
Abstract
Context:
Return-to-play (RTP) outcomes in elite athletes after cervical spine surgery are currently unknown.
Objective:
To systematically review RTP outcomes in elite athletes after anterior cervical discectomy and fusion (ACDF), cervical disc replacement (CDR), or posterior foraminotomy (PF) surgery.
Data Sources:
EMBASE, PubMed, Cochrane, and Medline databases from inception until April 2020. Keywords included elite athletes, return to play, ACDF, foraminotomy, and cervical disc replacement.
Study Selection:
Eligible studies included those that reported RTP outcomes in elite athletes after cervical spine surgery.
Study Design:
Systematic review.
Level of Evidence:
Level 4.
Data Extraction:
Data were extracted by 2 independent reviewers.
Results:
The primary outcomes of interest were rates and timing of RTP. Secondary outcomes included performance on RTP. A total of 1720 studies were initially screened. After inclusion criteria were applied, 13 studies with a total of 349 patients were included. A total of 262 (75%) played football, 37 (11%) played baseball, 19 (5%) played rugby, 10 (3%) played basketball, 10 (3%) played hockey, 9 (3%) were wresters, and 2 (1%) played soccer. ACDF was reported in 13 studies, PF in 3 studies, and CDR in 2 studies. The majority of studies suggest that RTP after surgical management is safe in elite athletes who are asymptomatic after their procedure and may lead to higher rates and earlier times of RTP. There is limited evidence regarding RTP or outcomes after CDR or multilevel surgery.
Conclusion:
The management and RTP in elite athletes after cervical spine injury is a highly complex and multifactorial topic. The overall evidence in this review suggests that RTP in asymptomatic athletes after both ACDF and PF is safe, and there is little evidence for decreased performance postoperatively. Surgical management results in a higher RTP rate compared with athletes managed conservatively.
Age-related degeneration of the cervical spine is common, with up to 85% of the asymptomatic general population older than 60 years demonstrating evidence of spondylosis on advanced imaging studies.22,34 When providing care for athletes, and in particular, elite athletes who participate in contact sports, it is critical to understand that cervical disease is much more prevalent than would be expected for age-matched controls. This has been demonstrated in studies of American elite football players, which showed significantly higher rates of cervical radiographic changes than the general population.2,12 Similar results and degenerative imaging changes have also been shown in professional rugby players. 30 Importantly, many of these degenerative changes were identified in athletes who reported no history of previous significant pain or injury to the neck, 2 highlighting the need for a high index of suspicion when caring for these athletes, due to possible occult underlying disease and risk for future injury. Early cervical degenerative changes and stenosis in athletes is thought to be a risk factor for radiculopathy, myelopathy, and even significant spinal cord injury (SCI). 34 Advanced degeneration of the cervical spine in contact athletes is multifactorial in nature but has been attributed in part to the repetitive microtrauma to the cervical region athletes may experience throughout their careers. Repeated trauma leads to both decreased vascularity as well as microfractures and compression of the bony elements over time.5,14 The body’s ultimate response to these repetitive insults is sclerosis and degeneration. 5
In addition to degenerative changes, the more feared and potentially catastrophic consequence of athletic participation is the possibility of acute cervical spine injury and/or SCI. Involvement in contact sports such as American football, wrestling, and basketball in the United States, 28 as well as rugby in other countries, 30 have all been associated with significant instances of cervical spine injury patterns. When caring for elite athletes with cervical spine disease or injuries, the decision-making for conservative versus operative management, as well as deciding when to allow return to play (RTP) are complex and often without clearly defined parameters. While failure of nonoperative management or persistent neurologic symptoms are typically accepted as operative indications, consideration of the athlete’s sport, age, career goals, and potential risk of future worsening of symptoms with conservative care are just some of the additional considerations that must be taken into account when discussing the best treatment course. 36
With regard to operative intervention for athletes with symptomatic cervical disc herniations, radiculopathy, or stenosis, the most commonly reported procedures are anterior cervical discectomy and fusion (ACDF), posterior foraminotomy (PF), and cervical disc replacement (CDR). 14 While the data for RTP after single-level ACDF surgery for disc herniation’s is fairly well established, with most studies finding approximately 80% RTP rates,25,36 outcomes for other cervical procedures are still without clear consensus in this population. Although prior systematic reviews have been published on this topic, new literature has been published in the interim and to our knowledge an updated systematic review on this topic with the most recent evidence is lacking. 25 Given the high stakes of decision-making when it comes to cervical pathology in elite athletes, this systematic study was performed to provide an updated review on RTP and performance outcomes in elite athletes after ACDF, PF, or CDR, to better guide clinicians faced with the task of caring for these patients.
