
Abstract
Background:
To reduce the rate of anterior cruciate ligament (ACL) graft rupture, recent surgeries have involved anterolateral ligament reconstruction (ALLR). This reconstruction procedure harvests more knee flexor muscle tendons than isolated ACL reconstruction (ACLR), but its influence on knee muscle strength recovery remains unknown. This study aimed to assess the influence of ALLR with a gracilis graft on the strength of the knee extensor and flexor muscles at 6 months postoperatively.
Hypothesis:
The additional amount of knee flexor harvest for ALLR would result in impairment in knee flexor muscle strength at 6 months postoperatively.
Study Design:
Retrospective cohort study.
Level of Evidence:
Level 2.
Methods:
A total of 186 patients were assigned to 2 groups according to the type of surgery: ACL + ALLR (graft: semitendinosus + gracilis, n = 119) or isolated ACLR (graft: semitendinosus, n = 67). The strength of the knee extensor and flexor muscles was assessed using an isokinetic dynamometer at 90, 180, and 240 deg/s for concentric and 30 deg/s for eccentric contractions and compared between groups using analysis of variance statistical parametric mapping.
Results:
Regardless of the surgery and the muscle, the injured leg produced significantly less strength than the uninjured leg throughout knee flexion and extension from 30° to 90° for each angular velocity (30, 90, 180, and 240 deg/s). However, the knee muscle strength was similar between the ACL + ALLR and ACLR groups.
Conclusion:
The addition of ALLR using the gracilis tendon during ACLR does not alter the muscle recovery observed at 6 months postoperatively.
Clinical Relevance:
Although more knee flexor muscle tendons were harvested in ACL + ALLR, the postoperative strength recovery was similar to that of isolated ACLR.
Anterior cruciate ligament (ACL) ruptures account for more than 50% of knee injuries in pivoting, jumping and landing sports. 14 Close to 80% of these ACL ruptures require surgical reconstruction, 14 which is primarily designed to restore knee stability. Only 63% of nonprofessional athletes, however, returned to sport at their preinjury level, 3 and the rate of subsequent ACL injury in a high-risk population, ranging between 10% and 28%, remains high,39,40 suggesting that additional knowledge is required to improve clinical outcomes.
Among autograft reconstruction techniques, the bone-patellar tendon-bone procedure is considered the “gold standard” for ACL reconstruction (ACLR), 1 but it results in large graft-site morbidity with persistent postoperative anterior knee pain and quadriceps strength deficits.1,28 Alternative procedures based on semitendinosus tendon grafts have become more common because they minimize the occurrence of postoperative knee pain and functional deficits.6,28,41 Recent studies32,34 have highlighted that ACL ruptures are often associated with concomitant injuries of the anterolateral structures of the knee. As these structures play a key role in knee rotational stability,17,24 recent ACLR procedures have combined additional extra-articular tenodesis (EAT), such as anterolateral ligament reconstruction (ALLR). Concomitant ACL and ALLR (ACL + ALLR) decreases the rate of graft rupture when compared with isolated ACLR12,36 but requires an additional amount of gracilis tendon to be harvested rather than the semitendinosus tendon alone.32,34 Such additional harvesting may then impair knee function restoration, particularly the postoperative recovery of knee muscle strength.
This study aimed to evaluate the influence of additional EAT using gracilis tendon harvesting on knee muscle strength recovery at 6 months postoperatively. It was hypothesized that the muscular strength produced by the injured limb was lower in patients with combined ACL and ALLR than in patients with isolated ACLR, indicating a negative influence of EAT on muscular recovery.
Methods
Patients
The sample size N = 158 was estimated using G*Power software for effect size = 0.25 (medium effect), α = 0.05, and power = 0.95.
