
Abstract
Background:
Although preservation of meniscal tissue is paramount, there are occasions when repair of a torn meniscus is not possible. The surgical option may be a partial meniscectomy, the objective being to alleviate the patient’s symptoms with resection of only that portion of the meniscus that is no longer functioning but is the cause of symptoms. Previous studies have questioned the need to perform such surgery and have recommended nonoperative treatment instead. Our goal was to compare the outcome of partial meniscectomy with that of physiotherapy alone for irreparable meniscal tears.
Hypothesis:
Clinical outcome following arthroscopic partial meniscectomy may differ from that following physiotherapy alone, for patients with symptomatic irreparable meniscal tears.
Study Design:
Nonrandomized prospective cohort study.
Level of Evidence:
Level 2.
Methods:
Patients satisfying the inclusion criteria chose to undergo knee arthroscopy (group A) or physiotherapy (group B). The diagnosis of a meniscal tear was made on physical assessment and magnetic resonance imaging examination. The meniscal tear was preventing them from continuing with their regular weightbearing exercise. Outcomes of interest were the following patient-reported outcomes (PROs): the Knee Osteoarthritis Outcome Score (KOOS) and Tegner Activity Score (TAS), with minimal clinically important differences being 10 and 1, respectively. PROs were completed at baseline, and at 1-year and 2-year follow-up. Changes in scores within and between groups were compared using analysis of variance and Wilcoxon tests (P <0.05). A power analysis demanded 65 patients in each group to produce a power of 80% and a P value of 5%.
Results:
Of 528 patients enrolled in the study, 10 were lost to follow-up and 8 were excluded. Data were complete for 269 in group A, and 228 in Group B. Group A and B were similar in terms of age (41.1 years, SD 7.8 vs 40 years, SD 13.3), body mass index (22.5 kg/m2, SD 3.1 vs 23.1 kg/m2, SD 2.3), radiographic grade of osteoarthritis (median grade 2, range 0-3 in both groups), gender (male:female = 134:135 vs 112:116), and duration of symptoms (44.4 days, SD 5.6 vs 46.6 days, SD 8.8), with P >0.05. At both 1-year and 2-year follow-up, Group A had higher scores in the mean total KOOS (88.8, SD 8.0 vs 72.4, SD 3.8), as well as in all subscales within the KOOS, and the TAS (median 7, range 5-9 vs median 5, range 3-6), with P <0.001 for each variable.
Conclusion:
Performing a knee arthroscopy with partial meniscectomy is associated with improved KOOS and TAS, relative to treatment with physiotherapy alone, at 2-year follow-up.
Clinical Relevance:
Physically active patients with symptomatic irreparable meniscal tears may experience a better clinical outcome following knee arthroscopy, relative to to physiotherapy alone.
The role of knee arthroscopy for some meniscal tears continues to be debated. Absolute indications for arthroscopy would include a locked knee and whenever a meniscal repair with preservation of meniscal tissue is likely to be possible, especially in younger patients. In many patients, a surgical repair of the meniscus is not possible, and the arthroscopic treatment involves excision of the unstable irreparable portion of the meniscus. This partial meniscectomy may alleviate symptoms but does not restore the function of the meniscus. There has been increased interest in nonoperative management of meniscal tears since the recent publication of research reporting that sham surgery was as effective as partial meniscectomy for degenerate meniscal tears. 25 In this study, one-third of eligible patients refused to take part, patients had symptoms for at median duration of 10 months, and the diagnosis of a meniscal tear was based on magnetic resonance imaging (MRI). The results of that research may not be applicable to patients with mechanical symptoms of sufficient severity that they are unable to delay treatment for as long as 10 months.
The discussion is complicated by multiple variables associated with meniscal tears and inconsistent use of terminology, including in diagnosis, etiology, symptomatology, severity of degeneration, patient variables, and definition of successful treatment. It is unlikely that the optimal treatment for all meniscal tears is the same in all patients.
