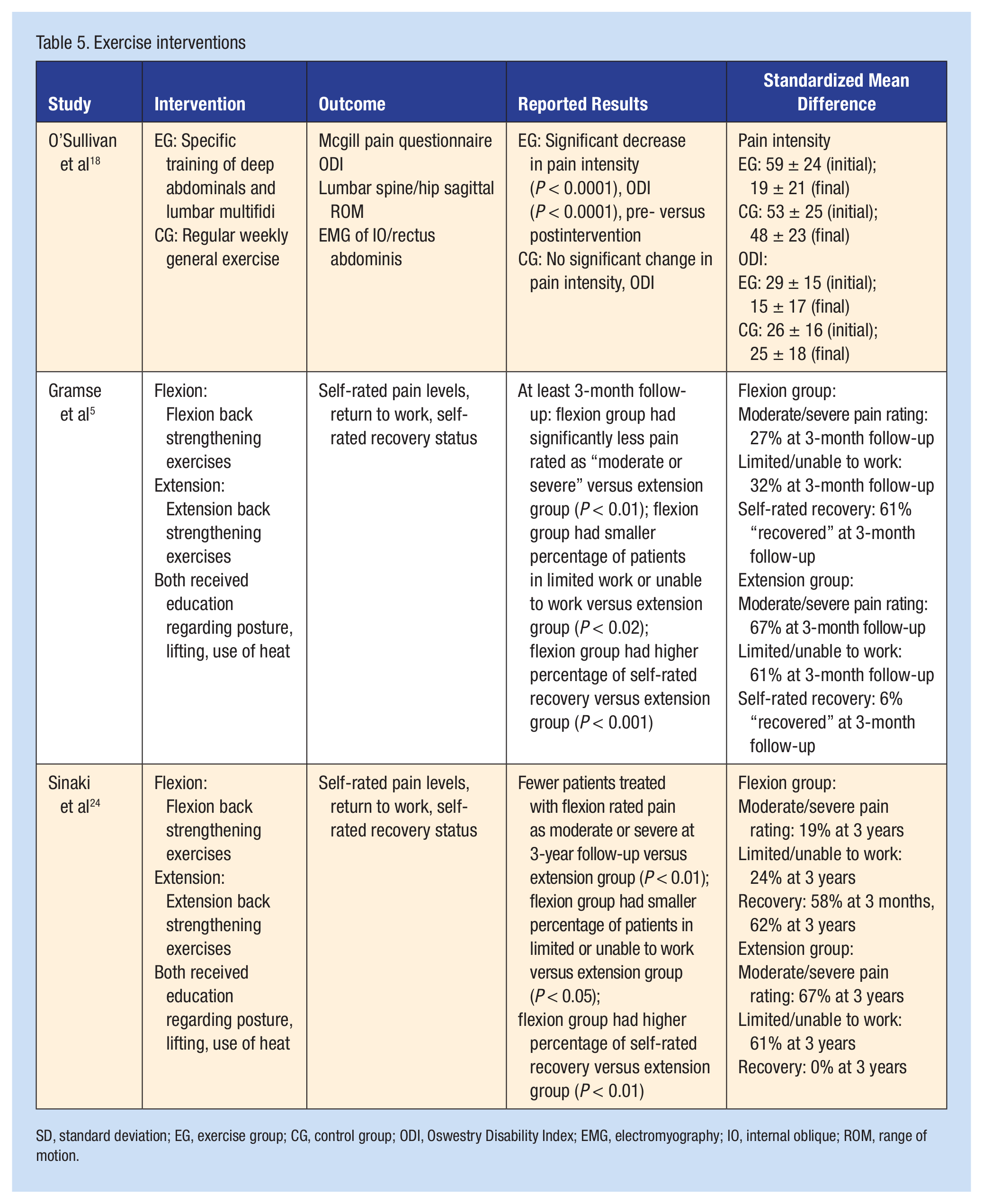
SD, standard deviation; EG, exercise group; CG, control group; ODI, Oswestry Disability Index; EMG, electromyography; IO, internal oblique; ROM, range of motion.
