
Abstract
Background:
While increased face mask use has helped reduce COVID-19 transmission, there have been concerns about its influence on thermoregulation during exercise in the heat, but consistent, evidence-based recommendations are lacking.
Hypothesis:
No physiological differences would exist during low-to-moderate exercise intensity in the heat between trials with and without face masks, but perceptual sensations could vary.
Study Design:
Crossover study.
Level of Evidence:
Level 2.
Methods:
Twelve physically active participants (8 male, 4 female; age = 24 ± 3 years) completed 4 face mask trials and 1 control trial (no mask) in the heat (32.3°C ± 0.04°C; 54.4% ± 0.7% relative humidity [RH]). The protocol was 60 minutes of walking and jogging between 35% and 60% of relative VO2max. Rectal temperature (Trec), heart rate (HR), temperature and humidity inside and outside of the face mask (Tmicro_in, Tmicro_out, RHmicro_in, RHmicro_out) and perceptual variables (rating of perceived exertion (RPE), thermal sensation, thirst sensation, fatigue level, and overall breathing discomfort) were monitored throughout all trials.
Results:
Mean Trec and HR increased at 30- and 60-minute time points compared with 0-minute time points, but no difference existed between face mask trials and control trials (P > 0.05). Mean Tmicro_in, RHmicro_in, and humidity difference inside and outside of the face mask (ΔRHmicro) were significantly different between face mask trials (P < 0.05). There was no significant difference in perceptual variables between face mask trials and control trials (P > 0.05), except overall breathing discomfort (P < 0.01). Higher RHmicro_in, RPE, and thermal sensation significantly predicted higher overall breathing discomfort (r2 = 0.418; P < 0.01).
Conclusion:
Face mask use during 60 minutes of low-to-moderate exercise intensity in the heat did not significantly affect Trec or HR. Although face mask use may affect overall breathing discomfort due to the changes in the face mask microenvironment, face mask use itself did not cause an increase in whole body thermal stress.
Clinical Relevance:
Face mask use is feasible and safe during exercise in the heat, at low-to-moderate exercise intensities, for physically active, healthy individuals.
Since the COVID-19 pandemic began, face mask use remains widely recommended to limit the transmission of airborne infectious agents.6,36 Face mask mandates have also been integrated into student-athlete organizations and professional levels based on statewide orders or organizational guidelines.21,23,26 The National Collegiate Athletic Association has identified sports with higher transmission risk of COVID-19 because of close contact during play, such as football, basketball, ice hockey, and wrestling. 23 Fortunately, face mask use has been associated with decreased COVID-19 incidence among both indoor and outdoor sports. 35 While increased face mask use has helped reduce COVID-19 transmission, there have been concerns about its influence on sport safety and performance; this includes concerns about increased risk for sustaining a heat-related illness because of theoretical effects face mask use may have on thermoregulation (ie, heat storage). As athletes continue to participate in sports with regulations requiring face mask use in warm environments, consideration for both COVID-19 exposure and heat-related illnesses must be given for those athletes.
Several reasons exist for why face mask use may impair heat dissipation mechanisms 31 and negatively influence overall thermal sensation and comfort. 24 Previous research demonstrated that N95 respirators and surgical masks induce significantly different temperature and humidity in the microenvironment of the face mask, with concurrent responses in heart rate (HR), thermal stress, and subjective perceptual of discomfort. 18 However, only a few studies have examined the thermoregulatory effect of face mask use by established gold standard measures 34 of core body temperature (ie, rectal or esophageal temperature).17,28,30 Additionally, no previous studies were conducted in warm environments (>27.8°C), or during prolonged low-to-moderate exercise intensity (greater than a walk).9,16,17,27,28,30,32 Thus, direct relationships between core body temperature and face mask use during exercise in the heat have not been clearly established.
Furthermore, consistent, evidence-based recommendations are lacking. The World Health Organization does not recommend a face mask during exercise; 36 however, the Centers for Disease Control and Prevention recommends face mask use for unvaccinated people during indoor, high-intensity activities 5 while maintaining at least 6 feet of social distancing. Although the risk of COVID-19 exposure has been lower during outdoor activities, it is still seemingly critical to wear face masks during indoor sport activities, when other prevention strategies, such as social distancing, are simply not possible. While the value of face mask use during exercise has been recognized based on these recommendations and supporting transmission data on face mask use,7,19 very little is known as to any added thermal burden or risk of face mask use within an athletic population.
Therefore, the purpose of this study was to determine if face mask use influences rectal temperature (Trec) and HR responses during 60 minutes of low-to-moderate exercise intensity in the heat. Additionally, we assessed differences between perceptual sensations (ie, breathing discomfort) across various types of face masks. We hypothesized there would be only minimal physiological differences between face mask trials and a control trial but perceptual sensations could vary.