In this retrospective study, which was approved by the local ethical committee (MR 4016020520), 186 patients who consented to the use of their clinical data for scientific purposes were assigned to 2 groups: ACL + ALLR (n = 119) and isolated ACLR (n = 67). The inclusion criteria were as follows: male sex, aged from 18 to 40 years, regular participation (at least 3 times a week) in a sport activity at the time of ACL rupture, having undergone a first ACLR, having a contralateral knee without history of injury, and having performed 40 rehabilitation sessions supervised by a physiotherapist. Patients were excluded if the delay between ACL rupture and surgery was longer than 365 days or if ACL rupture was associated with concomitant additional ligament or meniscus injuries. Patients were included in the ACL + ALLR group if they underwent ACLR with ALLR. Briefly, the ACL was reconstructed with a graft composed of tripled semitendinosus tendon, while ALLR was performed with the gracilis tendon. 34 Patients were included in the isolated ACLR group if they underwent ACLR using only a graft composed of a tripled semitendinosus tendon without ALLR. 31 Reconstructions were performed by 3 different surgeons (S1/S2/S3) using similar surgical techniques.
Rehabilitation Protocol
The rehabilitation protocol, adapted from the one presented by Quelard et al 25 and Machado et al, 20 was similar for both groups. This protocol included 1 preoperative stage with quadriceps activation exercises and 3 postoperative stages. The first postoperative stage started immediately after the surgery, lasting 45 days, and focused on restoring full knee extension and resumed full support and normal gait on flat ground. This stage included cryotherapy, thigh muscle contractions during open and close kinetic chain exercises, passive range of motion exercises, and ambulation with crutches. The second stage (from the 45th to the 90th day postoperatively) included global close kinetic chain exercises and focused on muscle and balance control and the strengthening of the quadriceps and hamstring. The last stage of this protocol was a gradual return-to-sport activities varying from 4 months after surgery for no pivoting sports to 6 months after surgery for pivoting no-contact sports and 8 to 9 months after surgery for pivoting contact sports. Since patients lived in different cities that may have been far from the orthopaedic center, this protocol was communicated to the patient’s physical therapist, who supervised the rehabilitation program.
