
Abstract
Background:
Preseason movement screening can identify modifiable risk factors, deterioration of function, and potential for injury in baseball players. Limited resources and time prevent high school baseball coaches from performing movement screens on their players.
Hypothesis:
The arm care screen (ACS) will be highly sensitive to detecting musculoskeletal risk factors.
Study Design:
Cross-sectional.
Level of Evidence:
Level 3.
Methods:
A total of 150 baseball players were independently scored on the ACS electronically by reviewing a video recording of each player’s screening performance. Discriminability of the ACS was determined with a 2 × 2 contingency table dichotomizing musculoskeletal risk factors as present or absent based on a predetermined cutoff value and those who passed or failed the corresponding ACS subtest.
Results:
High sensitivity was observed on the reciprocal shoulder mobility (0.89; 95% CI 0.81-0.94), 90/90 total body rotation (0.86; 95% CI 0.79-0.92), and lower body diagonal reach (0.85; 95% CI 0.78-0.91) tests of the ACS suggesting sufficient ability to identify musculoskeletal impairments and risk factors.
Conclusion:
The ACS is a simplistic screening tool that the coach can administer to discriminate between youth, high school, and college-level baseball players who possess musculoskeletal risk factors. The ACS subtests demonstrated high sensitivity for correctly identifying musculoskeletal risk factors common in baseball players and can be useful as a screening tool for baseball coaches developing arm care exercise programs.
Clinical Relevance:
A field-expedient screen could provide coaches the ability to identify musculoskeletal risk factors that need to be addressed to minimize injury risk factors in a time-efficient manner.
The incidence of shoulder and elbow injuries in baseball players of all age levels has continued to rise over the past several decades.4,6,33 Despite the development of pitch count and rest guidelines, nontraumatic musculoskeletal injuries due to overuse account for a large proportion of baseball-related arm injuries. 45 To mitigate overuse arm injuries, baseball coaches implement arm care programs to target musculoskeletal injury risk factors by improving strength, dynamic stability, and range of motion (ROM) of muscles and joints.20,22 However, these arm care programs tend to be more generalized, as identification of specific injury risk factors in each player is difficult for coaches without an athletic trainer or physical therapist (PT) on staff. 24
Identification of key musculoskeletal risk factors is critical for proper arm care exercise programming and reduction of injury incidence rates. Researchers have identified several intrinsic risk factors throughout the kinetic chain which can lead to the development of injury. Although some intrinsic risk factors such as age 12 and height 12 are nonmodifiable, many intrinsic risk factors can be managed with intervention. Musculoskeletal risk factors such as glenohumeral internal rotation deficit (GIRD),3,37,38 limited hip internal rotation (IR)30,35 and external rotation (ER) ROM, 11 decreased thoracic spine mobility, 31 asymmetrical shoulder total ROM (TROM),3,7,38 and poor dynamic single-leg balance 34 can place increased stress on the throwing arm. Typically, these risk factors manifest before the onset of injury and can be modified with arm care exercise programs.1,32,39
Injury risk factors could be more appropriately managed with more accurate and frequent musculoskeletal screening for early identification of risk factors, 40 but to do so takes time and resources that may not be available to all competitive levels. The identification of players who possess specific risk factors or impairments is more challenging for youth, high school, or college-level baseball coaches without a sports medicine staff or resources. 9 Furthermore, baseball coaches typically lack the training or time to remeasure the ROM of multiple joints throughout the season in an attempt to monitor the development of risk factors. 8 Recently, a 2-min equipment-free screening tool based on the principles of the Functional Movement Systems called the arm care screen (ACS) has demonstrated excellent intra-rater (k = 0.76; 95% CI 0.54-0.95) and inter-rater (k = 0.89; 95% CI 0.77-0.99) reliability among high school baseball coaches. 21 The simplicity of the ACS tests and scoring criteria is convenient for coaches without readily available access to a rehabilitation professional, but the diagnostic value of the screening tool to identify potential risk factors is unknown.
To date, there are no studies that have explored the discriminant validity of a field-expedient screening tool that baseball coaches can use accurately to identify musculoskeletal mobility and balance risk factors across different age levels. The purpose of this study is to investigate the accuracy of the ACS to detect common musculoskeletal risk factors in baseball players. It was hypothesized that poor performance on the ACS subtests would be highly sensitive at detecting the presence of at least one associated musculoskeletal risk factor in youth, high school, and college-level baseball players.
Methods
Study Design
A prospective cross-sectional design was used to establish the discriminability of the ACS to identify the presence of musculoskeletal risk factors among a cohort of baseball players. The Standards for Reporting Diagnostic Accuracy Studies (STARD) statement for a diagnostic accuracy study design was followed for standardized reporting. Approval was granted from the institutional review board at the University of Kentucky, and informed consent and assent forms were obtained before data collection.
Participants
Based on an expected participant injury risk factor prevalence of 75%, a minimum sample size of 46 players would be needed to detect a sensitivity of 0.90 on the ACS with a 0.10 CI width. 2 Anticipating a moderate effect size of 0.4, a sample of 49 participants in each group would have 80% power to detect an association between ACS failure and the presence of musculoskeletal risk factors at an alpha of 0.05 for a 2-tailed test. Therefore, the minimal accrual target was 49 participants in each group for a final sample size of 147 baseball players.
