
Abstract
Background:
Patients after anterior cruciate ligament reconstruction (ACLR) have decreased health-related quality of life (QoL) compared with healthy control participants. Few studies have verified the predictors of QoL using Quality of Life Outcome Measure Questionnaire for Chronic Anterior Cruciate Ligament Deficiency (ACL-QoL), and no study has verified the relationship of psychological factors and knee function with ACL-QoL in patients after ACLR.
Hypothesis:
Knee functional status, muscle strength, performance in hop tests, postural stability, and psychological factors would be the predictors of QoL after ACLR.
Study Design:
Cross-sectional study.
Level of Evidence:
Level 4.
Methods:
A total of 131 participants who had undergone ACLR at least 6 months previously were evaluated. QoL was assessed using ACL-QoL; knee functional status, using International Knee Documentation Committee Subjective Knee (IKDC) and global rating scale (GRS); psychological readiness, using Anterior Cruciate Ligament Return to Sport after Injury Scale (ACL-RSI); kinesiophobia, using Tampa Scale for Kinesiophobia (TSK-17); knee strength, using isokinetic dynamometer; performance, using single-leg hop tests; and postural stability, using Biodex Balance System. Pearson’s linear correlation and stepwise hierarchical multiple linear regression analyses were performed to verify the predictors of QoL.
Results:
ACL-QoL showed a moderate correlation with IKDC (r = 0.69), GRS (r = 0.55), ACL-RSI (r = 0.50), and TSK-17 (r = -0.49). ACL-QoL presented none to low correlations with the variables of muscle strength, postural stability, and performance in hop tests. The variables related to the knee functional status and psychological factors (IKDC, GRS, ACL-RSI, and TSK-17) were found to be the predictors of QoL (R2 = 0.56; P = 0.01).
Conclusion:
Knee functional status, psychological readiness, and kinesiophobia were the predictors of knee-related QoL in patients after ACLR.
Clinical Relevance:
These results can assist clinicians in the therapeutic monitoring of the factors that may interfere with QoL in patients after ACLR.
Annual incidence of anterior cruciate ligament (ACL) rupture is 68.6 per 100,000 person years. 41 The main objective of ACL reconstruction (ACLR) is to optimize the health-related quality of life (QoL) of the patient. 22 QoL pertains to how the patient perceives his or her health status and also nonhealth-related elements, such as work, family, friends, and other life circumstances. 15
Patients after ACLR have decreased QoL compared with healthy control participants. 17 QoL is generally measured by the Knee Injury and Osteoarthritis Outcome Score (KOOS), 36-Item Short Form Health Survey (SF-36),1,6,10,24 and International Knee Documentation Committee Subjective Knee (IKDC). 40 These questionnaires do not specifically assess QoL in patients who have incurred an ACL injury. Only 1 of the 14 studies included in the systematic review used a specific questionnaire to assess QoL in patients with ACL injuries.12,30 Patients assessed using a knee-specific measure (KOOS-QoL) report poorer QoL values than those assessed using a generic QoL measure (SF-36). 12 Furthermore, while the Quality of Life Outcome Measure Questionnaire for Chronic Anterior Cruciate Ligament Deficiency (ACL-QoL) considers 5 domains with 31 questions, 43 the KOOS-QoL is a subscale of the KOOS that is composed of only 5 questions. 37 Therefore, ACL-QoL can contribute to a real understanding of QoL in patients with ACLR.
ACL-QoL is the specific tool used for assessing QoL in patients with an ACL injury. 43 There was no difference between the ACL-QoL scores of men and women with patellar tendon graft 5 years after ACLR. 30 Not returning to the sport, a higher body mass index (BMI), subsequent knee surgery, and contralateral ACLR were found to be associated with worse ACL-QoL scores. 11 These factors, combined with sex, age, surgery revision, and years since ACLR, accounted for 36% of the ACL-QoL score variation 5 to 20 years after ACLR.
Investigating the factors related to the QoL of patients after ACLR can assist in the development of specific strategies to optimize the clinical outcomes in this population. Few studies have verified the predictors of QoL using ACL-QoL, and no study has verified the relationship of psychological readiness, kinesiophobia, and knee function (eg, muscle strength, performance in hop tests, and postural stability) with ACL-QoL in patients after ACLR.11,47 Therefore, this study was conducted to verify the relationship of knee functional status, muscle strength, performance in hop tests, postural stability, psychological readiness and kinesiophobia with QoL in patients after ACLR.
Methods
Study Design
A cross-sectional study was conducted at the Human Movement Analysis Laboratory at the Federal University of Ceará from August 2018 to July 2019. The data were reported according to the Strengthening the Reporting Observational Studies guidelines. 21 The study was approved by the Research Ethics Committee of the Federal University of Ceará (protocol number: 1000404), and all the participants signed a written consent form.
Sample
Participants were recruited in the university hospital, outpatient and orthopedic, trauma, and sports clinics. Eligibility criteria are described in Figure 1. Concomitant injuries such as meniscal and chondral lesions, and adjacent ligament injuries already treated were allowed as long as they did not prevent the performance of the tests or the sports practice. Pain, range of motion deficit, and swelling (see Figure 1) were potential confounding factors for the variables analyzed in this study.