The goal of the current study was to compare clinical outcomes in physically active patients presenting with a symptomatic meniscal tear, diagnosed on MRI and treated with arthroscopic partial meniscectomy, followed by postoperative rehabilitation, relative to treatment with physiotherapy alone.
Methods
Patients presenting to the lead author between February 1, 2013 and February 1, 2020 who satisfied the inclusion criteria in Table 1 were asked to take part in the study. The study criteria selected physically active patients with meniscal injuries that reduced their ability to continue with their usual physical activity, but excluded patients with true locking, significant ligament injury, and/or osteochondral lesion. All patients had to be fit for a general anesthetic and willing to provide consent to take part. “Physically active” was defined as taking part in weightbearing physical activity ≥3 times per week of ≥20 minutes duration.
Inclusion and exclusion criteria
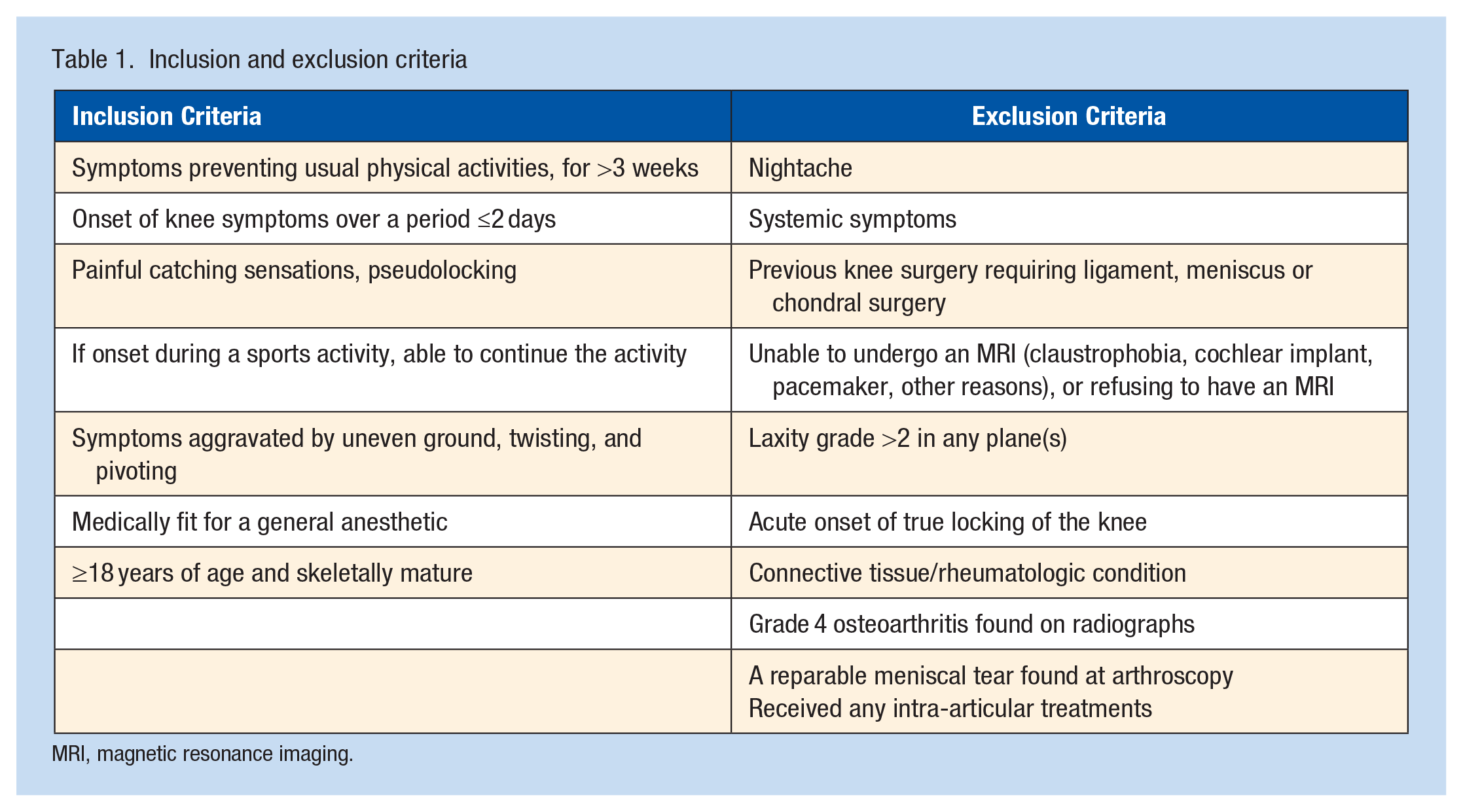
MRI, magnetic resonance imaging.