A convenience sample of 150 male baseball players (youth, n = 50; high school, n = 50; college, n = 50) volunteered to participate in this study. The head coaches allowed the researchers to attend team workouts to recruit and test the players. Inclusion criteria required the participant to be a current and active member of a men’s youth, high school, or college baseball team. Exclusion criteria included the inability to participate in sport due to current injury, recent surgery (within] 3 months), medical restriction from sports participation, recent concussion (within 1 month) or vestibular issue. Players under the age of 11 years or older than 25 years were excluded.
Procedures
Data collection occurred over 6 months during fall and winter off-season team workouts. Physical testing occurred during a single session before practice. Participants completed a demographic questionnaire that included information about their age, height, weight, playing position, baseball experience, and current injury status. All participants underwent ACS testing, ROM measurements of the shoulders, hips, thoracic spine, and dynamic balance testing.
The ACS
The ACS is a modified movement-based screening tool that utilizes components of the Functional Movement Systems developed to improve field expediency and reduce scoring complexity. The ACS consists of 3 subtests including (1) reciprocal shoulder mobility, (2) 90/90 total body rotation, and (3) lower body diagonal reach (Figure 1).
Reciprocal shoulder mobility: While standing with feet together, the athlete simultaneously reaches one hand behind his head and the other hand behind and up his back. Maintaining a tall posture, the athlete attempts to touch the fingertips of both hands together. A positive test is defined as the inability to touch fingertips together on one or both sides.
90/90 total body rotation: Standing with feet together and arms in the 90/90 position, the athlete rotates his entire body including his hips, shoulders, and head as far as possible keeping the feet pointed straight ahead. The test is considered positive if the coach is unable to see the front of the opposite shoulder while the athlete maintains a tall posture on either side.
Lower body diagonal reach: While standing 2 shoe lengths away from a wall, the athlete maintains single-leg balance while reaching the opposite leg behind and across to touch his toes to the wall 3 times without touching the ground to practice the movement. The athlete repeats the test by touching his toes to the wall 5 times without losing balance. Inability to touch the wall 5 consecutive times without losing balance is considered a positive test.
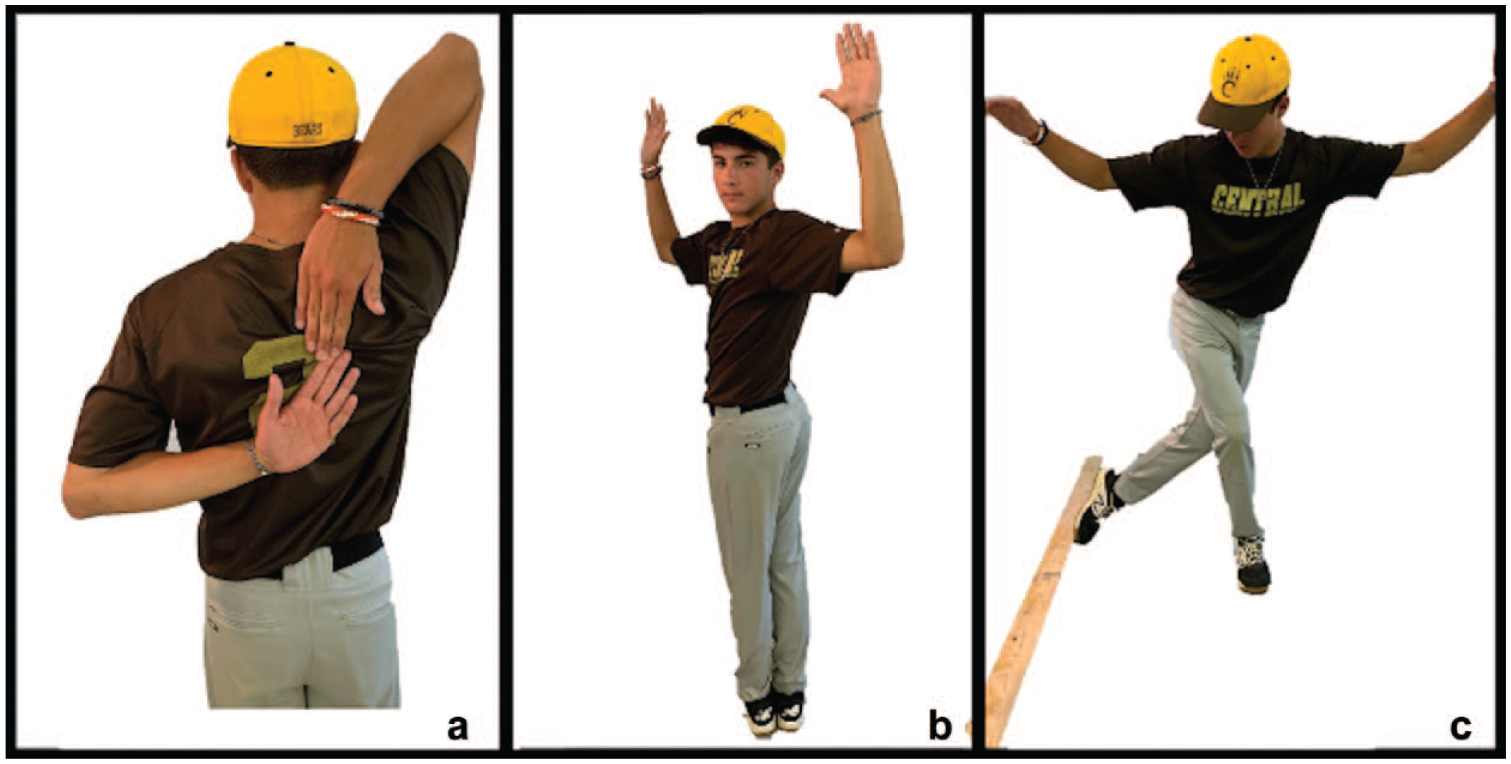
Arm care screen: (a) reciprocal shoulder mobility, (b) 90/90 total body rotation, and (c) lower body diagonal reach.