Methods
Search Strategy
We performed a systematic review as outlined by the Cochrane Handbook for Systematic Reviews 10 and reported according to the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 24 guidelines. Two independent reviewers in duplicate performed searches of EMBASE, PubMed, Medline Ovid, and Cochrane databases from inception until April 2020. See Appendix A (available in the online version of this article) for exact search terms and results.
Study Screening
All titles, abstracts, and full texts were screened by 2 reviewers to assess for potential study eligibility. In the instance of any disagreements at the title and abstract stages, a discussion was held among the reviewers, and was resolved by the senior author. A final consensus on eligibility was reached for all articles.
Assessment of Study Eligibility
Inclusion and exclusion criteria for this systematic review were defined a priori. Inclusion criteria were (1) studies in English, (2) studies on adult patients (age ≥18 years), and (3) studies that specifically reported on return-to-sport outcomes after ACDF, CDR, or PF surgeries in elite-level athletes. For this review, elite athletes were defined as those participating at the collegiate, professional, or Olympic level in any sport. Exclusion criteria consisted of nonclinical studies or reviews of literature. The primary outcomes of interest were rates and timing of return to sport. Secondary outcomes of interest were performance after return to sport.
Assessment of Study Quality
For the purposes of assessing quality and risk for bias in the included case series and case report studies, the Joanna Briggs Institute (JBI) Appraisal Checklist for Case Series and Case Reports was utilized.16,26 These are validated 10- and 8- question checklists. If studies received 4 or more answers of yes on the questionnaire, they were considered acceptable. For all retrospective cohort studies, quality and bias were assessed using the Critical Appraisal Skills Programme (CASP)9,16 cohort study checklist. This is a validated 12-item instrument designed for cohort studies. No score is calculated with this tool, it is designed to globally assess quality of studies. If studies received a majority of yes answers, they were considered acceptable. Two reviewers independently reviewed quality of all studies with above instruments, for accuracy and consensus on inclusion or exclusion.
Data Abstraction and Statistical Analyses
Demographic data of included studies were recorded, consisting of authors, publication year, study type, sport or sports of interest, pathology, type of surgical procedures performed, and the involved levels of surgery. Results on rates of RTP, timing of RTP, and outcomes after RTP were extracted when possible and included.
A Cohen’s kappa (κ) coefficient was used to calculated interobserver agreement at all stages according to guidelines laid out in Landis et al. 15 Strength of agreement was categorized as follows: κ = 0.01 to 0.20 was considered slight agreement,κ = 0.21 to 0.4 was fair agreement, κ = 0.41 to 0.6 was moderate agreement, κ = 0.61 to 0.8 was substantial agreement, andκ >0.8 was almost perfect.
Results
Study Identification
From the initial 2,215 records identified, 495 duplicates were subsequently removed, and this left 1720 unique studies. After full text review, 13 articles3,6,8,12,17,18,20,21,23,29,31,33,36 were determined to meet all inclusion criteria and subsequently used for data analysis, with a Cohen’s κ coefficient >0.8 between reviewers (Figure 1). See Table 1 for comprehensive demographics and major results from included studies. All 13 included studies were found to be appropriate for inclusion based on quality and risk of bias using the JBI and CASP checklists, with a Cohen’s κ coefficient >0.8 between reviewers for overall agreement.