The selection criteria included a history of mechanical symptoms (painful catching symptoms), subacute onset (over a period of <3 days), the absence of an acute twisting or contact/traumatic injury, symptoms present for ≥3 weeks, and preventing patients from taking part in their usual physical activity. The examination findings used as inclusion criteria have been used in similar previous studies and may be more accurate than MRI for the diagnosis of meniscal tears. 23 These were an effusion within the knee and tenderness over a joint line or chondral surface. To clinically diagnose a meniscal tear, the patient had to have 2 of the following 3 findings: (1) medial or lateral joint line tenderness, (2) pain during McMurray’s test, and/or (3) an effusion. Patients were excluded if they had received any intra-articular injection therapy (local anesthetic, corticosteroids, platelet-rich plasma, stem cells, or viscosupplementation), before or during the follow-up period.
The MRI was performed on a 1.5-T or 3-T MRI machine, using standard MRI sequences. The chondral degeneration seen on the MRI was graded 0 to 4 for each compartment using the validated International Cartilage Repair Society (ICRS) criteria.6,26 A meniscal tear was defined as an abnormal meniscal signal extending to one of the articular surfaces, missing meniscal tissue, and/or a displaced fragment.9,22 All images were reported on by fellowship-trained radiologists with a subspecialist interest in musculoskeletal MRI. For those patients not undergoing a knee arthroscopy, the MRI was repeated at 2 years after presentation.
All patients had a series of radiographs performed that included a posteroanterior (PA) weightbearing view, lateral view, and skyline views. The anatomic axis was measured using the PA weightbearing views and the technique described and validated by Iranpour-Boroujeni et al. 17 Patients were excluded from the study if they had a varus knee (anatomic axis <0°) or valgus knee (anatomic axis >8.5°). Although the use of long-leg mechanical axis views would have provided a more accurate measurement of the mechanical axis, this was deemed by the ethics committee to be an unacceptable additional exposure to radiation. Patients with advanced osteoarthritis (OA), defined as grade 4 Kellgren-Lawrence radiographic changes on radiographs, 19 were excluded on the basis that the severity of the OA was felt to be the most likely cause of the pain in these patients.
Patients selected which treatment they would like to undergo. They were informed that if they underwent a knee arthroscopy, the goal of the surgery would be to correct those symptoms caused by a meniscal tear, if confirmed at the time of surgery. It was explained that the MRI is not 100% accurate and therefore some patients may have false-positive MRI diagnoses. They were told that a repair of the meniscus would be performed if possible. Otherwise, a partial meniscectomy would be performed, with excision of only the damaged portion of the meniscus. Patients were also offered physiotherapy as an alternative treatment, following a protocol used successfully to improve patient outcomes for this indication. 27 Patients were told that there was no high-level evidence to assist with their choice of treatment. Patients undergoing knee arthroscopy comprised Group A, those undergoing physiotherapy comprised Group B. Group B patients were informed that they could change treatment group at any stage if they were not happy with their outcome. Patients were informed that it they did not wish to take part in the study, this would not impact their treatment.