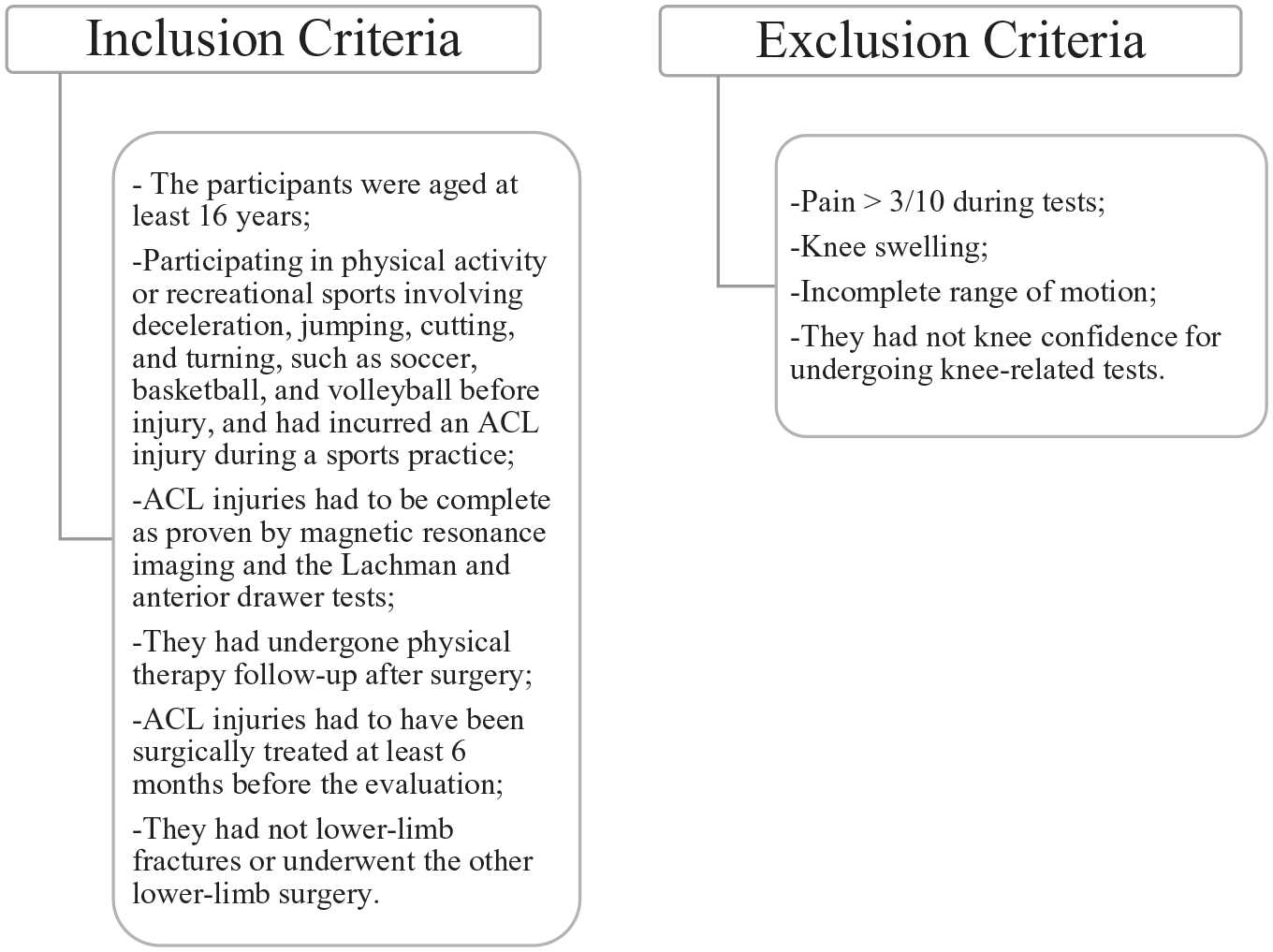
Eligibility criteria. ACL, anterior cruciate ligament.
Data Collection
Anthropometric, demographic, and clinical characteristics were collected through an evaluation form. The Tegner activity scale was used to determine the level of physical activity. 45 The before and after injury results of the Tegner activity scale were included. The QoL was assessed using ACL-QoL; knee functional status, using IKDC and global rating scale (GRS); psychological readiness, using Anterior Cruciate Ligament–Return to Sport after Injury Scale (ACL-RSI); kinesiophobia, using Tampa Scale for Kinesiophobia (TSK-17); knee strength, using isokinetic dynamometer; performance, using single-leg hop tests; and postural stability, using Biodex Balance System. The 3 evaluators in the study had 2 years’ experience in conducting the aforementioned tests. Meetings were held before the study for the training and standardization of the assessment.
