
Abstract
Background:
Fundamental movement skills (FMS) are critical components to lifelong participation in sports and physical activity. With the rise in early sports specialization, mastery of motor skills may be limited in youth athletes. The purpose of this study was to assess FMS proficiency in highly active middle school athletes and determine whether proficiency differed between specialization levels and sex.
Hypothesis:
(1) Most athletes would fail to achieve proficiency in all domains of the Test of Gross Motor Development (TGMD-2), (2) highly specialized athletes would demonstrate lower proficiency in all domains of the TGMD-2, and (3) male athletes would demonstrate higher proficiency than female athletes.
Study Design:
Cross-sectional.
Level of Evidence:
Level 4.
Methods:
A total of 91 athletes were recruited (44 male, 12.6 ± 0.9 years). Activity level was quantified using the Hospital for Special Surgery (HSS) Pediatric Functional Activity Brief Scale (Pedi-FABS), specialization level was determined using the Jayanthi Specialization Scale, and the TGMD-2 was used to assess FMS proficiency. Descriptive statistics were used to describe gross motor, locomotor, and object control percentile rank. A 1-way analysis of variance (ANOVA) was used to assess differences in percentile rank between low, moderate, and high specialization groups and independent samples t tests were used to compare sexes (α < 0.05).
Results:
Mean Pedi-FABS score was 23.6 ± 4.9. In total, 24.2%, 38.5%, and 37.4% of athletes classified as low, moderate, and highly specialized, respectively. Mean percentile ranks were 56.2%, 64.7%, and 62.6% for locomotor, object control, and gross motor domains, respectively. No athlete achieved a percentile rank >99% in any domain of the TGMD-2, and there was no significant difference between specialization groups or sex.
Conclusion:
Despite high activity levels, no athlete demonstrated proficiency in any domain of the TGMD-2, and there was no difference in proficiency between specialization levels or by sex.
Clinical Relevance:
Sport participation, regardless of level, does not ensure adequate mastery of FMS.
The concept of physical literacy has received increased attention over the past several years. With youth physical activity levels declining, early attrition and sedentary screen time at an all-time high, and the push for early sports specialization, children are not being exposed to as wide of a range of motor skills as they have been in previous years.7,12,15 It is postulated that this lack of exposure may be a contributing factor to the overwhelmingly low fitness levels facing modern youth.5,16 Physical literacy is a multifactorial concept that has been defined by Whitehead et al 35 as “the motivation, confidence, physical competence, knowledge, and understanding to value and take responsibility for engagement in physical activities for life.” The majority of physical literacy research has focused on the physical motor competence domain of this definition with a primary focus on fundamental movement skills (FMS).4,9,36 FMS consist of 12 motor skills that can be broken down into 2 main domains: object control and locomotor. Object control skills include overhead throwing, catching, kicking, striking, underhand rolling, and dribbling, whereas locomotor skills consist of running, jumping, hopping, galloping, sliding, and leaping. FMS have been recognized as a critical component to lifelong participation in sports and physical activity, with positive associations between motor competency and physical activity, youth sports, and fitness.2,21,24
Even with the known benefits of achieving motor competency, the overall competence in modern-day children and adolescents is alarmingly low and appears to decline with age.10,18,30 Erwin et al 10 assessed motor skill competency in a group of 180 fourth and fifth graders and found only 47% to be making satisfactory progress toward sufficient motor competency. Similarly, O’Brien et al 28 evaluated performance of 9 FMS tests in a group of 12- to 13-year-olds (N = 242) with only 11% of the participants achieving mastery or very near mastery for all skills. This same study also found a significant difference in the total mean composite FMS score between male and female participants, with adolescent males scoring higher than their female counterparts. 28
It is hypothesized that the rise in early sports specialization may be a contributing factor to the overwhelmingly low levels of motor competence observed in children and adolescents.17,26 In the United States, it has been reported that roughly 30% of athletes are highly specialized in their sport at a young age. 23 The most commonly used definition of sports specialization is intense training in a single sport at the exclusion of others, with a “highly” specialized athlete participating in 1 main sport, participating in that sport >8 months out of the year, and quitting other sports to play the main sport.22,23 Limiting sports participation to only a single sport may reduce the opportunities for children to be exposed to a variety of motor and sports skills, which, in turn, may negatively affect motor development.17,26 Essentially, highly specialized athletes may become exceptional at only 1 set of movement skills associated with their sport. Consequently, they may neglect to master the remaining skills required to achieve overall gross motor proficiency.
