
Abstract
Context:
Up to 90% of pediatric athletes return to sport (RTS) after anterior cruciate ligament reconstruction (ACL-R); however, <50% RTS at the same level and second ACL injury rates are up to 32%.
Objectives:
(1) Determine which physical and patient-reported outcome measures guide clinical decision-making on RTS in pediatric athletes after ACL-R and (2) present a framework with insights from cognitive and neurophysiological domains to enhance rehabilitation outcomes.
Data Sources:
PubMed, CINAHL, Embrase, and Cochrane library databases and gray literature.
Study Selection:
Data on pediatric (<18 years) ACL-R patients, RTS, tests, and decision-making were reported in 1214 studies. Two authors independently reviewed titles and abstract, excluding 962 studies. Gray literature and cross-reference checking resulted in 7 extra studies for full-text screening of 259 studies. Final data extraction was from 63 eligible studies.
Study Design:
Scoping review.
Level of Evidence:
Level 4.
Data Extraction:
Details on study population, aims, methodology, intervention, outcome measures, and important results were collected in a data chart.
Results:
Studies included 4456 patients (mean age, 14 years). Quadriceps and hamstring strength (n = 25), knee ligament arthrometer (n = 24), and hop tests (n = 22) were the most-reported physical outcome measures guiding RTS in <30% of studies with cutoff scores of limb symmetry index (LSI) ≥85% or arthrometer difference <3 mm. There were 19 different patient-reported outcome measures, most often reporting the International Knee Documentation Committee (IKDC) (n = 24), Lysholm (n = 23), and Tegner (n = 15) scales. Only for the IKDC was a cutoff value of 85% reported.
Conclusion:
RTS clearance in pediatric ACL-R patients is not based on clear criteria. If RTS tests were performed, outcomes did not influence time of RTS. Postoperative LSI thresholds likely overestimate knee function since biomechanics are impaired despite achieving RTS criteria. RTS should be considered a continuum, and biomechanical parameters and contextual rehab should be pursued with attention to the individual, task, and environment. There is a need for psychological monitoring of the ACL-R pediatric population.
The incidence of anterior cruciate ligament (ACL) injuries in young athletes (<18 years) has increased by 23% annually over the last 2 decades in both skeletally mature and immature children. 10 A subsequent increase of 74% to 174% of ACL reconstructions (ACL-R) was reported in this time period.17,100,103 However, surgical or nonsurgical management of ACL injuries in pediatric athletes remains a topic of controversy.
Return-to-sport (RTS) rates after ACL-R in young athletes have been reported to be as high as 90%.9,25,49,64 However, 46% to 84% return to a lower level of sport than their preinjury level. 9 For example, 37% of those participating at level 1 type of sport (pivoting contact sports) before injury were active at level 2 type of sport (pivoting noncontact sports) after ACL injury. 8 It is also of great concern that RTS is associated with a high rate of second ACL injury, which is reported to be as high as 32%.9,25 Of those, 19% are graft ruptures, 13% contralateral injuries, and 1% of patients sustain both.9,25 Of those reinjuries, 78% occur before the age of 20 years. 9 The risk of sustaining a graft injury after the first 12 months post ACL-R, is as high as 83%,5,9 and still unacceptable high (67%) after the second year postsurgery. 9
The high rates of second ACL injury highlight the need for secondary injury prevention. This would be preferably incorporated in the RTS decision-making process after pediatric ACL-R. There is a paucity of literature about RTS criteria for pediatric athletes after ACL-R. There is no consensus on RTS criteria to determine if a pediatric patient is ready to participate in sport again, and the validity of the current criteria remains unknown. 5 Recently, a scoping review presented an overview on the RTS tests used, showing sparse evidence for specific testing regarding RTS in children after ACL-R. 26
RTS testing has been studied extensively in adults with ACL injury. The difference between the affected and nonaffected leg is assessed using the limb symmetry index (LSI) and typically used to detect deficits in a hop test battery. An LSI >90% for hop distance is recommended as the RTS cutoff value. 54 This is also considered the cutoff value for quadriceps (QS) and hamstring strength (HS). 40 In pediatric ACL-R patients, the validity of these tests remains unknown. 5
Young athletes perform not only closed motor tasks like hopping. 6 In open skilled sports (eg, football, handball), athletes are subject to continuous change of playing situations. The capacity to anticipate is essential and a broad spectrum of motor skills is needed to participate fully in sports. This puts more cognitive load on the ACL-injured pediatric athlete since they experience a higher cognitive load to precise joint position and motor control during functional motor tasks. 36
Moreover, not being psychologically ready may negatively impact on RTS outcomes, 27 and therefore the psychological readiness to RTS needs to be evaluated.5,41,70
The aims of this scoping review were to (1) identify which physical outcome measures (POMs) and patient-reported outcome measures (PROM) should be considered to guide clinical decision-making on RTS in pediatric skeletally immature and mature ACL-R athletes and (2) present a framework integrating cognitive and neurophysiological principles to assessment and rehabilitation in these patients.
Methods
In this study, we used the Preferred Reporting Items for Systematic reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-ScR) checklist together with the PROSPERO Protocol for Systematic reviews. This study was registered prospectively with the Open Science Framework (https://osf.io/9b5mu).