Patient-Reported Outcome Measures
ACL-QoL contains 31 items divided into 5 domains: symptoms and physical complaints, work-related concerns, recreation activities, sports participation or competition, and lifestyle and social and emotional aspects. 43 IKDC contains 10 items divided into 3 domains: symptoms, function, and sports activity. 23 ACL-RSI contains 12 questions divided into 3 domains: emotions, performance, and risk assessment. 43 ACL-QoL, IKDC, and ACL-RSI scores range from 0 to 100 points, with 100 indicating the best score.23,43 TSK-17 contains 17 questions and the scale ranges from 17 to 68 points. A high score represents greater fear of movement/(re)injury. 44 All the questionnaires were translated and validated into Brazilian Portuguese.23,43,44 The GRS of perceived function contains 100 percentage points, where 0% means “unable to perform any activity” and 100% means “able to perform all pre-injury activities, including sports, without limitation.” 18
Knee Strength
The isokinetic dynamometer (Biodex Multi-Joint System Pro Biodex Medical System, Shirley, New York) was used to assess the torque of the quadriceps and hamstrings. Each participant was made to sit on a chair, with the popliteal fossa positioned 2 cm from the end of the seat, the hip positioned at 85° of flexion and the lever arm was positioned at 2 cm above the lateral malleolus. The protocol consisted of 5 and 15 concentric contractions at maximum speeds of 60º/s and 300º/s, respectively. The peak torque values were normalized by the weight of each participant (Nm/kg), and the limb symmetry index (LSI) was calculated. 3 The isokinetic dynamometer is considered a gold standard method for evaluating the muscle strength9,32 and is widely used as return-to-sport (RTS) criteria after ACLR. 35
Performance in Hop Tests
The participants were made to do a 5 min warm-up exercise on the stationary bike and then to perform 4 hop tests: single hop for distance, triple hop for distance, crossover hop for distance, and 6-m timed hop. The participants performed 1 to 2 practice trials followed by 2 recorded trials. The test was started with the nonoperative lower limb.27,28 If the patients lost their balance, they were made to hop again. To calculate the LSI for the hop tests for distance, the mean of the operative limb was divided by the mean of the nonoperative limb, and the result was multiplied by 100. 24 For the 6-m timed hop, the patient performed single-leg hops covering a distance of 6 m in the shortest possible time. The mean of the nonoperative limb was divided by the mean of the operative limb, and the result was multiplied by 100 for the 6-m timed hop. 28 The coefficients of interclass reliability for the tests were as follows: single hop test, 0.92 to 0.96; triple hop test, 0.95 to 0.97; crossover hop test, 0.93 to 0.96; and timed hop test, 0.66 to 0.92.8,38
Postural Stability
The Biodex Balance System (Biodex Medical System, Shirley, New York) was used to assess the overall stability index (OSI). Five stability levels were tested on the platform. For each repetition, the test began with a level less unstable (level 6) and ended with a level more unstable (level 2). After the practice trials, the evaluation was carried out in 3 20-s sets with 10 s rest intervals. Each participant was instructed to stand barefoot on 1 leg, with the arms at the sides of the body, the knee of the assessed limb flexed to 10º, and the eyes facing the screen. Smaller values indicated better stability. 4 The intratester reliability was 0.82 and 0.99 and the intertester reliability was 0.70 for OSI.39,42
Statistical Analysis
The Kolmogorov-Smirnov test was used to verify the normality of the data distribution. Descriptive analysis was performed for the numerical variables. The nominal variables were presented in absolute numbers and frequencies.
Pearson’s correlation coefficient was used to check the strength of the association between the dependent measure (ACL-QoL) and the independent measures (IKDC, GRS, ACL-RSI, TSK-17, quadriceps and hamstrings strength LSI at 60°/s and 300°/s, OSI of the operative limb, and LSI for the single hop, triple hop, crossover hop, and 6-m timed hop tests). These 13 variables were selected because they are usually evaluated in patients who wish to RTS at the end of the physical therapy rehabilitation process. The Pearson’s correlation coefficient was interpreted according to the following guide: 0 to 0.19 = none to slight; 0.20 to 0.39 = low; 0.40 to 0.69 = moderate; 0.70 to 0.89 = high; and 0.90 to -1 = very high. 46
Stepwise hierarchical linear multiple regression analyses were then performed with the independent variables that presented Pearson’s linear correlation with a value of P ≤ 0.10 to estimate the proportion of variance of ACL-QoL. The normality, linearity, and homoscedasticity assumptions were confirmed through the observation of both the normality probability plots of the regression standardized residual plots and the standardized residuals versus the regression standardized predicted value scatterplots. Multicollinearity was defined as Pearson’s correlation coefficient ≥0.7 between 2 variables.
The regression equation was constructed using nonstandardized regression coefficients (β), and the predictive power of each final model was determined by calculating the percentage of explained variance (R2). The data were analyzed using the SPSS 24.0 program (Statistical Package for the Social Sciences Inc, Chicago, IL), with the significance value set at 5%.
Sample size calculation was performed using G-Power (Dusseldorf, Germany). A total of 89 patients were needed to detect 13 possible predictors of QoL using linear multiple regression, with a 5% significance level and 95% power, and employing a medium effect size (f 2 = 0.15). Another 42 participants were included due to the great demand.
