
Abstract
Background:
Severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) was first identified in December 2019 in Wuhan, China. Although coronavirus disease-19 (COVID-19) affects every population group, the sports community and athletes require special consideration of the effects on cardiovascular, musculoskeletal, neurologic, and respiratory systems. A comprehensive understanding of imaging indications, findings, and features of COVID-19 supports appropriate imaging utilization and effective patient management and treatment.
Purpose:
To review the spectrum of sports imaging in COVID-19 infection, organ system manifestations, vaccine effects, and complications in recreational and competitive athletes.
Study Design:
Narrative review.
Level of Evidence:
Levels 4 and 5.
Methods:
Based on a PubMed database search, studies describing the imaging findings of COVID-19 infection, organ system manifestations, vaccine effects, and complications in recreational and competitive athletes were included.
Results:
On March 11, 2020, World Health Organization officially declared COVID-19 a global pandemic. As of May 9, 2022, more than 515 million confirmed cases of COVID-19 were reported globally. While the multisystem effects of COVID-19 are incompletely understood, the role of imaging in diagnosing, monitoring, and prognosticating active disease, long-term effects, and complications is evolving. In the respiratory system, imaging plays an important role in diagnosing, characterizing, and monitoring pulmonary COVID-19 infections, barotrauma, and COVID-19-associated chronic pulmonary opacities and fibrotic-like lung changes. Ultrasonography, computed tomography, and magnetic resonance imaging aid in the timely diagnosis of ischemic, embolic, and thrombotic peripheral and central cardiovascular events, including deep venous thrombosis, pulmonary embolism, myocarditis, and stroke. COVID-19-associated musculoskeletal and peripheral nervous system manifestations include rhabdomyolysis and myonecrosis, plexus and peripheral neuropathies, Guillain-Barré syndrome, and shoulder injury related to vaccine administration.
Conclusion:
In athletes, COVID-19 infections and associated effects on cardiovascular, musculoskeletal, neurologic, and respiratory systems require special consideration. With the increasing understanding of the multisystem effects of COVID-19, the role of imaging in diagnosing, monitoring, and prognosticating active disease, long-term effects, and complications is evolving. A comprehensive understanding of imaging indications, COVID-19 imaging features, and organ system effects aids in appropriate imaging utilization and effective patient management and treatments.
Coronaviruses, including severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2), first identified in December 2019 in Wuhan, China, are single-stranded RNA viruses of the subfamily Coronavirinae. 98 On March 11, 2020, World Health Organization (WHO) officially declared coronavirus disease-19 (COVID-19) a global pandemic. On May 9, 2022, more than 515 million confirmed cases of COVID-19 and more than 6.2 million deaths due to COVID-19 had been reported globally. 105
The signs and symptoms of COVID-19 infections range from no symptoms in some patients to fever, cough, myalgia, headache, and dyspnea.7,34 Although respiratory symptoms and complications are the most frequent findings, COVID-19 also affects the cardiovascular, neurologic, and musculoskeletal systems.21,62
Due to their perceived fitness level and often younger age than the general population, athletes are assumed to be less vulnerable to COVID-19 complications. 107 However, COVID-19 infection- and vaccine-related complications such as myocarditis have been reported mostly in young individuals. 84 Therefore, early diagnosis of COVID-19 infection- and vaccine-related complications in athletes is important to prevent morbidity, mortality, and decisions on appropriate return-to-play timing. 95
Imaging plays an important role in diagnosing manifestations and complications of COVID-19 infections. A thorough understanding of the indications and imaging features of COVID-19 infection aids in effective patient management and treatment.
This article reviews the spectrum of sports imaging in COVID-19 infection, organ system manifestations, vaccine effects, and complications in recreational and competitive athletes.
Respiratory System
Symptoms related to the respiratory system are among the most common presentations of COVID-19 infection. 72 The symptoms vary from cough and dyspnea to acute respiratory distress syndrome and severe hypoxemia with higher mortality rates. 27
Chest radiographs in posteroanterior and lateral projections are the appropriate imaging test for the initial assessment of athletes with respiratory symptoms. Chest radiographs are useful for detecting interstitial and airspace opacities in the setting of viral pneumonia, pleural effusions, pneumothorax, cardiomegaly, pulmonary edema, and congestive heart failure (Figure 1).
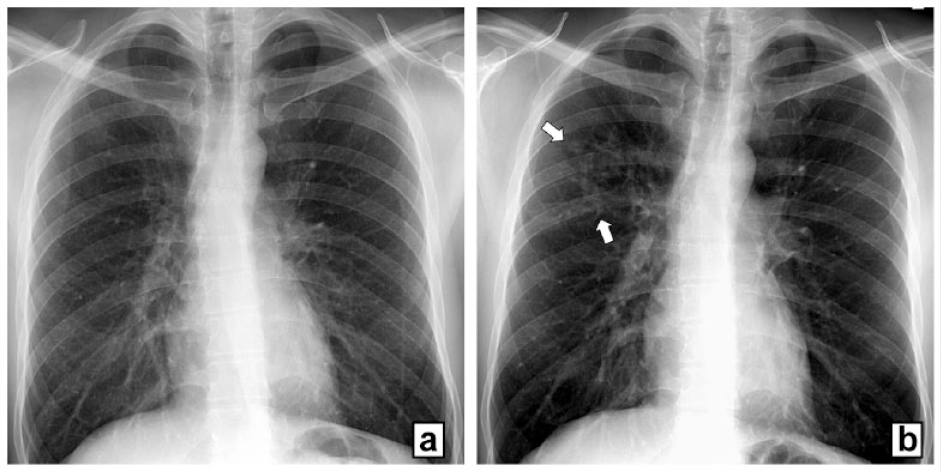
A 31-year-old COVID-19-positive recreational male athlete presenting with cough and exertional dyspnea. (a) Initial radiograph of the chest is normal. (b) Follow-up radiograph 5 days later demonstrates right upper lobe viral pneumonia (arrows).
Radiographs have low accuracy for detecting subtle viral parenchymal opacities of early-stage COVID-19 infections, whereas chest CT scans are most accurate in detecting and characterizing pulmonary parenchymal disease and, alternatively, may aid in detecting signs of acute heart failure indicating cardiac injury. 22 Thoracic chest CT findings include linear and reticular interstitial opacities, and ground-glass to dense consolidative airspace opacities (Figure 2). Multifocal nonconsolidative ground-glass opacities are the most common CT feature. 108
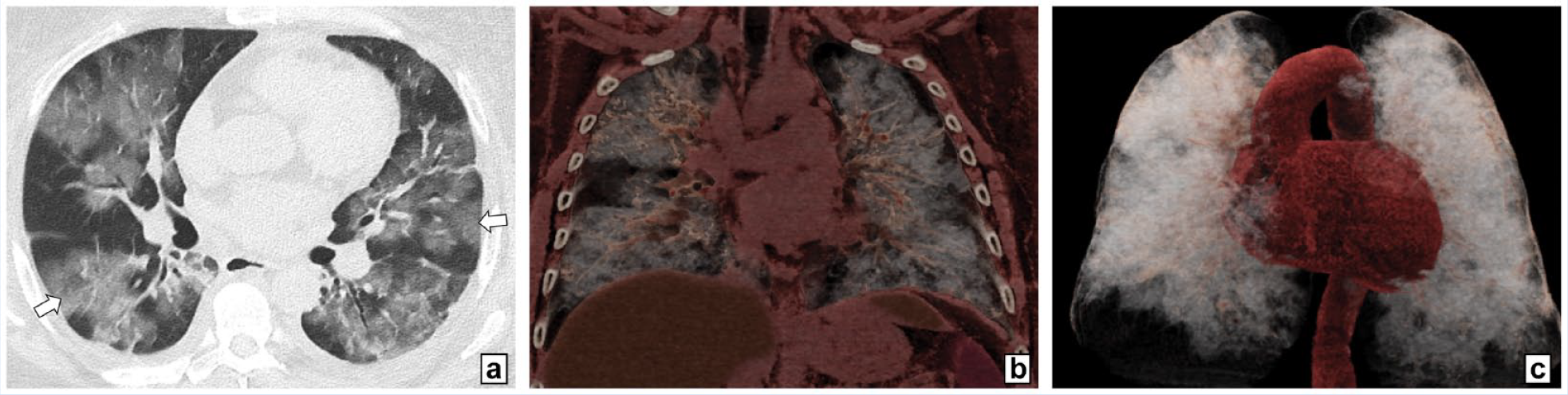
A 24-year-old COVID-19-positive male American football player presenting with cough and dyspnea. (a) Axial CT image demonstrates geographic nonconsolidative ground-glass opacities bilaterally (arrows). (b) Coronal 3-dimensional (3-D) CT rendering of the chest redemonstrates nonconsolidative ground-glass opacities in both lungs indicated by the bright opacified areas. (c) 3-D volume rendering of both lungs demonstrates the high burden of interstitial and airspace opacities indicated by the bright opacified areas.