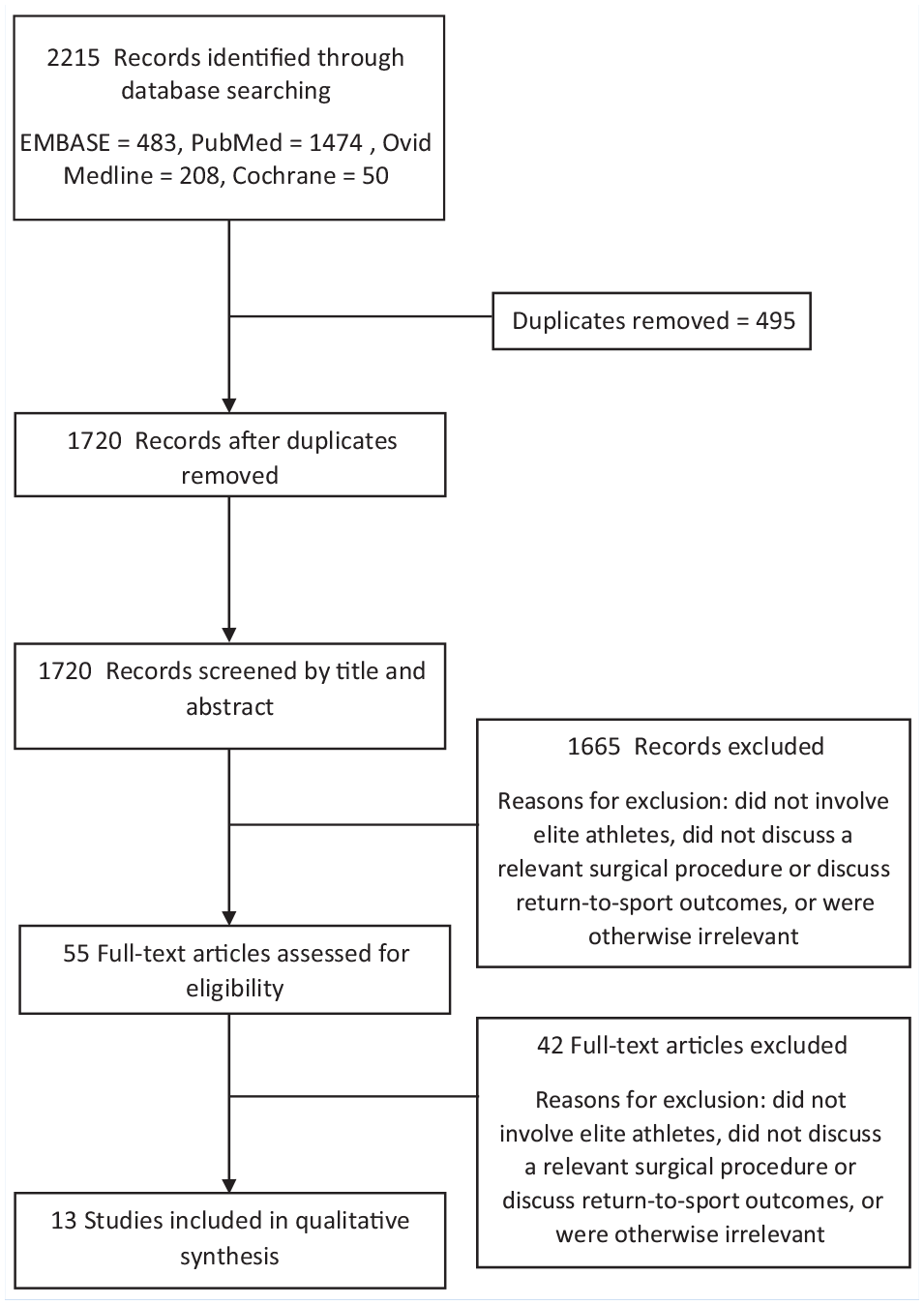
Flowchart of selected studies.