Results
A total of 284 potential participants was contacted, but 139 were excluded because they did not meet the eligibility criteria (Figure 2). Of the 145 participants, 14 (9.6%) were removed from analysis (see Figure 2). The clinical characteristics of the 131 participants are listed in Tables 1 and 2. Furthermore, 27 participants (20.6%) underwent meniscus suture; 23 (17.6%) meniscectomy; 3 (2.30%) medial collateral ligament reconstruction; 1 (0.80%) posterior cruciate ligament reconstruction; and 1 (0.8%) microfracture surgery.
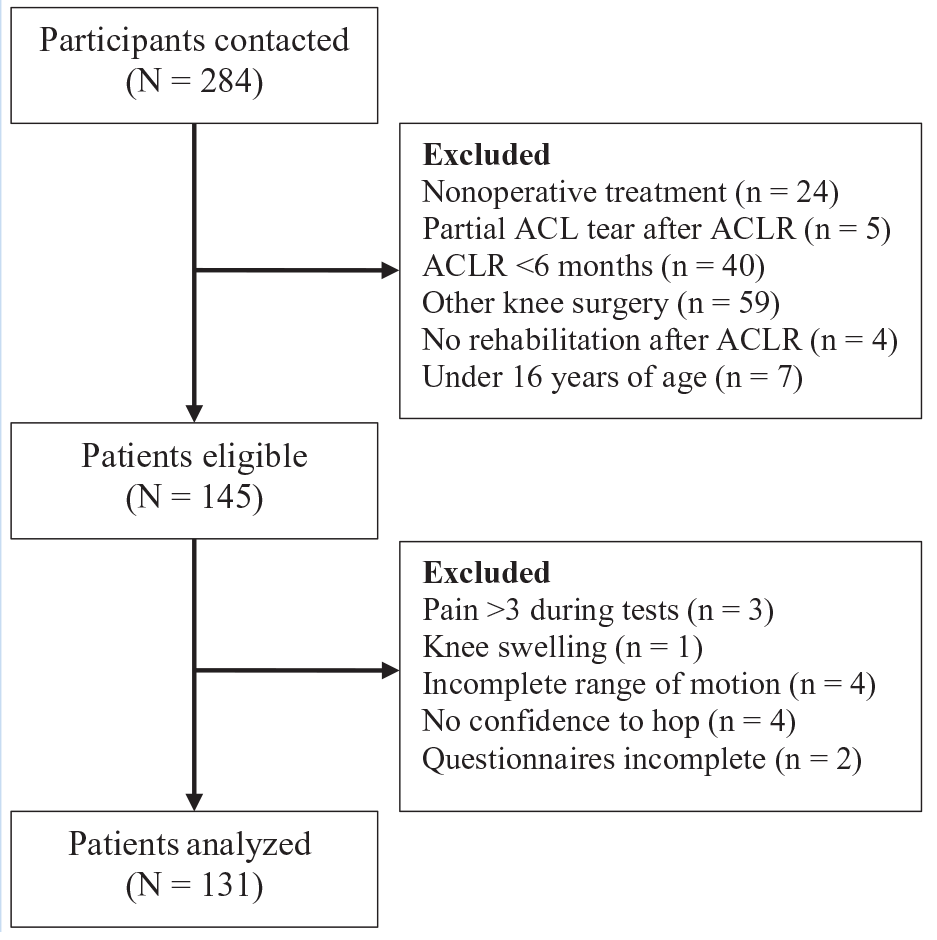
Recruitment flow chart. ACLR, anterior cruciate ligament reconstruction.