While common in the acute phase, ground-glass opacities may persist for months after the acute infection in patients, with varying degrees of persisting symptoms. In a cohort of 1733 patients who recovered from hospitalization due to COVID-19 infection, abnormal ground-glass opacities were present in over 40% of patients undergoing chest CT 6-month after the acute infection. 33
COVID-19 infections are associated with hypercoagulability and increased risk for thromboembolic events. Contrast-enhanced chest CT scans with pulmonary arterial bolus timing should be ordered in cases with suspected COVID-19-related pulmonary embolism. 83 A study evaluating the prevalence of pulmonary embolism in patients with COVID-19 found pulmonary emboli on CT pulmonary angiography in 37% of patients, which was more than double the frequency compared with a matched cohort without COVID-19 infection. 39 Elevated D-dimer levels correlated directly with the presence and severity of pulmonary embolism on CT studies.
Barotrauma is an important complication of COVID-19 characterized by the abnormal presence of air along pleural surfaces. The pathomechanism is incompletely understood, but increased pressures within the distal airways and alveoli play a role. Radiography and CT imaging features include pneumomediastinum, pneumopericardium, pneumothorax, and soft tissue emphysema (Figure 3). Barotrauma occurs in COVID-19 patients without and with intubation, representing an independent risk factor for COVID-19-associated death. 58 The implications for athletes recovering from COVID-19, including a higher susceptibility to exercise-induced structural lung trauma, have not been described in detail.
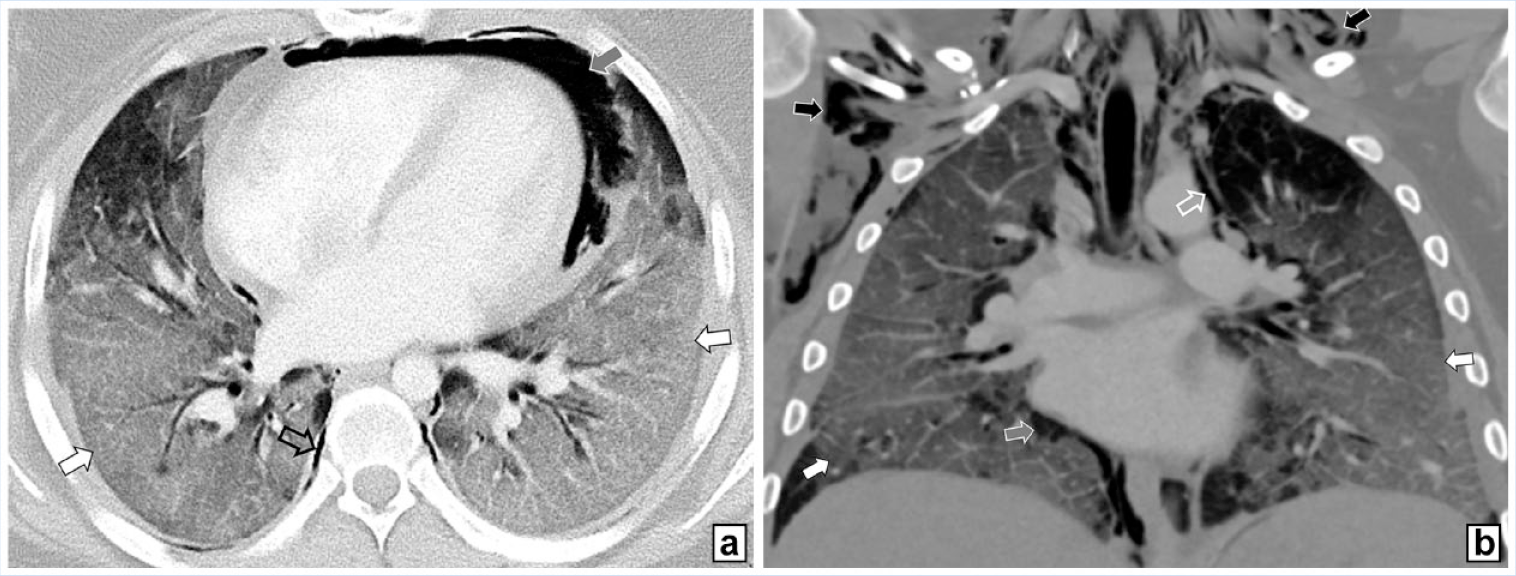
A 19-year-old COVID-19-positive female collegial athlete presenting with severe dyspnea and hypoxia. (a) Axial CT images demonstrate diffuse ground-glass opacities of both lungs (white arrows), pneumomediastinum (hollow arrow), and pneumopericardium (gray arrow). (b) Coronal CT image demonstrates diffuse ground-glass opacities of both lungs (white arrows), pneumopericardium (hollow arrow), pneumopericardium (gray arrow), and soft tissue emphysema of the thoracic wall and neck (black arrows).
Post COVID-19 syndrome (PACS) is an evolving syndrome characterized by persistent symptoms and delayed long-term complications beyond the acute infection. 68 Components of PACS include prolonged injury and permanent damage to the lungs, heart, kidney, and brain, which may be associated with impaired exercise capacity.
SARS-CoV-2 involvement of lung parenchyma upregulates profibrotic signaling pathways, explaining restrictive lung disease features in PACS. Patients with PACS may present on a spectrum ranging from subtle lingering subpleural opacities (Figure 4) to the rapid development of parenchymal lung fibrosis, which may present with architectural parenchymal lung distortions and an organizing pneumonia pattern with bilateral subpleural ground-glass opacities in the lower lung zones, interlobular septal thickening, perilobular and peribronchial dense consolidation, and traction bronchiectasis (Table 1).67,93 In contrast to fibrotic interstitial lung disease, PACS-associated fibrotic-like changes may improve or resolve over time. 32
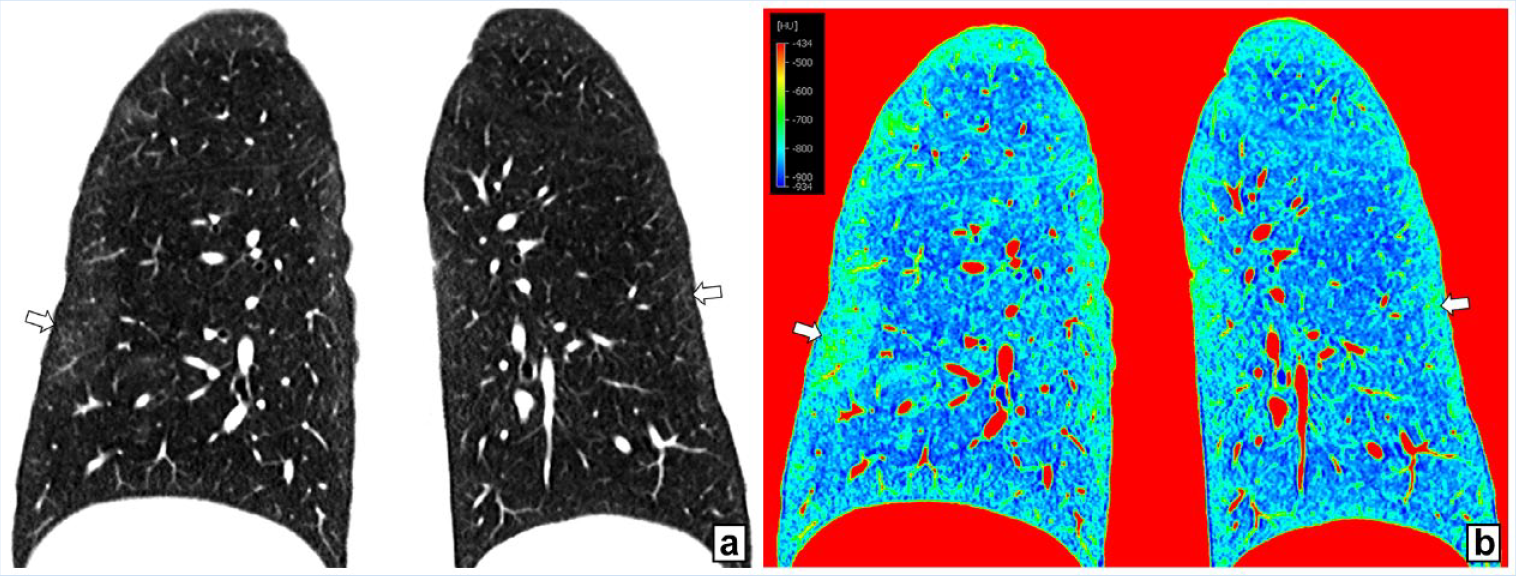
A 32-year-old female avid runner after recovered COVID-19 infection presenting with reduced exercise capacity and exertional dyspnea. (a) Coronal CT of the lung demonstrates subtle subpleural linear, reticular, and ground-glass opacities of both lungs (arrows). (b) Corresponding coronal Hounsfield Unit-based density map redemonstrate the higher density subpleural opacities (arrows).