With the rise in early sports specialization coupled with the decline in overall gross motor skills in children, it is unknown if sports participation ensures adequate levels of FMS proficiency. Therefore, the purpose of this study was to assess FMS proficiency in a group of highly active middle school athletes and to determine whether differences in proficiency existed between levels of sports specialization and sex. Our hypotheses were as follows: (1) the majority of highly active athletes would fail to achieve proficiency in all domains of the Test of Gross Motor Development (TGMD-2), a measure of FMS proficiency; (2) highly specialized athletes would demonstrate significantly lower proficiency in all domains of the TGMD-2; and (3) male athletes would demonstrate significantly higher proficiency in all domains compared with female athletes.
Methods
Participants
In this cross-sectional study, a group of early teenage athletes (N = 91, 44 male athletes) were recruited from middle school and club sport teams in Florida, Texas, and Missouri (Table 1). Male and female participants between the ages of 11 and 13 years who were active participants in organized or recreational sports within the last 12 months were included in the study. This age range was selected as it is a critical time point in sports participation trajectories where children may be making decisions related to sports specialization and may also be at risk for early sport dropout.34,27 Participants were excluded if they had a previous musculoskeletal injury in the last 3 months, a current injury (classified as an incidence for which medical attention was sought), or a diagnosis that is known to affect gross motor performance. Before the start of the study, this research was approved by each institution’s respective institutional review board. Informed written parent consent and participant assent were obtained before participation in the study. Data were collected from May 1, 2019 to March 31, 2022.
Participant characteristics (mean ± SD) a
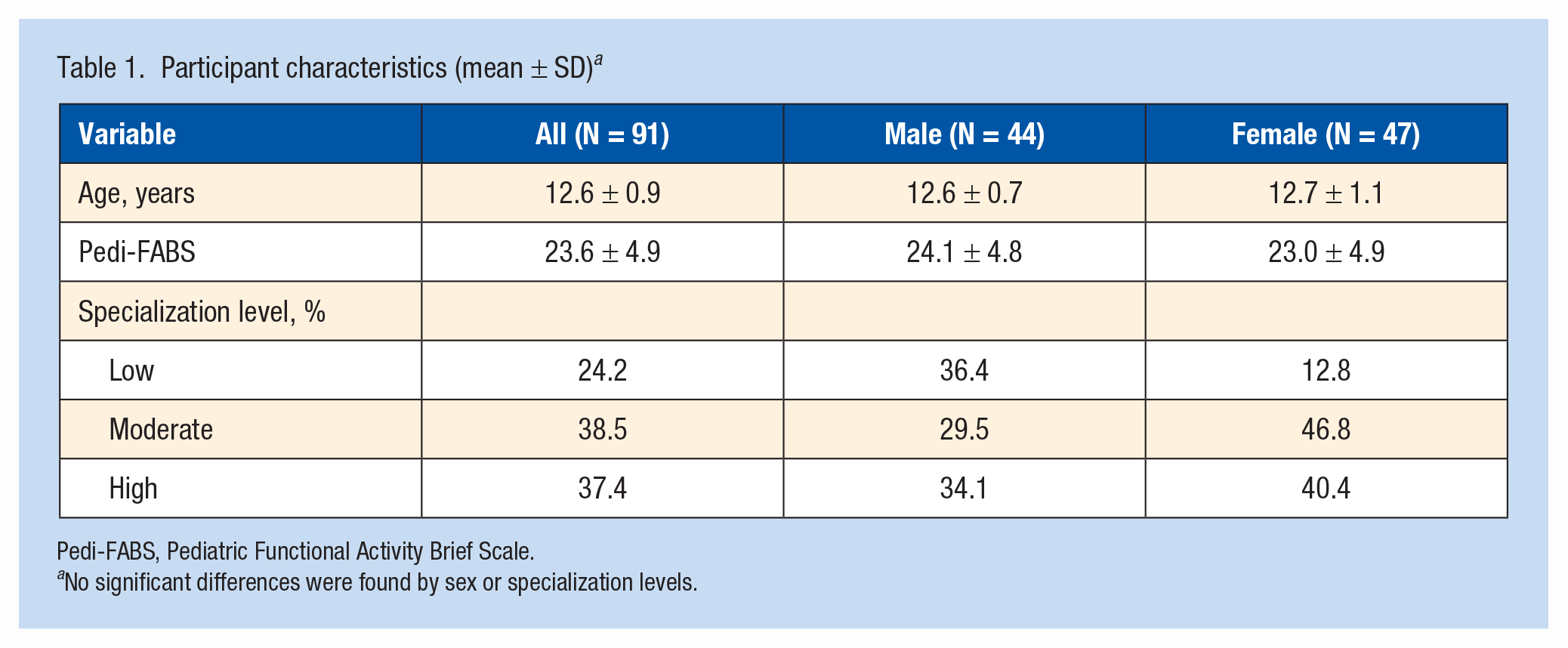
Pedi-FABS, Pediatric Functional Activity Brief Scale.