Demographics and results of included studies
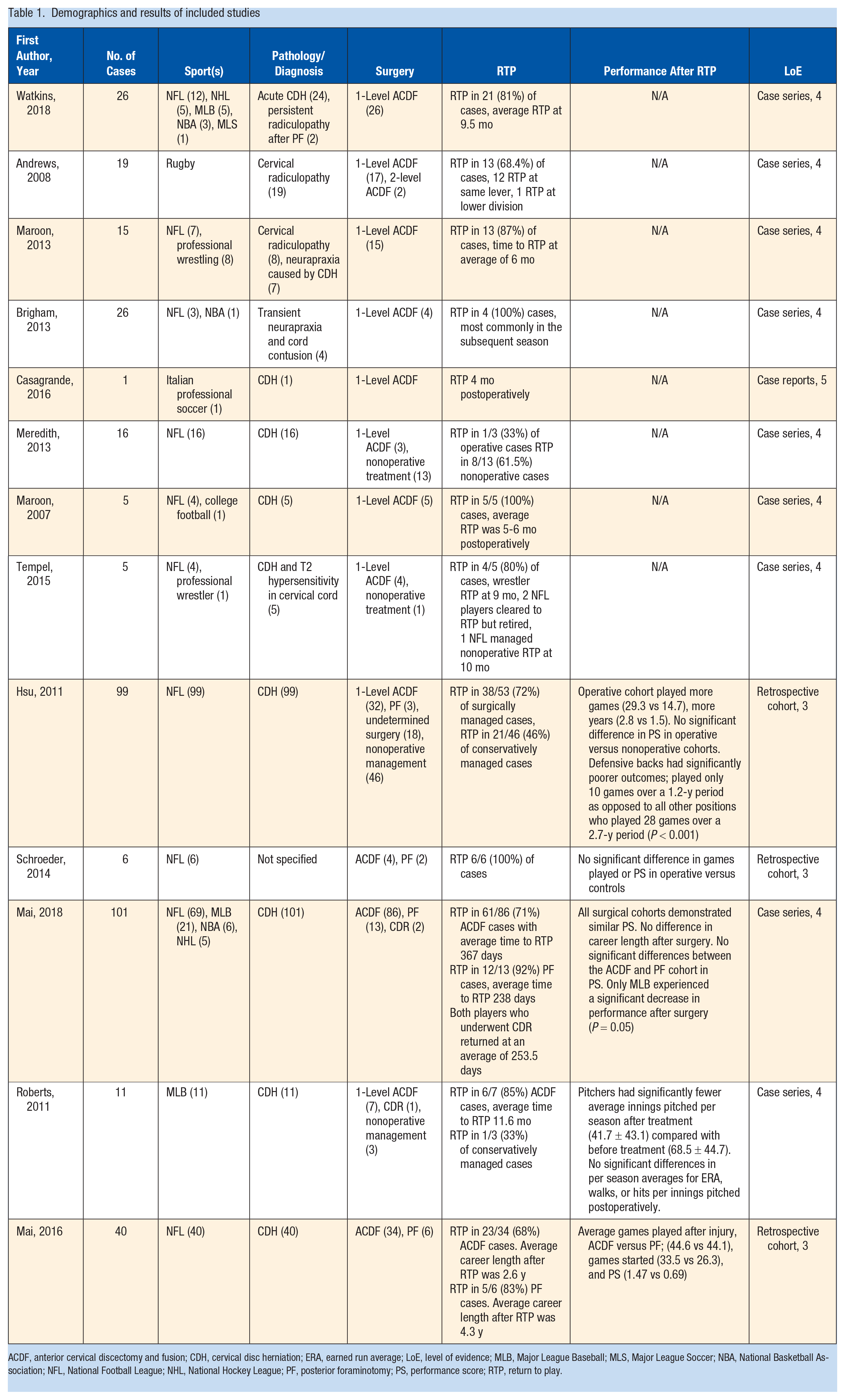
ACDF, anterior cervical discectomy and fusion; CDH, cervical disc herniation; ERA, earned run average; LoE, level of evidence; MLB, Major League Baseball; MLS, Major League Soccer; NBA, National Basketball Association; NFL, National Football League; NHL, National Hockey League; PF, posterior foraminotomy; PS, performance score; RTP, return to play.
