
Abstract
Background:
Prior studies have examined muscle power via the countermovement jump (CMJ). Studies to date have examined neither the reliability nor the construct validity of the ballet first position CMJ (hips in lateral rotation, toes facing away from one another, legs straight) as a measure of power.
Hypotheses:
There would be (1) good interrater reliability in the visual assessment of the best-quality first position CMJ (κ ≥ 0.60), (2) good test-retest reliability in the height of the first position CMJ of good quality (intraclass correlation coefficient [ICC] ≥ 0.80), and (3) a significant relationship between isokinetic torque of the quadriceps femoris and first position CMJ height (r ≥ 0.40).
Study Design:
Correlational study.
Level of Evidence:
Level 3.
Methods:
A convenience sample of 39 healthy young adults who reported moderate activity levels participated in a warm-up and 2 sessions of 6 jumps. Quadriceps femoris isokinetic torque was measured in the first session.
Results:
Significant agreement was found within the same day for the best-quality first position CMJ (κ = 0.81), and in the highest, best-quality first position CMJ between days (ICC2,1 = 0.88). The highest, best-quality first position CMJ, when solving for a single trial, was comparable to the average of 2 trials (single trial: ICC2,1 = 0.96 vs average of 2 trials: ICC2,k = 0.98). There was a good relationship between quadriceps femoris isokinetic strength and first position CMJ height (Pearson r = 0.69 and P < 0.001 at 60 deg/s; r = 0.64 and P < 0.001 at 180 deg/s; r = 0.65 and P < 0.001 at 300 deg/s).
Conclusion:
Visual video movement analysis has good to excellent interrater agreement and test-retest reliability. Selecting the single highest jump of good quality is acceptable. The first position CMJ is a measure of power.
Clinical Relevance:
Video analysis of the single highest first position CMJ of good quality is an acceptable method of assessing movement quality.
Countermovement jump (CMJ) height has been measured using the Just Jump Mat System (JJ) (Probotics) as an indirect measure based on time between jump takeoff and jump landing. 7 The JJ is a valid measure of vertical jump height when compared with a 3-camera system, 3 with significant correlation between the JJ, the Vertec (Vertec), and the 3-camera system, 5 and has been used in previous studies to measure standard CMJs. 6 The standard CMJ is a jump typically performed by athletes in neutral bilateral hip, knee, and foot alignment. However, the reliability of the JJ cannot be generalized from procedures using standard CMJs to first position CMJs, also known as the first position sauté, a foundational jump in many dance genres. The first position CMJ is performed from 2 feet with hips in lateral rotation, toes facing away from one another, and legs straight. While Wyon et al 9 found a significant increase in first position CMJ height after whole-body vibration intervention among dancers, the researchers did not assess the reliability of the jump.
In studies of isokinetic strength, the standard CMJ has a significant relationship with isokinetic strength dynamometer protocols during knee extension at 120 deg/s and a moderate relationship at 180 deg/s. 2 Annino et al 1 found that isokinetic strength is related to functional CMJ height in ballet dancers, though the study was limited by the dancers performing the standard parallel CMJ and not the turned-out, first position CMJ.
The isokinetic strength protocol of the Biodex System 3 Dynamometer (BS3D) controls for speed at all angles of movement and can therefore be used to measure torque output. Strength is not speed dependent, but power is, so the measurement of torque with speed as a controlled variable is used to calculate power, with preset isokinetic protocols such as 60, 180, and 300 deg/s. Therefore, isokinetic strength, as measured by the BS3D, can be used to calculate power. Since CMJ is also considered a measure of power, 4 the correlation between the 2 measures serves as a means to assess construct validation.
No studies to date have examined the relationship between isokinetic strength and turned-out first position sauté CMJ (first position CMJ), nor have any studies to date examined interrater reliability of visual assessment of the highest, best quality first position CMJ or the test-retest reliability in the choice of the highest, best-quality first position CMJ. The research aims of this study were to (1) investigate the interrater reliability in the visual assessment of the highest, best quality first position CMJ, (2) determine the test-retest reliability in the height of the first position CMJ of good quality, and (3) establish the relationship between isokinetic strength of the quadriceps femoris and CMJ height. It was hypothesized that (1) the visual assessment of best quality for first position CMJ would have good interrater reliability (κ > 0.60), (2) the height of the first position good-quality CMJ would exhibit good test-retest reliability by an intraclass correlation coefficient (ICC) greater than 0.80, and (3) the measures of isokinetic torque (units) of the quadriceps muscle group and the height of the first position jump would be highly correlated (>0.40).