No significant differences were found by sex or specialization levels.
Measures
All measures were conducted off-site at the participant’s school or club sports facility or onsite at 1 of the 3 participating institutions, which included 2 hospital-based outpatient rehabilitation centers and 1 sports science laboratory. Testing location was chosen based on geographic location of participants. All measures were performed by trained research team members, which included 5 doctors of physical therapy and 3 biomechanists. Each research team member participated in a 2-hour training session before data collection to standardize procedures for quality assurance. All data were collected in a single visit for each subject and entered into a REDCap database at the host institution (Research Electronic Data Capture). 19
TGMD-2
FMS proficiency was assessed using the TGMD-2, which has demonstrated validity and reliability in assessing gross motor abilities and competency in children aged 3 to 11 years. 33 Despite the age limitations of the TGMD-2, this assessment tool was chosen based on its specific design to measure FMS proficiency. The test assesses 12 motor skills, divided into 2 domains: object control skills (overhead throwing, catching, kicking, striking, underhand rolling, and dribbling) and locomotor skills (running, jumping, hopping, galloping, sliding, and leaping). 33 The total duration of the assessment is approximately 15 to 20 minutes per participant. Participants performed each skill twice in a standard order outlined in the TGMD-2 test manual. 33 Skills were evaluated visually in real time. Each skill includes several performance criteria, in which a score of 1 is awarded for correct performance and a score of 0 awarded for incorrect performance of each criteria. This scoring procedure was completed for each of the 2 test trials and scores were summed to obtain a total raw skill score for each skill. Raw skill scores were added to obtain locomotor and object control subtest scores which were subsequently converted into standard scores and percentiles. The sum of the 2 subtest scores were then added and the gross motor quotient (GMQ) was calculated. 33
Pedi-FABS
The Hospital for Special Surgery (HSS) Pedi-FABS was used to quantify each participant’s activity level. 11 The Pedi-FABS is a reliable, valid, and brief rating scale of functional activity for children between 10 and 18 years of age. The scale asks questions regarding frequency of running, cutting, decelerating, pivoting, and endurance activities as well as sports competition and supervision. The Pedi-FABS was filled out independently by each participant in paper format. The total points derived from each question were summed to generate the total score with a total possible score range of 0 to 30 points. 11 The total score was compared with normative data to quantify each participant’s activity level. 11
Jayanthi Sports Specialization Scale
The Jayanthi Sports Specialization Scale was used to classify each participant’s level of sports specialization using a 3-point system. Each participant received 1 point for each “yes” response to the following 3 questions: (1) do you have 1 main sport, (2) do you spend >8 months of the year participating in this main sport, and (3) did you quit other sports to play this main sport. Participants were classified into levels of low specialization for score 0 to 1, moderate specialization for a score of 2, and high specialization for a score of 3. 23
Statistical Analysis
Descriptive statistics (mean, standard deviation, and frequency) were computed for all measures across the cohort as well as by sex and specialization level. Sex differences in locomotor, object control, and GMQ percentile ranks were compared using independent samples t tests. In addition, differences between specialization levels for all percentile rank measures were evaluated using 1-way analysis of variance (ANOVA) tests with Tukey post hoc comparisons when appropriate. A conventional 0.05 level of significance was set for all statistical tests (IBM SPSS Statistics for Windows, Version 24.0).
Results
A total of 91 middle school aged children (aged 12.6 ± 0.9 years) completed the TGMD-2 assessment, and activity scales and sport specialization levels are presented for male and female participants separately in Table 1. Mean Pedi-FABS score was 23.6 ± 4.9, indicating high levels of physical activity (Table 1), and the distribution of Pedi-FABS is depicted in Figure 1. Similarly, sport participation distribution is shown in Figure 2. For the TGMD-2, mean percentile ranks for the locomotor and object control subtests were 56.2% and 64.7%, respectively, while the GMQ was 62.6%. No athlete achieved a percentile rank of >99% in any domain of the TGMD-2. The overall level of skill proficiency was low despite high activity levels and multisport participation (76.9%) in this group of athletes. Furthermore, when considering proficiency levels in male versus female participants, there were no significant differences in locomotor or object control scores, even when controlling for age and level of physical activity (Table 2).
