
Abstract
Background:
Balance assessment is used by clinicians as part of athlete concussion screening. The King-Devick (K-D) Balance app is designed to provide an objective balance assessment value. The purpose of this study was to investigate the responsiveness of a balance assessment using the K-D Balance app.
Hypothesis:
The K-D Balance app will demonstrate acceptable responsiveness for balance assessment.
Study Design:
Repeated-measures study.
Level of Evidence:
Level 5.
Methods:
A convenience sample of 25 participants between the ages of 20 and 25 years completed testing procedures. A battery of balance tests using the K-D Balance app on an iPhone were conducted 1 week apart. After a 5-minute warm-up, 3 stances were assessed: double leg, tandem right, and tandem left. The K-D Balance app guided the test positions and test times. A value representing movement was generated by the app algorithm. Analysis included descriptive statistics along with intraclass correlation coefficient and minimal detectable change (MDC).
Results:
The median score of the K-D test was 0.5 for session 1 and 0.4 for session 2. The ICC was 0.42 (95% CI, 0.04-0.70), and the MDC was 1.58.
Conclusion:
The MDC value of 1.58 represents the threshold of meaningful change in balance, as measured with the K-D Balance app.
Clinical Relevance:
Clinicians can use the results of this study to objectively assess changes in balance over time using the K-D Balance app.
Concussion can acutely impair static balance ability.2,5,6,9,10 The current consensus statement on concussion in sport recommends balance assessment as part of concussion management. 8 Studies support force platforms, motion capture systems, Microsoft Kinect sensors (Microsoft), Wii Balance Boards (Nintendo), and dynamic posturography as reliable means to obtain an objective assessment of balance.1,3,4,9,14 Unfortunately, the portability and financial investment of force platforms, motion capture systems, Wii Balance Boards, and dynamic posturography systems are limiting factors. Previous studies investigating the Balance Error Scoring System (BESS), a low-tech balance test, reported poor interrater reliability.1,3,13 There is a need for objective, easy-to-administer balance tests.
New mobile technology is being developed as an objective and portable means to measure balance. An iPad (Apple) positioned over the sacrum has been used to objectify data during the BESS test. 1 Data from the iPad were compared with a 3-dimensional motion capture system, and it was found that all kinematic outcomes were significantly correlated between the 2 devices. A new mobile alternative, the King-Devick (K-D) Balance application (app), was designed to provide an objective score of balance.
The responsiveness or ability of the measure to detect change in balance using the K-D Balance app (King-Devick Technologies Inc) has not been reported. Therefore, the purpose of this study was to investigate the responsiveness of the balance measurement screen using the K-D Balance app. Our hypothesis was that the K-D Balance app would demonstrate acceptable responsiveness for balance assessment. This information can aid clinicians in assessing acute balance impairments relative to baseline measurements and aid in assessing improvement over time after injury.
Methods
Participants
Based on an a priori power analysis, 22 or more participants would provide adequate power to detect a test-restest reliability coefficient of 0.80 or higher against a minimally acceptable coefficient of 0.50. A total of 25 healthy individuals (15 females, 10 males; mean age, 23 ± 1 years; mean height, 173.80 ± 10.21 cm; mean weight, 72.58 ± 12.29 kg; mean body mass index, 23.24 ± 2.8 kg/m2) participated. Inclusion criteria for participation included age between 20 and 25 years. Exclusion criteria included any diagnosed concussions within the past year, having greater than 1 diagnosed concussion in one’s medical history, or any medical restriction or injury limiting the ability to perform a balance screen. Participants provided written consent prior to their participation. The study was approved by the institutional review board at the authors’ institution.
Instrumentation
The K-D Balance app, an app available for Apple products, was used to provide an objective score of balance. The K-D Balance app measures triaxial coordinate data (pitch, yaw, and roll) via the internal accelerometer of the mobile device providing a quantitative measure of balance performance. The balance score is derived from a proprietary algorithm. Currently, the app is available for $5 per license.