Methods
Participants
This study was approved by the Texas Woman’s University Institutional Review Board. The consent form and protocol were reviewed, and informed consent was given by each participant prior to testing.
The study included 39 healthy young adults (18 men, 21 women; age range, 21-32 years) recruited from the physical therapy classes at Texas Woman’s University. The following exclusion criteria were applied: presence of active cancer, current pregnancy, lower extremity fracture within the past year, surgery within the past year, strain or sprain within the past 3 months, metal plates in the body, history of migraines, or resting blood pressure >200 mm Hg systolic or >100 mm Hg diastolic. Participant demographics can be found in Table 1.
Participant a demographics
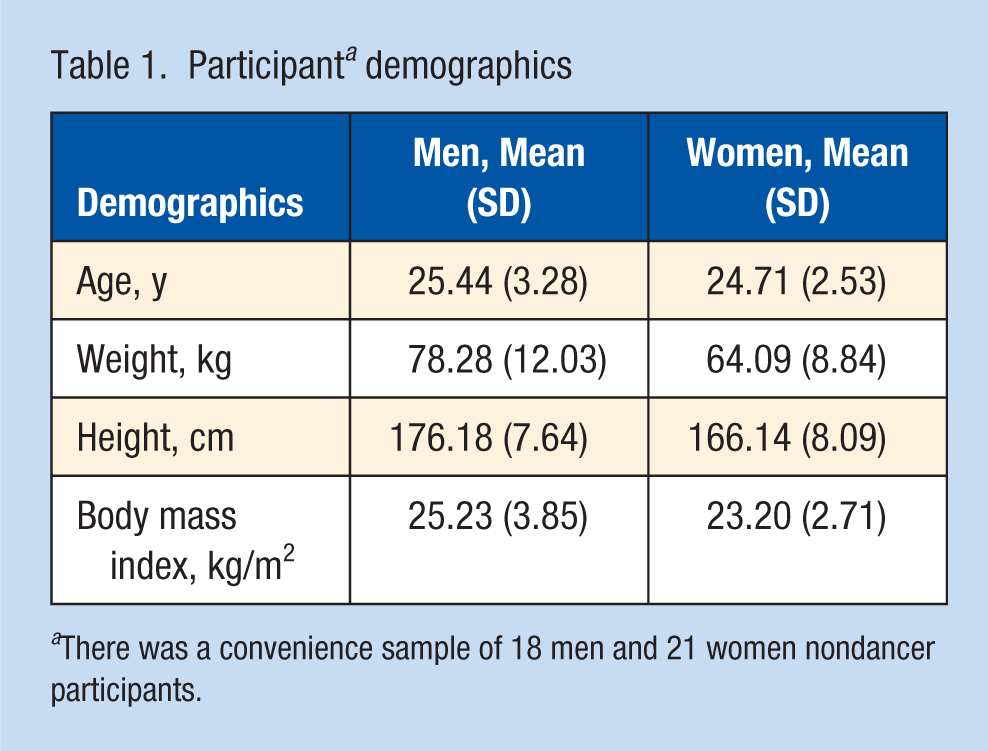
There was a convenience sample of 18 men and 21 women nondancer participants.
Procedure
The study had a correlational design. The following equipment was used: the JJ, a video camera, a Polar Heart Rate Monitor, a Monarch Cycle Ergometer, a blood pressure cuff, and the BS3D.
Each participant completed the International Physical Activity Questionnaire (Short Form–Past 7 Days) (IPAQ) 8 to verify moderate activity participation. The IPAQ moderate activity was established in meeting any of the following criteria: (1) 3 or more days of vigorous-intensity activity of at least 20 minutes per day, (2) 5 or more days of moderate-intensity activity and/or walking of at least 30 minutes per day, or (3) 5 or more days of any combination of walking, moderate-intensity, or vigorous-intensity activities achieving a minimum total physical activity of at least 600 metabolic equivalent of task minutes per week. Participants provided demographic information including sex, age, height, weight, and exclusion screening questions as listed above. Resting blood pressure was taken as a screen for participation.