Imaging findings of COVID-19
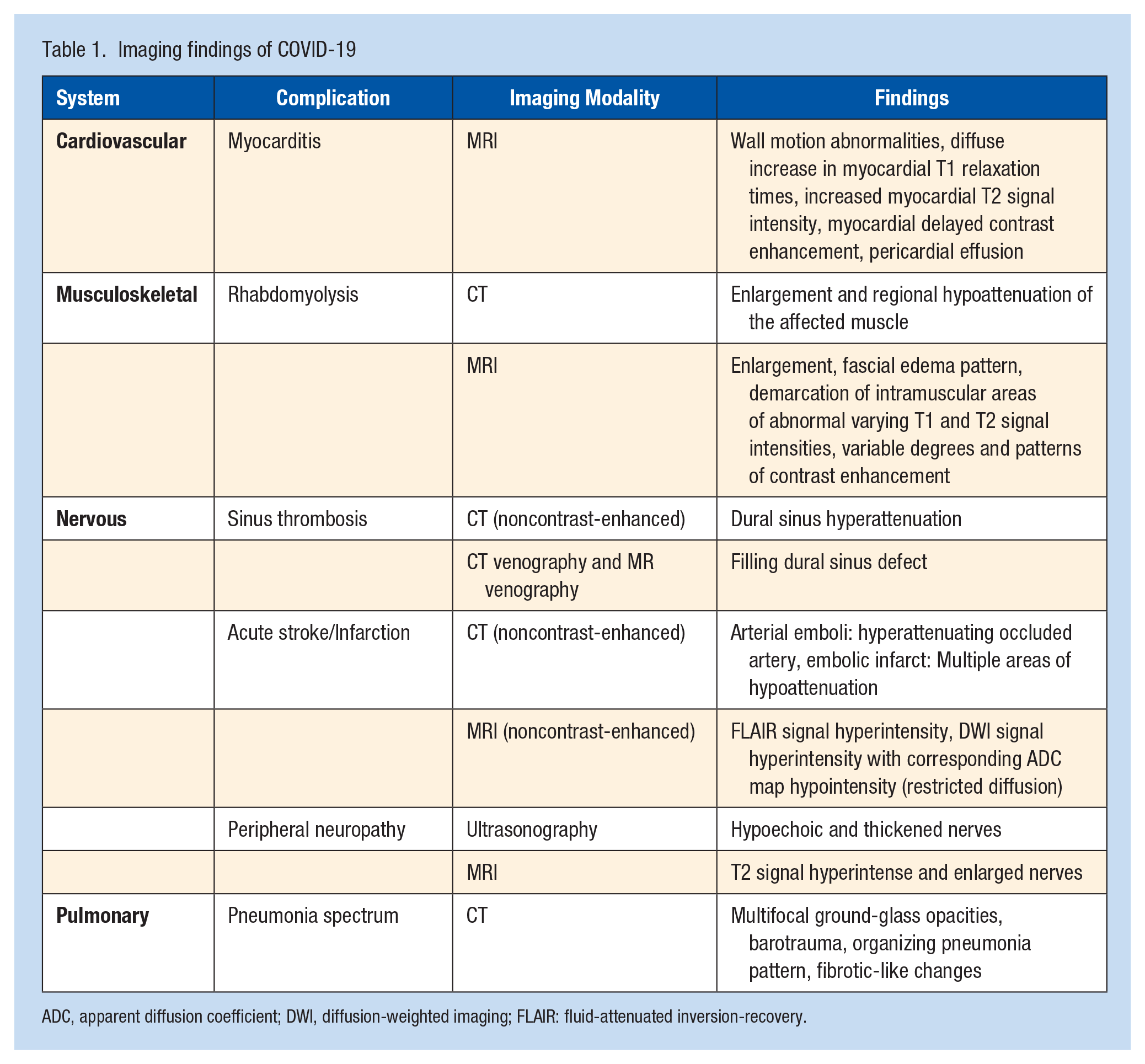
ADC, apparent diffusion coefficient; DWI, diffusion-weighted imaging; FLAIR: fluid-attenuated inversion-recovery.
COVID-19 vaccine-related complications of the respiratory system reported in association with viral vector and mRNA vaccines are rare and, in part, anecdotal.1,6,54,103 Reports of COVID-19 vaccine-related complications appear similar to COVID-19 infection-related complications, including pulmonary embolism due to hypercoagulability and fibrotic-like lung parenchyma changes.74,109
Cardiovascular System
Cardiac injury in patients with COVID-19 infection was described early during the pandemic. In a 41-patient cohort with COVID-19 infection from Wuhan, China, 12% (5/41) developed acute cardiac injury. 34 A larger cohort study of 416 patients with COVID-19 reported a 20% incidence of cardiac injury with higher morbidity and mortality rates (hazard ratio, 4.26 [95% CI, 1.92-9.49]) compared with COVID-19 patients without cardiac injury. 87
COVID-19-associated cardiac injury may present as nonischemic myocardial injury and myocarditis, 40 acute myocardial infarction, 49 heart failure and cardiomyopathy, 110 and arrhythmia. 102 Myocardial injury may result from direct cardiac infection and cell damage, or indirectly through thrombotic activity, stress cardiomyopathy, and other factors. 100 Patients with COVID-19-associated myocardial inflammation with or without underlying cardiovascular disease have a higher mortality rate than patients without myocardial involvement and underlying cardiovascular disease. 31
In competitive athletes, myocarditis is a leading cause of sudden death. COVID-19-induced myocardial injury may be diagnosed based on clinical symptoms; however, cardiac MRI is more accurate in detecting myocarditis in patients with COVID-19 infections.18,66 In a study of 145 student-athletes recovering from COVID-19 infection, screening cardiac MRI found a 1.4% prevalence of myocarditis. 91
In athletes, COVID-19-induced myocarditis may be clinical or subclinical. In a large-scale multicenter cohort study, 1597 competitive US collegiate athletes undergoing comprehensive cardiovascular testing had a 0.31% prevalence of COVID-19 myocarditis with a symptom-based clinical screening strategy, whereas the prevalence of COVID-19 myocarditis was 2.3% when cardiac MRI was used. 18 Screening with cardiac MRI increased the prevalence of clinical and subclinical myocarditis by a factor of 7.4.
A large multicenter cohort study of collegial competitive athletes found a 0.5% prevalence of COVID-19-associated myocarditis in athletes undergoing clinically indicated cardiac MRI, whereas the prevalence was 3.0% when primary cardiac MRI screening was employed. 66
Athletes recovering from COVID-19 may undergo cardiac screening as part of the return-to-play clearance process, including 12-lead electrocardiography, serum cardiac troponin level, transthoracic echocardiography, and cardiac MRI.53,56,66 The rate of cardiac MRI findings of COVID-19-induced myocardial inflammation is approximately 4 times higher if electrocardiography, troponin level, or transthoracic echocardiography are abnormal. 66 A path to manage the cost of cardiac MRI may include using electrocardiography, troponin level, or transthoracic echocardiography as a screening test and cardiac MRI as a confirmatory test.