Procedure
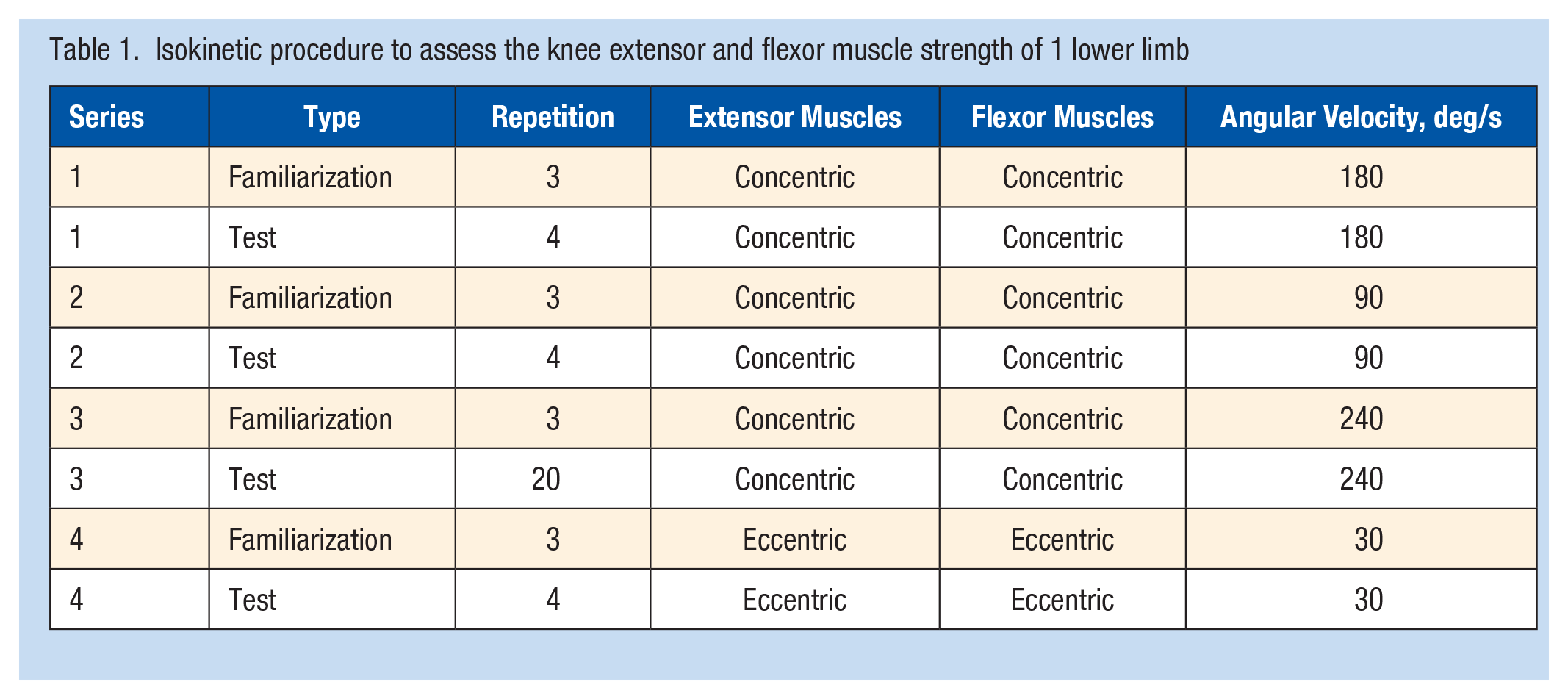
Six months (±20 days) after surgery, knee extensor and flexor muscle concentric and eccentric strengths were assessed on both sides using an isokinetic dynamometer (Contrex MJ; sampling rate 256 Hz; gravity correction). After a 6-minute warm-up on a stationary bicycle, the participant sat with a hip angle of 85°, the knee center of rotation aligned with the center of rotation of the isokinetic dynamometer, and the chest and contralateral thigh fixed by belts. From 0° to 118° (0° for knee fully extended) of knee flexion, the patient had to push and pull as hard as possible against a pad attached 3 cm above the lateral malleolus. Four angular velocities (90, 180, and 240 deg/s for concentric strength and 30 deg/s for eccentric strength) were used to assess the knee extensor and flexor muscle strength. Each series was composed of a familiarization repetition and a test repetition (Table 1). The recovery was fixed at 30 seconds between the familiarization and test repetitions and 1 minute between the test and familiarization repetitions. The uninjured knee was assessed first to ensure patient confidence when the operated knee was evaluated.
Isokinetic procedure to assess the knee extensor and flexor muscle strength of 1 lower limb
For each angular velocity and lower limb, the muscle torque curve containing the maximal value was retained. All torque values produced from 30° to 90° of knee flexion (Figures 1 and 2) were kept for statistical analysis, since this range of motion corresponded to the effective constant velocity, 26 and were normalized by the participant’s body mass. The functional ratio (Figure 2), namely, the ratio between knee flexor muscle eccentric torque at 30 deg/s and knee extensor muscle concentric torque at 240 deg/s, was also calculated at each degree from 30° to 90° of knee flexion and used for further analysis.