Group A patients underwent a standard knee arthroscopy. The severity of the worst area of chondral damage in each of the compartments was recorded using the ICRS system,6,26 as well as the presence or absence of a meniscal tear defined as a disruption of the joint surface of the meniscus into which the tip of the arthroscopic probe could be introduced, and/or a portion of the meniscus could be displaced. Patients who underwent a meniscal repair were excluded from the study. In these patients, an arthroscopy was clearly indicated. The goal of the study was to include patients whose meniscal tears were not amenable to surgical repair. Group A patients were referred for a maximum of 3 weeks of physiotherapy to rehabilitate them after the knee arthroscopy as opposed to treating the meniscal tear, which had been addressed arthroscopically.
Group B patients were referred for physiotherapy to follow a standardized protocol consisting of both neuromuscular and strengthening exercises, of ≥12 week’ duration. 27
The primary outcomes of interest included the Knee injury and Osteoarthritis Outcome Score (KOOS) and the Tegner Activity Score (TAS). The KOOS is a 42-item self-administered knee-specific questionnaire, assessing 5 separate subscales: pain (9 items), other symptoms (7 items), activities of daily living (ADL) (17 items), sport and recreation (5 items), and knee-related quality of life (4 items). Raw scores are converted to a score between 0 and 100, where 100 is the highest level of knee function and 0 the lowest. It is reliable, responsive, and has been validated for both short- and long-term follow-up studies of knee injury. The minimally important change is 10 points. 8 The TAS is a standardized, validated 10-point scale, used to grade work and sporting activity, with a value of 1 being the minimally important change. 5
SPSS computer software (Version 22; IBM) was used to perform the statistical analysis. Baseline characteristics in the treatment groups were compared using Chi-square tests for gender, and analysis of variance (ANOVA) for age, body mass index (BMI), and KOOSs. Nonparametric analysis (Wilcoxon test) was used to compare TAS at baseline, and the radiographic grade of OA. Changes in KOOSs over time were compared, both within and between groups, using mixed model ANOVA, and the Wilcoxon test for changes in TASs. A P value of <0.05 was regarded as statistically significant, using 2-sided probability. Using 10 as a minimally important change in the total KOOS and 15 as the standard variation, 65 patients were required in each group to produce a power of 80% and a P value of 5%. 8
Secondary outcomes of interest included any complications, return to the operating theater, and performance of further surgery. All patients in Group B were also asked to undergo a repeat MRI 24 months after the initial MRI, to determine whether the MRI diagnosis had changed, and/or whether the meniscal tear remained visible. This was not performed on the patients in Group A as the meniscal fragment had been excised and therefore assessing healing of it was deemed irrelevant.
The study was approved by the Ethics Committee of the institution where the research was performed and registered (Barton Private Hospital, ACT, Australia) and was performed in accordance with the Declaration of Helsinki, and all patient information remains anonymous. Patients provided consent for their anonymized data to be used for research and the dissemination of research findings.
Results
Of the 537 patients who satisfied the inclusion criteria, 528 enrolled in the study. A total of 287 patients elected to undergo knee arthroscopy, comprising Group A, and 241 elected for physiotherapy, comprising Group B. Figure 1 is a patient flow chart; 13 patients crossed from Group B to Group A during the first 12 months and their data were not included in the final analysis. In all, 10 patients were lost to follow-up, all from Group A; 9 of these patients had relocated (on follow-up via the internet none had experienced significant complications) and 1 had moved overseas and was not contactable. In addition, 8 patients in Group A were excluded because they underwent a meniscal repair rather than a partial meniscectomy. This was because the goal of the study was to study the outcome after partial meniscectomy, not meniscal repair.