Adequate cardiac MRI protocols vary but may include morphological short-axis cine and T2-weighted MR images, quantitative T1 and T2 mapping, and delayed contrast-enhanced MRI scans following the intravenous administration of a gadolinium-based contrast agent. 80
Cardiac involvement of COVID-19 infection presents with a spectrum of cardiac MRI findings (Table 1 and Figure 5). Acute myocardial inflammation, such as COVID-19-associated acute myocarditis, typically presents as T2 and short tau inversion recovery (STIR) signal hyperintensity and T1 and T2 value prolongation on quantitative maps. 80 Cine MRI scans may show regional and global wall motion abnormalities in the COVID-19-associated myocarditis and cardiac injury. 80 Quantitative T1 values on regional maps can aid in differentiating areas of myocardial edema and fibrosis. 14 Prolonged T1 relaxation times indicate increased tissue water, typical for myocardial edema. Shortened T1 relaxation times indicate decreased tissue water, typical for myocardial fibrosis. 76 Myocardial fibrosis can be identified as late gadolinium enhancement. COVID-19-associated pericardial abnormalities include pericardial effusion, which manifests as T2 hyperintense water signal interposed between the myocardium and the visible pericardium. Pericardial late gadolinium enhancement may be seen in pericarditis. 14
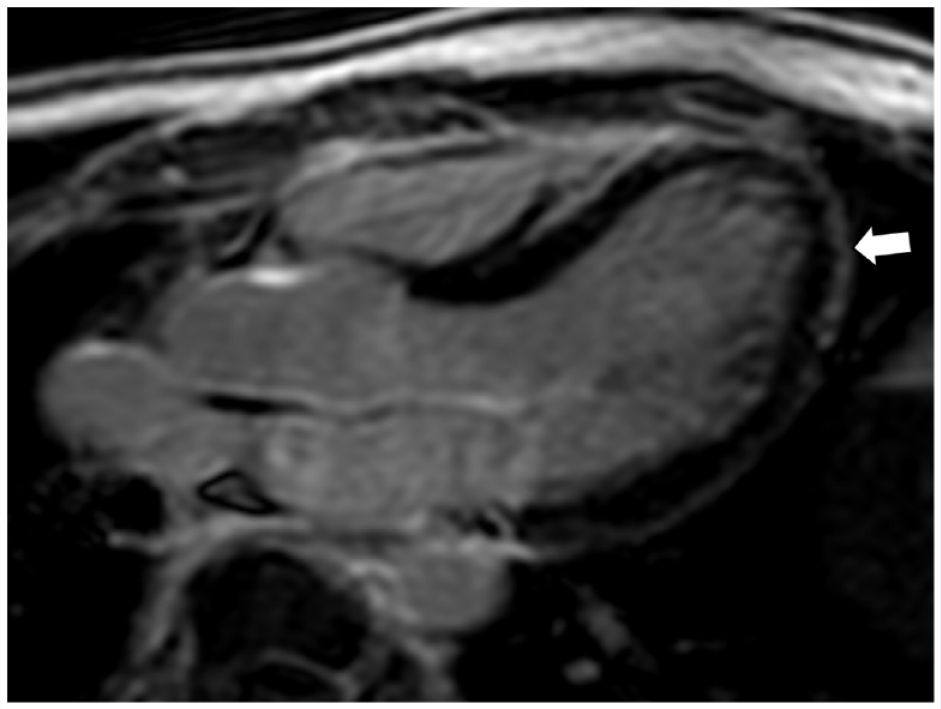
A 19-year-old COVID-19-positive male soccer player with myocarditis. (a) Axial late gadolinium enhancement MRI scan demonstrates linear subepicardial enhancement (arrow).
Cardiac MRI findings in athletes with COVID-19 infection need to be interpreted with caution. In a study including 59 COVID-19-positive athletes, 60 COVID-19-negative athletes, and 27 healthy participants, focal inferoseptal right ventricle insertion late gadolinium enhancement was a common, nondiscriminatory finding attributed to athletic training-related remodeling. 15 Hence, abnormal cardiac MRI findings in COVID-19-positive athletes with a low pretest probability of myocardial inflammation should not be attributed to a COVID-19 infection-induced injury. 43 Guidelines by the European Society of Cardiology and the American College of Cardiology discourage using isolated abnormal cardiac MRI findings to confirm myocarditis.75,77 The Canadian Cardiovascular Society recommends using cardiac MRI to confirm myocarditis in clinically suspicious cases. 59 The European Society of Cardiology guidelines indicate that late gadolinium enhancement in asymptomatic athletes with otherwise normal examinations and tests, including electrocardiogram and stress test, may not constitute a rationale to restrict the return to play. 75
Return-to-play determinations and screening algorithm implementation for athletes recovering from COVID-19 infections are challenging. A cohort study of 30 professional soccer players concluded that comprehensive screening protocols, including resting and stress electrocardiogram, echocardiogram, spirometry, and blood tests, were unnecessary in athletes with asymptomatic or mild COVID-19 infections. 28 Experts of the Leadership Council of the Sports and Exercise Cardiology Section of the American College of Cardiology recommend a gradual approach of increasing training intensity for all athletes after COVID-19 infections, regardless of the severity of the symptoms. 43
Expert opinions, emerging observational data, and publicized reports of competitive athletes with COVID-19-associated cardiac symptoms suggest limited usefulness of return-to-play risk stratification in COVID-19-positive athletes with asymptomatic, mild, and self-limiting symptoms, whereas athletes with moderate or severe COVID-19 infection are recommended to undergo comprehensive return-to-play cardiovascular risk stratification, including clinical evaluation, electrocardiography, troponin level, or transthoracic echocardiography, and in patients with abnormal baseline test results, cardiac MRI or stress testing. 43
Venous thromboembolism is a common vascular complication of COVID-19 infections. A meta-analysis including more than 1 million patients demonstrated a significantly higher risk of venous thromboembolism in COVID-19 patients than non-COVID-19 patients, specifically in intensive care unit settings. 97
Mild COVID-19 infection has also been identified as an independent risk factor for venous thromboembolism. In a case-control study, the odds of venous thromboembolism in mild COVID-19 infection were 1.82 in univariate and 2.62 in multivariate analyses. 16
Elevated alkaline phosphatase and D-dimer, specifically in severe COVID-19 infection, should be considered an indication for further evaluation of thrombotic complications, including deep vein thrombosis. 65
COVID-19-associated endothelial damage, hypoxia, and reduced mobility may contribute to hypercoagulability. A study on 102 hospitalized patients assessing the prevalence of venous thromboembolic disease in patients with COVID-19 and the usefulness of age-adjusted D-dimer cut off values and point-of-care ultrasonography screening found venous thromboembolic disease in 26.5% of the included participants. 4 For a D-dimer level cut off point of 2000 ng/mL, there was a 100% sensitivity and 49.5% specificity for the presence of deep vein thrombosis. For a D-dimer level cut off point of 6000 ng/mL, there was a 100% sensitivity and 67.7% specificity for the presence of pulmonary embolism. Ultrasonography evaluation for deep vein thrombosis may be considered in COVID-19-positive athletes with D-dimer levels of 2000 ng/mL and greater, whereas ultrasonography and pulmonary CT angiography may be considered with D-dimer levels of 6000 ng/mL and greater. Although these cut off values provide high sensitivities, the lower specificity may result in a substantial number of negative ultrasonography and pulmonary CT angiography (false-positive D-Dimer screenings).
Ultrasonography employing B-mode, color and spectral Doppler, and manual augmentation techniques are the first-line diagnostic test for deep vein thrombosis. On ultrasonography, acute or subacute deep vein thrombosis presents absent venous compressibility and optional venous distention, echogenic occlusive or nonocclusive intraluminal clot, minimal or absent centripetal blood flow, and absent or diminished manual augmentation pulse waves (Figure 6). Equivocal ultrasonography evaluation and concern for pulmonary embolism warrant CT or MR venography of the lower extremities.
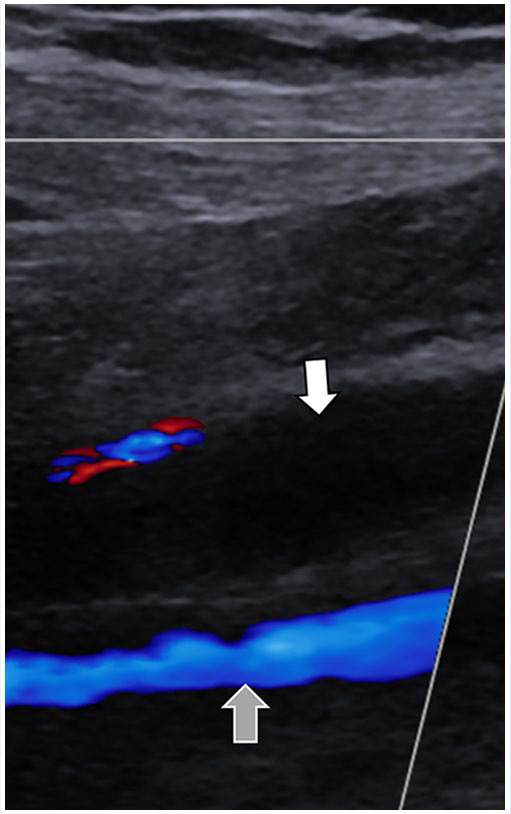
A 29-year-old COVID-19-positive male cyclist presenting with pain and swelling of the right lower extremity. Doppler ultrasonography demonstrates posterior tibial vein thrombosis (white arrow) and normal flow in the subjacent peroneal vein (gray arrow).