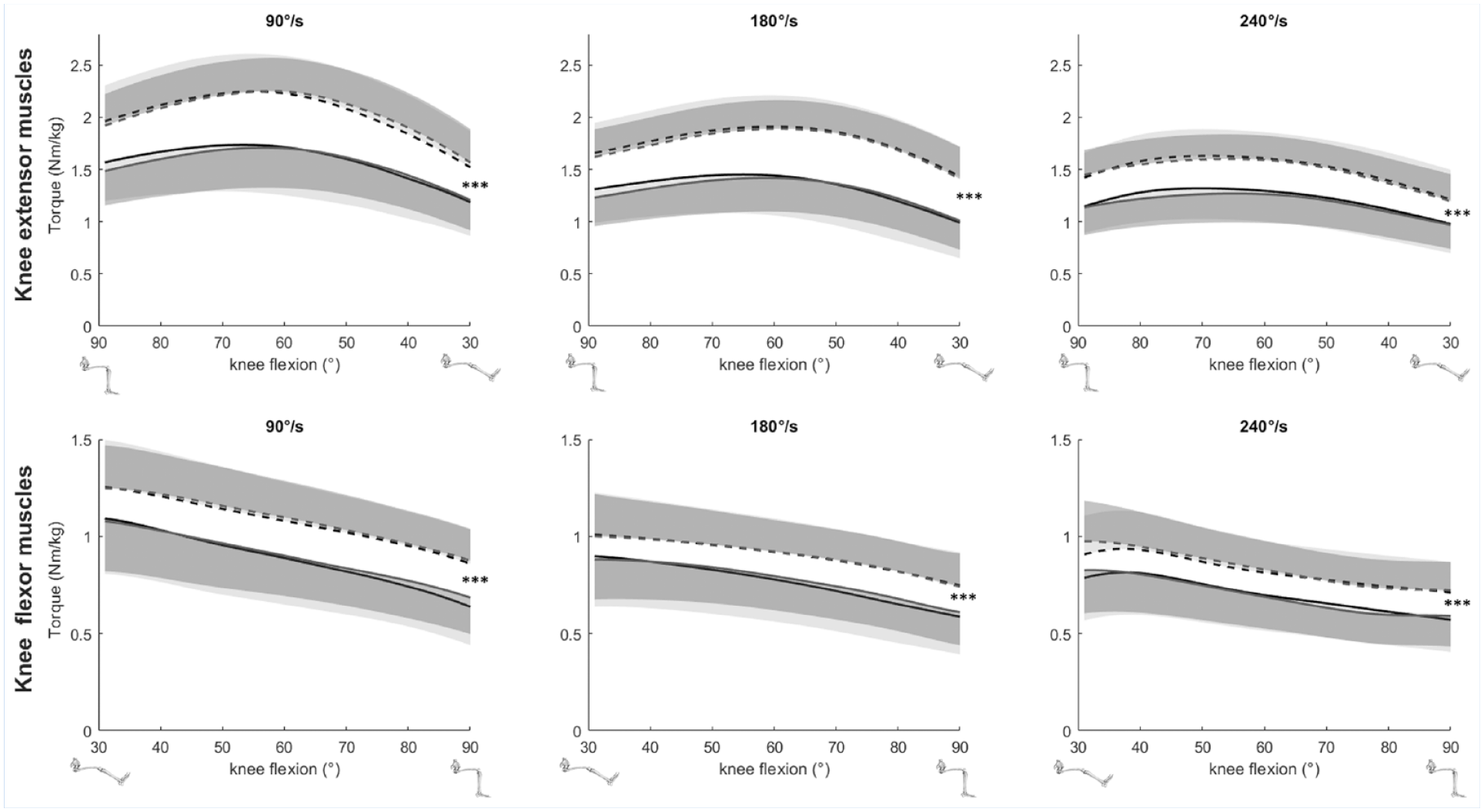
Mean and standard deviation of the concentric torques of the knee extensor and flexor muscles assessed at 90 deg/s (left), 180 deg/s (middle), and 240 deg/s (right) with respect to knee flexion angles in patients with combined anterior cruciate ligament and anterolateral ligament reconstruction (in black) and patients with isolated anterior cruciate ligament reconstruction (in gray). The dotted lines denote the uninjured side, and the solid line denotes the injured side. ***indicates a significant difference between the 2 sides from 30° to 90° with P < 0.001.