Each component of the ACS was scored as pass or fail on both the right and left sides. Pain with testing was recorded but did not factor into the scoring criteria. All participants were video-recorded performing the ACS testing procedures during the live testing. An iPhone 10XR cell phone was placed approximately 15 feet directly posterior to the participant. A youth baseball coach with more than 5 years of coaching experience electronically reviewed all video recordings and independently scored the ACS tests as pass or fail on each side. The results of the coaches’ ACS scoring results were used in the data analysis.
Musculoskeletal Impairment Measurements
Following ACS testing, 2 pairs of PTs (J.G./J.K. and A.H./L.B.) with 2 to 7 years of experience testing baseball players performed all ROM and balance impairment measures. The PTs were blinded to the results of the ACS testing. To improve reliability, the same PT from each team always stabilized the joint and performed the passive movement while the other PT measured with the goniometer. Intra-rater and inter-rater reliability for all ROM and balance measures were established in 10 male athletes before beginning data collection. Intraclass correlation coefficients (ICCs) for the PTs performing the testing were determined. Intra-rater (ICC (3,k) = 0.75-0.95) and inter-rater (ICC (3,k) = 0.79-0.97) reliability ranged from “good” to “excellent” for all measurements based on a mean-rating (k = 3), absolute agreement, and a 2-way mixed-effects model. 27
Shoulder Passive ROM
Dominant and nondominant shoulder IR, ER, and flexion were measured on a portable treatment table with a standard goniometer. Measurements for shoulder IR and ER passive ROM (PROM) were performed with the participant in the supine position with the shoulder placed in 90° of abduction, elbow flexed to 90°, and neutral forearm rotation. A small towel was placed under the humerus to maintain the plane of the scapula. One examiner stabilized the scapula and passively internally or externally rotated the humerus until first resistance was achieved. A second examiner aligned a standard goniometer with the axis at the olecranon process, the stationary arm along the midline of the forearm. 37 Shoulder TROM was determined as the sum of ipsilateral shoulder ER and IR. Shoulder flexion PROM was measured with the participant in supine position with the knees bent. The arm was positioned in 0° shoulder abduction and elbow extension with the shoulder and forearm in neutral rotation. One examiner provided light stabilization to the lateral scapular border and passively elevated the shoulder in the sagittal plane until first resistance was achieved. The second examiner aligned the axis of the goniometer with the lateral aspect of the acromion process and the stationary arm along the midline of the humerus. The average of 3 trials for each measurement was used for analysis. 44
Thoracic Spine Rotation PROM
The participant was placed in quadruped and instructed to sit with his hips back on his heels to flex the hips maximally. Upper extremities were positioned with elbows flexed and forearms together resting on a portable treatment table. The participant placed 1 upper extremity behind his back in the lower lumbar region. One examiner placed a bubble inclinometer between the spinous processes of T1 and T2. While stabilizing the ipsilateral hips and torso, the second examiner grasped the contralateral anterior shoulder of the participant and passively rotated the thoracic spine until first resistance was achieved. The examiner monitored for compensations such as excessive spinal side-bending, weight shifting, or inability of the hips to remain on the heels. The participant was encouraged actively to rotate his neck in sync with the thoracic rotation. Measurements were taken bilaterally and the average of 3 trials was used for analysis. 17
Hip Rotation PROM
Hip IR and ER PROM was measured with the participant in prone position on a portable treatment table with the hips adducted and the knees flexed to 90°. One examiner stabilized the pelvis and passively rotated the femur internally or externally until first resistance was achieved. The second examiner aligned a standard goniometer with the axis at the tibial tuberosity and the stationary arm along the midline of the tibia. Measurements were taken bilaterally and the average of 3 trials was used for analysis.13,25,28
Y Balance Test-Posterolateral Reach
The Y Balance Test-Posterolateral Reach (YBT-PL) was performed consistent with the protocol and testing kit developed by Plisky et al. 26 The participant stood on the stance platform with shoes off and toes behind the red line. The participant was instructed to push the reach indicator in the posterolateral direction as far as possible with the free limb while maintaining balance on the stance limb. The trial was not counted if the participant lost his balance, touched the reaching foot to the ground, shoved the reach indicator, or rested on top of the reach indicator to gain support. To mitigate the learning effect, 6 practice trials were performed on the YBT kit followed by 3 trials which were scored and recorded. The average of the 3 scored trials was recorded, and the same procedure was performed on the opposite leg.