In addition to cardiac tests, return-to-play screening regimens may include D-dimer, prothrombin time, and activated partial thromboplastin time levels. 38
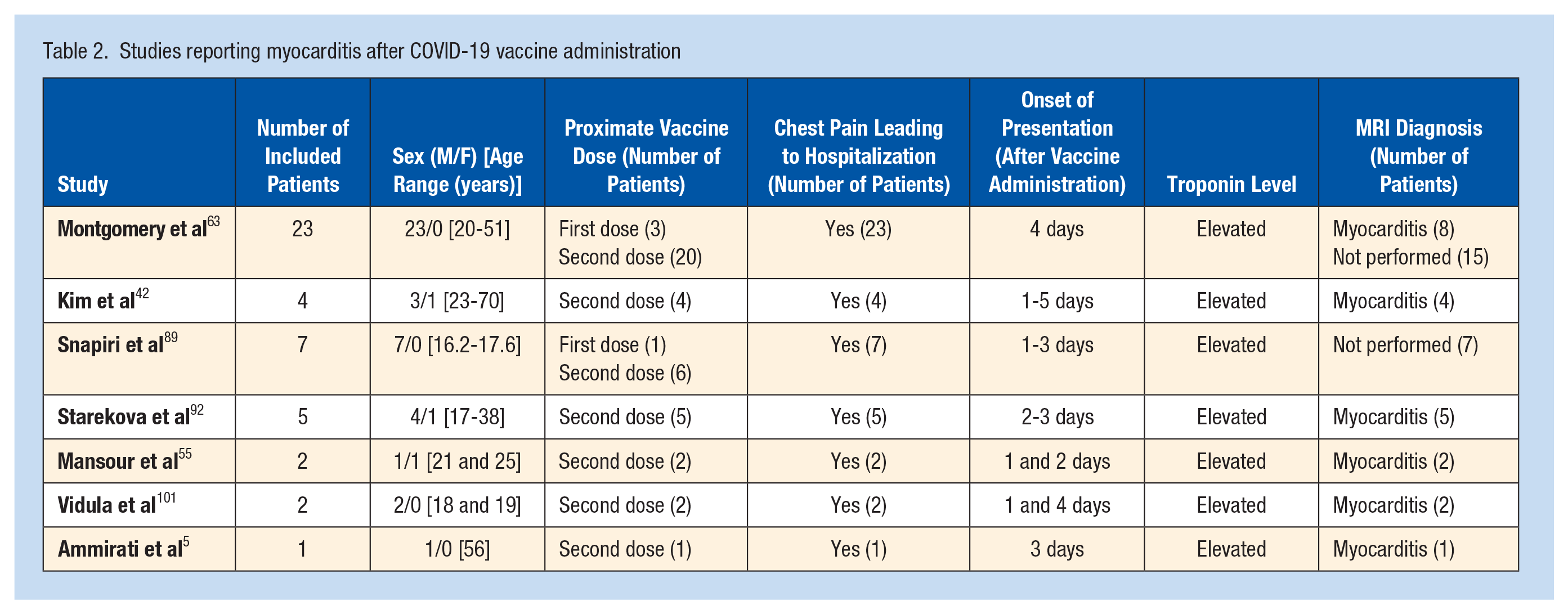
Myocarditis has been described as a complication of mRNA COVID-19 vaccines.5,42,55,63,89,92,101 Among 44 reported patients with mRNA COVID-19 vaccine-associated myocarditis, all patients experienced chest pain within 5 days of vaccine administration and had elevated cardiac troponin levels (Table 2). Of these 44 patients, 4 were diagnosed with myocarditis after receiving the first dose of the vaccine,63,89 whereas 40 were hospitalized following the second dose of mRNA COVID-19 vaccine. All patients who underwent cardiac MRI demonstrated findings supporting the diagnosis of myocarditis. Vaccine-related myocarditis may be considered a differential diagnosis in athletes with cardiac symptoms after COVID-19 vaccination.
Studies reporting myocarditis after COVID-19 vaccine administration
Musculoskeletal System
Myalgia is a common musculoskeletal symptom of systemic viral and COVID-19 infections. 81 Two large meta-analyses reported a prevalence of approximately 22% to 36% in patients with COVID-19.48,112
Case reports associate COVID-19 infections with myositis, rhabdomyolysis, and myonecrosis of skeletal muscles (Figures 7 and 8).3,8,11,25,36,88,90,94,99 Most reported patients were men and presented with myalgia (Table 3). Rhabdomyolysis includes acute skeletal muscle necrosis, leakage of muscle fiber components into the bloodstream, and may cause acute renal failure and death. 61 The diagnosis of rhabdomyolysis is typically based on clinical findings and increased serum creatine kinase. 113
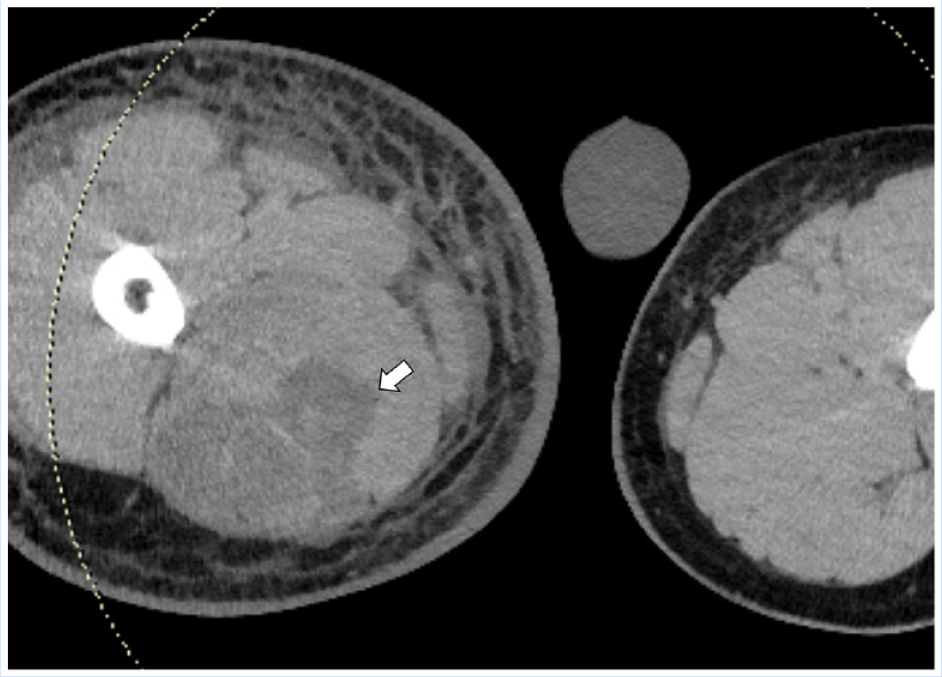
A 23-year-old man with severe COVID-19 disease who developed right thigh swelling. Axial CT image through the upper thigh demonstrates right hamstring myonecrosis (white arrow).
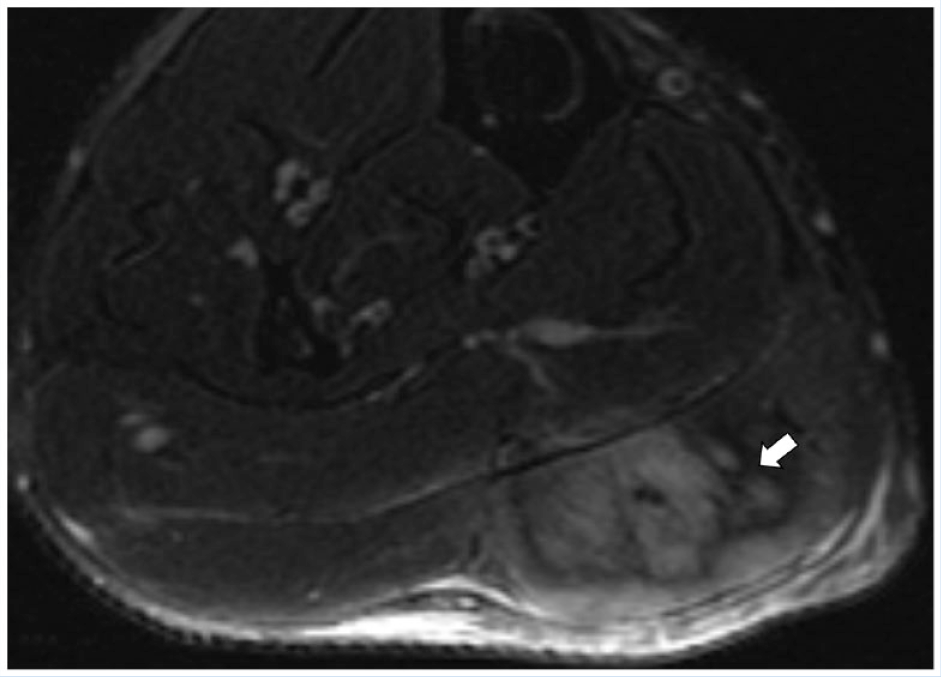
A 25-year-old COVID-19-positive male runner presenting with gradual-onset left calf pain. Axial fat-suppressed fluid-sensitive T2-weighted MR image through the calf shows an area of myonecrosis (arrow) in the medial gastrocnemius muscle.