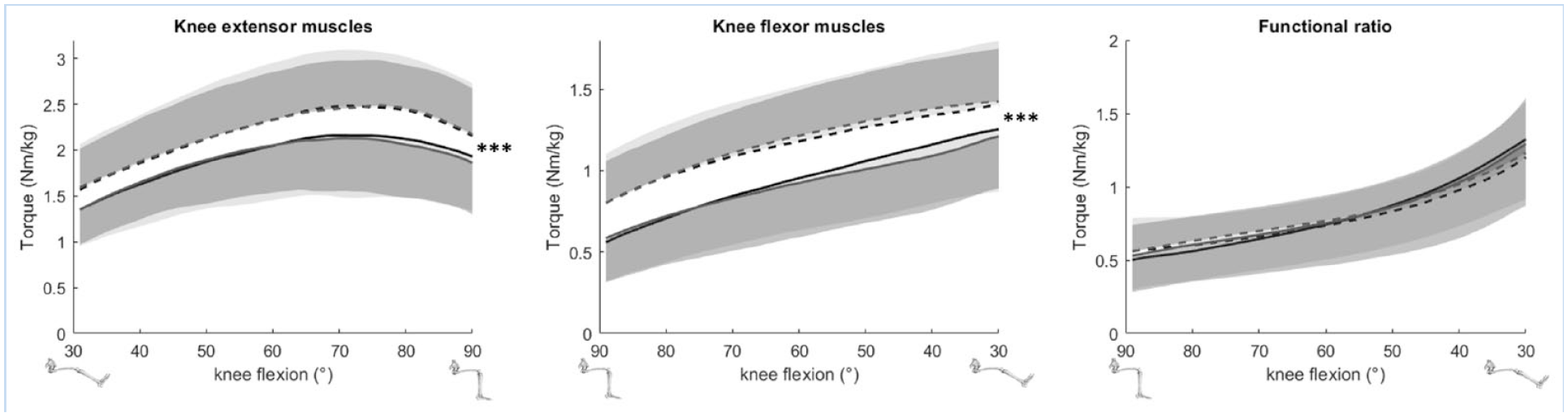
Mean and standard deviation of the eccentric torques (left and middle) of the knee extensor and flexor muscles assessed at 30 deg/s and the functional ratio (knee flexor muscles eccentric at 30 deg/s divided by knee extensor muscles concentric at 240 deg/s; right) with respect to knee flexion angles in patients with combined anterior cruciate ligament and anterolateral ligament reconstruction (in black) and patients with isolated anterior cruciate ligament reconstruction (in gray). The dotted lines denote the uninjured side, and the solid line denotes the injured side. ***indicates a significant difference between the 2 sides from 30° to 90° with P < 0.001.
Statistical Analysis
Student t tests for independent samples were first used to compare quantitative demographic (age and mass) and surgery (rupture-surgery delay and surgery-test delay) measures between the ACL + ALLR and ACLR groups, while Pearson chi-square tests were applied to qualitative demographic (surgeons and sports activities) measures. These statistical tests were performed using SPSS 11.0 software (IBM Corp), and the level of significance was fixed at P ≤ 0.05.
In line with Rogowski et al, 26 statistical parametric mapping (SPM) tools were used to explore all torque values produced by the knee muscles throughout knee flexion and extension from 30° to 90°. Analyses of variance SPM{F} with 1 intersubject factor (group: ACL + ALLR vs ACLR) and 1 intrasubject factor (laterality: injured vs uninjured) were performed independently on the knee flexor and extensor muscle torques for each angular velocity and on the ratio between the knee flexor muscle eccentric torque at 30 deg/s and the knee extensor muscle concentric torque at 240 deg/s (functional ration). The SPM analysis was conducted using the open-source toolbox SPM-1D (Todd Pataky, 2014, Version M0.1) in MATLAB 2018b. For analysis of variance (ANOVA) SPM{F}, due to multiple comparisons, Bonferroni’s correction was applied, and the level of significance was set at P ≤ 0.006.
Results
For the demographic and surgery characteristics, Student t tests revealed no differences between the ACL + ALLR and ACLR groups (Table 2). Pearson chi-square tests also showed no difference in the sport activity distribution (ie, soccer, rugby, ski, basketball, handball, others) at the time of ACL rupture, but there was a significant difference in the distribution of the ACLRs performed by surgeons (P = 0.005). One surgeon (S3) performed more ACL + ALLR than isolated ACLR than the other surgeons (S1 and S2).