Each participant warmed up for 5 minutes on the Monarch Cycle Ergometer at 40 to 60 rpm while maintaining a heart rate between 120 and 140 beats per minute. Participants then had 5 minutes of static and dynamic stretching guided by researchers for proper technique, similar to a previously reported protocol for dancers 9 as follows:
Standing with both feet parallel and balancing with hands on the wall, press over the ball of each foot (alternating feet, Figure 1), then rising up on both feet and bending the knees over a forced arch (Figure 2); repeat twice.
With heels together and feet turned out, bend the knees maximally, making sure to keep both heels on the ground with the inner knee aligned over the second metatarsal (Figure 3); complete 8 repetitions.
Stretching of the following muscles for 30 seconds each in standard stretching positions: gastrocnemius, soleus, hamstrings, and quadriceps, alternating sides; once each.

Foot press.

Forced arch.
First position plié warm-up.
After the warm-up, participants rested 5 minutes while watching a video of the primary researcher describing the desired jump technique and common errors. The participants performed 10 practice first position CMJs as follows: Participants stood on the JJ in bare feet with hands on the hips. Each participant was instructed to first straighten (Figure 4) and then bend knees quickly to maximum plié (a ballet semisquat with heels remaining on the floor and bilateral hips in end-range lateral rotation) (Figure 5) and jump as high a possible while straightening knees in the air and pointing the feet and toes downward (Figures 6 and 7). The participant lands first on the forefoot, then the midfoot, and then both feet into first position plié with the knees bent maximally, with both feet and inner knees laterally rotated and aligned over the second metatarsal and maintained. Participants were cued as above and provided technique correction by researchers.