Methods
Trial Design
In this randomized, crossover study design, each participant completed a baseline visit and 5 trials. Each trial was scheduled 3 to 5 days apart. The baseline visit included anthropometric measures (height and weight) and a maximal oxygen consumption treadmill test (VO2max) to determine relative intensities for the exercise protocol during the trials. Nude body mass was obtained while the participants were in a private room. Prior to VO2max test, the participants were familiarized with the perceptual scales and completed 5 minutes of a self-selected pace warm-up. The speed was increased either 0.5 or 1.0 mph after each 2-minute stage during the test and continued until reaching volitional fatigue. The study was approved by the University of Connecticut institutional review board and all participants provided written informed consent.
Participants
Men and women between 18 and 35 years of age who reported participating in moderate to vigorous physical activity 3 to 5 times per week were recruited for this study. Only women who reported eumenorrhea (1 menstrual cycle every 28 ± 5 days) were included. Exclusion criteria included any current musculoskeletal injury that would limit physical activity and individuals with a history of cardiovascular, metabolic, or respiratory disease. Participants were asked if they had experienced claustrophobia while wearing a face mask or might have face mask anxiety that would affect their ability to participate. All participants were medically cleared by a designated physician and completed a prescreening questionnaire prior to every laboratory visit confirming that they had not knowingly been infected with or previously exposed to COVID-19. All participants had their tympanic temperature taken prior to entering the facility to confirm the absence of a fever (≤38.0°C).
Exercise Protocol
Prior to each trial, urine specific gravity (USG) and urine color 3 were assessed to ensure euhydration (USG ≤ 1.025). If the participant arrived with a USG between 1.020 and 1.025, he or she was asked to drink 500 mL of water to ensure adequate hydration status. If the participant arrived with a USG more than 1.025, the visit was rescheduled for the next available day. For each of the 4 face mask trials, participants donned one of the following face masks (Figure 1): surgical mask (Surgical; Co.Protect), N95 respirator (N95; Co.Protect), adjustable gaiter (Gaiter; MISSION), or adjustable sport mask (Sport; MISSION). A fifth trial was conducted with no face mask (control trial). Trained key personnel performed an Occupational Safety and Health Administration fit-test to ensure participants were properly fitted to the N95 prior to the trial. All face masks were worn to fully cover the nose and mouth throughout the entire trial. Participants were not provided fluids during the trial to maintain constant face mask coverage and to control effects on dependent variables.
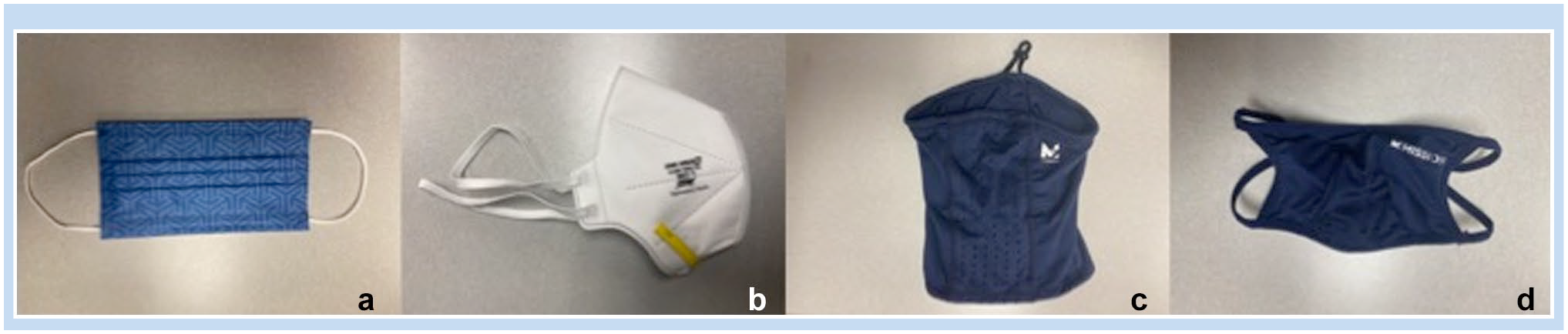
Four types of face masks used in this study: (a) surgical, (b) N95, (c) gaiter, and (d) sport.
Prior to the start of exercise, participants were asked to insert a rectal thermometer (YSI Inc) 10 cm beyond the anal sphincter to provide readings of body temperature and then fitted with a HR strap (POLAR). Sensors capturing temperature and humidity (DS 1923-F5#; iButtons) were placed by a researcher directly above the corner of the participant’s mouth to measure the face mask microenvironment temperature (Tmicro_in) and relative humidity (RHmicro_in) and directly beside the corner of the participant’s eye to measure the environment (Tmicro_out, RHmicro_out) immediately outside of the face mask.
