
Abstract
Context:
The overhand pitch is one of the fastest known human motions and places enormous forces and torques on the upper extremity. Shoulder and elbow pain and injury are common in high-level pitchers. A large body of research has been conducted to understand the pitching motion.
Evidence Acquisition:
A comprehensive review of the literature was performed to gain a full understanding of all currently available biomechanical and clinical evidence surrounding pitching motion analysis. These motion analysis studies use video motion analysis, electromyography, electromagnetic sensors, and markered motion analysis. This review includes studies performed between 1983 and 2016.
Study Design:
Clinical review.
Level of Evidence:
Level 5.
Results:
The pitching motion is a kinetic chain, in which the force generated by the large muscles of the lower extremity and trunk during the wind-up and stride phases are transferred to the ball through the shoulder and elbow during the cocking and acceleration phases. Numerous kinematic factors have been identified that increase shoulder and elbow torques, which are linked to increased risk for injury.
Conclusion:
Altered knee flexion at ball release, early trunk rotation, loss of shoulder rotational range of motion, increased elbow flexion at ball release, high pitch velocity, and increased pitcher fatigue may increase shoulder and elbow torques and risk for injury.
Keywords
Overhand baseball pitching is one of the fastest known human motions. 52 Pitching places exceptional forces and torques on the upper extremity.22,23,52 As a result, pitching-related shoulder and elbow pain is highly prevalent at up to 46% to 57% of pitchers. 34 Considerable research has focused on pitching motion analysis to provide insight into the mechanisms of these injuries. The objective of this review is to describe the relationship between pitching mechanics and injury.
Basics of Motion Analysis
Motion analysis allows the calculation of in vivo kinetics. Within the upper extremity, kinetics are derived from inverse dynamics, 19 which assume the human body is composed of inflexible segments linked at joints. Markered motion analysis with reflective markers has been used for most pitching motion analysis because of the accuracy, speed, and ease of data collection.28,36,38,45 However, these systems are subject to several important limitations.
Limitations of Motion Analysis
Motion analysis has several important limitations. Variations in laboratory setup, marker placement, sampling rate, synchronization, calibration, and software assumptions can create significant error. Small variations in marker placement can create large variations in kinematic output within the system. 38 This factor has been identified as the single largest source of variability. 28 Even with this precaution, these markers are affixed to the skin, which can move with respect to the bones during rapid motions. In one review, comparison of bone pins to skin markers during running revealed 63% to 70% average error for rotation and abduction/adduction motions. 45 These factors likely explain the wide variation in the reported reliability of 3-dimensional motion analysis. 36
Electromyography
Muscular activation can be measured with electromyography in synchrony with pitcher motion.8,11,13,18,27,29,30,49,50,55 Understanding these patterns may help to identify at-risk pitchers and rehabilitate injured pitchers.11,26,27 These studies have demonstrated that pitching requires whole-body coordination, with precisely timed and balanced muscular coactivation of nearly every muscle group, including antagonists from the lower extremity,8,55 to the trunk, 50 shoulder musculature,11,18,27,29,30 and forearm musculature.13,49 These results26,27 suggest that neuromuscular activation plays a critical role in the normal pitching motion.