First position pre–countermovement jump.
Plié transition into the first position countermovement jump.
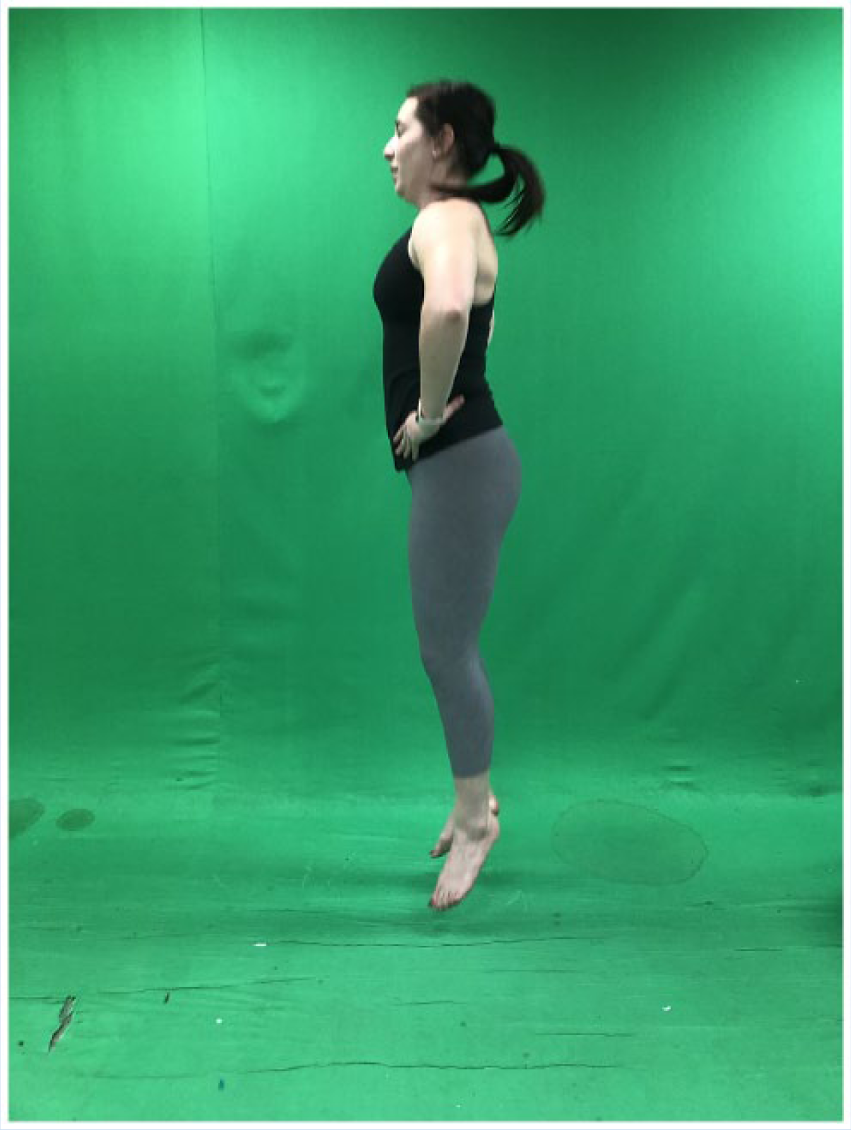
First position countermovement jump by a nondancer
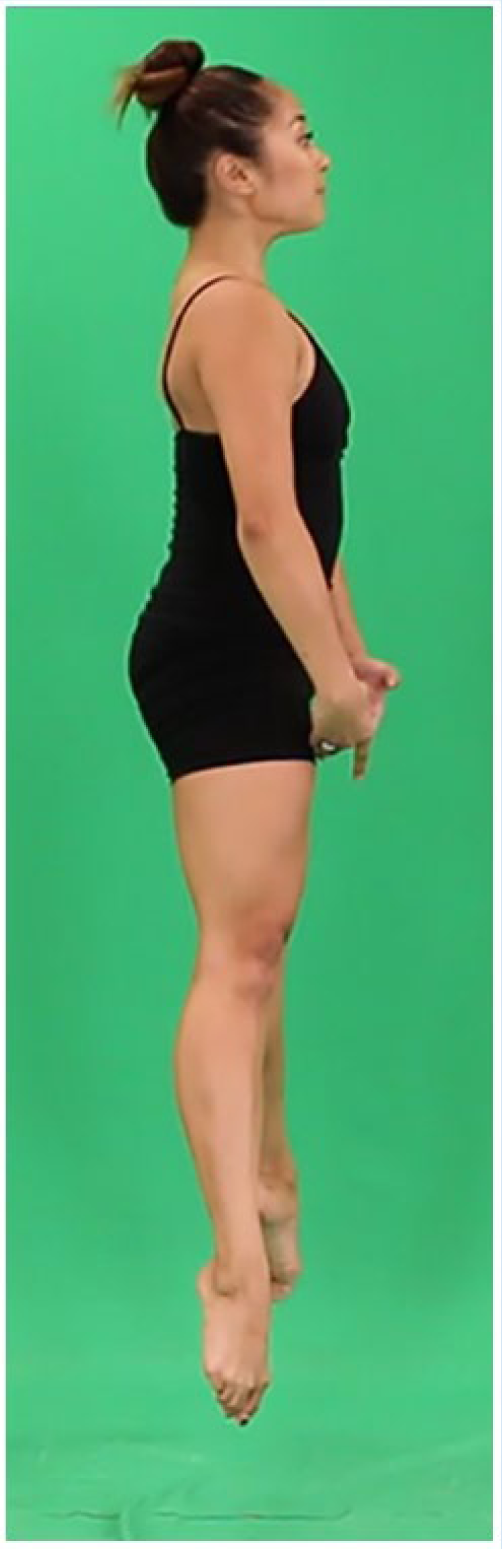
First position countermovement jump by a dancer.
After a 5-minute rest, participants performed 6 height-scored jumps for the same criteria, with at least a 15-second rest between jumps. Jumps were digitally recorded from the left side view. The height of each jump was recorded from the JJ output screen. Height was calculated from the time lapse between bilateral foot takeoff and landing contact on the mat, as
At a later time, using the videos, 2 testers independently chose the 3 best-quality jumps for each participant from the first session. Each of the 2 testers selected the jumps separately and without knowledge of the other’s selections. Testers had previously practiced this assessment, agreeing on jump quality as postural landmarks closest to midline in takeoff, flight, and landing as a baseline for judgment of quality movement. During the quality assessment, jump height was not considered.
Participants performed warm-up and jump protocol in 2 different sessions 7 to 14 days apart. In the first session, participants were given a 5-minute rest break after the warm-up and jump protocol. Then peak quadriceps femoris isokinetic torque (maximum anterior thigh muscle contraction ability) was measured for each individual on the BS3D. The isokinetic protocol was preset at 60, 180, and 300 deg/s. Participants performed 3 submaximal knee extension/flexion repetitions followed by 5 maximal repetitions at each speed with the dominant limb. The dominant limb was the limb with which the participant would kick a ball. In the second session, 7 to 14 days later, participants were finished with data collection after jump protocol and no isokinetic data were taken.