Each trial was conducted in an environmental controlled chamber with an ambient temperature of 32.3°C ± 0.04°C and a RH of 54.4% ± 0.7%. After a 10-minute period of environment equilibration while seated inside the environmental chamber, participants began the exercise protocol on the treadmill. The protocol consisted of 60 minutes of walking and jogging at relative speeds based on the treadmill speed at which they achieved their VO2max test during a baseline visit (4 consecutive bouts of 15-minute exercise; 5 minutes at 35%, 7 minutes at 50%, and 3 minutes at 60%, with the treadmill set at 2% grade). Exercise intensities were determined using the wet-bulb globe temperature (WBGT) activity modification guidelines. It is recommended that at a WBGT of ~29°C to 33°C, physical activity should be limited to 1 hour with 20 minutes of rest breaks distributed throughout. 12 The four 5-minute bouts at 35% represented this active rest time. Exercise and performance testing was terminated if one of the following criteria was met: (1) Trec reached 40°C, (2) participant requested to stop, (3) participant exhibited altered or uneven gait, or (4) HR was greater than estimated HR max for 5 minutes.
Outcome Measures
Face masks were weighed before and after each trial to obtain data on saturation of each face mask from sweat and exhaled water vapor. Nude body mass, USG, and urine color were recorded before and after each trial to determine hydration changes. Measures of Trec, HR, Tmicro_in, RHmicro_in, Tmicro_out, RHmicro_out, were taken continuously throughout each trial and recorded every 5 minutes while environmental conditions (ambient temperature, RH, and WBGT) were recorded every 15 minutes. Using visual Likert-type scales, the 9-point thirst sensation scale (ranging from not thirsty to very very thirsty), 8 8-point thermal sensation scale (ranging from unbearably cold to unbearably hot), 37 and 10-point fatigue level scale (ranging from no fatigue at all to completely fatigued) were assessed every 10 minutes. Rating of perceived exertion (RPE; Borg RPE 6-20 scale) 4 and 7-point scale of overall breathing discomfort (ranging from no discomfort to intolerably high discomfort) 17 were assessed every 5 minutes.
Statistical Analysis
One-way repeated-measures analyses of variance (ANOVAs) with least significant difference post hoc tests were performed to examine differences between face mask types and percentage body mass loss (%BML), USG, and face mask weight, which was calculated by subtracting the preexercise face mask weight from the postexercise face mask weight. Two-way repeated-measures ANOVAs with Tukey post hoc tests were performed to examine differences between face mask trials and time at 0-, 30-, and 60-minute time points for mean Trec, mean HR, Tmicro_in, Tmicro_out, RHminro_in, humidity difference between inside and outside of the face mask (ΔRHmicro), RPE, thermal sensation, thirst sensation, fatigue level, and overall breathing discomfort. Pearson product-moment correlations were used to calculate associations between mean overall breathing discomfort and other mean variables. Correlation coefficient thresholds were used with 0.1, 0.3, 0.5, 0.7 and 0.9, indicating small, moderate, large, very large, and extremely large associations, respectively. 15 Stepwise linear regression analysis was used to predict mean overall breathing discomfort from other mean variables. Data are reported as mean (M) ± SD and effect size (ES). ES was calculated using Cohen d with the resulting effects identified as either small (0.20-0.49), medium (0.50-0.79), or large (>0.8) effects. 20 All statistical analyses were completed using SPSS Statistics, Version 25 (IBM Corp) and Jamovi (Jamovi Version 1.2; The Jamovi Project 2020). Significance was set a priori at P ≤ 0.05.
Results
All participants completed all face mask trials and the control trial within 3 weeks. Twelve healthy participants (8 male, 4 female; age = 24 ± 3 years; height = 175 ± 10 cm; weight = 69.24 ± 14.30 kg; VO2max = 52.21 ± 7.31 mL·kg−1·min−1) participated in this study. There were no significant differences in %BML between face mask types (P = 0.39). Prior to each trial, all of the participants were ensured euhydrated status (USG ≤ 1.025). No significant differences were found between trials in both preexercise USG (P = 0.98) and postexercise USG (P = 0.43).
Physiological Measurements
Mean Trec (Figure 2) and mean HR (Figure 3) increased at 30- and 60-minute time points in face mask trials and None compared with 0-minute time point (P < 0.01). However, there were no significant differences in mean Trec (P = 0.73) and mean HR (P = 0.87) throughout the 60 minutes of exercise between face mask trials and None.