Studies reporting rhabdomyolysis and myonecrosis in COVID-19 patients
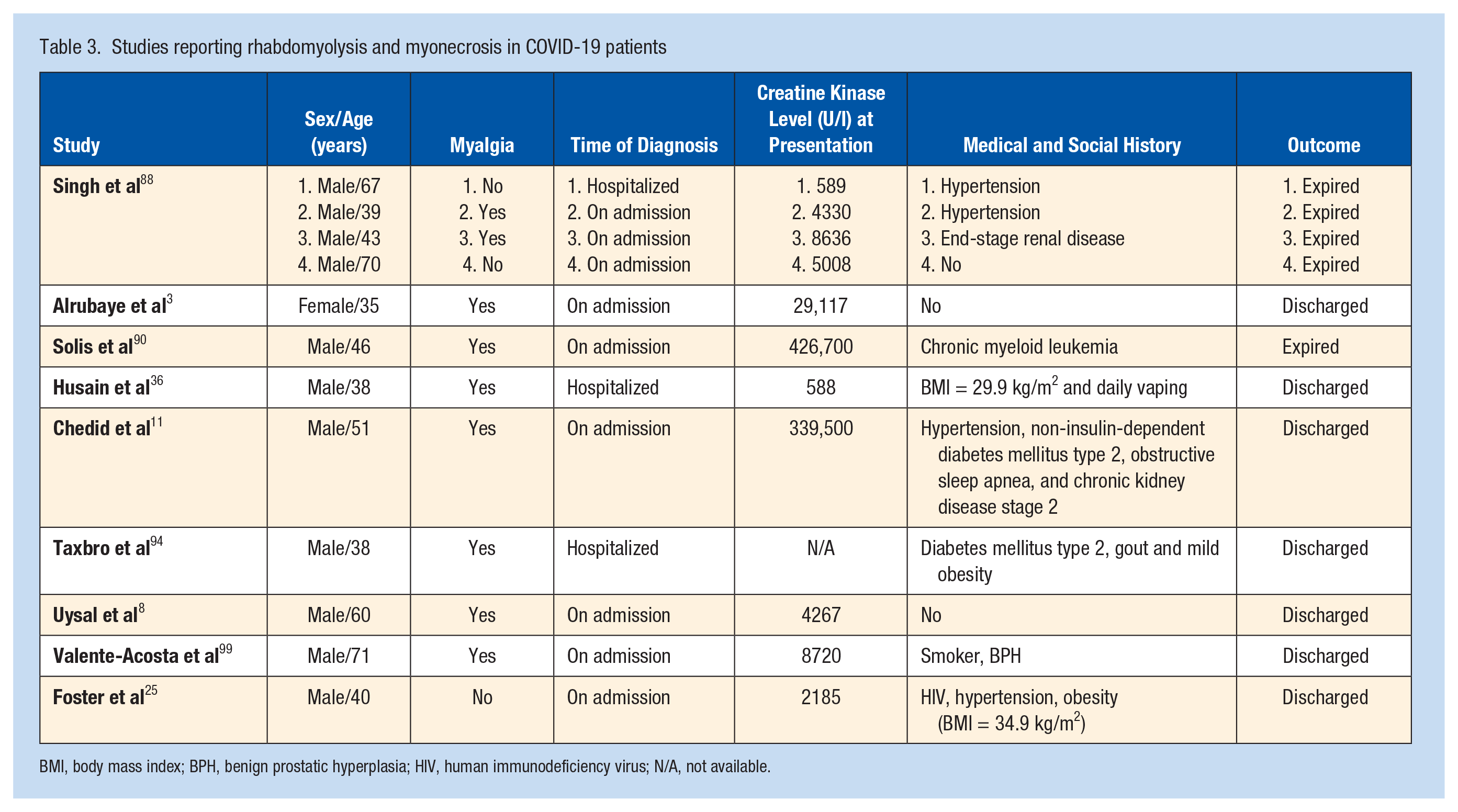
BMI, body mass index; BPH, benign prostatic hyperplasia; HIV, human immunodeficiency virus; N/A, not available.
Imaging can help confirm the presence and characterize the extent of rhabdomyolysis (Table 1). CT scans may demonstrate enlargement and heterogeneous attenuation of affected muscles. 80 Type 1 rhabdomyolysis may present with homogeneously iso- to hyperintense T1 signal, homogeneously hyperintense T2-weighted and STIR signal, and homogeneous gadolinium contrast enhancement. Type 2 rhabdomyolysis may present with homogeneously or heterogeneously iso- to hyperintense T1 signal, heterogeneously hyperintense T2-weighted and STIR signal, heterogeneous CT, and rim enhanced on contrast-enhanced MR and CT images with “stipple sign,” described as dot-like or linear streaky foci within an area of rim enhancement. 51
Diaphragm muscle dysfunction is an important COVID-19-associated complication, described primarily in critically ill and ventilator-dependent patients.30,79 Useful imaging tests to qualitatively assess diaphragmatic muscle dysfunction include the fluoroscopy sniff test and real-time ultrasonography visualization. While the fluoroscopy sniff test gives an immediate and quick evaluation of diaphragm dysfunction, ultrasonography may provide additional information on diaphragm muscle atrophy in a subset of patients.30,79
Arthralgia is another common symptom of systemic viral illnesses and COVID-19. Arthralgia and myalgia often present together, as shown in several studies with a prevalence up to 29%.12,13,111
COVID-19 has been associated with acute monoarticular and polyarticular arthritis.26,73 However, the presentations of the reported patients were more suggestive of activation of reactive or crystal-induced arthritis rather than virus-induced arthritis.19,50,104 Radiography may help detect erosions of advanced arthritis, differentiate types of arthritis based on the distribution patterns, and detect mineralized deposits of crystal-induced arthropathies. MRI may help detect and quantify synovitis and tenosynovitis in patients with negative radiographs and to guide arthrocentesis for fluid analysis.