Data Analysis
Kappa statistic was established for interrater reliability for the first jump session based on the 3 jumps, selected as those of highest quality by each rater. First position CMJ height from all 6 trials was then reviewed to determine whether the highest first position CMJ was included in the first tester’s selected quality jumps. ICCs were calculated for average height of the 2 highest, good-quality first position CMJs on a single day, solving for a single high-quality jump. Day-to-day reliability of jump height for the highest, good-quality first position CMJ on each day was also determined. Pearson correlations were calculated to determine the relationship between quadriceps isokinetic strength and first position CMJ height, with alpha set at 0.05.
Results
Good to excellent interrater agreement was found between raters within the same day in judging the best-quality first position CMJ (κ = 0.81). For 13 participants, the highest first position CMJ was also 1 of the 3 best-quality first position CMJs, but for the remaining 26 participants, the highest first position CMJ was not of good quality. Good to excellent test-retest reliability was found for the highest, best-quality first position CMJs between days (ICC2,1 = 0.88). The results for the highest, best-quality first position CMJ when solving for a single trial was comparable with the average of 2 trials (single trial, ICC2,1 = 0.96; average of 2 trials, ICC2,k = 0.98). Both demonstrated excellent test-retest reliability. The standard error of measure at the 95% CI was 0.70 inches, and the minimal detectable change (MDC) was 1.93 inches based on highest, good-quality first position CMJ. See Table 2 for reliability results. There was a good relationship between isokinetic strength of the quadriceps femoris and first position CMJ height (Pearson r = 0.69 and P < 0.001 at 60 deg/s; r = 0.64 and P < 0.001 at 180 deg/s; r = 0.65 and P < 0.001 at 300 deg/s). See Table 3 for correlations between isokinetic strength measures and first position CMJ height.
Reliability results
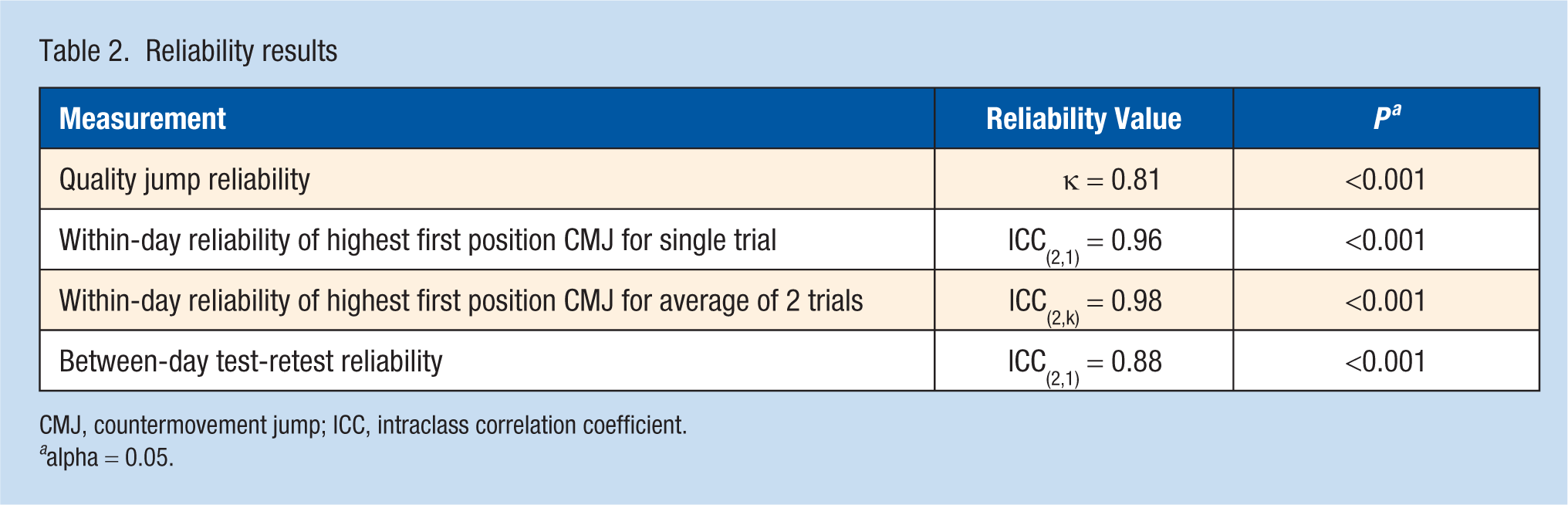
CMJ, countermovement jump; ICC, intraclass correlation coefficient.
alpha = 0.05.