Mean (± standard deviation, and range in brackets) demographic and surgery characteristics for the groups of patients with combined anterior cruciate ligament and anterolateral ligament reconstruction (ACL + ALLR) and with isolated anterior cruciate ligament reconstruction (ACLR)
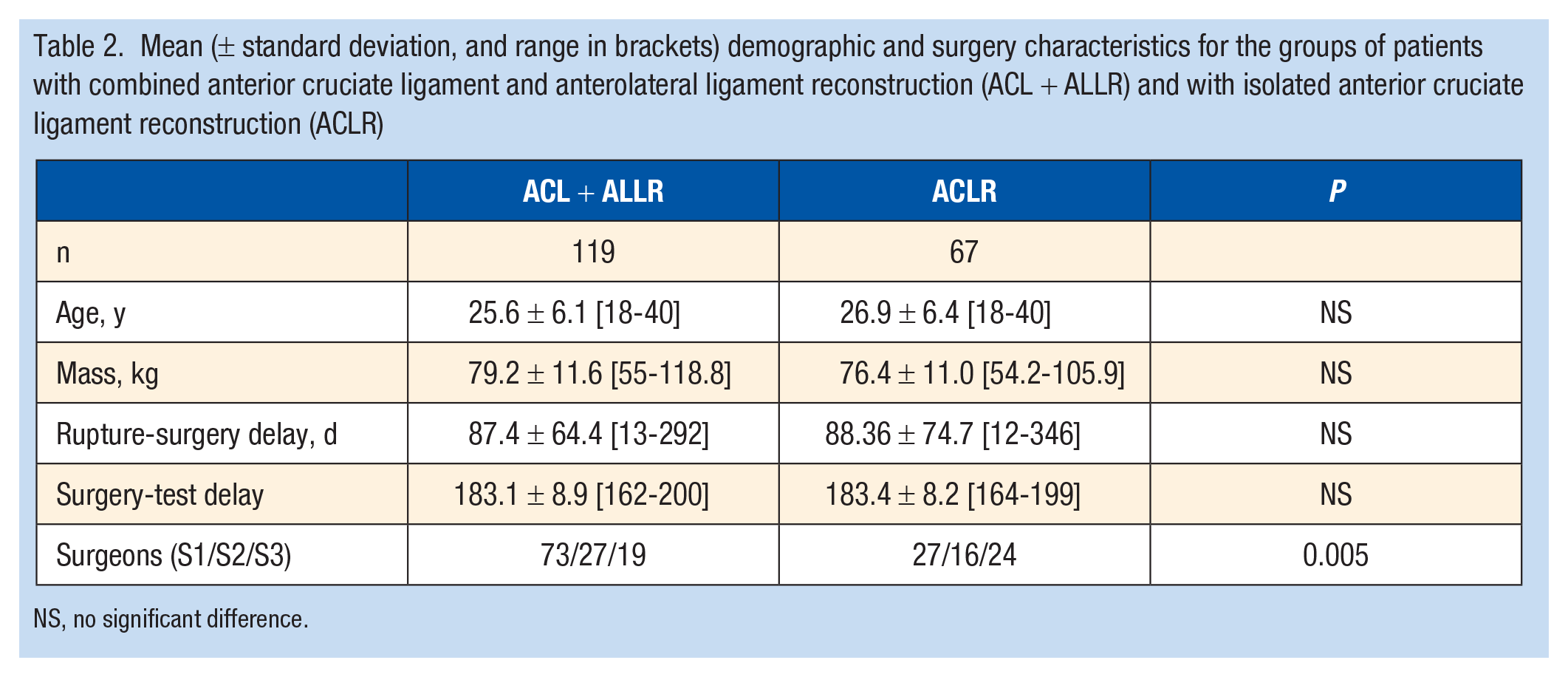
NS, no significant difference.
Regarding the concentric and eccentric torques of the knee extensor and flexor muscles, the ANOVA SPM{F} showed neither an interaction nor a group effect. A significant laterality effect was found at each angular velocity for both the knee extensor and flexor muscles (P < 0.001 for all angular velocities) (Figures 1 and 2). For both groups and muscles, all torques produced at each degree from 30° to 90° of knee flexion by the injured limb were lower than those produced by the uninjured limb. The percentage of decrease between the injured and uninjured lower limbs ranged between 5% and 30% for the knee extensor muscles and between 6% and 26% for the knee flexor muscles for all angular velocities throughout knee flexion and extension from 30° to 90° (see Appendix 1, available in the online version of this article, for the mean range of percentage strength decrease at each velocity). Furthermore, no significant interaction, group or laterality effect was highlighted on the functional ratio (Figure 2).