Musculoskeletal Risk Factors
For the ACS to identify musculoskeletal risk factors, specific cutoff thresholds had to be established for each risk factor. Impairments below established physical impairment cutoff values were dichotomized as present or absent from the previous literature when available. Nine musculoskeletal risk factors were measured by blinded PTs independent of the ACS scoring.
Reciprocal Shoulder Mobility
If any of the following shoulder or thoracic spine impairments were present during specific goniometric measures, the athlete was dichotomized as possessing at least 1 musculoskeletal risk factor. These measures were compared to the reciprocal shoulder mobility screen outcome to determine test validity. Definitions of the impairments are as follows:
Limited shoulder IR PROM <45°: The dominant shoulder was measured to have <45° of IR PROM at 90° abduction. 3
GIRD ≥20°: The difference between nondominant shoulder IR and dominant shoulder IR was ≥20°.36,38
Shoulder TROM deficit ≥10°: The difference between dominant shoulder TROM and nondominant shoulder TROM was ≥10°.3,42
Shoulder flexion deficit ≥5°: The difference between dominant shoulder flexion PROM and nondominant shoulder flexion PROM was ≥5°. 43
Thoracic spine rotation PROM <50°: Either dominant or nondominant thoracic rotation PROM was measured to have <50° in the quadruped position. 15
90/90 Total Body Rotation
If any of the following thoracic spine rotation impairments described above (1-5) or hip rotation PROM limitations were present during specific goniometric measures, the athlete was dichotomized as having at least 1 musculoskeletal risk factor. These measures were compared to the 90/90 total body rotation screen outcome to determine test validity. Definitions of the impairments are as follows:
Lower Body Diagonal Reach
If any of the following hip rotation PROM impairments described above (6 and 7) or dynamic single leg balance deficits were present during specific goniometric measures the athlete was dichotomized as possessing at least 1 musculoskeletal risk factor. These measures were compared with the lower body diagonal reach screen to determine test validity. Definitions of the impairments are as follows:
8. Normalized YBT-PL reach distance: Stance and stride leg YBT-PL reach was measured using the YBT test kit and protocol. To control for the effect of player height on absolute reach distance, the YBT-PL reach was normalized by dividing the participant’s YBT-PL reach by their dominant lower body limb length and multiplied by 100. The means of the normalized YBT-PL reach distances were calculated for each age level. YBT-PL reach distance performance below the lower third quartile for the youth (<92 cm), high school (<95 cm), and college (<98 cm) age levels were considered risk factors. 29
9. YBT-PL reach asymmetry: The absolute difference between stance and stride YBT-PL reach distance was ≥5.5 cm. 5
Statistical Analysis
Descriptive statistics reported as average ± SD or frequency counts were calculated for all variables. The accuracy of the ACS to discriminate between players with at least 1 musculoskeletal injury risk factor was determined using cross-tabulations. The presence of any corresponding musculoskeletal risk factor was dichotomized as described previously and entered into separate 2 × 2 tables for each component of the ACS. For the ACS reciprocal shoulder mobility screen, the reference standard was the goniometric measurement of musculoskeletal risk factors with the ACS as the clinical screen. A true positive (TP) was represented by the presence of at least 1 shoulder or thoracic mobility risk factor which was correctly identified by a positive ACS reciprocal shoulder mobility test on either side. A true negative (TN) was indicated by the participant passing all the goniometric shoulder and thoracic ROM tests and testing negative on the reciprocal shoulder mobility screen bilaterally. A false positive (FP) was defined as the absence of any shoulder or thoracic risk factors but the participant tests positive on either side of the reciprocal shoulder mobility test. A false negative (FN) occurred when a participant possessed at least 1 shoulder or thoracic risk factor but was negative on the reciprocal shoulder mobility screen bilaterally. The 2 × 2 tables for the 90/90 total body rotation and lower body diagonal reach screens were constructed following a similar process. Univariate analyses were performed using the chi-square test for categorical variables to evaluate significant differences between ACS performance and those above or below the corresponding cutoff value. A Fisher’s exact test was used to measure the association if 1 or more cells had an expected count less than 5. Sensitivity, specificity, positive predictive value (PPV), negative predictive value (NPV), likelihood ratios (LRs), and odds ratios (ORs) were calculated with 95% CIs to describe the accuracy of the ACS to detect musculoskeletal risk factors. All data analyses were performed with R for Mac OS 4.1.2 statistical software (RStudio for Mac, version 1.4). An alpha level of P < 0.05 was considered statistically significant for all tests.