Data Search
The following databases were searched: PubMed, CINAHL, Embase, and the Cochrane Library. The following Mesh terms were used: ‘Anterior Cruciate Ligament’ AND ‘Pediatric’ AND ‘Return to sport.’ Search terms were adjusted for the specific database (Figure 1).
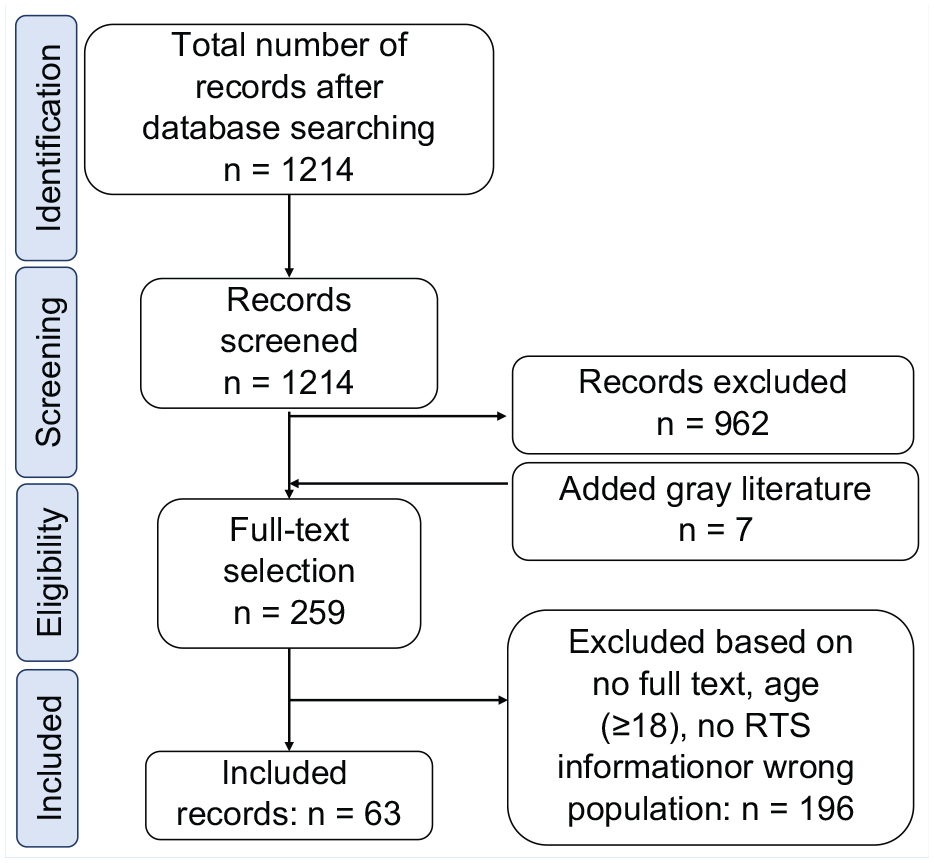
PRISMA flowchart article selection. 71 PRISMA, Preferred Reporting Items for Systematic reviews and Meta-Analyses; RTS, return to sport.
Appendix 1, available in the online version of this article, describes further details about the literature search.
Studies were considered eligible for inclusion if they (1) contained information on (1) athletes <18 years of age; (2) athletes with ACL-R (with and/or without associated lesions) treated either surgically or nonsurgically; (3) POM and/or PROM for RTS testing and/or RTS criteria; and if they (4) had full text available in (5) English or Dutch language. All study levels, except scoping reviews, were included. Gray literature was also searched. Studies on bony ACL lesions (avulsions) and animal studies were excluded.
The data search was performed incorporating literature up to November 21, 2021. Two authors independently reviewed titles, abstract, and full-text articles using Rayyan (https://www.rayyan.ai/). Any disagreements about the interpretation of the results were resolved by discussion. A third reviewer was consulted in case of any disagreement. Crossreference checking was performed to retrieve additional studies at the final stage of selection. One reviewer charted the retrieved data separately. The data were collected in 2 separate data searches, as was the reviewing process, which had a Kappa agreement of 0.77.
Data Charting Process
A data chart was created to assist structured data extraction. Details on study population, aims of the study, methodology, intervention type, outcome measures, and important results were collected.
Results
Search Results of This Study
A total of 1214 studies were included for title and abstract screening. After screening, 259 potentially relevant studies were retrieved. Of these, 58 annual meeting reports were excluded. From the remaining 201 studies, 65 were excluded as these reported on athletes aged ≥18 years. In addition, we excluded 62 studies as these lacked information about RTS and/or criteria, 5 studies that did not contain information about ACL injury or reconstruction, 2 that were duplicate records, 3 based on study type, and 1 as a published research protocol without any data. Consequently, a total of 63 studies were included for analyses.
Data Extraction
Participant Characteristics
The total number of included patients was 4456. The mean age of athletes was 14 years (range, 5.7-18.0 years). Some studies did not report the distribution of boys and girls. When reported, there were 2024 girls and 2071 boys in total. Table 1 presents patient demographics and Figure 2 the type of sport they participated.