Basics of The Pitching Motion
The overhand pitch is a tightly timed motion that transfers torque generated largely by the lower extremity and core musculature with the stride, pelvic rotation, and torso rotation through the upper extremity. The overhand pitch is a kinetic chain 19 in which each subsequent segment receives the potential and kinetic energy received and generated by the previous segment. These segments are governed by the summation of speed principle 1 in which energy transfer is optimized when the subsequent segment begins rotating as the prior segment has reached maximal angular velocity. 44 In the real world, rotational timing is usually imperfect. 17
The pitch has been traditionally divided into 6 phases: (1) wind-up, (2) stride, (3) cocking, (4) acceleration, (5) deceleration, and (6) follow-through. Each phase serves a specific function. The phases can be defined based on major events during the pitch (Figure 1).14,22,23,51
Wind-up: This phase positions the body in preparation for force generation. The hands are brought together to the chest and the pitcher lifts the lead leg.14,22,23,51
Stride: Initiates velocity generation through linear forward movement and positions the arm in the cocking position. The lag foot remains planted while the lead foot moves forward and down the mound, with the hip and knee extending. As this peaks, the pelvis also rotates to face home plate.14,22,23,51
Cocking: Transfers energy from the lower extremity and core into potential energy stored in the shoulder capsule. Begins with front foot strike and hand separation. The shoulder remains abducted 90° while externally rotating up to 180° through both the glenohumeral and scapulothoracic joints.14,22,23,51 The torso rotates toward home plate, receiving the energy transferred from the pelvis. 43 Late within this phase, shoulder rotational torque and elbow valgus torque peak2,3,22,40 (this moment in the pitch may be critical for superior labral anterior posterior [SLAP] tears and ulnar collateral ligament [UCL] tears).4,7
Acceleration: Transfers all the energy generated within the body onto the baseball. The shoulder internally rotates using the potential energy stored within the capsule as well as explosive power within the internal rotators. The elbow extends and the wrist flexes, imparting further velocity on the ball.14,22,23,43,51
Deceleration: Slows down arm movement beginning with ball release. The arm continues to internally rotate, although with decreasing angular velocity.14,22,23,51 Shoulder proximal or compressive force peaks at several times body weight as the rotator cuff resists the distractive momentum of the arm.16,22
Follow-though: Returns the body to a fielding position in preparation for the next play.14,22,23,43,51
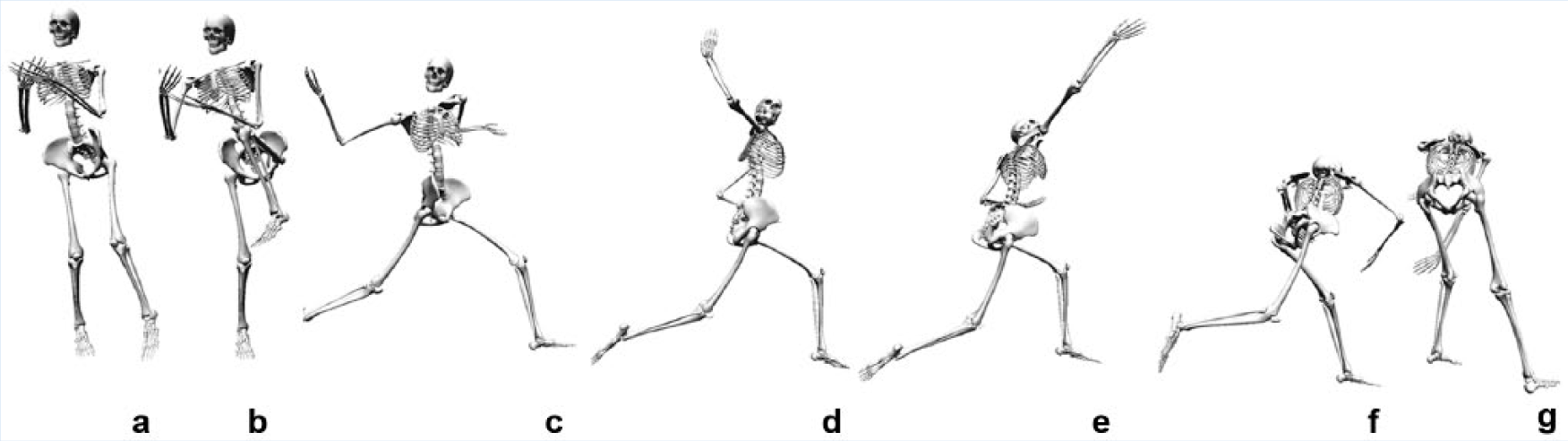
Phases of the pitch for a left-handed pitcher: (a) wind-up, (b) stride, (c) cocking, (d) acceleration, (e) deceleration, (f) follow-through, and (g) end of the pitch.
Pitching Mechanics and Injury
Evidence is divided into empirical clinical data that have informed subsequent motion analysis studies for lower extremity, core and trunk, shoulder, elbow, pitch velocity, and pitcher fatigue.