Results
A total of 150 male baseball players from 6 different teams met the inclusion and exclusion criteria and agreed to participate in the study. Demographic characteristics of all youth, high school, and college participants are listed in Table 1. The mean age ± SD of all participants in this sample was 16.7 ± 3.3, 29.3% (n = 44/150) were primarily pitchers, 64.0% (n = 96/150) were infield or outfield position players, and 6.7% (n = 10/150) were catchers.
Descriptive characteristics of baseball players
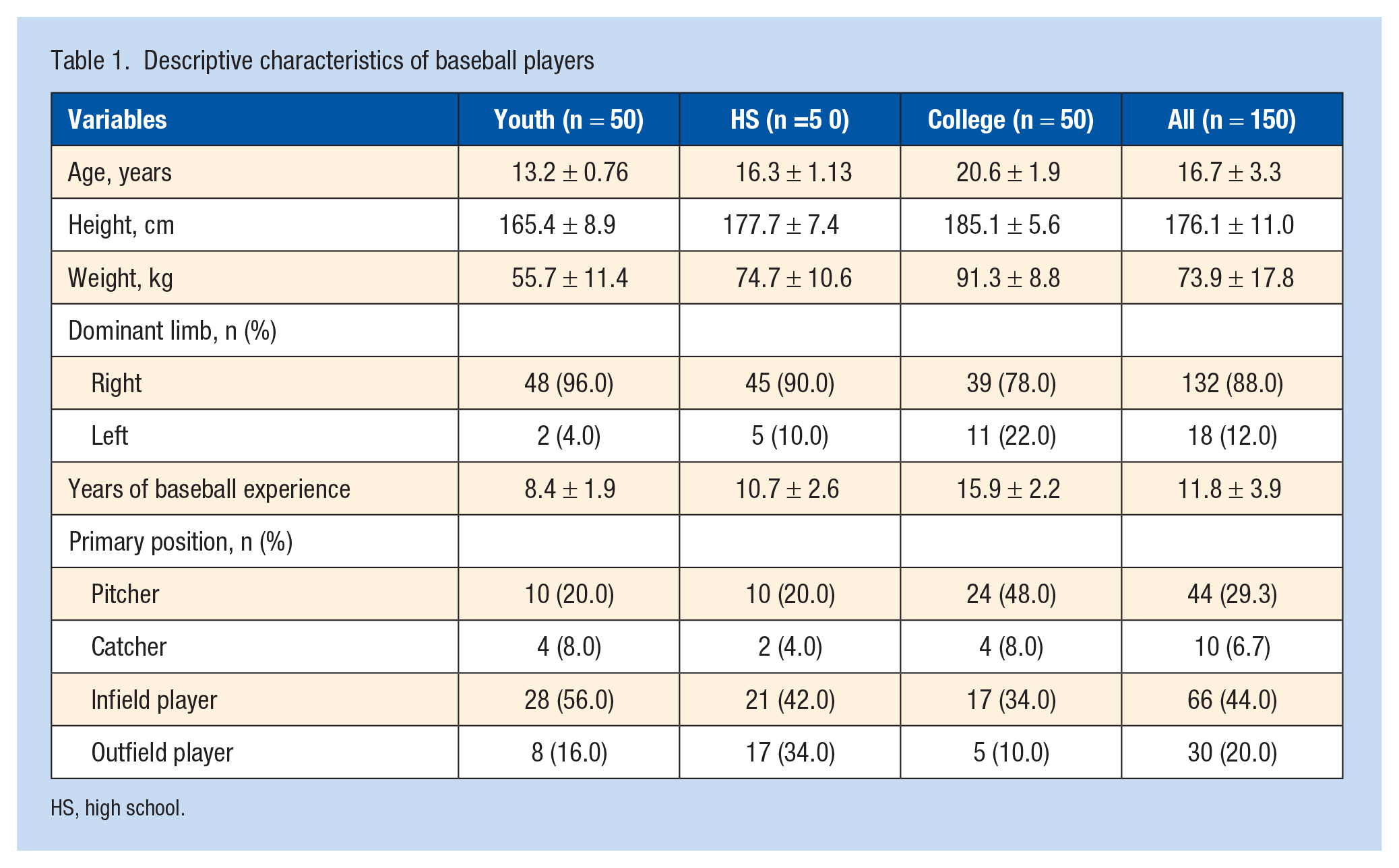
HS, high school.