ACDF Outcomes
All 13 included articles reported on outcomes in elite athletes after ACDF. In total, 261 National Football League (NFL) athletes, 1 college football player, 10 National Hockey League (NHL) athletes, 37 Major League Baseball (MLB) athletes, 10 National Basketball Association (NBA) players, 2 Major League Soccer (MLS) players, 9 professional wrestlers, and 19 rugby players underwent ACDF.
Watkins et al 36 looked at single-level ACDF outcomes in 26 NFL, NHL, MLB, NBA, and MLS players. The major pathology was disc herniation. They reported that 21 of 26 (81%) athletes returned to play at an average 9.5 months postoperatively. There was 1 NFL and 1 NBA player who suffered recurrent herniations, 1.7 and 6.2 years after index procedure, respectively. The NFL player required further extension fusion surgery.
Andrews et al 3 examined 19 professional rugby players, 17 of whom underwent single-level and 2 who underwent 2-level ACDF. Radicular symptoms were the major pathology. They noted that 13 (68.4%) players returned to their same level of play, 1 player returned to professional play, but in a lower league. The authors noted that 9 of 13 athletes who returned to their previous level did so at 6 months, and 1 player returned 12 months postoperatively. Time to RTP in the remaining 3 was not reported. Three players required additional surgery, 1 of whom originally underwent a 2-level ACDF, this player never returned to play due to pain.
Maroon et al 20 analyzed outcomes after single-level ACDF in 7 NFL players and 8 professional wrestlers. Radiculopathy and neurapraxia were the most common operative indications, and stenosis was noted in 14 of the athletes. They reported that 13 of 15 (87%) players returned to sport at an average of 6 months postoperatively. The 2 who did not return were NFL players. A second ACDF was required in 1 cornerback for adjacent segment disease.
Brigham and Capo 6 reported on 3 NFL and 1 NBA player who underwent single-level ACDF for congenital stenosis and symptomatic cord contusion after hyperextension injuries. All 4 athletes returned to play, most commonly in the next season. One NFL player underwent fusion extension for adjacent level disc herniation after a hit. The NBA player retired 7 years after index procedure for recurrent intermittent symptomatology related to recurrent cord contusions.
Casagrande et al 8 reported on a professional soccer player who underwent single-level ACDF for CDH. He returned to play in less than 4 months and was still playing at time of publication.
Meredith et al 23 reported on 16 NFL players with radiculopathy as the most common symptom. There were 3 players who underwent single-level ACDF, with 1 of 3 (33%) returning to play the next season. In the 13 players managed nonoperatively, 8 (62%) returned to play. No player had to retire because of further symptoms or subsequent cervical injury.
Maroon et al 21 discussed outcomes for 4 NFL and 1 collegiate football athlete after CDH. All underwent single-level ACDF. All returned to sport, on average at 5 to 6 months postoperatively. Two players, a defensive back and a linebacker, had recurrent herniations 27 and 7 games after index procedure, respectively. The defensive back underwent additional surgery and did not return to sport. The linebacker was managed nonoperatively but did not return to sport.
Tempel et al 33 reported on 4 NFL players and 1 professional wrestler with CDH. In their cohort, 4 of 5 athletes underwent ACDF and 1 athlete was managed nonoperatively. The wrestler returned to sport 9 months postoperatively. There were 2 NFL players cleared for return to sport but elected to retire, 1 is waiting for clearance 9 months postoperatively, and 1 underwent nonoperative management and went back to sport 10 months postinjury without issues.