In a 1-year empirical prospective study of 476 youth baseball pitchers—172 with video motion analysis—no motion analysis factor could be linked to injury. 34 In a 3-year prospective study with video motion analysis of 23 professional baseball pitchers, there was a significant relationship between elbow injury and elbow valgus torque and shoulder maximum external rotation torque. 3 Currently, no prospective clinical evidence exists to connect shoulder proximal force with rotator cuff tears,22,52 shoulder rotational forces with proximal humeral epiphysiolysis, 46 or shoulder rotational torques with internal impingement. 5 Studies have linked velocity to elbow valgus torque 20 and pitching injury (Table 1). 41 While kinetic factors such as elbow valgus torque are difficult to measure, kinematic factors can be readily and inexpensively measured with video motion analysis and are more easily understood. These factors are changeable for injury prevention by pitchers and coaches (Table 2). As a result, numerous motion analysis studies have been conducted to identify kinematic correlates (such as elbow flexion angle) with kinetic factors (such as elbow valgus torque and humeral rotational torque) (Figure 2). The most frequently identified factors include knee flexion at front foot contact,2,15,32,37,47,48 trunk rotational timing (Figure 3),1,31 shoulder rotation,2,48 and elbow flexion at ball release.2,14,32,47,48
Quantitative kinematic factors from a variety of laboratories a
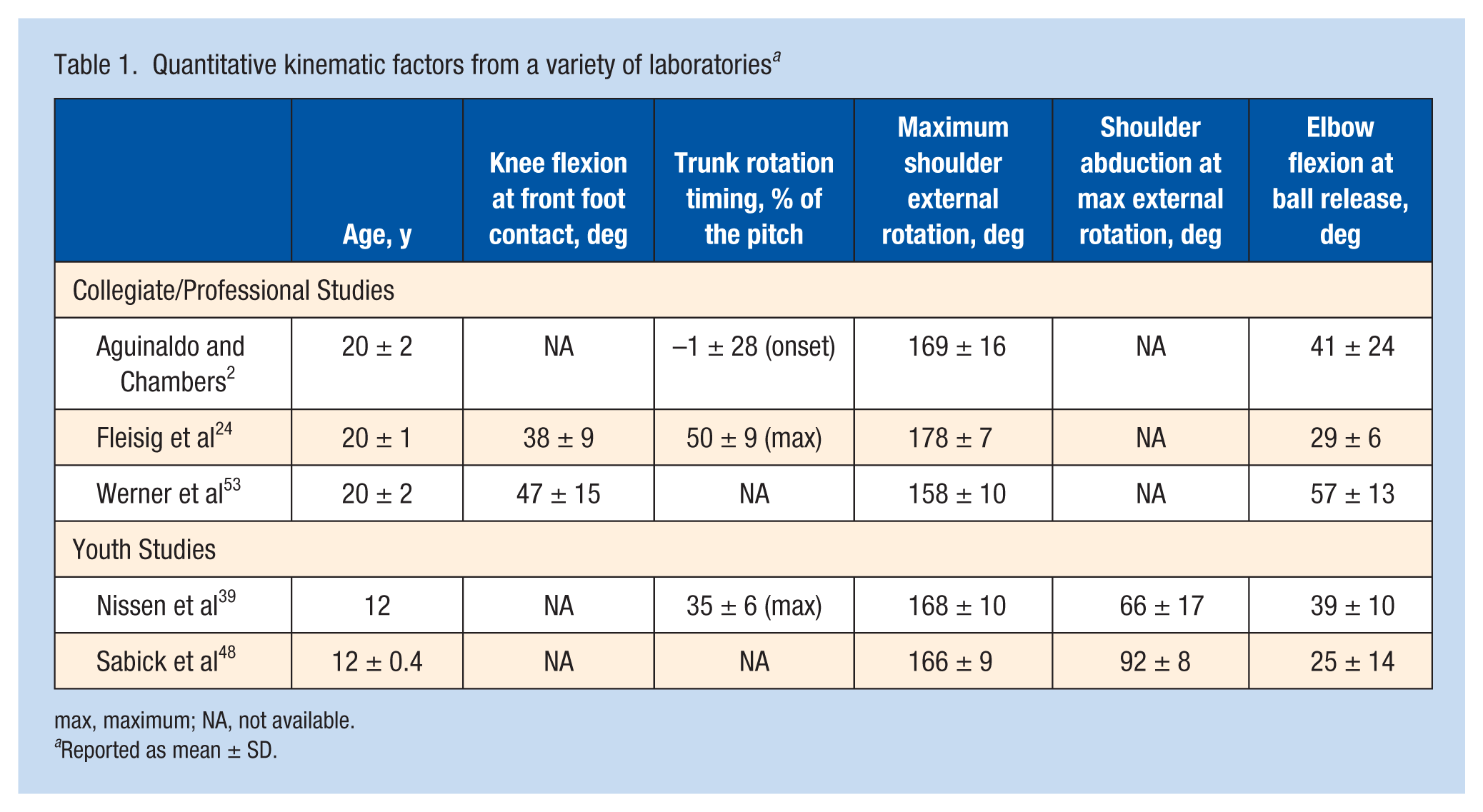
max, maximum; NA, not available.