Discriminant Validity of ACS by Level Using Impairment Score Thresholds
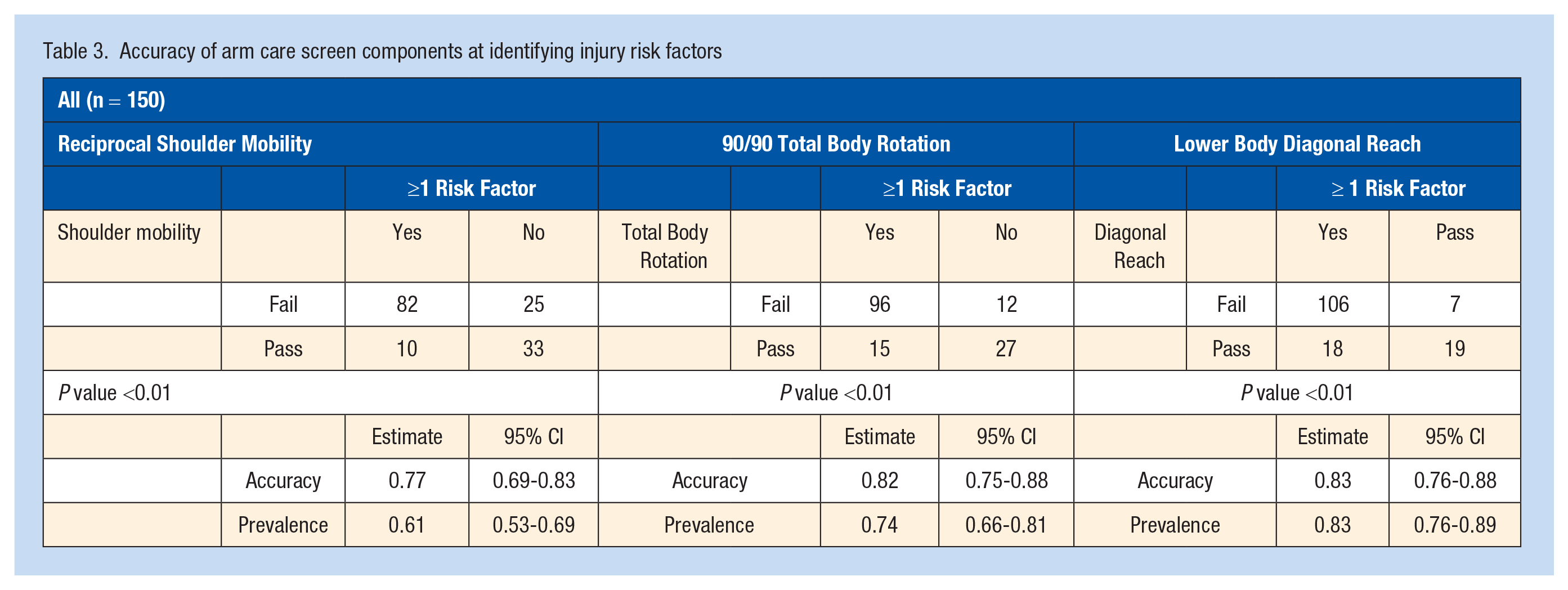
The accuracy of the ACS to discriminate between those possessing musculoskeletal risk factors for each age level is listed in Table 2. Chi-square tests showed significant associations for the 2 × 2 contingency tables created for each ACS subtest (P < 0.01) across all age levels (Table 3). The prevalence of existing musculoskeletal risk factors among all 3 age groups ranged from 0.61 to 0.83, and the accuracy of each component of the ACS ranged from 0.77 to 0.83. Each ACS subtest demonstrated higher sensitivity ranging from 0.85 to 0.89 compared with specificity which ranged from 0.57 to 0.73. The sensitivity of the reciprocal shoulder mobility screen was 0.89 (95% CI 0.81-0.95), while the 90/90 total body rotation and lower body diagonal reach screens had a sensitivity of 0.86 (95% CI 0.79-0.92) and 0.85 (95% CI 0.78-0.91), respectively. Overall, baseball players with musculoskeletal risk factors were at 10.8 (95% CI 4.7-25.0), 14.1 (95% CI 6.03-34.4), and 16.0 (95% CI 5.9-43.5) times greater odds for failing the reciprocal shoulder mobility screen, 90/90 total body rotation screen, or lower body diagonal reach screen compared with players without musculoskeletal risk factors, respectively.