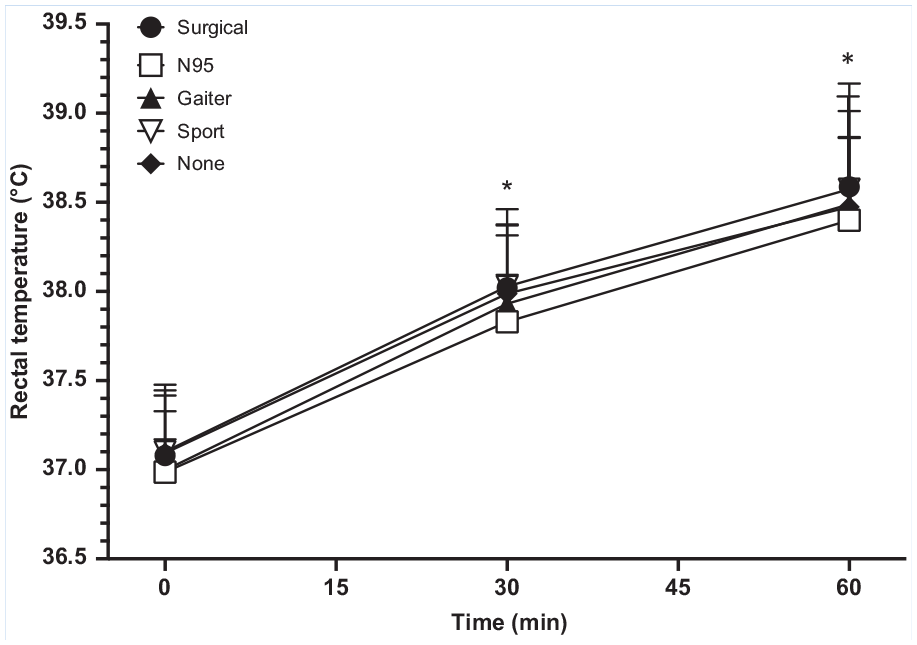
Mean rectal temperature at 0-, 30-, and 60-minute time points during exercise in the heat while wearing various face masks. *Indicates significant difference from the 0-minute time point for all trials, P ≤ 0.05.
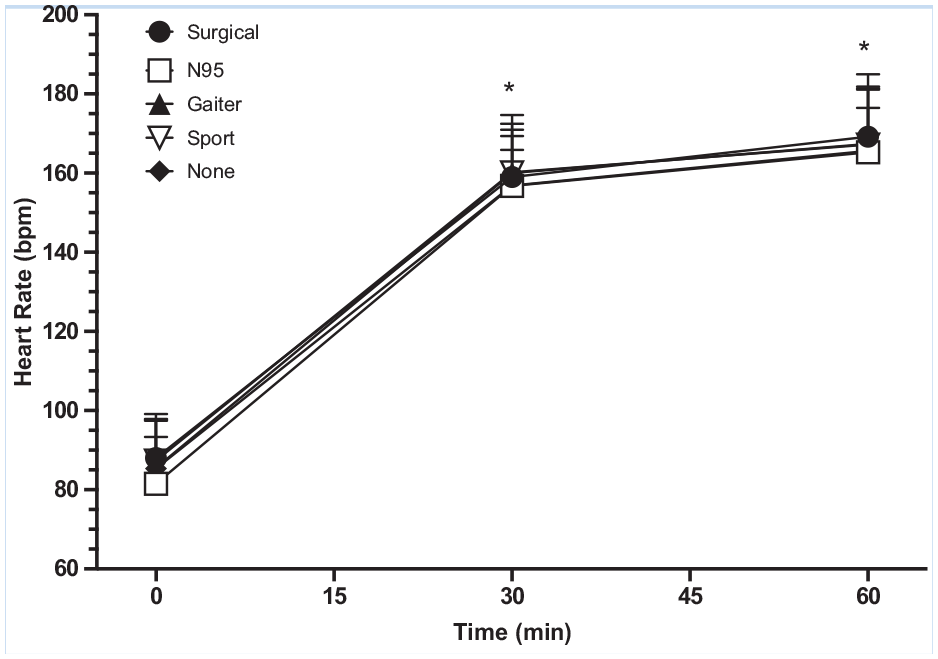
Mean heart rate at 0-, 30-, and 60-minute time points during exercise in the heat while wearing various face masks. *Indicates significant difference from the 0-minute time point for all trials, P ≤ 0.05.
Face Mask Microenvironment Temperature and Humidity
Table 1 displays mean values of each face mask microenvironment variable at 0-, 30-, and 60-minute time points. Face mask weight was significantly different between face mask trials (P < 0.01). The weight of the gaiter mask was significantly greater compared with other face mask types (P < 0.01; ES > 0.8). Mean Tmicro_in and mean Tmicro_out increased at 30- and 60-minute time points in face mask trials, and the control trial compared with 0-minute time points (P < 0.01). There was difference in mean Tmicro_in (P < 0.01) between face mask trials independent of time while no difference existed in Tmicro_out (P = 0.09). Mean Tmicro_in was significantly higher in the gaiter mask trial compared with the control trial (P = 0.02; ES = 3.89). Mean RHmicro_in increased at 30- and 60-minute time points in face mask trials compared with 0-minute time points (P < 0.01). Mean RHmicro in the sport mask trial was also significantly higher than the N95 mask trial independent of time (P < 0.01; ES = 3.72). Interaction effects between face mask trials and time at 0-, 30-, and 60-minute time points were found in ΔRHmicro (P = 0.03); however, there were no trial by time interactions in Tmicro_in (P = 0.53), Tmicro_out (P = 0.80), or RHmicro_in (P = 0.16). ΔRHmicro was greater in face mask trials compared with the control trial at 0-, 30-, and 60-minute time points (0 minutes: P < 0.01, ES > 0.8; 30 minutes: P < 0.01, ES > 0.8; 60 minutes: P < 0.01, ES > 0.8; Figure 4). ΔRHmicro in the sport mask trial was also significantly greater than the surgical and N95 mask trials at 30-minute time (P < 0.01; ES > 0.8).