Clinical and anthropometric characteristics of research participants (n = 131)
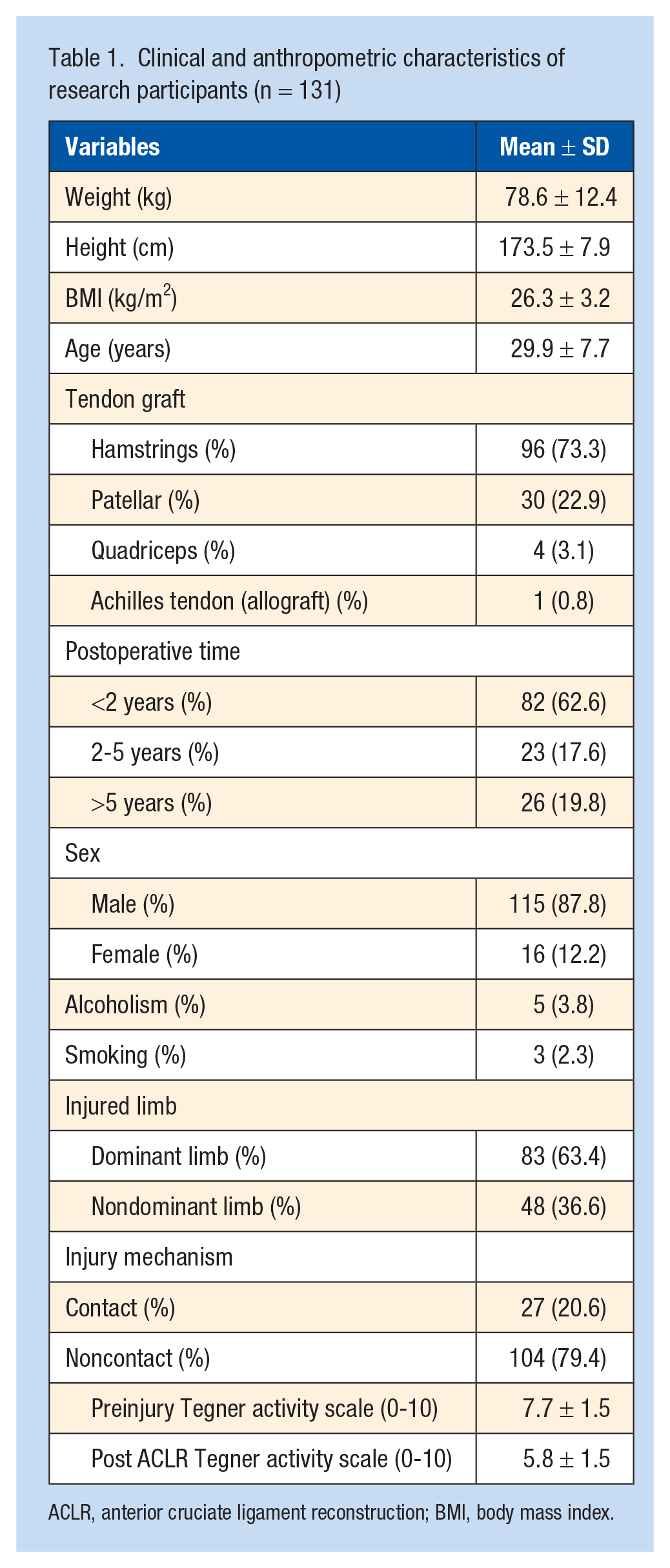
ACLR, anterior cruciate ligament reconstruction; BMI, body mass index.
Knee-related QoL, function, psychological factors, strength, performance, and postural stability after ACLR (n = 131)
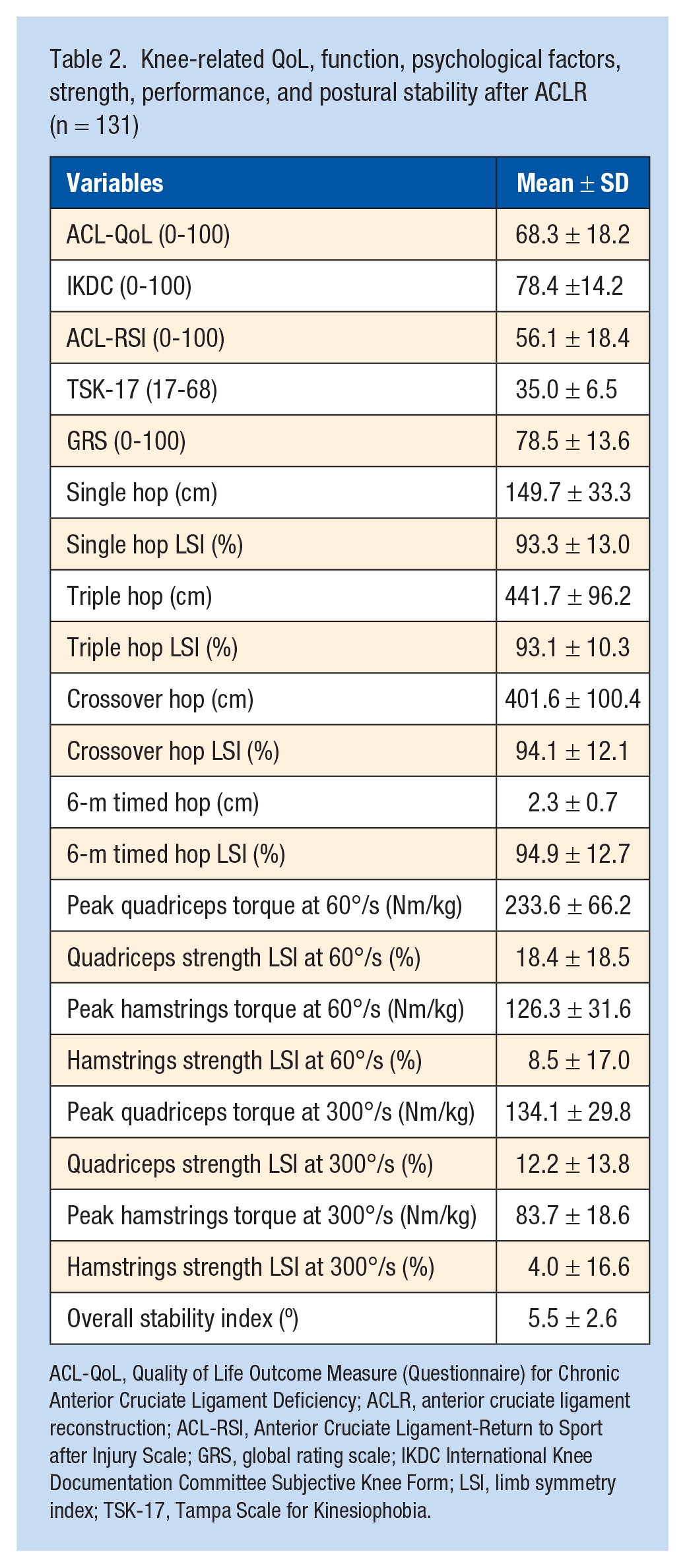
ACL-QoL, Quality of Life Outcome Measure (Questionnaire) for Chronic Anterior Cruciate Ligament Deficiency; ACLR, anterior cruciate ligament reconstruction; ACL-RSI, Anterior Cruciate Ligament-Return to Sport after Injury Scale; GRS, global rating scale; IKDC International Knee Documentation Committee Subjective Knee Form; LSI, limb symmetry index; TSK-17, Tampa Scale for Kinesiophobia.