Participant characteristics
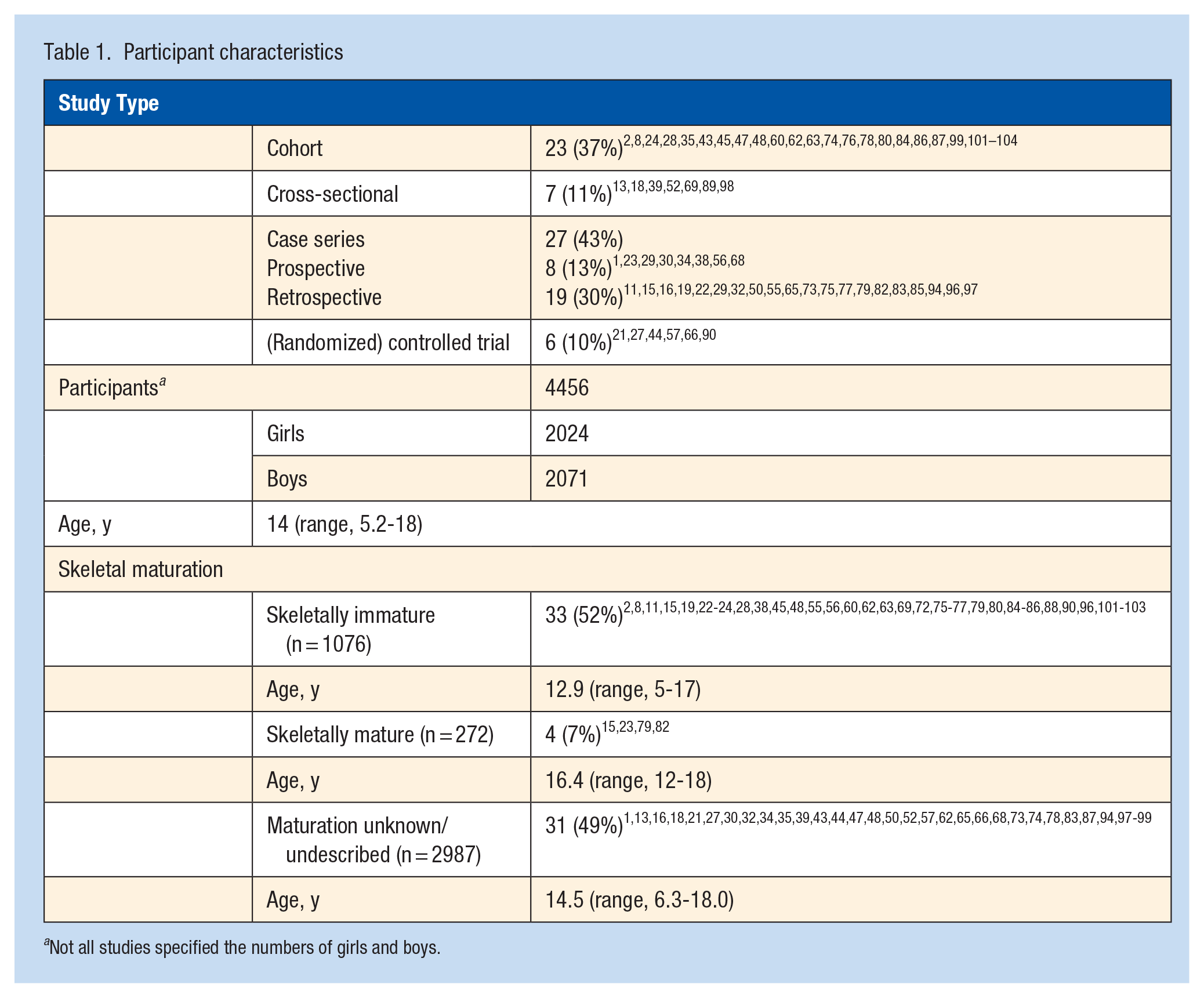
Not all studies specified the numbers of girls and boys.
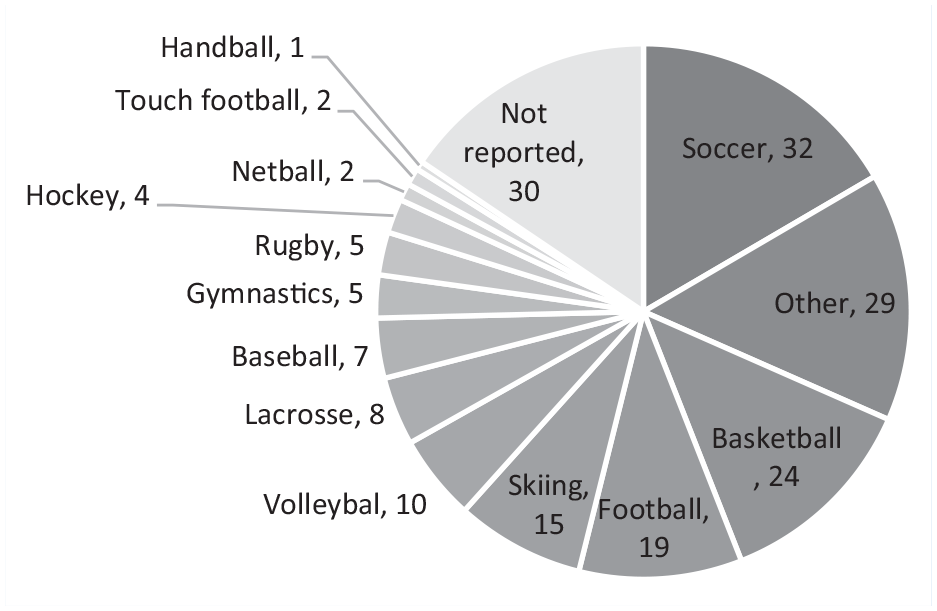
Distribution of sport types.