There is limited information on osseous complications of COVID-19 infection. Reduced bone mineral density has been observed in patients with COVID-19, which may be associated with acute illness and corticosteroid treatment. 21 Osteonecrosis has been observed sporadically in severe COVID-19, similar to SARS, after longer doses of corticosteroids and pressor treatment.29,47 The hypercoagulability associated with COVID-19 and SARS may lead to large-vessel infarction. 70
An investigation focusing on the effects of COVID-19-related home confinement in athletes found 1.13 (95% CI 0.78-1.64) times increased odds for injury and a more than 3 times higher injury rate per game after the COVID-19 lockdown. 86 In young athletes with a history of COVID-19 infection, a study observed decreased aerobic exercise capability and diminished oxygen consumption despite a multimodal training program at home. 20
Peripheral neuropathies are increasingly recognized complications of COVID-19. 24 The differential diagnosis of peripheral nerve injury in patients with COVID-19 includes infection-associated inflammatory neuropathy, positioning-associated stretch and compression injuries, systemic neuropathy, and hematoma-associated nerve entrapment and compression. Affected sites may include the brachial plexus, lumbosacral plexus, and extremity nerves. In patients with respiratory distress, prone positioning increases the risk of brachial plexus injuries by stretching the nerves across the humeral head, compression between the clavicle and the ribs, and compression at the scalene muscles level. 24
Ultrasonography and MRI can be used to confirm a diagnosis of neuropathy, characterize nerve injuries, visualize the extent, and diagnose types of extrinsic compression (Table 1). On ultrasonography, neuropathic nerves typically present thickening, hypoechoic, and decreased visibility of the internal fascicular-type pattern. Magnetic resonance neurography provides a larger field-of-view and higher contrast resolution. Similar to ultrasonography, neuropathic nerves appear thickened and edematous on fat-suppressed fluid-weighted magnetic resonance neurography images. 24
COVID-19 vaccine-related effects and complications affect primarily the shoulder and the regional axillary and retropectoral lymph nodes. Most imaging findings are incidental on musculoskeletal CT, MRI, and ultrasonography examinations for the shoulder, breast, axilla, chest wall, and upper extremity obtained for other reasons and require no action. Normal findings following recent ipsilateral COVID-19 vaccine administration include regional magnetic resonance fluid signal in the deltoid muscle and prominent axillary and retropectoral lymph nodes. Persistent shoulder pain and decreased range of motion the week after the COVID-19 vaccine administration may indicate a vaccine-related shoulder injury related to vaccine administration. The spectrum of imaging findings includes subacromial-subdeltoid bursitis and glenohumeral synovitis with hypertrophy of synovial fronds and, rarely, myonecrosis (Figure 9). 9
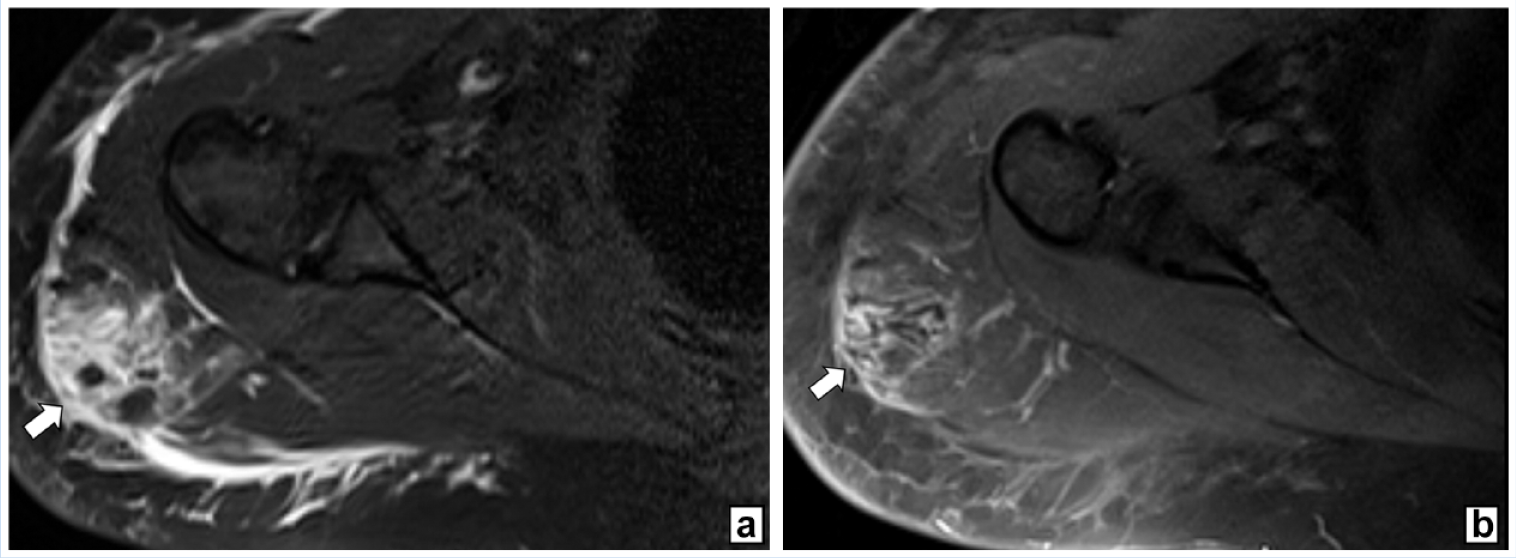
A 30-year-old recreational female athlete presenting with increasing pain and swelling of the right shoulder following Covid 19 mRNA vaccination. (a) Axial fat-suppressed fluid-sensitive T2-weighted MR image through the right shoulder region shows an area of myonecrosis (arrow) characterized by an irregular edema pattern and small interspersed foci of necrotic muscle tissue. (b) Corresponding axial fat-suppressed contrast-enhanced T1-weighted MR image redemonstrates myonecrosis area characterized by irregular enhancement with small nonenhancing foci (arrow). The infection workup was negative.
Neurologic System
COVID-19 infections may affect the central nervous system (CNS) and peripheral nervous system (PNS). Symptoms of CNS involvement include headache, seizure, ataxia, dizziness, and acute cerebrovascular disease, while symptoms of PNS involvement include hypogeusia/ageusia (reduced/loss of taste), hyposmia (reduced smell), anosmia (loss of smell), and Guillain-Barré syndrome. 69
Headache is thought to be the most common symptom of CNS involvement in COVID-19 infections, with a prevalence of up to 23%.69,82 Olfactory and gustatory dysfunction is another common manifestation of COVID-19 infection, presenting 4 to 5 days after other symptoms and lasting 7 to 14 days on average. 85 In a cohort of 6537 patients with COVID-19 from 127 European centers, impaired smell and taste were present in 9% and 13% of patients, respectively. 44 In a systematic review studying olfactory and gustatory dysfunction in patients with COVID-19, anosmia followed by hyposmia and ageusia were the most frequent presentations of olfactory and gustatory dysfunction. 60
Neurologic symptoms and complications in patients with COVID-19 may require evaluation with neuroimaging (Table 1). Approximately one-third of patients with COVID-19 with neurologic symptoms demonstrate brain abnormalities on neuroimaging, including ischemic strokes, meningitis, encephalitis, diffuse leukoencephalopathy, and microhemorrhages (Figure 10).23,45,64,78
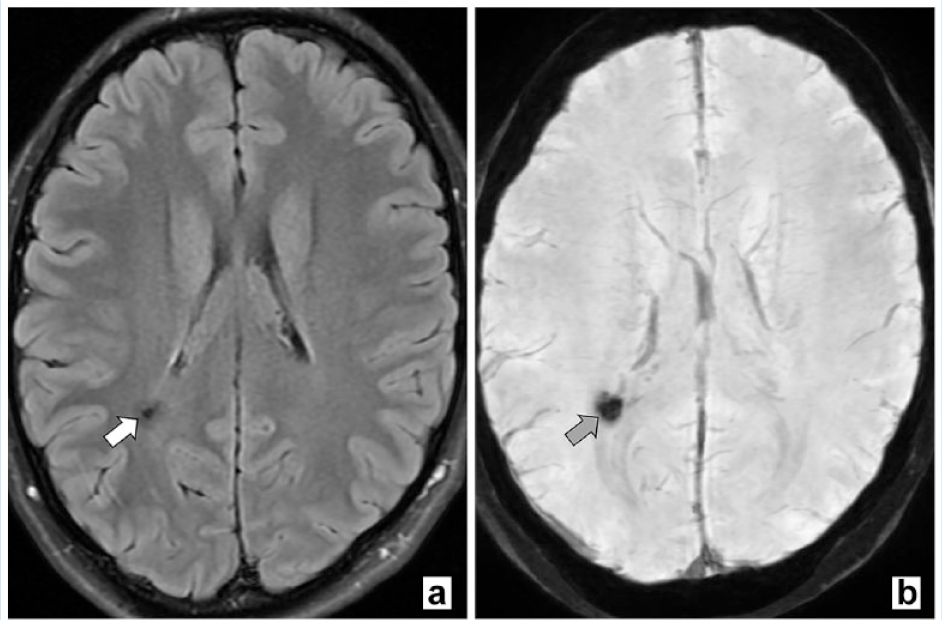
A 21-year-old collegial male runner following COVID-19 recovery presenting with chronic fatigue and headaches. (a) Axial fluid-attenuated inversion recovery and (b) susceptibility-weighted MR images show a focus of chronic microhemorrhage (arrows) within the posterior right corona radiata.
Acute cerebrovascular disease is one of the leading morbidities in patients with severe COVID-19, which may present as acute stroke. 71 Noncontrast-enhanced head CT can detect ischemic and hemorrhagic strokes of the arterial and venous systems. 80 Hypoperfused and infarcted brain tissue is hypoattenuating, resulting in decreased density and loss of gray-white matter differentiation. Retracted clot is hyperattenuating on CT, presenting with increased density, such as intracranial hemorrhage, arterial emboli, and thrombosed venous sinuses (Figure 11). CT and MR venography can confirm cerebral venous sinus thrombosis diagnosis.