Procedure
Participants performed a self-paced walk for 5 minutes as a warm-up, after which an iPhone with the downloaded app was secured to the midline of their chest with the K-D harness. Three stance positions were assessed in the following order: double leg (DL), tandem right (TR), and tandem left (TL) (Figure 1). In the DL stance position, participants stood with their feet together; in the TR position, the right heel was directly in front of the left toes; and in the TL position, the left heel was directly in front of the right toes. Participants performed the test barefoot on a firm surface. The K-D Balance app provided verbal and visual guidance through all positions and test times (see Figure 2 for app screenshots). Participants held each stance for 20 seconds with their eyes closed and hands on the hips. This test sequence was repeated 1 week later to establish test-retest reliability.
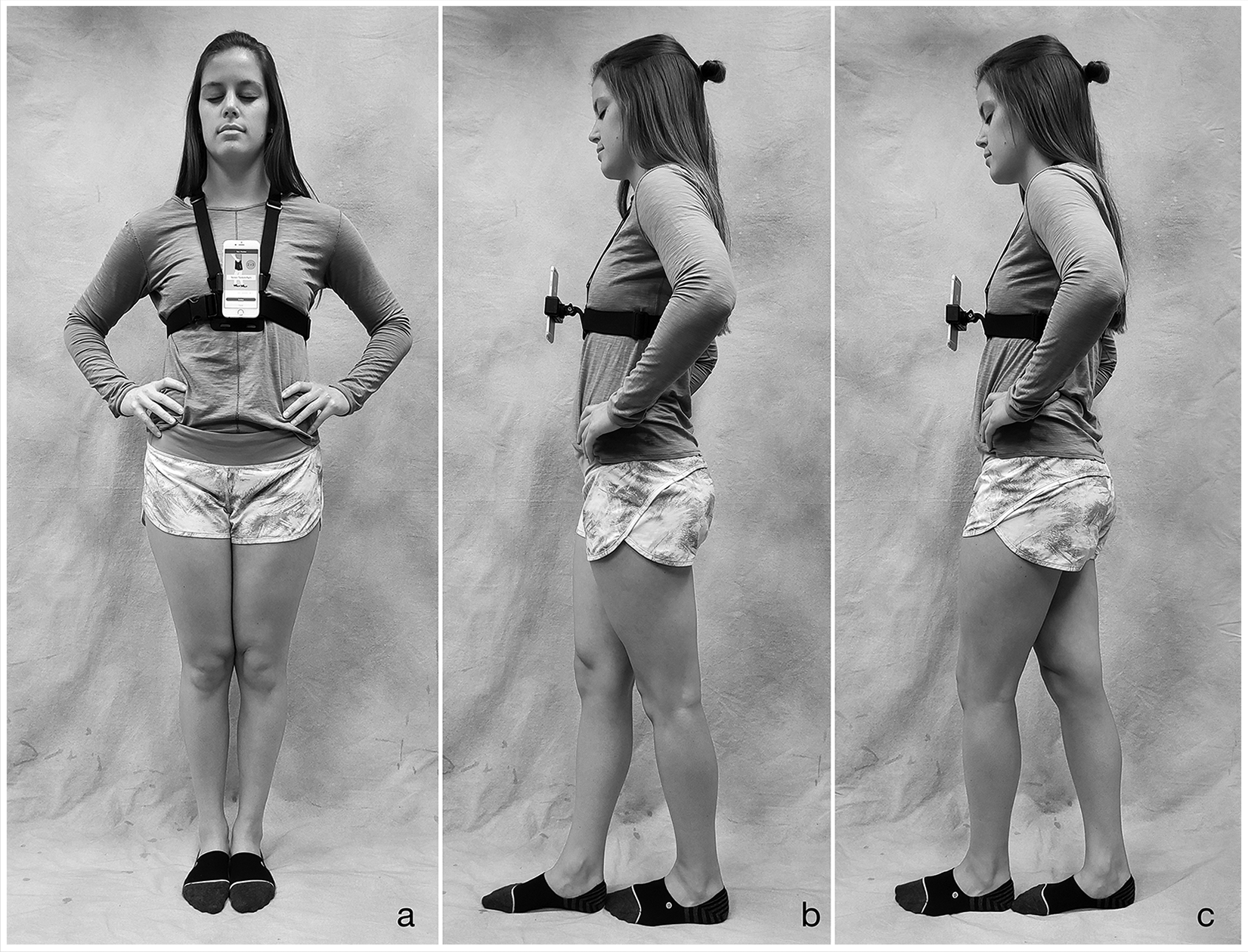
Three stance positions were assessed using the K-D Balance app: (a) double leg, (b) tandem right, and (c) tandem left. Participants held each stance for 20 seconds. K-D, King-Devick.