ACDF Versus PF Outcomes
Mai et al 17 reported on single-level ACDF and PF outcomes in 40 NFL players for CDH. A total of 34 players underwent ACDF, and 23 (67.6%) returned to play for an average of 2.6 years postoperatively. A 10% adjacent segment disease rate requiring additional fusion was noted. This occurred in 1 lineman, 1 linebacker, and 2 defensive backs. PF was performed in 6 players, 5 (83.3%) of whom returned to play for an average of 4.3 additional years. Notably, 3 of these 6 players required subsequent ACDF for symptom recurrence, on average at 14.3 months after the index foraminotomy. Of these 3 players, 2 returned to sport. They also compared outcomes for upper-level (C2-4) versus lower-level (C4-T1) CDH. They found no difference in RTP, recovery rates, games started, performance scores, or career length between the 2 groups.
Schroeder et al 31 identified 4 NFL players who underwent ACDF and 2 who underwent PF and found no significant difference in games played, career lengths, or performance scores when compared with control matched players.
ACDF Versus PF Versus CDR
Mai et al 18 compared outcomes for ACDF versus PF versus CDR in a total of 101 athletes from the NFL, MLB, NHL, and NBA. They found that those in the PF group returned to sport sooner and more frequently; however, this group also had higher reoperation rates. They noted that MLB players had worse performance scores postoperatively but did not find differences in performance between surgical groups. The CDR group was excluded from performance analysis due to small sample size (n = 2), but both these players did return to sport after an average of 253 days.
Operative Versus Nonoperative Management
Hsu 12 performed a retrospective cohort study comparing outcomes in NFL players who underwent ACDF or PF for CDH versus those managed nonoperatively. Those treated operatively returned to play at a rate of 72%, compared with 46% in the nonoperative group, and this was a significant difference. Career length was significantly longer after injury in the operative versus nonoperative group, 2.8 versus 1.5 years. No significant differences in performance scores were noted in either group after RTP. The authors did note that defensive backs as a whole did have worse outcomes than other positions, playing for an average of only 10 games over 1.2 years after treatment. Last, they noted that age at diagnosis of CDH was a significant negative predictor for overall career length.
Pitching Performance Postoperatively
Roberts et al 29 analyzed outcomes in 11 MLB pitchers after CDH. In their cohort, 7 were treated with single-level ACDF, 1 received CDR, and 3 were managed nonoperatively. They found that 7/8 (88%) in the operative group and 1/3 (33%) in the nonoperative group returned to play, but this difference was not significant. Overall, the pitchers returned to sport at an average 11.6 months after injury. They did note significantly fewer innings pitched per season after treatment. However, no significant difference was noted in performance-based outcomes after treatment, such as walks, runs, or earned run averages. Mai et al 18 noted that all the pitchers in their cohort who underwent ACDF returned to play; however, 3 of 8 starting pitchers were moved to a relief role postoperatively.
Discussion
This systematic review of the literature identified 13 studies investigating the surgical management of cervical spine conditions in elite athletes. All 13 studies documented RTP after ACDF, 3 discussed RTP after PF, and 2 reported on RTP after CDR. The majority of athletes were NFL players, representing 75% of the athletes, while MLB, NHL, NBA, MLS, professional wrestlers, and rugby players made up the remaining 25%. The most common operation performed in those treated surgically was ACDF (93%), while PF was undergone in 6% and CDR in 1%. Notably, all but 1 study 23 reported that the majority of elite athletes were able to RTP after ACDF, CDR, or PF. There was a limited amount of evidence regarding outcomes after ACDF versus PF. There were 2 studies17,18 that did report more frequent and sooner RTP in the PF group, but with higher reoperation rates, and 1 study 31 that reported no significant differences in performance outcomes between these interventions. There was very limited evidence regarding outcomes after multilevel surgery, with only 1 study 3 reporting a 2-level ACDF in 2 athletes. Similarly, the evidence on CDR was also very limited, with only 2 studies18,29 reporting CDR outcomes in a total of 3 athletes. Notably, although recurrent symptoms or need for further surgery were documented in multiple studies,3,6,8,16,20,23,24,26,33,36 no study reported any catastrophic outcomes in these elite athletes after RTP. RTP after cervical spine surgery is likely safe in both contact and noncontact professional sports. These findings have been supported elsewhere in the literature as well. 13 Caution should be taken when attempting to extrapolate the results of our analysis to sports like gymnastics, swimming, and winter sports, as they are poorly represented in this literature review.