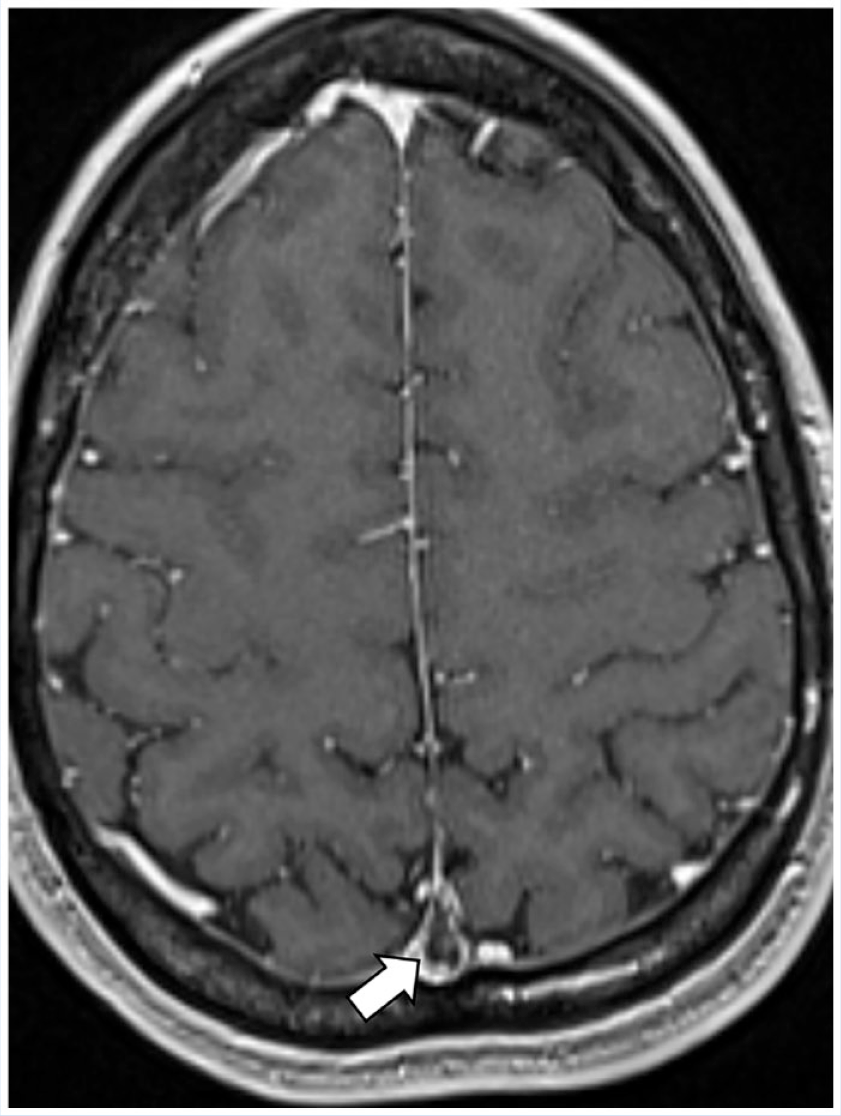
A 27-year-old COVID-19-positive male runner presenting with headaches. Axial fat-suppressed contrast-enhanced T1-weighted MR image redemonstrates nonocclusive sagittal venous sinus thrombosis (arrow).
MRI is most accurate for stroke diagnosis and may be obtained in uncertain cases and for further characterization of etiology and extent of strokes. Native axial T2-weighted fluid-attenuated inversion-recovery (FLAIR) sequence and diffusion-weighted imaging (DWI) with corresponding apparent diffusion coefficient (ADC) mapping are essential pulse sequences of stroke protocols. Typical acute ischemia and infarction patterns include FLAIR signal hyperintensity and restricted diffusion indicated by DWI signal hyperintensity and corresponding hypointensity on the ADC map.2,52 FLAIR signal hyperintensity and restricted diffusion, specifically in insular cortex or temporal lobes, may indicate encephalitis. 80 Contrast-enhanced MRI may be helpful in viral encephalitis.
A study evaluating brain MRI in patients with COVID-19 found medial temporal lobe signal abnormalities in 43%; multifocal nonconfluent white matter lesions with FLAIR signal hyperintensity, abnormal diffusion, and variable enhancement in 30%; and white matter microhemorrhages in 24% of patients. 46 Over 50% of patients presented with intracerebral hemorrhagic lesions, associated with worse clinical outcomes; 24% of patients demonstrated more than 1 neuroimaging pattern.
Guillain-Barré syndrome and Miller-Fisher syndrome are uncommon neurologic presentations in COVID-19 infection. A study evaluating 37 published cases of COVID-19-associated Guillain-Barré syndrome found that, in most patients with Guillain-Barré syndrome, symptoms occurred in the 2nd week of the COVID-19 with a severity similar to that of non-COVID patients (Figure 12). 10 Cerebrospinal fluid assessments showed albuminocytologic dissociation in 76% of patients, whereas the cerebrospinal fluid was negative for COVID virus in all patients. Similarly, a systematic review of COVID-19 patients with Miller-Fisher syndrome found albuminocytologic dissociation without SARS-CoV-2 RNA in 78% of patients. 57
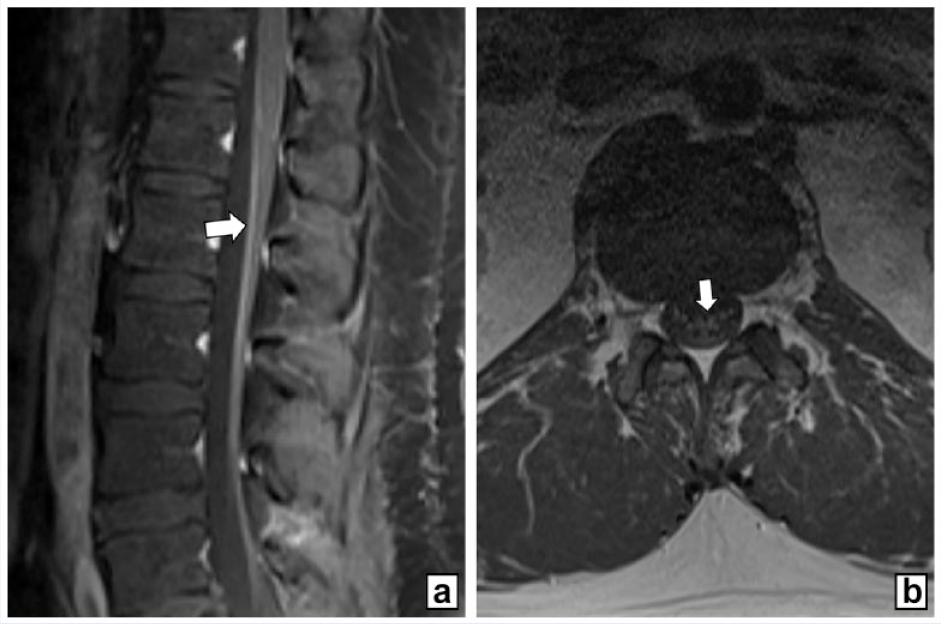
A 26-year-old COVID-19-positive male professional coach presenting with weakness and paresthesia of the lower extremities. (a) Sagittal and (b) axial fat-suppressed contrast-enhanced T1-weighted MRI scans redemonstrate contrast enhancement of the conus medullaris and the anterior cauda equina (arrows), characteristic of the MRI appearance of Guillain-Barré syndrome.
In athletes, data on the impact of COVID-19-associated neurological symptoms are sparse. A study investigating the illness pattern and symptom duration of COVID-19 in 147 athletes described fatigue as the most common symptom. 35 In athletes with symptoms of less than 28 days, 45% had headaches, and 23% had olfactory and gustatory dysfunction. In athletes with prolonged symptoms, 52% had headaches, and 24% had olfactory and gustatory dysfunction.
Rare neurological complications of COVID-19 vaccines have been reported. Cerebrovascular venous thrombosis, intracerebral hemorrhage, and internal jugular vein thrombosis have been associated with adenoviral COVID-19 vector vaccines, including Ad26.COV2.S (Janssen/Johnson & Johnson) and ChAdOx1 nCoV-19 (AstraZeneca). A study including 40 patients found similar mortality for cerebrovascular venous thrombosis after Ad26.COV2.S (Janssen/Johnson & Johnson) and ChAdOx1 nCoV-19 (AstraZeneca) vaccines. 37 However, cerebral venous thrombosis after ChAdOx1 nCoV-19 vaccination occurred later then after Ad26.COV.2.S vaccination, although ChAdOx1 nCoV-19 vaccination was associated with more intracranial hemorrhage and lower d-dimer levels.
A study evaluating vaccine-associated Guillain-Barré syndrome found 130 entries in Vaccine Adverse Event Reporting System (VAERS) following the Ad26.COV2.S (Janssen/Johnson & Johnson) vaccination. 106 A single-center study described 21 cases with neurological autoimmune diseases, including demyelination, inflammatory peripheral neuropathies, cerebral venous sinus thrombosis, myositis, myasthenia, giant cell arteritis, and limbic encephalitis in 232,603 cases after COVID-19 vaccines. 41
Case report descriptions include myoclonus, acute encephalitis, and Sweet syndrome after mRNA-1273 vaccination (Pfizer). 96 Ischemic stroke, facial nerve palsy, and myelitis after ChAdOX1 nCoV-19 vaccination (AstraZeneca) have been reported. 17
Conclusion
SARS-CoV-2 is a novel virus with severe morbidity and mortality, and the new aspects of its complications are still being discovered. While long-term complications of COVID-19 infection are yet to be investigated, a comprehensive understanding of imaging features aids clinicians in determining the most effective patient management and treatment strategies.
Footnotes
The authors report no potential conflicts of interest in the development and publication of this article.