Discussion
This study aimed to assess the influence of the additional EAT using a gracilis tendon harvesting on the knee muscle strength recovery at 6 months postoperatively. The main findings were that the knee muscle isokinetic strength at 6 months after ACLR was similar between patients with combined ACL + ALLR using semitendinosus and gracilis and patients with isolated ACLR using semitendinosus alone. Using the gracilis tendon in EAT may not therefore negatively influence muscular strength recovery at 6 months.
Since isokinetic testing allows the strength production of a muscular group to be assessed during concentric and eccentric contractions at different angular velocities, it takes a large place to monitor the strength recovery in the knee extensor and flexor muscles after ACLR.1,21,37 After isolated ACLR or ACL + ALLR, torques produced by the uninjured lower limb flexor and extensor muscles throughout knee flexion or extension (from 30° to 90°) were equivalent regardless of the type of contraction and angular velocity. They were in the range reported for healthy athletes during a concentric contraction at velocities between 240 and 60 deg/s, namely, peak torques ranging from 1.7 to 3.5 N·m/kg for the knee extensor muscles and 1.05 to 1.9 N·m/kg for the knee flexor muscles.7,8,18 We then considered that the uninjured lower limb of our participants may be used as a reference to highlight the postoperative consequences of ACLR. In addition, confounding factors have been limited since no difference was found in demographic or surgery characteristics. Hence, the potential difference in strength between patients with isolated ACLR and those with ACL + ALLR may be due to the reconstruction type.
Six months after isolated ACLR with a semitendinosus graft, the injured lower limb produces concentric peak torques ranging from 1.2 to 1.88 N·m/kg for the knee extensor and from 0.7 to 1.52 N·m/kg for knee flexor during knee flexion/extension at 60 to 180 deg/s.1,2,23 Compared with the uninjured limb, strength deficits of 10% to 30% in knee flexor and extensor muscles in the injured limb are reported.1,2,11,23 Throughout knee flexion and extension for both types of contractions and for each angular velocity, the magnitude of the deficits observed after such surgery was in this range. Although the strength deficit is usually resolved in 12 to 18 months1,23 with tendon regeneration, 22 in high-risk populations, such as pivoting and contact sport players, the graft rupture rate remains high39,40 because of insufficient recovery in knee rotation stability.33,34 To reduce this rate of failure as well as to improve the return to sport, EAT is now proposed to be added to ALCR.10,27,35,36 Two types of EAT are currently promoted: the historical modified Lemaire using a strip of iliotibial band and the more recent ALLR, mostly performed with the gracilis tendon. 33 Using a gracilis tendon for EAT is a major concern because a larger amount of knee flexor muscle tendon is harvested (semitendinosus and gracilis vs semitendinosus). Hence, the influence of harvesting gracilis has been well documented, and a knee flexor muscle strength deficit in deep knee flexion (>90°) is commonly reported.11,30,38 Most of these studies9,10 investigated isolated ACLR using a semitendinosus and gracilis graft and to the best of our knowledge, few studies11,30,38 have focused on knee muscle strength recovery after ACL + ALLR. Six months after such surgery, a knee muscle strength deficit between the injured and uninjured limb ranging from 18% to 26% is observed in the isokinetic peak value recorded at 90 deg/s. 9 Throughout knee flexion and extension from 30° to 90°, deficits observed after ACL + ALLR were in this range for each type of contraction and at each angular velocity. This magnitude of strength deficit was also similar to those reported for isolated ACLR.1,2,11,23 However, it remained higher than the 10% expected to return to play, 13 which would be reached close to 12 months postoperatively.1,9,23 Getgood et al 9 also reveal a greater bilateral deficit at 6 months postoperatively, which is resolved during the subsequent month, for knee flexor and extensor muscle strength peak values of concentric contractions recorded at 90 deg/s in patients undergoing ACL + ALLR compared with those undergoing isolated ACLR. 9 In our study, regardless of the type of contraction and angular velocity, the knee extensor and flexor muscle strengths were compared throughout knee flexion and extension (and not only the peak value) and were similar between both reconstructions. Therefore, we can consider that additional ALLR confers better knee stability12,33 without alteration of muscle strength recovery compared with isolated ACLR.