ACL-QoL showed a moderate direct correlation with IKDC (r = 0.69), GRS (r = 0.55), ACL-RSI (r = 0.50), and a moderate inverse correlation with TSK-17 (r = -0.49). It presented none or low correlation with muscle strength, postural stability, and performance in the hop tests (Table 3).
Correlation between ACL-QoL and function, psychological factors, strength, performance, and postural stability (n = 131)
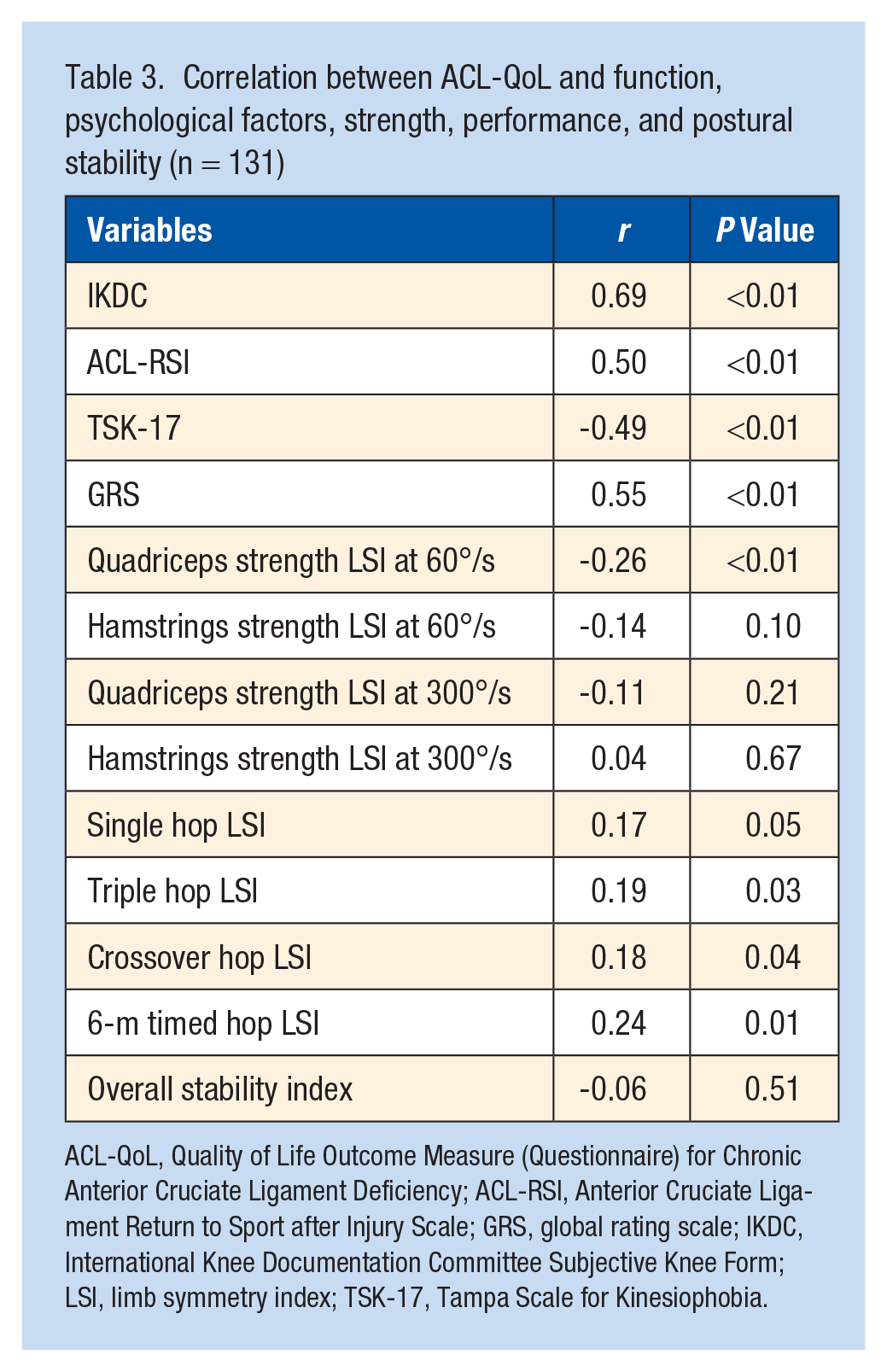
ACL-QoL, Quality of Life Outcome Measure (Questionnaire) for Chronic Anterior Cruciate Ligament Deficiency; ACL-RSI, Anterior Cruciate Ligament Return to Sport after Injury Scale; GRS, global rating scale; IKDC, International Knee Documentation Committee Subjective Knee Form; LSI, limb symmetry index; TSK-17, Tampa Scale for Kinesiophobia.