Correlation between isokinetic power and first position countermovement jump height
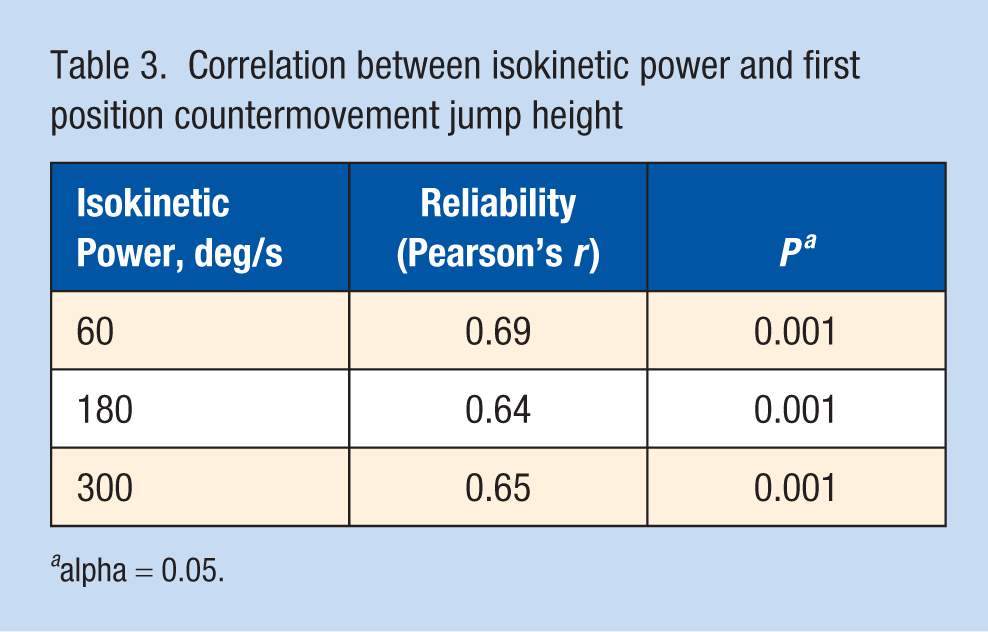
alpha = 0.05.
Discussion
The strong kappa value supports the ability of clinicians to judge the quality of first position CMJ and to assess movement, with quality defined as postural landmarks closest to midline in takeoff, flight, and landing. Because of the high test-retest reliability of quality jump height between sessions, it may not be necessary to take jump height measures over multiple sessions to obtain reliable data.
When performing first position CMJ measures, it is sufficient to have participants perform 3 trials of good quality in a single session and select the highest jump height of the 3 because correlations between the average of the highest 2 good-quality jumps and the single highest jump of good quality are almost equal. Since the calculated MDC was 1.93 inches, a clinically meaningful change in jump height in first position CMJ must be more than 1.93 inches. The results indicate that a majority of participants’ highest jumps were not of good quality; therefore, in an attempt to increase vertical jump height, quality is often sacrificed. Because there was a good correlation between isokinetic strength protocols using the BS3D and first position CMJ height on the JJ, construct validity of the first position CMJ as a measure of power is supported.
The importance of the first position CMJ in dance warrants the attention of the physical therapist assessing the first position CMJs in the clinic. It is not enough to measure a high jump. The dancer needs to perform the highest jump of good quality during testing, training, and performance. Because the JJ only assesses flight time, the form during jumping must be monitored by a clinician or there may be false representation of CMJ improvement.
Limitations to this study include the use of healthy, active adults, and not solely dancers, as well as the small number of participants. However, both men and women were tested, making the results generalizable to a larger subset of the population, including professional dancers, who are healthy, active adults. The results cannot be generalized to participants outside of the population of healthy, active adults. Another strength is finding an MDC for comparison of CMJ height differences in future studies.
The JJ is a portable and easily operable piece of equipment. In this study, the JJ is also seen to be a reliable tool to measure vertical jump height of a jump that is performed by most dancers and is thus a valuable clinical tool. In contrast to athletic jump height measures, the quality of jumps in dancers is important because quality is an important contribution to the esthetic of dance performance.
Footnotes
Acknowledgements
The authors would like to acknowledge Huynh Nguyen, DPT, and Elizabeth Lemos, DPT, for their contributions to this study.
The authors report no potential conflicts of interest in the development and publication of this article.