Physical Outcome Measures
The studies reported on a wide range of POMs for testing, mostly closed tasks and strength tests and, though to a much lesser extent, RTS decision-making criteria. Table 2 lists the number of studies reporting on POMs. Table 3 lists all the tests used for decision-making and, when reported, also the RTS cutoff point values.
Number of studies describing the physical outcome measures
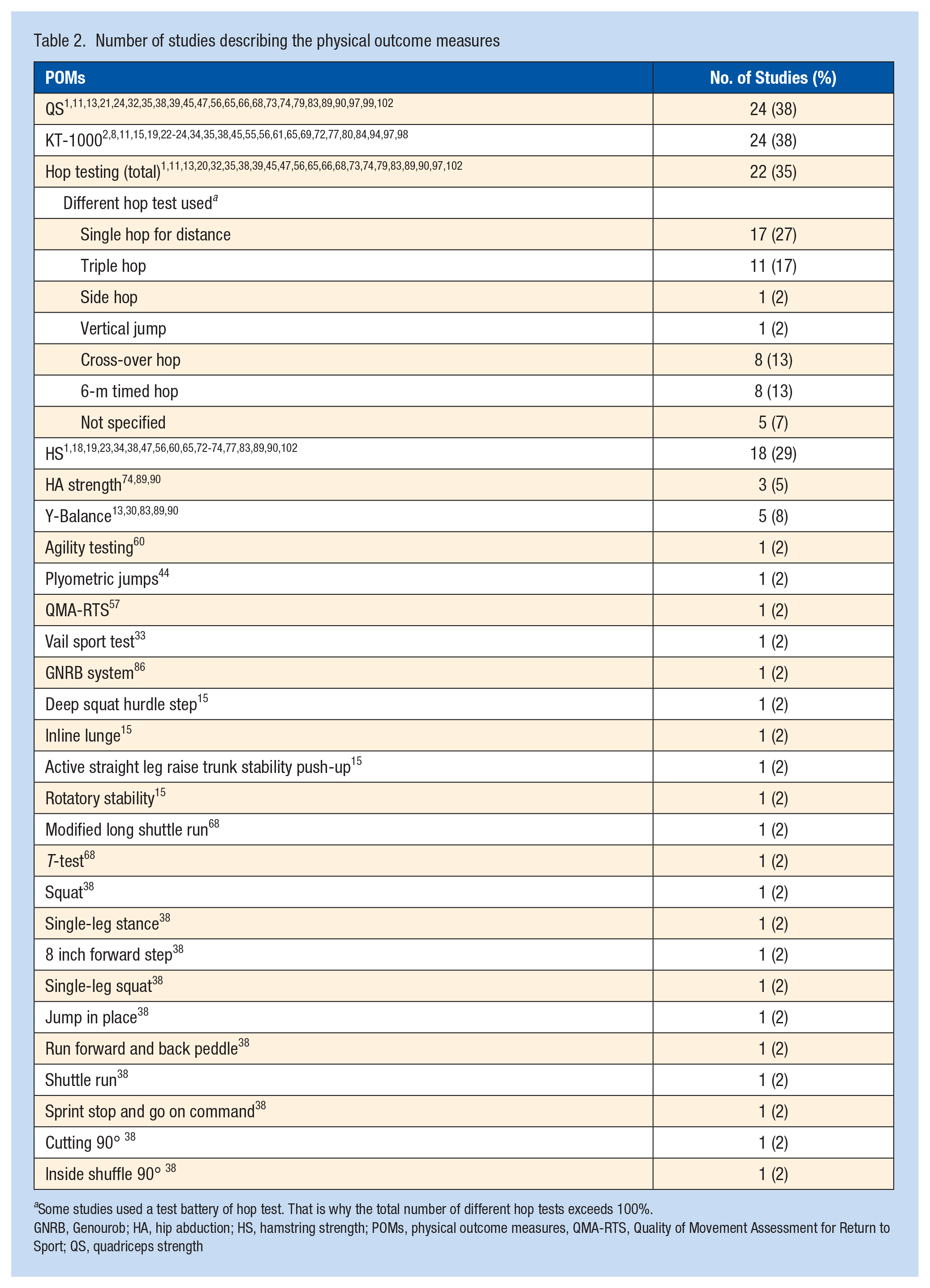
Some studies used a test battery of hop test. That is why the total number of different hop tests exceeds 100%.