Accuracy of ACS components at identifying injury risk factors
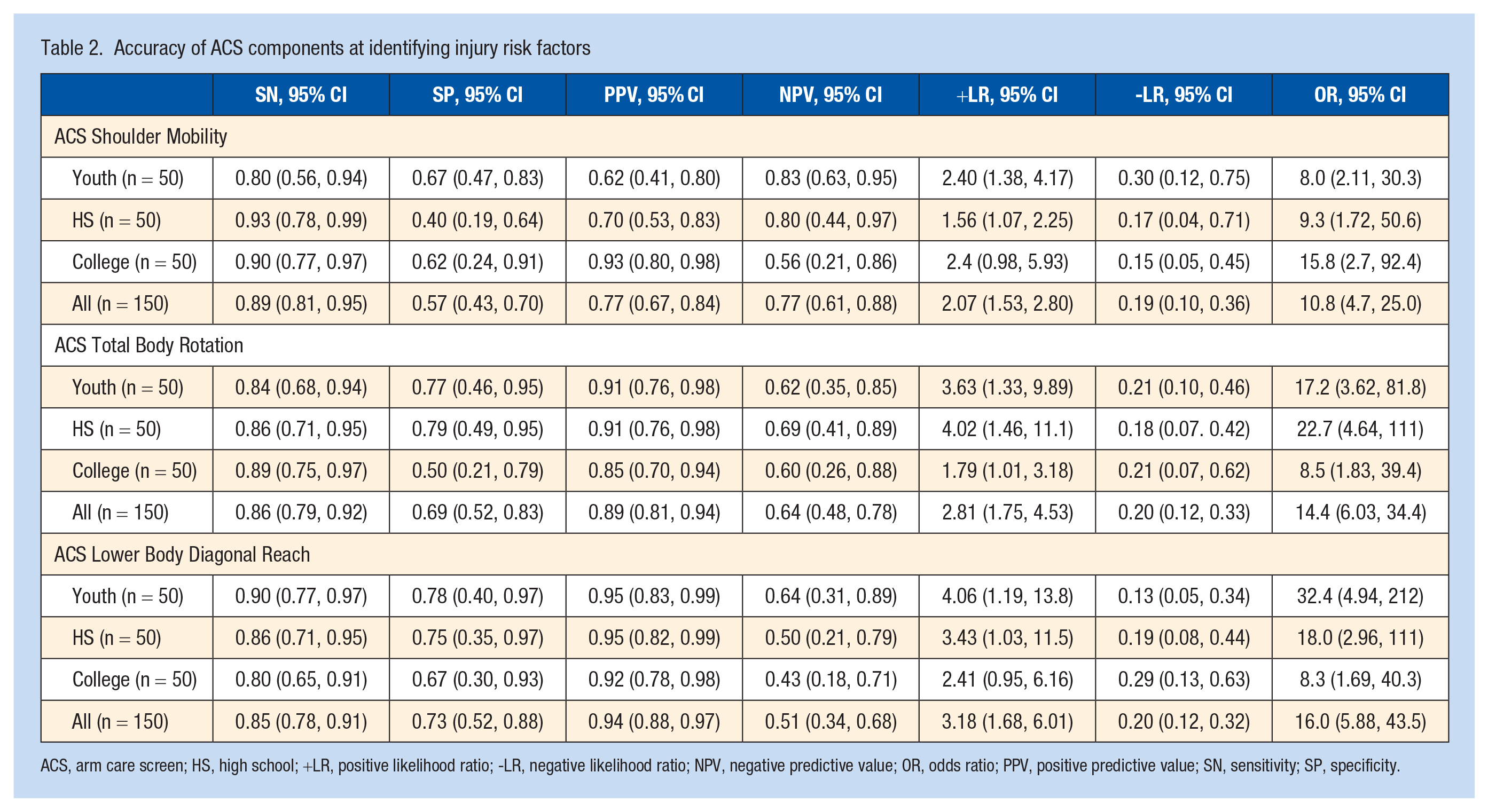
ACS, arm care screen; HS, high school; +LR, positive likelihood ratio; -LR, negative likelihood ratio; NPV, negative predictive value; OR, odds ratio; PPV, positive predictive value; SN, sensitivity; SP, specificity.
Accuracy of arm care screen components at identifying injury risk factors
Discussion
The goal of the ACS was to evaluate global movement patterns with the assumption that the inability to meet the passing criteria would be associated with a corresponding local impairment. As the reason for movement pattern limitations could vary among individuals and change over the course of a season, we expected the ACS to capture at least 1 musculoskeletal risk factor which could be affecting the global movement pattern. The findings from this study support the hypothesis that the ACS tests can accurately discriminate between baseball players with or without musculoskeletal risk factors. All 3 subtests of the ACS exhibited high sensitivity for detecting at least 1 corresponding musculoskeletal risk factor. Furthermore, players with musculoskeletal risk factors had significantly greater odds of failing the ACS tests regardless of age level. Therefore, baseball coaches working with youth, high school, or college-level players can confidently use the ACS to screen their players for musculoskeletal risk factors.
Identifying the presence of these risk factors in baseball players is difficult for coaches who have limited time to measure each joint impairment involved in throwing. The ACS is a simple screen that can aid the medical staff or coaches in identifying potential impairments that need to be addressed to minimize injury risk factors. In the current study, players who did not have musculoskeletal risk factors were approximately 5 times more likely to pass compared with those who fail. Owing to its high sensitivity and NPV and low negative LRs, the ACS can serve as a true screening tool effectively ruling out the presence of risk factors given a negative test. Implementation of the ACS would allow coaches to capture players with musculoskeletal risk factors, as well as some players who were falsely positive without risk factors. Although some baseball players without musculoskeletal risk factors would be performing additional arm care exercises, the inclusion of more exercise is typically low risk and would not cause physical harm to the player.
Baseball players commonly present with normal asymmetries in shoulder IR ROM due to a humeral retrotorsion adaptation. 10 However, dominant shoulder IR ROM limitations that become too great are commonly associated with increased injury risk. Shanley et al 37 found that high school baseball players with a >25° GIRD were at 3.7 (relative risk 3.7; 95% CI 1.6-8.9) times greater risk for injury. Furthermore, pitchers with an ulnar collateral ligament (UCL) tear had on average 21° of shoulder IR ROM loss compared with 13° of average shoulder IR loss in those without a UCL tear. 23 In the current study, extreme limitations in shoulder IR ROM and GIRD were detected by the reciprocal shoulder mobility screen. There were no high school or college-level players who passed the reciprocal shoulder mobility screen and had <45° of shoulder IR PROM or GIRD >20°. This suggests that the ACS reciprocal shoulder mobility screen can serve as a quick method for ruling out shoulder IR and GIRD limitations.