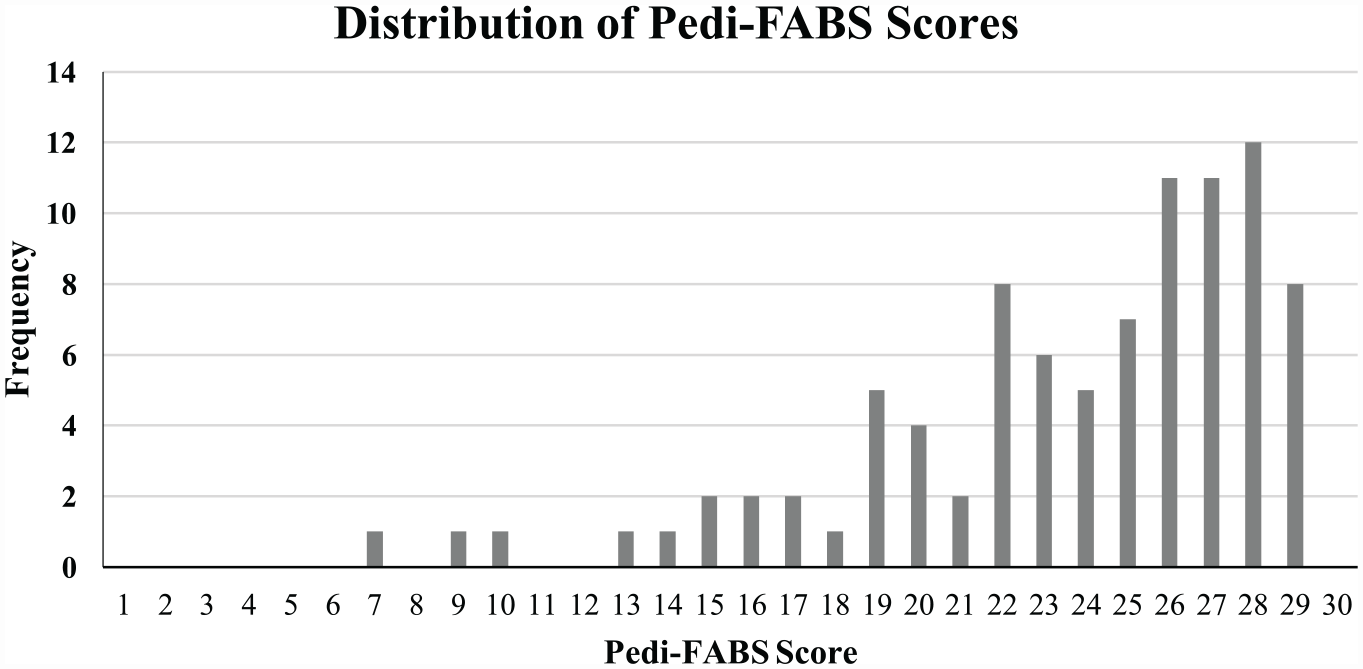
Distribution of Pedi-FABS scores. Pedi-FABS, Pediatric Functional Activity Brief Scale.
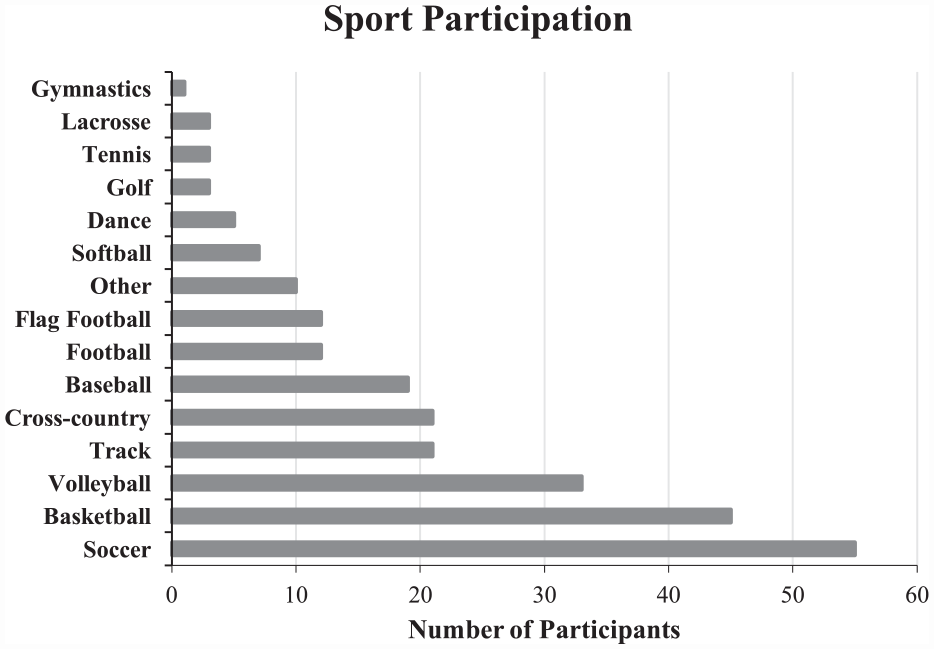
Distribution of sport participation.