Reported as mean ± SD.
Quantitative kinetic factors from a variety of laboratories a
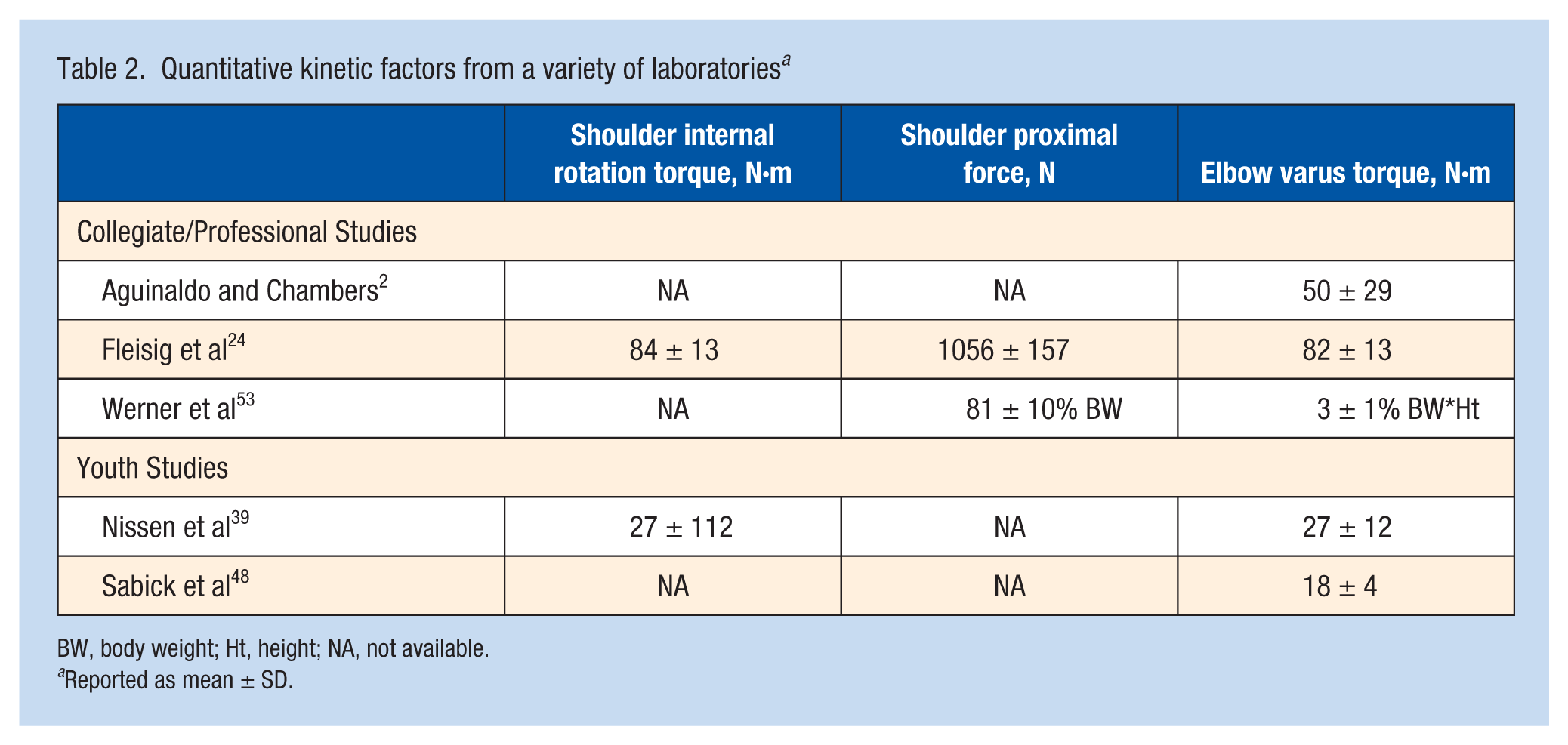
BW, body weight; Ht, height; NA, not available.