Results
The systematic search through MEDLINE, CINAHL, and EMBASE yielded 10 eligible studies for data extraction. Of these 10 studies, 5 were randomized controlled trials,4,18,25,29,30 1 was a prospective randomized study, 17 and 4 were comparative studies without randomization or a control group.1,5,23,24 One study compared the use of brace treatment with activity restriction, 1 5 studies compared nonoperative care to surgical interventions,4,17,23,29,30 and 3 studies compared exercise protocols.5,18,24 One remaining study compared a combination of bracing and specific exercise protocol with a placebo control group. 25
One study included a combination of patients with spondylolysis and spondylolisthesis, 18 1 only spondylolysis, 1 while the remaining 8 used spondylolisthesis.4,5,17,23-25,29,30
The age of subjects in the studies varied widely: 2 had a mean subject age in the teens (13 and 13.8 years).1,23 Four had mean ages in the 30s or 40s.17,18,24,25 One study did not report the age of the subjects. 5 The 3 remaining studies had a mean age in the 60s.4,29,30
The 5 studies comparing nonoperative care to surgical interventions found nonoperative care was not as favorable as surgery. Grade of pathology was only reported in 2 of the 5 studies comparing nonoperative and surgical care (Table 2). These studies reported improvement in various pain ratings with fusions or laminectomies compared with strength and postural training, 17 patients with diabetes receiving lumbar fusions or decompressions versus nondescript “conservative care,” 4 and patients undergoing decompressive laminectomy versus patients treated with physical therapy.29,30
Two studies used the same patient population to compare flexion exercises and extension exercises.5,24 Both found significant improvement in pain, return to work, and self-rated recovery in the flexion-based group.5,24 Another study compared lumbar stabilization exercises to general exercise and found significant improvement in functional score and pain rating in the stabilization group. 18
When bracing was combined with flexion or extension exercises and a placebo group, extension exercises and bracing showed significant improvements in pain ratings compared with the flexion group and placebo. 25 A study comparing immediate bracing versus initial activity modification found improved healing of pars interarticularis defects on SPECT imaging in patients braced immediately compared with those treated with activity modification. 1
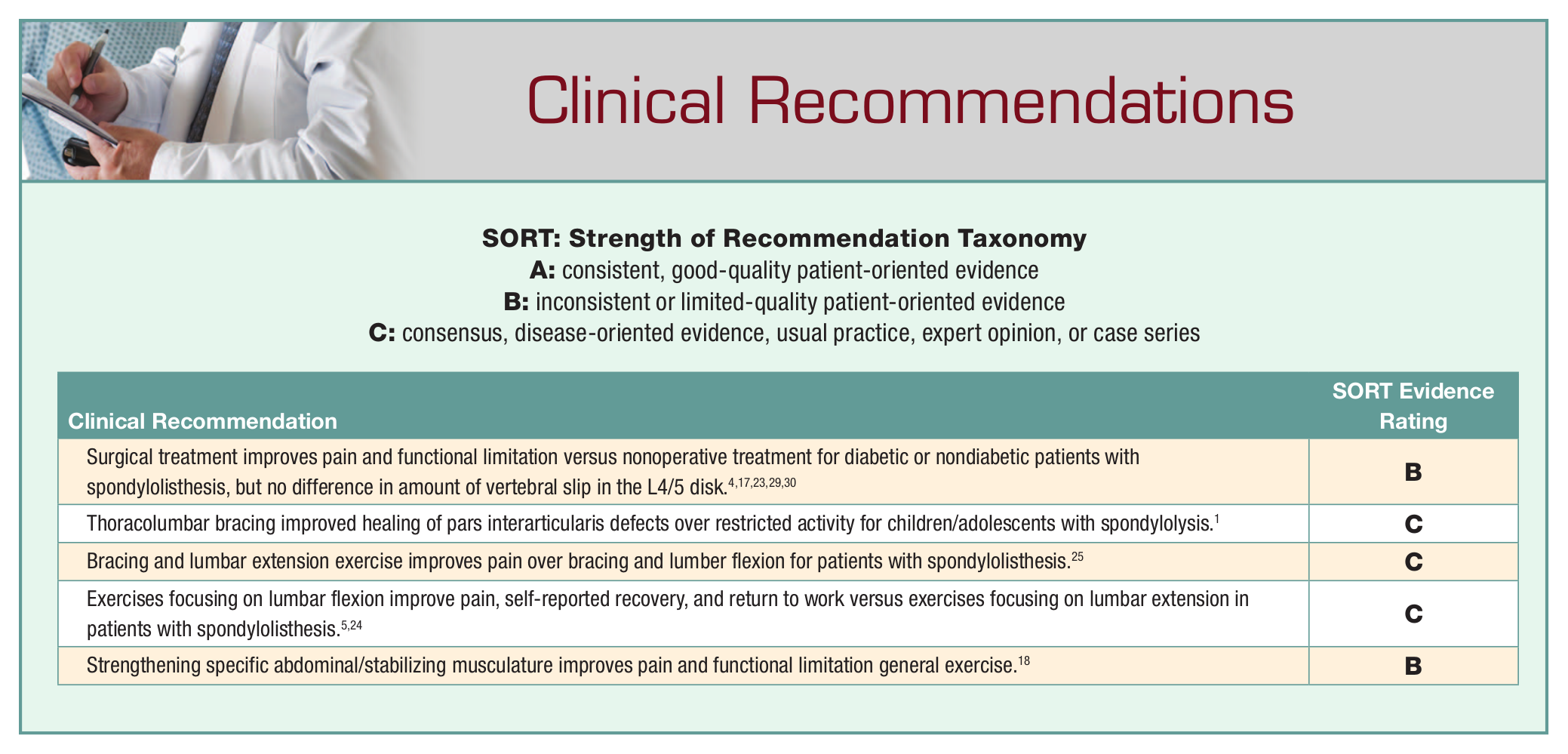
Four studies found surgical intervention more successful than nonoperative treatment for treating pain and functional limitation.4,17,29,30 One found no difference between surgery and nonoperative treatment in regard to vertebral slip, damage to the L4-L5 disk, and low back pain. 23 Of the studies comparing nonoperative treatments, improvement was found in bracing, 1 bracing and exercises emphasizing lumbar extension, 25 range of motion and strengthening exercises focusing on lumbar flexion,5,24 and strengthening specific abdominal and lumbar muscles. 18
Discussion