GNRB, Genourob; HA, hip abduction; HS, hamstring strength; POMs, physical outcome measures, QMA-RTS, Quality of Movement Assessment for Return to Sport; QS, quadriceps strength
Overview of the tests used and RTS cutoff point values
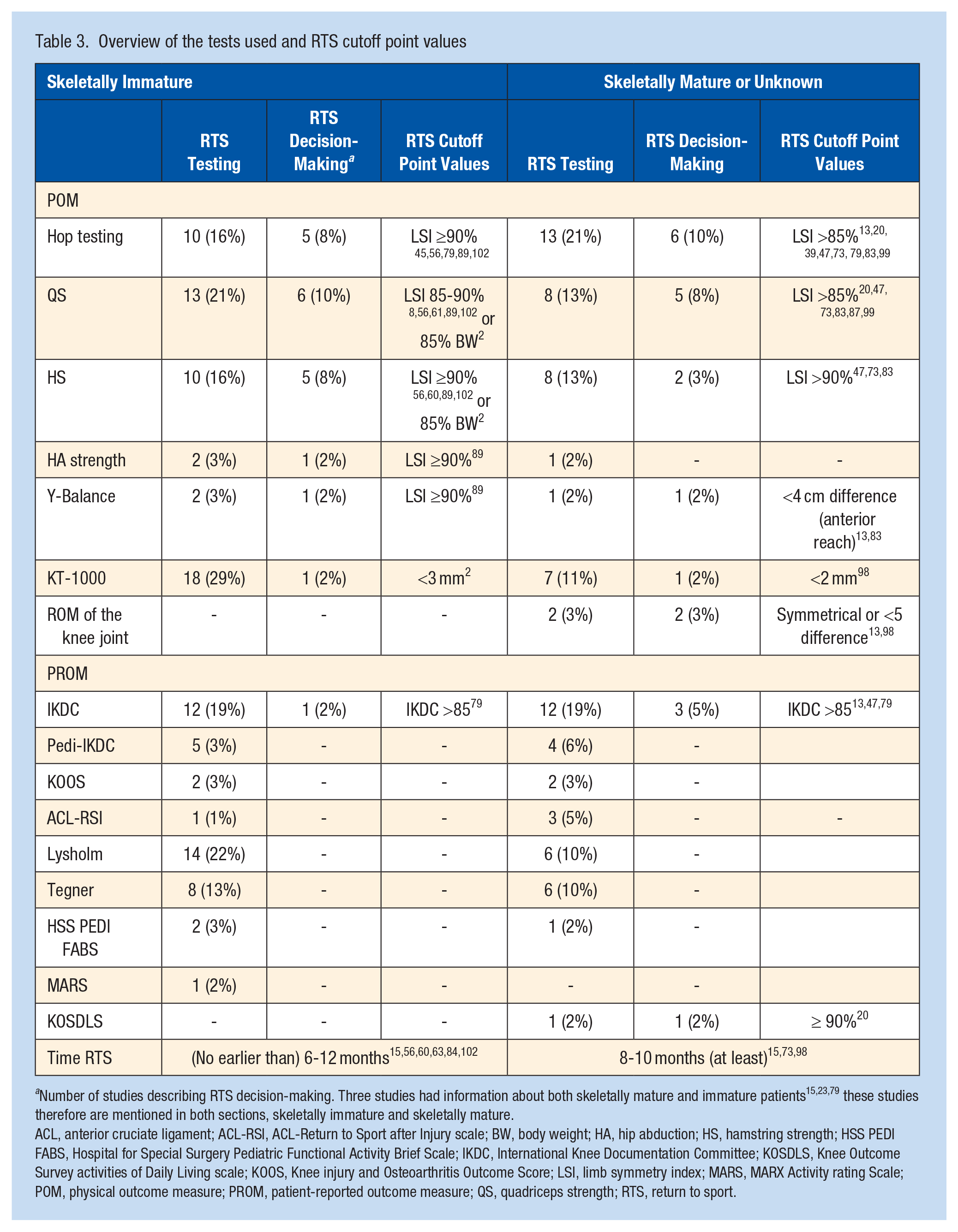
Number of studies describing RTS decision-making. Three studies had information about both skeletally mature and immature patients15,23,79 these studies therefore are mentioned in both sections, skeletally immature and skeletally mature.
ACL, anterior cruciate ligament; ACL-RSI, ACL-Return to Sport after Injury scale; BW, body weight; HA, hip abduction; HS, hamstring strength; HSS PEDI FABS, Hospital for Special Surgery Pediatric Functional Activity Brief Scale; IKDC, International Knee Documentation Committee; KOSDLS, Knee Outcome Survey activities of Daily Living scale; KOOS, Knee injury and Osteoarthritis Outcome Score; LSI, limb symmetry index; MARS, MARX Activity rating Scale; POM, physical outcome measure; PROM, patient-reported outcome measure; QS, quadriceps strength; RTS, return to sport.