Reported as mean ± SD.
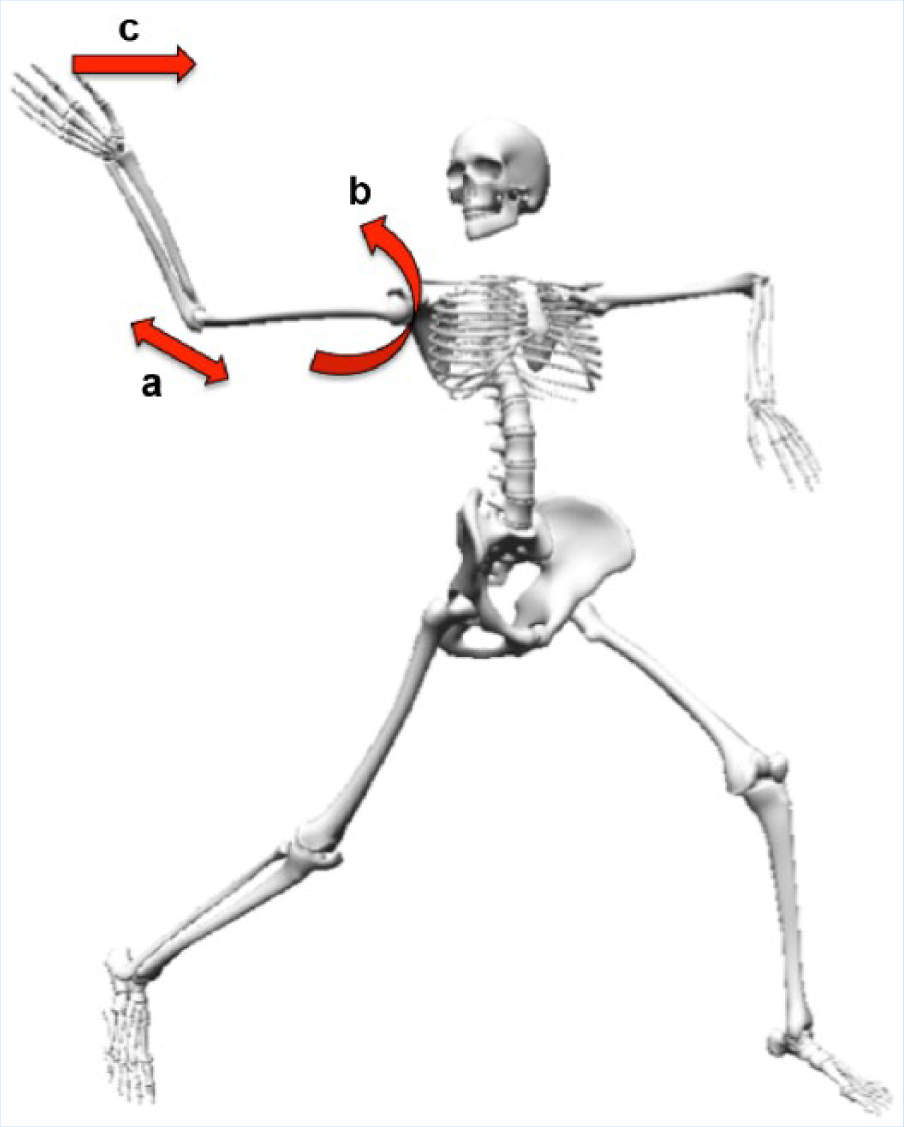
The 3 kinetic factors shown to correlate with injury: elbow valgus torque (a), shoulder external rotation torque (b), and pitch velocity (c).