Poor movement of the thoracic spine can disrupt the kinetic chain sequence, cause to undesired compensation of the low back and shoulder girdle, and lead to musculoskeletal injury. 14 Decreased thoracic spine ROM is associated with increased kyphosis and scapular protraction which could limit shoulder mobility 16 and contribute to the development of pain. 41 Sakata et al 31 reported that reduced thoracic spine mobility increased the risk for injury in baseball players 2.5-fold. The goal of the 90/90 total body rotation screen was to evaluate the interaction of thoracic spine rotation and hip rotation collectively. Screening the thoracic spine and hips independently is less desirable because the upper and lower body must function simultaneously during rotational sports.
Risk factors throughout the entire kinetic chain have been identified in baseball players as potentially contributing to injury. The lower quarter has been implicated in contributing to injury risk when not functioning ideally. Sekiguchi et al 35 reported that stride hip IR ROM <36° was associated with elbow or shoulder pain (OR 0.93; 95% CI 0.87-0.99) in youth baseball players. The results of the present study suggest that thoracic spine mobility deficits are prevalent, especially among high school and college-level players. Deficits in single-leg balance lead to poor lumbopelvic control and can disrupt the kinetic sequencing of the throwing motion, requiring a greater contribution from the upper extremity to develop the force needed for pitching performance. 19 The goal of the lower body diagonal reach screen was to evaluate dynamic single leg balance near the limits of the player’s hip rotational ability. Previous research has reported that normal hip IR and ER ROM are associated with better dynamic balance performance. 18
Multimodal arm care exercise programs have targeted several different musculoskeletal risk factors to mitigate injury incidence. In a prospective cohort, Sakata et al 32 reported that improvements in shoulder TROM, stride hip IR PROM, and thoracic spine mobility were the most predictive variables associated with reduced odds of medial elbow injury in 305 youth baseball players. In the current study, numerous musculoskeletal risk factors throughout the kinetic chain were plausible impairments that the ACS could identify. This could provide baseball coaches with more guidance as to which risk factors are being identified during the screening process so that exercise intervention can be recommended prior to the onset of injury. As a result, the ACS can serve as a useful tool for detecting declining mobility and is a valid measure for distinguishing between unique limitations in mobility and balance in youth, high school, and college-level baseball players. Future research should investigate the predictive validity of the ACS to identify baseball players who are at risk for injury.
Limitations
The results of this study should be interpreted conservatively as it has significant limitations. First, the prevalence of musculoskeletal risk factors was high in this sample limiting confidence in the interpretation of PPV and accuracy due to the oversaturation of risk factors. This was especially true in the lower body diagonal screen as prevalence and accuracy were similar. However, both the reciprocal shoulder mobility and 90/90 total body rotation screen demonstrated accuracy that exceeded the upper bound 95% CI for the prevalence. Second, the current study focused on youth, high school, and college-level baseball players who played a variety of positions. The results of this study may not be generalizable to baseball players at the professional level or female softball players. We included only male baseball players to maximize the homogeneity of our sample because the pitching mechanism and injury risk factors vary in softball players; however, we also included both position players and pitchers. The musculoskeletal function differs between pitchers and position players and likely resulted in increased heterogeneity among our participants. Finally, the ACS is only a screen and does not implicate a specific risk factor. Baseball players who failed the reciprocal shoulder mobility screen could have GIRD, asymmetrical shoulder TROM, limited shoulder flexion ROM, or decreased thoracic spine rotation ROM. Although not specific to a particular risk factor, the goal would be to raise awareness that a greater dosage of arm care exercises should be dedicated to the upper quarter compared to the lower quarter.
Conclusion
The ACS is a simplistic screening tool that can be administered in less than 3 min to discriminate between common musculoskeletal risk factors associated with injuries in youth, high school, and college-level baseball players. The ACS subtests demonstrate high sensitivity for correctly identifying musculoskeletal risk factors common in baseball players and can be useful as screening tools for baseball coaches and healthcare professionals in developing and potentially monitoring arm care exercise programs.
Footnotes
Acknowledgements
The authors thank Evansville North High School and head baseball coach Jeremy Jones, Gibson Southern High School and athletic trainer Sean Malone, University of Evansville and head coach Wes Carroll, University of Southern Indiana and head coach Tracey Archuleta, Harrison High School and head coach Houston Dillman, and youth coaches Mindy Humphrey and Tarron Acuff for access to the players. Special thanks to physical therapists Dr Jenna Gourlay, Dr Jonathan Kirsch, Dr Logan Blair, Dr AJ Hermann, and Adam Devery for assistance with data collection.
The authors report no potential conflicts of interest in the development and publication of this article.