Mean (SD) percentile ranks for TGMD-2 measures by sex and specialization level a
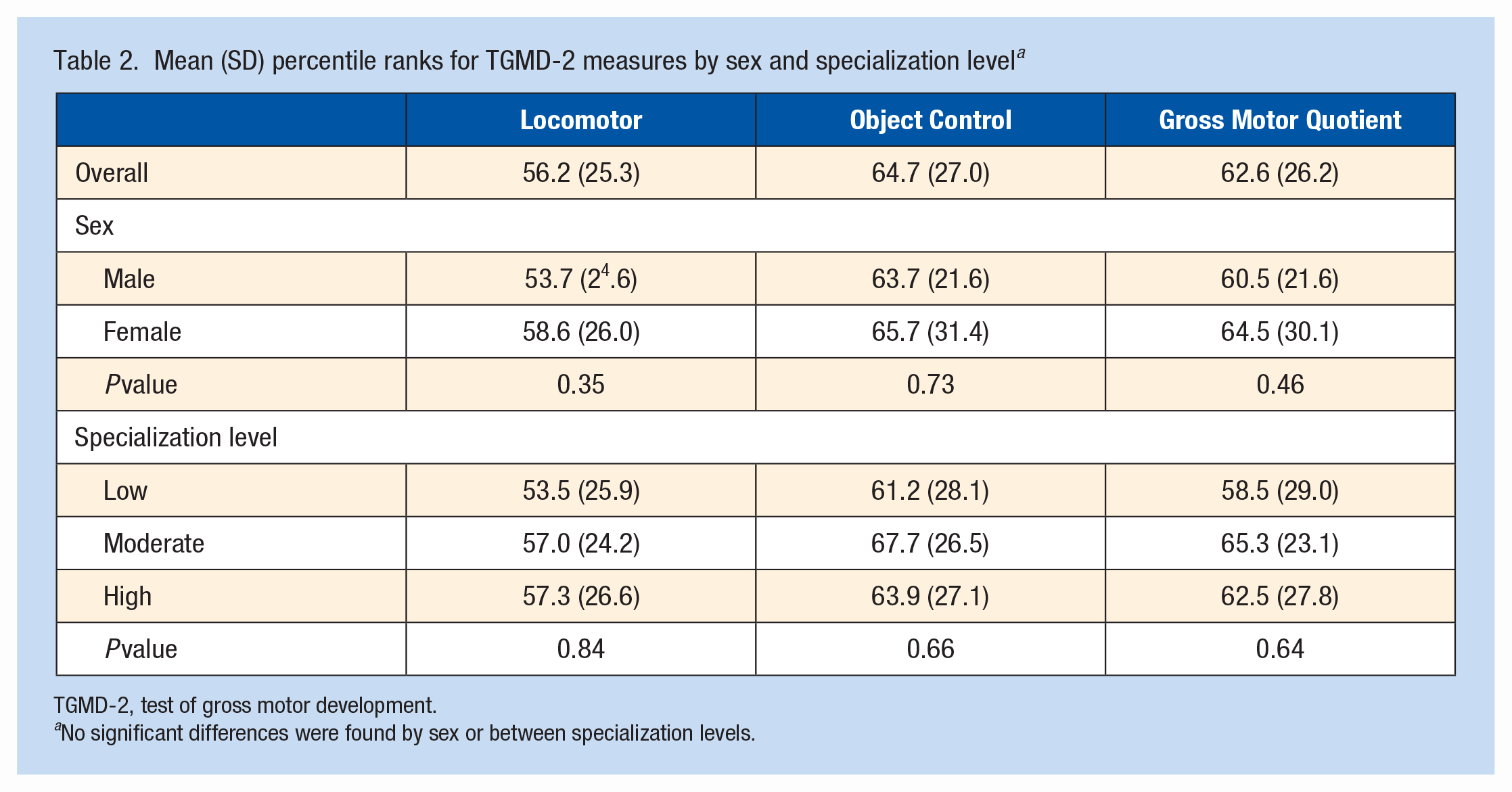
TGMD-2, test of gross motor development.