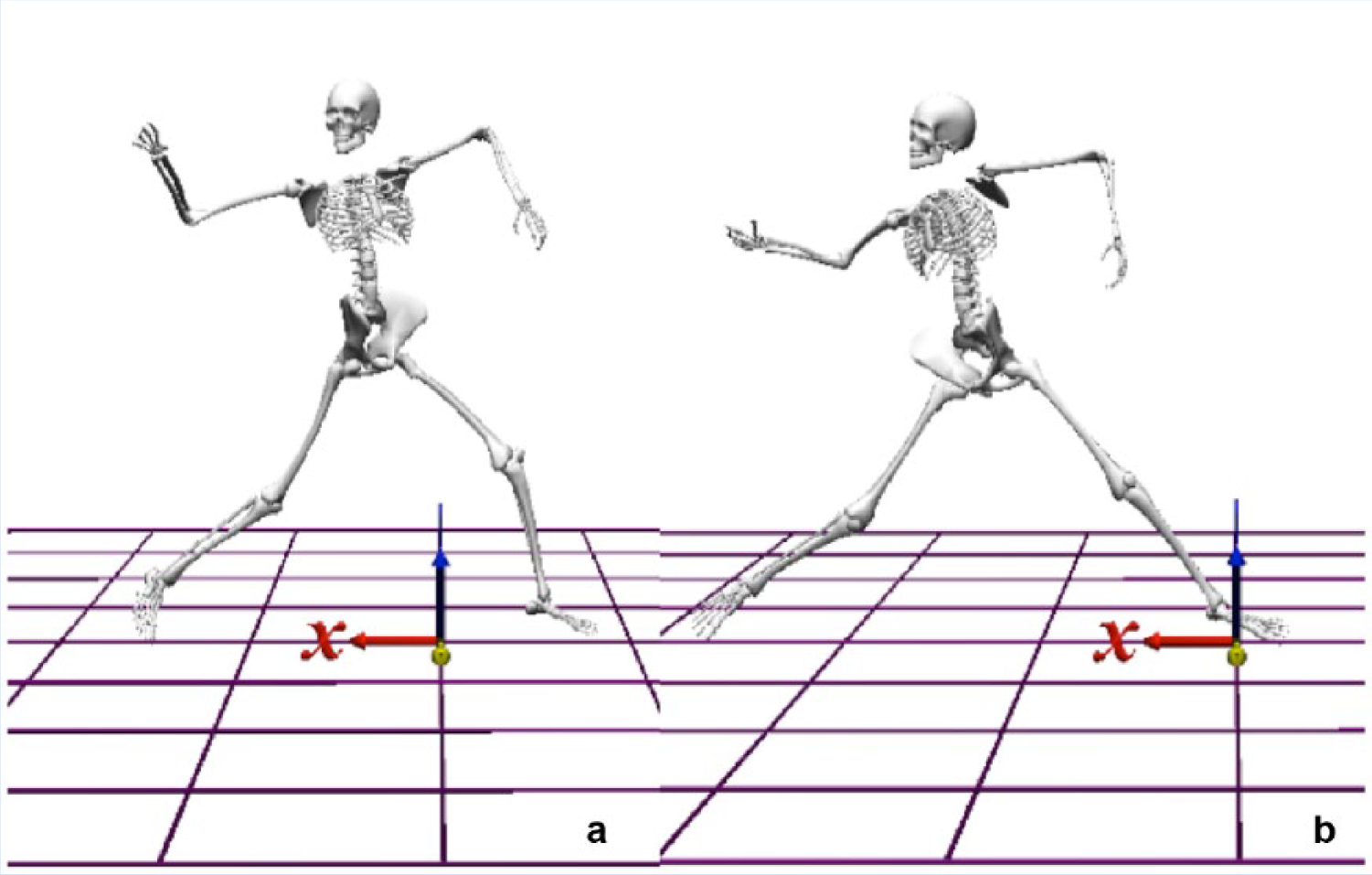
Two pitchers each at the moment of front foot contact. Marked differences can be seen in thoracic rotation, between (a) rotation 30° toward the pitchers and (b) rotation 45° toward second base. The axes for the environment are shown in red (x), blue (y), and yellow (z).