Mean face mask microenvironment outcomes during 60 minutes of exercise while wearing various face masks a
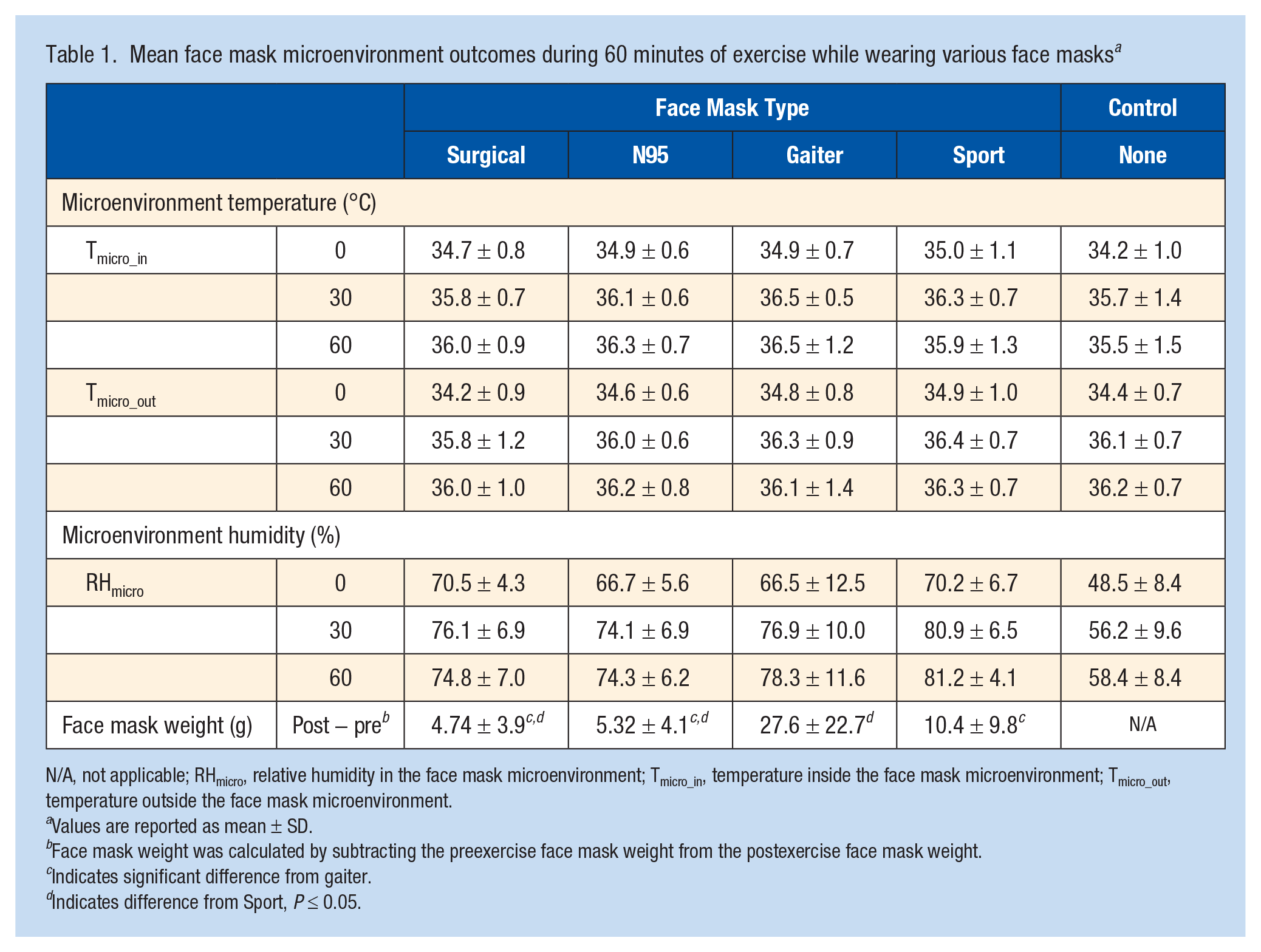
N/A, not applicable; RHmicro, relative humidity in the face mask microenvironment; Tmicro_in, temperature inside the face mask microenvironment; Tmicro_out, temperature outside the face mask microenvironment.
Values are reported as mean ± SD.
Face mask weight was calculated by subtracting the preexercise face mask weight from the postexercise face mask weight.
Indicates significant difference from gaiter.
Indicates difference from Sport, P ≤ 0.05.