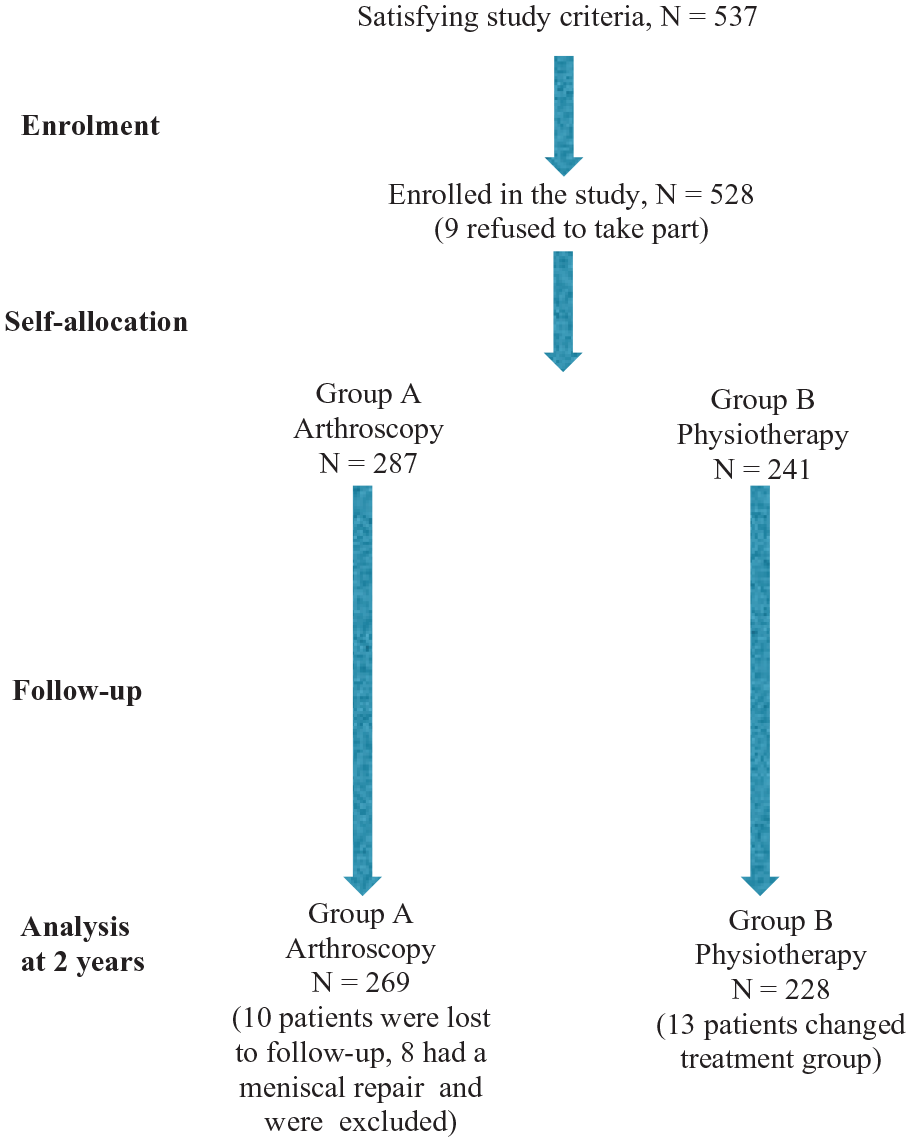
Patient flowchart.
Table 2 details the data collected and the results of statistical analysis. The 2 groups were similar in terms of mean age, male:female ratio, BMI, radiographic grade of OA, baseline KOOS and Tegner scores, and duration of symptoms before treatment.