In the included studies, 19 different questionnaires were used. The questionnaires reported were the International Knee Documentation Committee (IKDC) in 25 studies (38%),1,3,11,13,19,22,24,28,34,35,43,45,47,62,63,65,74,77-79,82,84,86,96,98 Pediatric (Pedi)IKDC in 11 studies (17%),18,30,32,50,55,78,83,96,101-103 Knee injury and Osteoarthritis Outcome Score (KOOS) in 4 studies (6%),27,74,80,86 the ACL-Return to Sport after Injury scale (ACL-RSI) in 5 studies (8%),18,30,52,57,102 the Lysholm score in 23 studies (37%),8,16,19,22,24,32,35,45,50,55,62,63,65,72,75-77,80,82,83,85,94,101 the Tegner in 15 studies (23%),16,27,28,46,50,55,62,63,75-77,82-84,101 the MARX Activity Rating Scale (MARS) in 1 study (2%), 24 the Hospital for Special Surgery Pediatric Functional Activity Brief Scale (HSS PEDI FABS) in 4 studies (6%),24,30,78,103 and the Single Assessment Numeric Evaluation (SANE) was used in 3 studies (5%).75,76,97 The following outcome measures were used once (2% of studies): the Knee Outcome Survey of Daily Living Scale (KOSDLS), 20 the Functional Knee Scoring Measure, 50 the Tampa Scale of Kinesiophobia (TSK-11), 27 the Athlete Fear of Avoidance Questionnaire (AFAQ), 27 International Society of the Knee Questionnaire, 69 and the Pediatric Patient-Reported Outcomes Measurement Information System (PEDI-PROMIS). 69 One study used both the VAS and the Knee Outcome Survey Activity of Daily Living Scale (KOS-ADLS). 65 The following 4 questionnaires were used in the same study (2%): Athletic coping scale-28 (ACSI28), Athletic Identity Measurement Scale (AIMS), Multidimensional Scale of Perceived Social Support (MSPSS) and the Impact of event scale (IES). 30 Note that the sum of percentages presented exceeds 100% as >1 questionnaire was used in various studies.
Discussion
The main outcome of this scoping review was that clearance for RTS in pediatric patients after ACL-R is not based on clear criteria. Although some form of RTS testing was performed in the included studies, no consequences were attached to the outcomes of these tests in 70% of cases, so RTS criteria were applied in only 30% of the studies. In those cases, the same cutoff values for adults were also used for pediatric patients.
PROMs were not applied consistently, including psychological readiness, the latter being used in only 6% (n = 4) of the studies. We will discuss our findings below. The LSI is used commonly to assess for differences in function between limbs. This review showed that LSI ≥85% cutoff criterion was used for RTS for hop testing and both QS and HS for pediatric athletes after ACL-R. These cutoff scores were the subject of vigorous debate. In adults, only 50% of patients who RTS after ACLR passed the criterion LSI ≥90%. 91 In healthy youth athletes, 95% were able to pass 1 of the hop tests (LSI ≥90%); however, this dropped to only 45% when all 4 hop test criteria had to be met. 58 Applying criteria from adult populations to pediatric patients seems a priori invalid; the appropriateness of these tests to serve RTS decision-making in pediatric athletes should be questioned.
Regarding hop testing in skeletally immature patients, it has been postulated that quality of movement should be assessed rather than LSI alone. 5 This was underpinned recently in adults,53,54 where those scoring within cutoffs of LSI of 90% were still found to demonstrate clear kinematic deficits. Incorporating the assessment of quality of movement in RTS clearance in pediatric athletes after ACL-R was also proposed by Dietvorst et al. 26
Isokinetic strength testing of QS and HS showed larger measurement errors in children than in adults and, as such, should be interpreted with caution. 5 Despite this, QS and HS testing was used widely in RTS decision-making in pediatric ACL-R patients (usually with cutoff LSI>90%2,8,20,47,56,60,73,87,91,99,102). Hannon et al 42 studied differences in muscle strength between noninjured type 1 (pivoting) young athletes (mean age, 14.9 years) and ACL-injured patients (mean age, 15.6 years). They found a 26% decrease in QS of the nonaffected leg in ACL-injured patients over time. When the nonaffected leg was considered to be the 100% reference, this indicated that QS of the ACL-R side is then only 74% upon RTS. Using an LSI ≥90% for RTS clearance for the affected leg as acceptable indicates that, upon RTS, QS may still only be at a 64% level of functioning. 42 Applying LSI in this manner likely increases the risk for the young ACL-R athlete as strength will be overestimated despite using the ≥90% threshold.
The limited use of the clear RTS criteria and the high number of reruptures warrant further research. Quantitative values were used to assist RTS clearance, but LSI symmetry may exist when quality of movement is still largely different. 54 Knee function was thus then likely overestimated when using the current quantitative RTS clearance criteria. Specific tests should be sought for the developing child and should be based on more than just kilograms, distance, or seconds. Quality of movement assessment may thus be the next valuable step in RTS decision-making in young patients.
Emerging evidence is addressing the importance of psychological status in RTS after ACL-R.7,92 The use of PROMs in pediatric ACL-R patients was rare, and the outcomes overall seem not to be weighted in the RTS decision-making process. Only 4 of the included studies used an RTS cutoff value. The only PROM with RTS cutoff values specified was a score <85 for the IKDC13,47,79 and ≥90% for the KOSDLS. 20
The PEDI-IKDC, specifically designed for children with knee disorders, is valid.51,95 However, we found that the adult version of the questionnaire was used in pediatric ACL-R patients rather than the pediatric version.