Screenshots of the K-D Balance application. K-D, King-Devick.
Data Analysis
This study was of repeated-measures design. Descriptive statistics were calculated along with the two-way mixed effect model intraclass correlation coefficient (ICC) to establish test-retest reliability of the measurements and minimal detectable change (MDC) calculations to establish the measure’s responsiveness. MDC at the 95% confidence level (MDC95) was calculated using the following equation:

In the equation, 1.96 represents the z-score at the 95% confidence level, and SD represents the standard deviation of the first measurement distributions.7,11 IBM SPSS Statistics Version 25 (IBM Corp) was utilized for statistical analysis.
Results
The median K-D total score for session 1 was 0.5, with an interquartile range (IQR) of 0.95. For session 2, the median score was 0.4, with an IQR of 1.0. ICC and MDC results are displayed in Table 1. Individual test results for both testing sessions are illustrated in Figure 3.
Intraclass correlation coefficients (ICCs) with 95% CIs, mean scores with SDs, and minimal detectable change (MDC) for the K-D total and 3 test positions
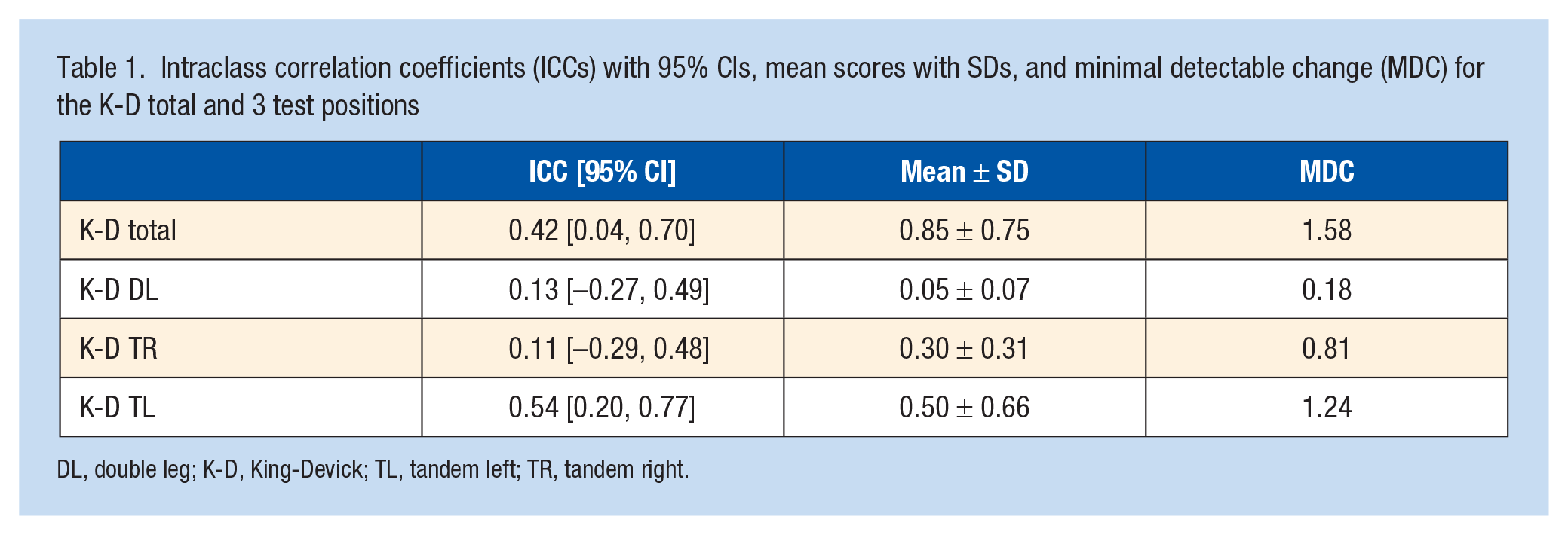
DL, double leg; K-D, King-Devick; TL, tandem left; TR, tandem right.