Within the lower extremity, knee flexion at front foot contact correlates with shoulder and elbow torques.15,37 This angle is consistent between subjects and may be an adaptive factor for continued high-velocity pitching in older pitchers.2,15,32,37,47,48 Knee flexion at front foot contact increased from 38.5° to 43.8° as pitchers aged from <20 years old to >27 years old. 15 Knee flexion at foot strike is critical to allow force transfer from the powerful stride up the kinetic chain. Alteration of knee flexion at ball release likely impacts pelvic, torso, and shoulder rotational timing, which likely propagates up the kinetic chain to translate into higher shoulder and elbow torques.2,15,32,37,47,48
Recent clinical studies suggest that trunk rotational timing may be linked to injury.1,31 In a comparison of normal controls, SLAP repairs had altered thoracic rotation. 11 Improper trunk rotational timing correlates with higher peak elbow valgus load 2 as well as higher shoulder proximal force and shoulder external rotational angle. 42 Desynchronization of trunk timing with stride and pelvic rotation may lead the peak of potential energy to pass through the shoulder and elbow.1,31 Desynchronization of rotational timing between the pelvis and the torso has been described by pitching coaches as “flying open at the shoulders” or lacking “hip and shoulder separation.” 12
While glenohumeral internal rotational deficit is a primary risk factor for injury, 6 loss of total rotational range of motion may be the critical injury factor. 54 The complementary side of glenohumeral internal rotational deficit is glenohumeral external rotation excess, which may be linked to increased elbow valgus load,2,48 SLAP tears, 5 and UCL tears. 25 Improving shoulder external rotation is a crucial target for rehabilitation after injury. 33
Elbow flexion angle at ball release correlates with shoulder and elbow kinetics and varies little between pitchers.2,14,32,47,48 Small changes can alter the lever arm between the forearm and the humerus. 2,14,32,47,48 Elbow flexion increases the length of the lever arm, the inertial moment of humeral rotation, and elbow valgus torques and strain on the UCL.2,14,32,47,48