Psychological readiness is of current interest in ACL rehab and RTS. Fear of reinjury, perceived functional limitations, decreased quality of life, and changes in social roles all impact negatively upon the rehabilitation process. 27 In young athletes, a correlation was found between knee function and self-esteem, mental health, emotional role, and social limitations. 14 This suggests that quality of life in this population is affected by physical limitations as a result of knee joint dysfunction. It was suggested that young patients are affected differently than adults by an ACL injury, as emotional functioning of pediatric patients was likely more affected in than adults. 14 This shines a light on the important dark sides of long-lasting disability and the time-consuming rehabilitation processes, especially in this specific young group and has direct implications for improving quality of rehabilitation, with elements that need to be addressed for this young population. Fun can be targeted, for example, by using gamification or appealing to the preferred sport context, especially in the early phases. This will likely increase compliance and eventually rehabilitation outcomes.
RTS is not a single moment at the end of the rehabilitation process. RTS is considered to be a continuum, starting during rehabilitation, and task and context is applied more and more to prepare the injured athlete to perform again. 6 This indicates that certain cutoff values are prerequisites that guide taking a next step in the process. Of the 4 ACL injuries, 3 are noncontact by nature, implying that movement patterns (local joint kinematics or whole-body kinematics) may matter when it comes to staying safe after an ACL injury.4,12 Only with proper loading and sufficient demands during rehabilitation is there optimal preparation for sustainable knee function.
Despite ACL-R, abnormal movement patterns were reported consistently in the literature.53,54 This raises questions regarding whether common rehabilitation strategies are sufficient to target aberrant movement. In pediatrics, learning new motor skills through an external focus of attention and implicit learning are often described.31,37,59,93 Rehabilitation using external focus and implicit learning seems promising as movement patterns transfer to sports and could therefore be a sustainable solution for movement skills, reducing the risk of graft rupture. 37 RTS should therefore include improving motor patterns and thus quality of movement should be incorporated into rehabilitation. 36
We propose that movement quality be assessed not only in closed motor tasks like hopping but also in tasks that align with the sport-specific context.
There should preferably be attention on several factors during the rehabilitation process: the individual athlete (body-joint kinematic, movement pattern, and learning ability), task, and environment. 67 Athletic performance depends on all 3 factors, so if a performance deficit remains regarding 1 of these, this will likely have a negative impact upon total performance and increase the (re-)injury risk.
Figure 3 shows that movement patterns and perception likely relate to injury. There are 3 types of mechanical factors related to an ACL injury. Suboptimal local joint pattern, kinematics in the whole-body kinematic, and a (non)contact trauma.
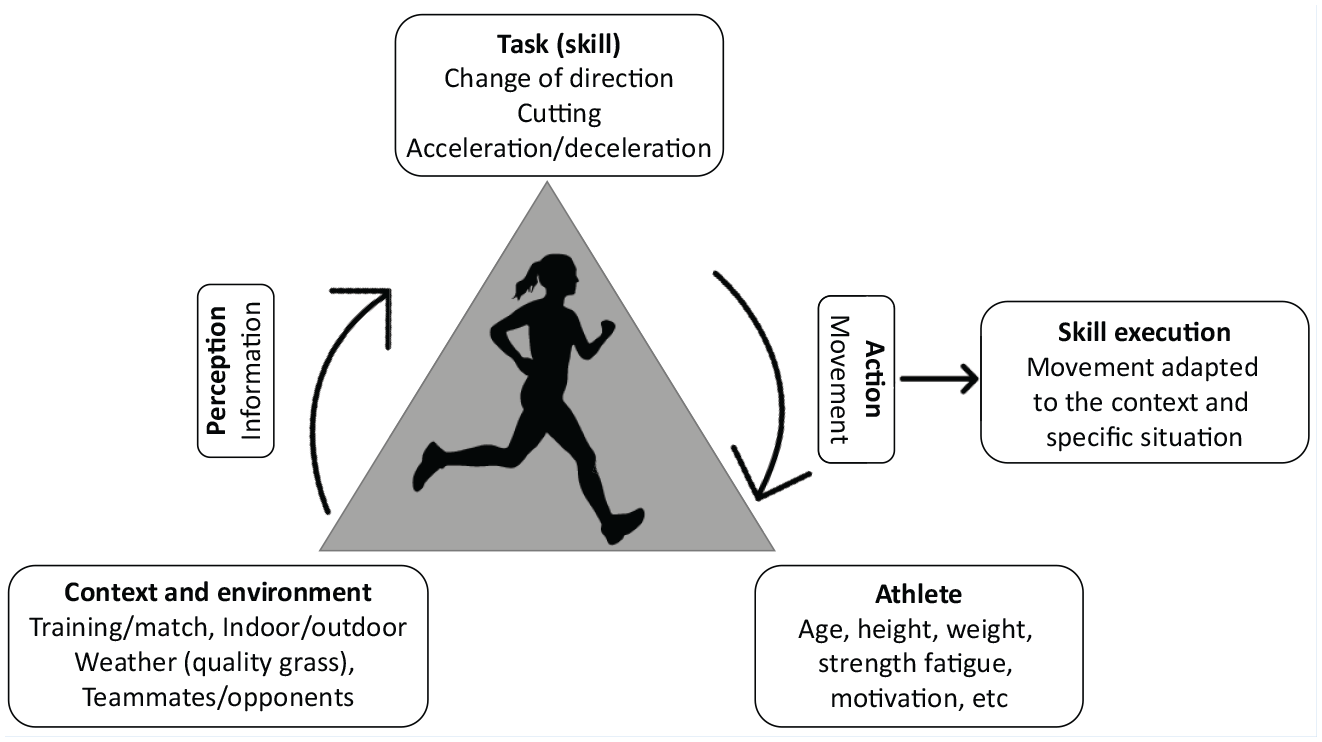
Example football dynamic system (modified from Mullally and Clark 67 ).