Data for patients included in study at baseline, and at 1-year and 2-year follow-up with results of statistical analysis expressed as a P value, comparing the changes in groups over time a
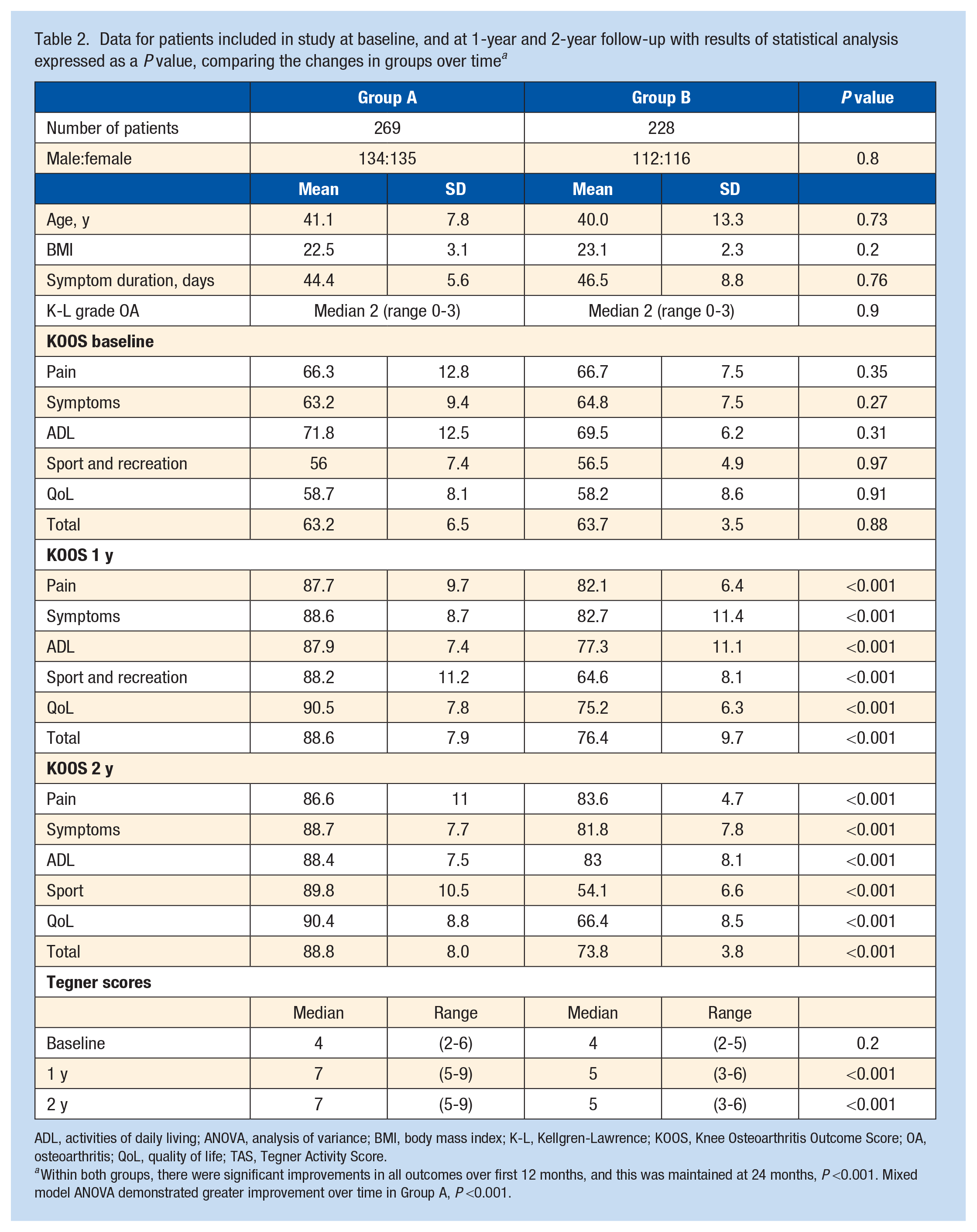
ADL, activities of daily living; ANOVA, analysis of variance; BMI, body mass index; K-L, Kellgren-Lawrence; KOOS, Knee Osteoarthritis Outcome Score; OA, osteoarthritis; QoL, quality of life; TAS, Tegner Activity Score.
Within both groups, there were significant improvements in all outcomes over first 12 months, and this was maintained at 24 months, P <0.001. Mixed model ANOVA demonstrated greater improvement over time in Group A, P <0.001.