IKDC, GRS, ACL-RSI, TSK-17, quadriceps and hamstrings strength LSI at 60°/s, and LSI for the single hop, triple hop, crossover hop, and 6-m timed hop tests were included in the multiple linear regression analysis of ACL-QoL after the analysis of the prerequisites for inclusion in the model (Table 4). In the final model, the variables IKDC, GRS, ACL-RSI, and TSK-17 were the predictors of QoL, explaining 56% of the QoL variation assessed by ACL-QoL (R2 = 0.56; P = 0.01). IKDC explained the highest proportion of the ACL-QoL score variation (β = 0.43; P < 0.01). The indices of the isokinetic-strength assessment and single-leg hop test results were not included in the model generated for P > 0.05.
ACL-QoL multiple linear regression analyses
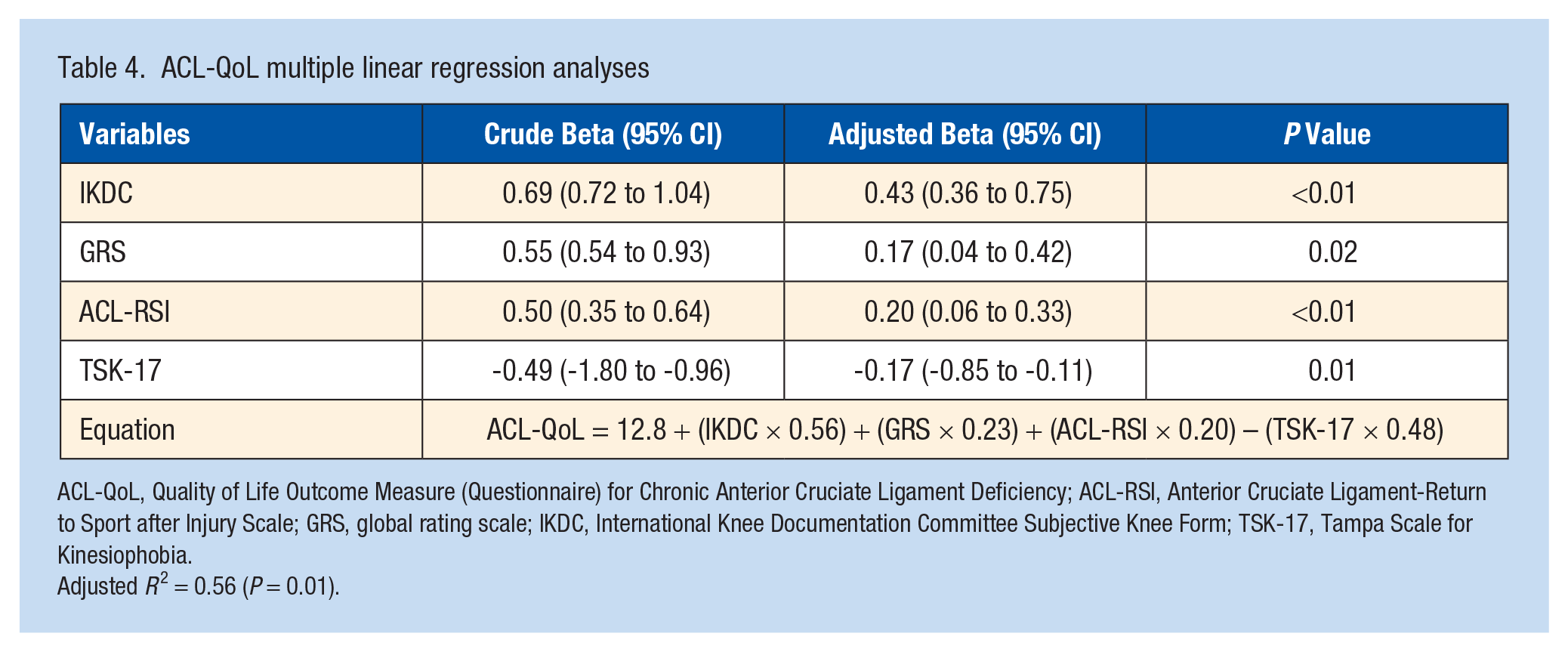
ACL-QoL, Quality of Life Outcome Measure (Questionnaire) for Chronic Anterior Cruciate Ligament Deficiency; ACL-RSI, Anterior Cruciate Ligament-Return to Sport after Injury Scale; GRS, global rating scale; IKDC, International Knee Documentation Committee Subjective Knee Form; TSK-17, Tampa Scale for Kinesiophobia.