A previous review examined exercise interventions in these 2 conditions, 15 while this review included bracing, activity restriction, and surgical procedures. This review suggests surgical intervention is more effective than nonoperative treatments for pain and functional limitation in patients with spondylolisthesis when directly compared with each other. Studies that did compare the various nonoperative treatments revealed a variety of conclusions, ranging from no improvement with lumbar flexion exercises and bracing 25 to significant improvement with lumbar flexion exercises 5 and significant improvement with specific muscle strengthening exercise. 18
Previous studies supported the use of various braces with children and adolescents involved in sport. Case series by Sys et al 28 and Iwamoto et al 8 each found a high percentage of return to sport (89.3% and 87.5%, respectively) with nonoperative treatment and bracing.
Repetitive extension and hyperextension, along with rotation, are risk factors for developing and aggravating spondylolysis and spondylolisthesis.11,26,27 The highest levels of stress on the pars interarticularis were found with lumbar extension and rotation. 2 Some patients have greater improvement with extension. 25 Older subjects may have had simultaneous disk pathologies that responded positively to repetitive extension exercises and bracing.
The deep multifidi exert compressive forces as well as aid in control of spinal motion at the segmental level. 10 Therefore, specific strengthening of these stabilizing muscles could be beneficial in an instability condition like spondylolysis or spondylolisthesis. However, muscle activity can be constrained with trunk strength training utilizing functional tasks. 13
Nine of the 10 articles in this review described chronic spondylolysis and/or spondylolisthesis conditions.4,5,17,18,23-25,29,30 One study of the acute condition found that bracing was effective. 1 Positive results with nonoperative treatments were seen within lower grade slippage (grades 0, 1, 2).18,24
Only 4 of 9 studies describing interventions for spondylolisthesis reported the degree of slippage, 1 study showed significant improvement with surgery over nonoperative care (98% of patients had grade 1 or 2 slips), 17 1 study showed no significant difference between surgery and nonoperative care (average slip in nonoperative group was 21.8%, in the surgery group, 45.2%), 23 and 2 studies found improvement with specific exercise compared with different exercise (100% of patients had a grade 2 or less slippage in one study, 92.3% and 77.7% of patients in the 2 exercise groups had a grade 1 slippage in the other study).18,24
Conclusion
No consensus can be reached on the role of nonoperative versus surgical care because of limited investigation and heterogeneity of studies reported. Current studies investigating both nonoperative and surgical outcomes for individuals with spondylolysis/spondylolisthesis are generally poorly defined and suffer from bias, lack of control groups, and blinding of assessors. Poor patient compliance was noted with many of the exercise programs. Many studies lacked uniform reporting of the spondylolisthesis grade, making it difficult to compare patient populations.
Footnotes
The authors report no potential conflicts of interest in the development and publication of this manuscript.