All subscales within the KOOS, and the total scores, showed a greater improvement in Group A than Group B, at both 12 and 24 months after surgery, with P <0.001. Tegner scores also improved significantly more in Group A, than Group B, with P <0.001.
A total of 13 patients crossed over from Group B to Group A, all within the first 12 months, citing deteriorating knee function as their reason. Their data were not included in the analysis as they had completed only baseline data before changing treatment groups.
With regard to complications, 3 patients in Group A required an aspiration for hemarthrosis, 12 had significant bruising related to portals, and there were 3 deep vein thromboses. In Group B, there were 2 cases of pseudogout and 3 deep vein thromboses. There were 3 cases of spontaneous osteonecrosis of the knee in Group B, and 1 in Group A. These were all treated with a protocol of nonweightbearing until pain free, and all recovered without further treatment. The incidence of complications was too low to allow statistical comparison of the groups.
During the follow-up period, 11 patients in Group A had a similar procedure performed on their contralateral knee, but no patients underwent any further knee surgery on the index side. Apart from the 13 patients who crossed over treatment groups, none of the other patients in Group B had surgery performed on their injured knee.
A total of 188 patients in Group B had a repeat MRI 2 years after enrolment; 7 patients refused because their symptoms had resolved, while 33 offered no reason. In all 188 patients, the repeat MRI reported that a “meniscal tear” was still present.
Discussion
The principal finding of this study is that patients satisfying our inclusion criteria experienced significantly greater improvement after a knee arthroscopy in terms of KOOSs and TASs at 2 years postsurgery relative to those patients who chose physiotherapy. Although their KOOSs were inferior, only 13 of the 241 patients in Group B crossed over to Group A. The results of this study are applicable to physically active patients with clinical features consistent with a meniscal tear who select their treatment.
Our inclusion criterion selected symptomatic patients with a meniscal tear diagnosed using both clinical assessment and MRI. Although mechanical symptoms may not reliably diagnose a meniscal tear, when combined with physical signs, they are more accurate than MRI.12,23 All patients in Group A had meniscal tears confirmed at arthroscopy, while in Group B the diagnosis was not confirmed arthroscopically, and some of these may be false positives. The presence of false-positive diagnoses in Group B may be expected to bias the study in favor of this group. Some of these patients may have no significant pathology within the knee, and thus will have a favorable prognosis with any treatment. In all 188 patients in Group B who had a repeat MRI 2 years after presentation, the meniscal tear remained present and these may be false-positive diagnoses, meniscal tears that did not heal, or asymptomatic meniscal tears. There were 8 patients in Group A who were found to have repairable meniscal tears at arthroscopy, and these were excluded from the study.
A confounding factor in our study, and in much of the published research performed on the nonoperative management of meniscal tears, is the relative inaccuracy of MRI.4,11,20,23 The accuracy of MRI for the diagnosis of meniscal tears has been reported to be only 80% to 96%, is less accurate than clinical assessment, and ≥56% of MRI-diagnosed meniscal tears may be incidental asymptomatic findings, especially in older men.6,7 This is problematic for the validity of any research that uses MRI diagnosis as a key inclusion criterion without allowing for its inherent inaccuracy.21,27 Papers refer to the common diagnosis of meniscal tears on MRI in asymptomatic persons, without questioning the accuracy of the MRI. 14 Even if there is a meniscal tear present at arthroscopy, there is no certainty that this is the source of the patient’s symptoms. Other research has questioned the role of routine MRI for many patients presenting with knee symptoms. Adelani et al 2 found that 48% to 95% of MRIs performed before seeing an orthopaedic surgeon made no contribution to treatment, with significant financial repercussions for the health system. The randomized controlled study performed by Gauffin et al 13 used “meniscal symptoms” as an inclusion criterion rather than relying on MRI diagnosis, and found these patients, despite an average duration of symptoms of 7 months, did better with arthroscopy compared with physical therapy alone in a randomized controlled trial (RCT). Hence, clinical assessment may be more useful for selecting those patients appropriate for knee arthroscopy.