Knowledge of the mechanical factors and an effective intervention may prevent a secondary injury in the future. An ACL injury can occur in a direct contact situation with an opponent or in an indirect noncontact situation with or without an opponent. Direct contact is hard to prevent in the future, but movement strategies in indirect or noncontact situations can be trained, aiming to prevent a secondary knee/ACL injury in the future. 67
Early specialization is increasing in youth sports, resulting in less broad motor skill development in children. There is a long competition season, with increasing pressure on younger athletes. 24 Also, children seem to be less fit than 40 years ago, which includes a decrease in neuromotor fitness (ie, muscle strength, flexibility, speed of movement, and coordination), both negatively affecting the young athlete’s activity level as well as long-term health. This may result in a higher risk of injury, including sports injuries like those of the ACL. 81
There is still no consensus or sustainable solution regarding RTS in pediatric ACL-R patients. Current practice is still derived from the adult and skeletally mature patient. But, at 3-year post surgery, about 19% suffer a graft rerupture and around 13% sustain a contralateral ACL injury. 25 This suggests that we are still insufficiently able to determine whether an ACL-R pediatric patient is ready to return to pivoting sports safely.
The most important limitation of this study was that some more data seemed to be available but not usable within the stated inclusion criteria. Attempts were made to get in touch with the authors of these studies, but due to (1) no response to the email or (2) being unable to provide separate data for participants under the age of 18, these data could unfortunately not be included in this review.
This study does not describe different types of grafts or operation techniques, such as physeal-sparing ACL-R, partial transphyseal, or transphyseal techniques, and does not provide any information about risk related to graft maturation.
In addition, there is a paucity of literature pertaining effectiveness of pre- and postoperative bracing in pediatric ACL-injured athletes.
Clinical Relevance
A safe and successful RTS after pediatric ACL-R should be established and several factors then considered. A minimal assessment should entail hop testing, incorporating movement quality as well as QS and HS testing. A minimum LSI of 90% must be pursued for HS and QS as well as for the hop tests, and postinjury data should be collected as early as possible after trauma as these will serve as reference to strive for during rehabilitation. Quality of movement such as ‘soft landing’ during the hop tests is essential as stiff landing strategies may result in larger stress on the ACL. 53 New sensor technology will allow clinicians to collect kinematic data so they will have insight into movement quality, not only in the clinical situation but also in the sport-specific tasks and context. 36 This is a new domain to be discovered in the near future.
A minimum score of 85% should be strived for on the Pedi-IKDC score. Readiness to RTS should be monitored during the rehabilitation process and not only at the end stage at RTS testing. Also, psychological health should be subject of ongoing attention as quality of life is likely to be impaired in this young age group after knee injury.
Transferring the skills learned from a rehabilitation setting toward the specific sporting context is an import not-to-be-missed aspect of the RTS continuum. So rehabilitation should, for example, take place on the field or athletic track at some stage. Having a prosperous rehabilitation or not, the advice is to wait at least 9 months after ACL-R before RTS, and in pivoting sport this should be a minimum of 12 months as longer RTS duration is associated with a lower reinjury risk. 5
Conclusion
A wide set of POMs and PROMs are available for assessment after pediatric ACL-R. Clear criteria are rarely applied to guide RTS decision-making. Currently used LSI thresholds likely overestimate knee function: knee function of the nonaffected knee deteriorates, and biomechanics are likely still impaired when limb symmetry is within previously reported ranges. In the absence of functional assessment, insufficient knee function will remain undiscovered. Testing to aid RTS decision-making should include the individual (biomechanics), task (sport type), and environment. Psychological monitoring is essential in this young population with knee injury.
Supplemental Material
sj-docx-1-sph-10.1177_19417381221146538 – Supplemental material for Reconsideration of Return-to-Sport Decision-Making After Pediatric ACL Injury: A Scoping Review
Supplemental material, sj-docx-1-sph-10.1177_19417381221146538 for Reconsideration of Return-to-Sport Decision-Making After Pediatric ACL Injury: A Scoping Review by Anne Hendrika Johanna Pauw, Tristan Marcel Frank Buck, Alli Gokeler and Igor Joeri Ramon Tak in Sports Health: A Multidisciplinary Approach
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.