From a holistic perspective, pitching velocity and fatigue are injury predictors. 8 Higher pitch velocity is the best predictive factor of UCL reconstruction in Major League Baseball pitchers. 9 Several prospective studies have also identified fatigue as a risk factor for injury.21,34,56 Based on these findings, USA Baseball, Little League America, and Major League Baseball have all developed age-based guidelines regarding rest and pitch counts (Table 3). These guidelines focus on proper pitch mechanics to reduce shoulder and elbow torque. 35 Pitch velocity correlates with pitching injury in youth pitchers. 10
Current Major League Baseball Pitch Smart recommendations 35
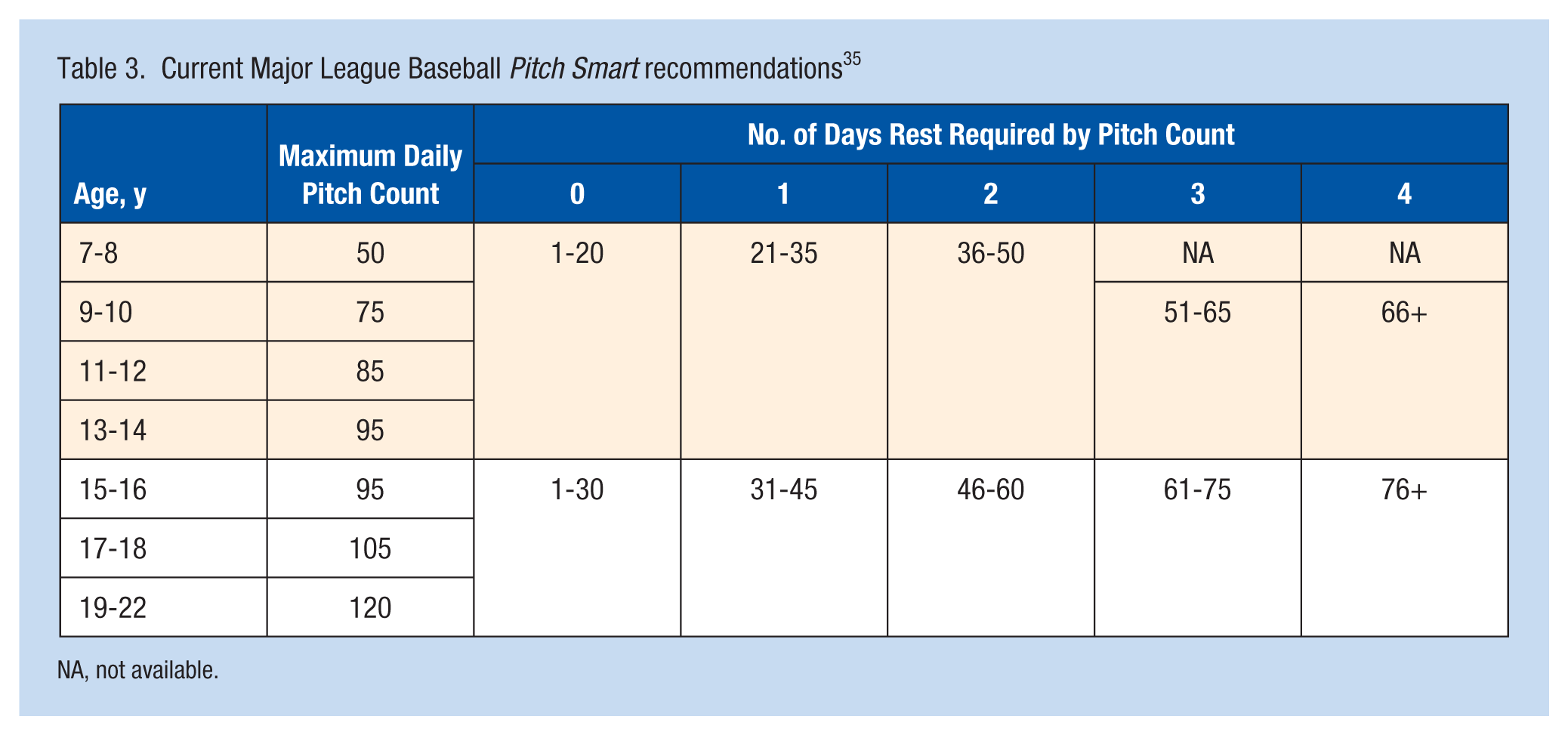
NA, not available.
One method to combine pitch velocity with motion analysis is to calculate “pitching efficiency.” 12 This concept was recently used in a qualitative motion analysis study of the pitching motion. Pitchers with proper hip and shoulder separation and the hand-on-top position demonstrated improved pitching efficiency. 12
In conclusion, several mechanical factors correlate with pitch injury: elbow valgus torque, knee flexion at front foot contact, pitcher fatigue, early thoracicc of the hips and shoulders, and decrease in shoulder rotational range of motion. These factors can decrease pitch velocity and produce pitcher fatigue, leading to injury.
Footnotes
The following authors declared potential conflicts of interest: Markus A. Wimmer, PhD, has grants/grants pending from Biomet, Ceramtec, and Zimmer. Nikhil N. Verma, MD, is a paid consultant for Smith and Nephew; receives royalties from Arthroscopy, Vindico, and Smith and Nephew; and has stock/stock options in Cymedica, Minivasive, and Omeros. Brian J. Cole, MD, MBA, is a paid consultant for Arthrex, Regentis, and Zimmer; receives royalties from Arthrex, DJ Orthopaedics, Elsevier, Saunders, and SLACK; and has stock/stock options in Carticept and Regentis. Anthony A. Romeo, MD, is a paid consultant for, and received payment for lectures from, Arthrex, and also receives royalties from Arthrex and Saunders.