Adjusted R 2 = 0.56 (P = 0.01).
Discussion
The main objective of this study was to verify the relationship of knee functional status, psychological factors, muscle strength, performance in hop tests, and postural stability with QoL in patients after ACLR. The patient-reported outcome measures related to functional status and psychological factors showed a moderate correlation with QoL after ACLR, being responsible for 56% of the ACL-QoL score variation. The factors related to RTS, higher BMI, subsequent knee surgery, contralateral ACLR, sex, age, surgery revision, and years since ACLR explained only 36% of the ACL-QoL score variation. 11 Performance in hop tests, muscle strength, and postural stability were not related to QoL in this population.
This study showed that both instruments used for assessing knee functional status are associated with knee-related QoL. Total score of IKDC was the main predictive variable for QoL in patients after ACLR, by itself explaining 43% of the ACL-QoL score variation. Sánchez Romero et al 40 used IKDC to measure QoL and showed that a better IKDC score was associated with male sex and sports-associated injury in patients with ACL injury, but was not associated with bone bruise, surgical or conservative treatment and concomitant ligament injuries. Williams et al 47 used the 2-factor structure of IKDC (symptoms and knee articulation and activity level) and found that the symptoms and knee articulation construct of IKDC have a significant association with ACL-QoL 6 months and 2 to 9 years after ACLR.
GRS was the second predictive variable for QoL. Although it has a good correlation with IKDC, 19 the authors did not find any study that verified its correlation with QoL. Núñez et al 29 found an association between the IKDC and SF-36 scores in patients 2 years after ACLR, while Möller et al 24 found no correlation between the Lysholm scale and SF-36. This study highlights that the choice of instruments for assessing knee functional status and QoL could impact the results and interpretation.
Psychological readiness has been identified as an important factor to be assessed for RTS after ACLR.2,33 Patients who have returned to their preinjury activities reported greater psychological readiness assessed by ACL-RSI and higher QoL assessed by ACL-QoL and the KOOS-QoL subscale. 5 ACL-QoL involves questions about emotional/psychological aspects; therefore, ACL-RSI has a moderate correlation with ACL-QoL. 43
Fear associated with movement has an impact on the functionality and RTS of patients after 1 ACLR.5,10,16,26 The authors found that the TSK-17 (kinesiophobia) explains the ACL-QoL score variation and that there is a moderate inverse correlation between these 2 scales. Corroborating our results, Kvist et al 20 found that kinesiophobia has a moderate inverse correlation with QoL after ACLR. Furthermore, a qualitative study demonstrated that fear of a new injury influences QoL in people up to 20 years after ACLR. 13 Clinicians should be aware of the development of kinesiophobia in the period after ACLR.
The variables of muscle strength, postural stability, and performance in hop tests presented none to low correlations with ACL-QoL, and these variables were found to be nonpredictors of the ACL-QoL score. QoL is a broad construct and depends on other factors perceived by the patient regardless of muscle strength, postural stability, and performance in hop tests. 15 Our sample was mostly composed of recreational athletes (Tegner before injury = 7.7 and Tegner after injury = 5.8). RTS at the same level and performance-based test probably has a lower impact on the perceived QoL in recreational athletes.14,24 Perhaps performance-based tests have greater impact on the QoL in professional/competitive athletes aiming to RTS at the same preinjury level.
No correlation was also found between quadriceps LSI and the KOOS-QoL subscale, 34 and between knee extension and flexion torque in the isokinetic dynamometer and the KOOS-QoL subscale 2 and 4 years after ACLR.14,23 Patterson et al 31 and Möller et al 24 also found no association between LSI in the hop tests and QoL. Furthermore, patients after ACLR have demonstrated poorer balance stability during single-leg stance than healthy controls, 25 and it has been associated with RTS at the same preinjury level. 2 However, previous studies7,36 found no correlation between QoL assessed by KOOS-QoL subscale and postural stability assessed by anterior direction symmetry of the Y Balance Test and the mean speed of the center of pressure.
Our study had major limitations: (1) the patients’ postoperative rehabilitation process was not controlled, (2) it was not possible to determine the impact of the analyzed variables on long-term QoL as the study was a cross-sectional one, and (3) the follow-up in some patients was only 6 months, far too short to make QOL assessments.
Conclusion
Knee functional status, psychological readiness, and kinesiophobia were the predictors of knee-related QoL in patients after ACLR, explaining 56% of its variation. IKDC was the major predictor of the ACL-QoL score variation. These results can assist clinicians in the therapeutic monitoring of the factors that may interfere with QoL in patients after ACLR.
Footnotes
The authors report no potential conflicts of interest in the development and publication of this article.
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was financed in part by the Coordenação de Aperfeiçoamento de Pessoal de Nível Superior - Brasil (CAPES) - Finance Code 001.