There has been a tendency to classify meniscal tears as either traumatic and occurring in young patients, or degenerate and occurring in older patients. 13 Some studies have attempted to specifically exclude traumatic tears on the basis of a the relationship between the onset of symptoms and an “obvious traumatic event,” thus possibly including only patients with stable meniscal tears and/or false-positive MRI diagnoses that are unlikely to have an arthroscopically remediable source for their symptoms. 24 This classification of meniscal tears is an oversimplification, with meniscal tissue shown to be on a continuum with regard to the degree of degeneration and the vulnerability to tearing. 29 Recommendations and position statements based on this arbitrary classification and the presumed accuracy of MRI are likely to be impractical and/or incorrect.3,10,24,28 The specific morphology of the tear will also influence outcome after partial menisectomy. 18 For these reasons, the authors believe that the nature of the symptoms with which the patient presents are more useful as indicators as to whether or not an arthroscopy is likely to provide clinical benefit.
There are other weaknesses in studies used to support the role of physiotherapy alone over arthroscopy for meniscal tears. Volunteer bias is present to some degree in all the published studies including RCTs, with up to 75% of patients satisfying the inclusion criteria refusing to take part.15,25 This volunteer bias may result in those patients with the most debilitating mechanical symptoms, and most appropriate indications for arthroscopy refusing to take part in an RCT with a 50% chance of not having an arthroscopy performed.
Most of the published research comparing knee arthroscopy with nonsurgical management of meniscal tears has suffered in terms of quality. A meta-analysis reviewed the current literature and was able to find only 10 trials suitable for inclusion. 1 Of these 10 trials, using the Cochrane “risk-of-bias tool,” 9 studies had ≥1 design feature consistent with a high level of bias. 16 The Sihvonnen et al 25 study was deemed to have a low risk of bias, but did have a significant volunteer bias with one-third of eligible patients opting out. All patients in that study had symptoms present for a median duration of 10 months, and therefore the study was unlikely to include those patients with more acute debilitating symptoms likely to be more amenable to arthroscopic surgery. Sihvonnen et al 25 excluded patients with an obvious traumatic onset of symptoms, and included only degenerate meniscal tears without a valid definition of “obvious” or “degenerate.” Despite these significant weaknesses in 90% of their pooled data, Abram et al 1 concluded that performing an arthroscopic partial meniscectomy is not appropriate for all patients with both knee pain and a meniscal tear, and went on to state that there may be a benefit from arthroscopy compared with physiotherapy for patients without OA. Our study confirms that those patients with knee pain and a meniscal tear can benefit from knee arthroscopy when the source of the pain is mechanical in nature and related to the meniscal tear.
Weaknesses of this study include the lack of randomization and volunteer bias. These factors raise some concerns regarding the study’s outcome. In addition, we did not consider medial and lateral meniscal tears separately, because to do so would have reduced the power of our study to below the level we regarded as acceptable. The study is ongoing and when there is sufficient data this may become possible. The relative inaccuracy of MRI for diagnosing meniscal tears in Group B is a potentially significant confounding factor. The inclusion criteria included symptoms for a very short period of ≥3 weeks. This criterion applied to patients in both treatment groups and thus would be expected to influence the outcome equally in both groups. The final mean duration of symptoms was closer to 6 weeks and was similar in the 2 groups. In all those patients in the physiotherapy group who underwent a repeat MRI 2 years after their enrolment in the study, the meniscal tear was still visible. This may represent a false positive diagnosis at the initial presentation and/or at 2-year review.
Conclusion
We found that physically active patients presenting with subacute onset of mechanical symptoms and corresponding physical signs, who self-selected their treatment, had a better outcome after arthroscopic partial meniscectomy, and postoperative rehabilitation relative to physiotherapy alone, in terms of patient-reported outcomes and level of activity at 2-year follow-up.
Footnotes
The authors report no potential conflicts of interest in the development and publication of this article