Knee extensor (quadriceps) and flexor (semitendinosus, semimembranosus and gracilis) muscles ensure dynamic joint stability.15,19 This function is commonly assessed by calculating the functional ratio (flexor eccentric strength/extensor concentric strength) since it is thought to mimic muscular involvement during sport activities.1,13,29 During knee extension (from 90° to 0° of knee flexion), this functional ratio increases from 0.48 to 1.30 in an uninjured population.5,16 Throughout knee extension, our patients’ ratio increased in this range for both sides, regardless of the type of surgery. Such ratio values indicate that the knee flexor muscles are able to counteract the action of the knee extensor muscles near full knee extension. 5 Interestingly, the ratio was similar between the 2 sides and the types of surgery throughout knee extension (from 30° to 90°). Although ACLR combined with ALLR requires harvesting more knee flexor muscle tendons than isolated ACLR, this surgery may thus result in no alteration in the recovery of dynamic knee stability.
This study has significant limitations warranting discussion. A first limitation consists of the retrospective nature of the study. Although exclusion and inclusion criteria were set to ensure homogeneous groups, some differences may remain. In particular, although the same rehabilitation program was recommended for all the patients, the procedure was supervised by different physical therapists with various levels of experience. This procedure is, however, commonly used after ACLR.20,25 The knee muscle strength deficits observed in our study were similar to those described 6 months postoperatively,1,2,11,23 suggesting that this deficit may not be due to the rehabilitation program. A second limitation lies in the absence of a preoperative strength evaluation or control group with healthy participants to more precisely assess the postoperative strength recovery, but the return-to-play decision is usually assessed by comparing the injured with the uninjured side.1,13 Finally, although the standing position is more representative of muscle solicitation during sports activities, the sitting position3,7,8,18 was preferred for isokinetic assessment to avoid compensatory mechanisms. This study, however, was 1 of the first to assess the strength of the knee extensor and flexor muscles 6 months after combined ALLR and ACLR. Although this surgery harvested more knee flexor muscle tendons than isolated ACLR, the strength recovery may be similar for these 2 methods at 6 months postoperatively. Future studies should include functional tests as proposed by Blakeney et al 4 to confirm the efficiency of this surgery.
Conclusion
The addition of ALLR using the gracilis tendon during ACLR does not alter the muscle recovery observed at 6 months postoperatively when compared with ACLR using the semitendinous tendon alone. Nevertheless, muscular recovery is not complete, which raises questions regarding the risk of iterative ruptures when resuming sports.
Supplemental Material
sj-docx-1-sph-10.1177_19417381211005405 – Supplemental material for Isokinetic Strength After ACL Reconstruction: Influence of Concomitant Anterolateral Ligament Reconstruction
Supplemental material, sj-docx-1-sph-10.1177_19417381211005405 for Isokinetic Strength After ACL Reconstruction: Influence of Concomitant Anterolateral Ligament Reconstruction by Benoit Gillet, Yoann Blache, Isabelle Rogowski, Grégory Vigne, Bertrand Sonnery-Cottet, Jean-Marie Fayard and Mathieu Thaunat in Sports Health: A Multidisciplinary Approach
Footnotes
The following authors declared potential conflicts of interest: Y.B. received fees from Ramsey Santé. B.S.-C. and M.T. are paid consultants for Arthrex. B.S.-C. received royalties from Arthrex. J.-M.F. is a paid consultant for Arthrex and NewClip Technics. J.-M.F. received royalties from XNov and NewClip Technics.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.