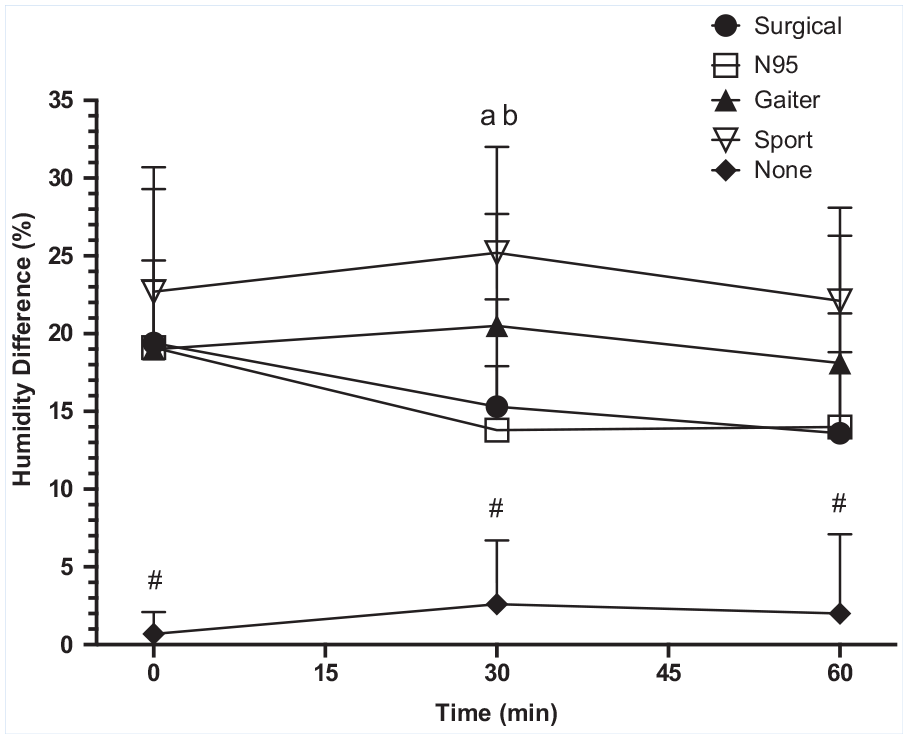
Mean face mask microenvironment humidity difference between inside and outside of the face mask at 0-, 30-, and 60-minute time points during exercise in the heat while wearing various face masks. #Indicates significant difference from all face mask trials. Significant difference from the surgical mask (a). Significant difference from N95 mask (b), P ≤ 0.05.
Perceptual Measurements
Table 2 displays mean values of each perceptual variable at 0-, 30-, and 60-minute time points. Mean RPE, thermal sensation, fatigue level, and overall breathing discomfort were greater at 30 and 60-minute time points compared with 0-minute time points (P < 0.01) while thirst sensation was greater at 60-minute time points compared with 0- and 30-minute time points (P = 0.01 and P < 0.01, respectively). There was no difference in mean RPE (P = 0.81), thermal sensation (P = 0.54), thirst sensation (P = 0.89), and fatigue level (P = 0.61) between face mask trials and the control trial independent of time, except mean overall breathing discomfort (P < 0.01). Mean overall breathing discomfort was significantly higher in face mask trials compared with the control trial independent of time (P < 0.01; ES > 0.8). Interactions effects between face mask trials and time at 0-, 30-, and 60-minute time points were also found in overall breathing discomfort (P < 0.01) (Figure 5). The control trial was significantly lower than the N95, gaiter, and sport mask trials at 30-minute time points (P < 0.01; ES > 0.8) and all face mask trials at 60-minute time point (P < 0.01; ES > 0.8). Overall breathing discomfort in the sport mask trial was significantly higher than the surgical mask trial at 60-minute time point (P < 0.01; ES = 0.74).
Mean perceptual outcomes during 60 minutes of exercise while wearing various face masks a
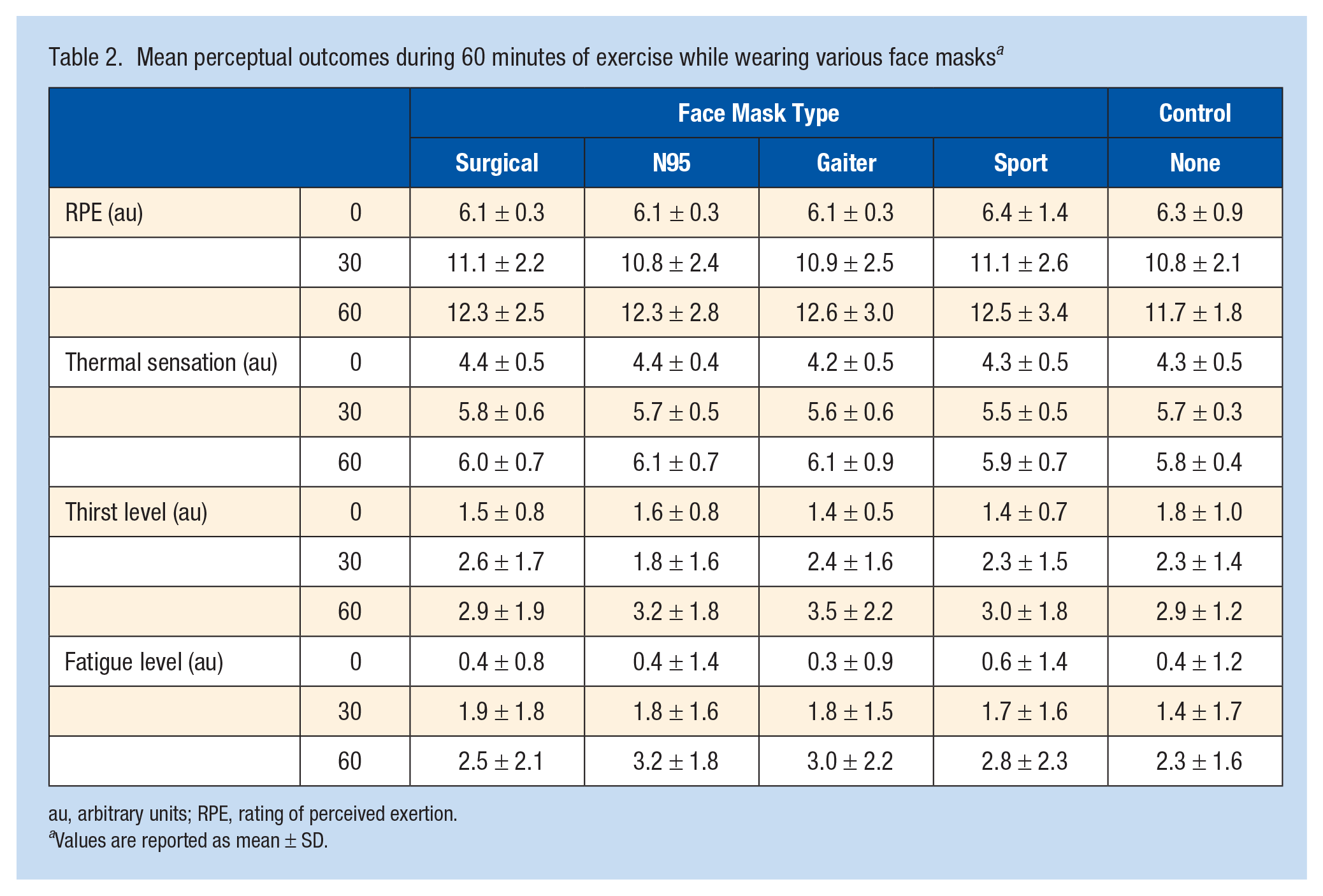
au, arbitrary units; RPE, rating of perceived exertion.
Values are reported as mean ± SD.
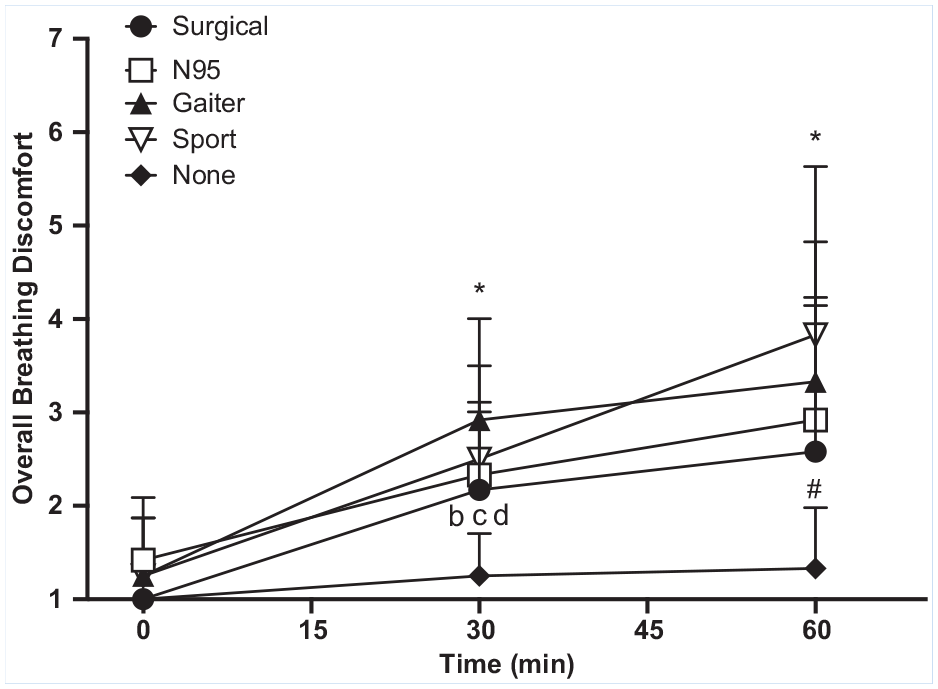
Mean overall breathing discomfort at 0-, 30-, and 60-minute time points during exercise in the heat while wearing various face masks. *Indicates significant difference from 0-minute time point. #Indicates significant difference from all face mask trials. Significant difference from N95 mask (b). Significant difference from the gaiter mask is indicated by (c). Significant difference from the sport mask (d), P ≤ 0.05.