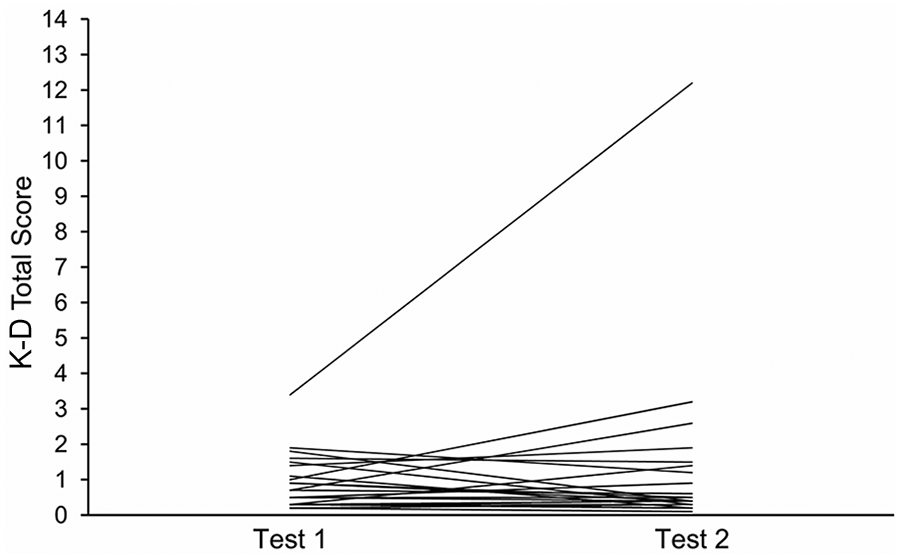
Individual performance scores for test session 1 and test session 2. K-D, King-Devick.
Discussion
The purpose of this study was to examine the responsiveness of a balance assessment using the K-D Balance app. The MDC value of 1.58 provides a reference for clinicians to evaluate whether change beyond measurement error has occurred and may help health care professionals more accurately determine when an athlete is able to return to play.
The reliability coefficients were rated based on the following values: 0.75 and greater, excellent reliability; 0.40 to 0.75, fair to good reliability; and less than 0.40, poor reliability.10,12 Based on this standard, the measurements of the K-D composite (ICC, 0.42) is fair to good. This lower-than-expected reliability may in part be attributed to the use of young, healthy, and active subjects with limited variability between participants. In addition, the testing procedures may not have provided an adequate challenge to postural stability. We used a firm surface consistent with the K-D Balance app protocol. Foam surfaces have been found to provide greater challenge to balance than firm surfaces.1,10 If an unstable surface was incorporated, the added challenge may have resulted in greater variability between participants and more favorable ICC values. Last, as illustrated in Figure 3, it did not appear there was a practice effect, as many participants performed poorer on the second test.
Use of mobile devices in the assessment of balance has been compared with more sophisticated systems. As an example, an iPad accelerometer and gyroscope was significantly correlated with a 3-dimensional motion capture system while completing a postural stability assessment. 1 This provides support for the ability of the iPhone/iPad internal components to function with the K-D app to provide a balance assessment tool that is valid as well as portable.
Our purpose was to determine responsiveness. We are not able to provide a cutoff score for what constitutes an abnormal test as we did not include participants with known balance impairments. Future studies could investigate K-D balance results in this population.
Major limitations include the composition of our participant pool. Participants in this small study were a homogeneous group of healthy participants without significant concussion history or balance impairment. Greater variability between participants may have resulted in a more favorable ICC value. Also, testing on a firm surface may not have provided adequate challenge to postural stability in this population.
Conclusion
The minimal detectable change of 1.58 represents a threshold to evaluate change over time in the K-D composite balance score.
Footnotes
The following authors declared potential conflicts of interest: D.A.K. is a consultant for DPT student capstone projects with the University of Montana. J.H.H. is a paid consultant for Winona State University and University of St Augustine.