Some of the most feared cervical injuries in athletes are an acute cervical SCI, or a cervical SCI due to an underlying untreated or unidentified pathology. The mechanism of injury and frequency of SCIs varies depending on the popularity of sport in a given region. In the United States, American football, gymnastics, and wrestling are sports that are most frequently associated with cervical SCIs. 32 Rugby is the most common sport in Europe and ice hockey is the most common sport in Canada in which cervical SCIs are sustained.4,32 Contrary to sports like football, hockey, and rugby, cervical spine injuries that result from diving and cycling are more likely to occur during recreational play as opposed to structured competitions.1,11 Although SCIs are relatively rare, 2.4% of all sports-related hospitalizations are due to SCI and 9.4% of all SCIs in the United States are caused by athletics-related activities. 27
Managing athletes with cervical spine pathology is challenging and there is often no right answer in terms of when to operate, which operation to perform, and what results can be expected with regard to timing and level of RTP. The frequency of cervical spine injuries in contact athletes makes this an important topic of review and understanding for both the sports medicine physician, as well as spinal surgeons. For example, when looking at American football and the NFL, Mall et al 19 identified 2208 injuries in players from 2000 to 2010, with 44.7% of these involving the cervical spine. They also identified cervical fractures, disc degeneration and herniation of the cervical region, and SCIs to be among the leading injuries requiring time off from play in these athletes. The most common causes for injury they identified were blocking and tackling. 19 Several authors have proposed guidelines for the management of cervical SCIs and RTP recommendations in athletes.7,35 The general consensus is that athletes should be managed on a case-by-case basis depending on injury patterns and symptomatology, with most authors advocating for RTP only once the athlete is asymptomatic with return of strength and range of motion.
Strengths and Limitations
The present study is the most recent to analyze the available literature with regard to cervical surgery in elite athletes and includes new studies that were not assessed in earlier studies. This updated comprehensive review can assist providers when tasked with the difficult decision-making when it comes to operative decision-making and RTP discussions with elite athletes.
One limitation of this study is the level of evidence of included studies, which was mostly level 4, with some level 3 and level 5 studies. Similarly, some of the included studies were case reports with 1 patient, or case series with limited numbers of included patients.
Last, the included studies were heterogeneous in terms of sport analyzed, type of surgery, level of surgery, and types of outcomes reported. Given this vast array of reported data, no comprehensive meta-analysis could be performed.
Conclusion
The vast majority of current evidence on elite athletes undergoing cervical spine surgery is reported on NFL players, with ACDF being the most commonly documented treatment for cervical spine pathology across all sports. RTP in asymptomatic athletes after surgery is safe, and there is little evidence for decreased performance postoperatively. Surgical management provides a higher RTP rate compared with athletes managed conservatively. There may be slightly higher RTP rates in those undergoing PF versus ACDF; however, the data are limited. There is not enough evidence in the literature regarding CDR to make any recommendation on RTP or performance outcomes. The management of cervical spine pathology in elite athletes is complex and individualized management is recommended. Further investigation in this field is needed, particularly with regard to multilevel surgery and CDR, before clearer recommendations can be elucidated.
Supplemental Material
sj-docx-1-sph-10.1177_19417381211007813 – Supplemental material for Return-to-Play Outcomes in Elite Athletes After Cervical Spine Surgery: A Systematic Review
Supplemental material, sj-docx-1-sph-10.1177_19417381211007813 for Return-to-Play Outcomes in Elite Athletes After Cervical Spine Surgery: A Systematic Review by Joseph Leider, Joshua David Piche, Moin Khan and Ilyas Aleem in Sports Health: A Multidisciplinary Approach
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.