Associations and Predictions Between Overall Breathing Discomfort and Other Variables
Higher overall breathing discomfort was significantly associated with higher RHmicro_in (r = 0.427; P < 0.01), higher RPE (r = 0.427; P < 0.01), higher thirst level (r = 0.411; P < 0.01), higher fatigue level (r = 0.404; P < 0.01), higher thermal sensation (r = 0.376; P < 0.01), greater ΔRHmicro (r = 0.312; P = 0.02), higher mean HR (r = 0.275; P = 0.03). Stepwise linear regression indicated higher RHmicro_in, RPE, and thermal sensation significantly predicted higher overall breathing discomfort (r2 = 0.418; P < 0.01) while higher RHmicro_in and RPE by themselves predicted higher overall breathing discomfort (r2 = 0.350; P < 0.01).
Discussion
The primary purpose of this study was to determine if face mask use influences Trec and HR responses during exercise in the heat. To our knowledge, our study is the first to evaluate the effect of face mask use on thermoregulation during 60 minutes of low-to-moderate exercise intensity in the heat.
The Effect of Face Mask Use on Rectal Temperature and Heart Rate
Our finding showed Trec was not affected by face mask use during exercise in environments up to 32°C. While previous studies were conducted in milder ambient temperatures (ie, 20°C-25°C) during low-intensity exercise, our result was consistent with the findings from those previous studies,17,28 reporting only minor or no effects of face mask use on Trec. Although more extensive clothing or protective equipment during physical activity have demonstrated significant impacts on Trec due to decreased evaporative heat loss,2,11 our study suggests that face mask use, and its smaller surface area coverage, did not significantly affect the body’s ability to dissipate heat produced by metabolism during exercise. Additionally, HR was affected by the duration and intensity of the exercise as hypothesized, but no significant differences were found between face mask trials and the control trial. Previous research has reported that surgical mask use results in increased HR (9.5 bpm) and respiratory rate (1.6 breaths·min−1) during low-intensity exercise. 30 While our participants completed higher exercise intensity in a warmer environment compared with the previous study, change in HR was minimal and nonsignificant between the face mask and control trials. As other studies described,9,10,29 a small increase in HR due to face mask use would not affect ventilation and oxygen saturation during exercise in healthy individuals. However, there may be alterations to Trec and HR during higher exercise intensities (greater than 85% of VO2max 33 or greater BML >2% 1 ), which were not explored by this study.
Changes in Face Mask Microenvironment During Exercise in Heat
Multiple studies suggested that face mask microenvironment temperature and humidity have been considered a key parameter in indicating thermal sensation.18,22,25,28,31-33 A face mask may resist the passage of water vapor and decrease heat loss by evaporative cooling. 11 Thus, as the temperature gradient between the ambient environment and the face mask microenvironment decreases, heat dissipation from the face mask microenvironment also decreases. 31 Although discussion regarding the types of face mask material is beyond the scope of this article, our results suggest that gaiter and sport masks retained more water vapor and sweat after the exercise compared with surgical and N95 masks (Table 1). Since higher Tmicro_in, RHmicro_in, and ΔRHmicro were observed in those face mask trials, changes in face mask microenvironment due to decreased heat dissipation would affect thermal sensation of the covered facial area, but face mask use itself did not cause whole body thermal stress.
Breathing Discomfort Caused by Face Mask Use
In addition to physiological variables, our study investigated perceptual variables that may be affected negatively with face mask use during exercise in the heat. Our result demonstrated that overall breathing discomfort was significantly higher between face mask trials compared with the control trial, and increased with exercise duration. Furthermore, higher RHmicro_in, RPE, and thermal sensation significantly predicted higher overall breathing discomfort. Because face mask wetness caused by retention of water vapor and sweat may cause breathing resistance and discomfort,13,18 those results can be explained by changes in the face mask microenvironment. Our findings are supported by multiple previous studies; however, no adverse physiological effects or risk of face mask use during exercise were reported.14,17,18,32,33 Therefore, overall breathing comfort should be used to guide type of face masks when exercising in the heat.
Limitation and Future Research
One of the limitations of our study was that the effectiveness of face mask use for the transmission and protection against COVID-19 or other airborne viruses was not assessed. Since it is important to consider the risk of COVID-19 exposure during the pandemic, the effectiveness of the face mask use during exercise should be examined along with thermoregulation responses to maintain a safe environment for all levels of athletes. Further research should be extended to evaluate face masks with consideration for prevention of COVID-19 transmission during indoor sports activities in a warm environment. This would be beneficial to establish a more detailed guideline of face mask use during exercise in the heat.
Conclusion
Our study revealed that face mask use during 60 minutes of low-to-moderate exercise intensity in the heat (32°C) was associated with no significant changes in Trec or HR. Although face mask use may affect overall breathing discomfort due to the changes in face mask microenvironment, face mask use itself did not cause whole body thermal stress. Therefore, our findings suggest that face mask use is feasible and safe during exercise in heat, at low to moderate intensities, for physically active healthy individuals.
Footnotes
The authors report no potential conflicts of interest in the development and publication of this article.