No significant differences were found by sex or between specialization levels.
Of the 91 participants tested, 76 (83.5%) reported having a main sport and 65 (71.4%) of those reported playing their main sport for >8 months out of the year. Only 38 of the 76 (41.2%) participants. Who reported having a main sport, indicated that they had quit other sports to play their main sport. According to the Jayanthi Sports Specialization scale, 24.2%, 38.5%, and 37.4% of athletes were classified as low, moderate, and high sport specialization, respectively (Table 1). In total, 75.9% of athletes were classified as moderate to highly specialized. There was no significant difference in gross motor, locomotor, or object control percentile ranks between low, moderate, and high specialization groups (Table 2).
Discussion
This study showed that, despite the high physical activity levels of this cohort, no athlete demonstrated proficiency in any domain of the TGMD-2. The mean percentile ranks for all domains ranged from 56.2% to 64.7%. Given the age of the athletes in this study (12.6 ± 0.9 years), these results are lower than expected based on published normative data for the TGMD-2, which is capped at age 10 years and 11 months. FMS proficiency, often used synonymously with motor competence, has been identified as a key component to leading a physically active lifestyle.24,31,32 Therefore, it would seem plausible that teenage children who report high levels of physical activity would also demonstrate competence in these skills. However, the findings of this study suggest that high physical activity levels may not be enough to ensure adequate motor competency development. FMS proficiency is unlikely to be achieved without appropriate practice, instruction, and feedback. 14 Although all the athletes in this study participated in sports, it is unknown whether their PA came from specific sports participation, free play, or, perhaps, physical education. It is possible that the current youth sports structure may not adequately support the development of motor competency. The rise in club sports coupled with both the decline of recreational sports and focus on winning over simply the promotion of activity may lead to greater single sport-specific skill development rather than the development of overall coordination/fundamental movement mastery. Similarly, while not the focus of this paper, the trend toward club sport participation rather than recreational sport involvement may lead to even more limited opportunity for participation in sports for children and adolescents due to cost and the perception that school aged athletes may not have the skill set to participate on club teams.
In general, the results of this study corroborate with other works that have found poor FMS proficiency in middle- and high-school aged children.3,28 This highlights the need for interventions aimed specifically at improving FMS in early to middle childhood irrespective of sports participation. We have been able to demonstrate that we cannot assume that participation in sports, even at a relatively high level, will necessarily lead to the development of adequate FMS mastery. In this study, we found no difference in FMS proficiency between athletes with various levels of sports specialization. This contradicts other works that have suggested that more specialized athletes demonstrate poorer movement patterns.6,8,13 Current guidelines recommend delaying sports specialization until age 12 years. 21 This sample had a mean age of 12.6 years, placing them right at the age where the decision to select a primary sport (specialization) is expected to occur. This may have contributed to some athletes identifying as moderate or highly specialized who just recently chose a specialization pathway. If these athletes had a multisport background up until the time of testing, and thus the time of choosing a specialization pathway, then this could explain why no differences were observed between athletes with various levels of sports specialization. The prevalence of sports specialization has been reported in the literature and ranges from approximately 13% to 36% of athletes classifying as highly specialized.1,23,32 The highest specialization rates were reported by Bell et al, 1 identifying 36.4% of high-school aged athletes as highly specialized. The lowest specialization rates were reported by Post et al, 29 with 13.4% of participants with a mean age 16.1 years classifying as highly specialized. In the current study, 41% of athletes were classified as highly specialized, which is slightly higher than what has been reported previously. This may be a result of the age differences of participants in our study, who were younger than participants reported previously. Future studies should report specialization prevalence in younger cohorts, from geographically diverse regions, and include an explicit definition of sports specialization, considering the age at which a specialization pathway is chosen. In addition, the works of Bell and Post included participants from only a single geographic region. The present study included athletes from 3 diverse regions: Florida, Texas, and Missouri. Given that specialization varies by sport, and sport availability varies geographically, this may have influenced the findings. Future studies should report specialization prevalence in younger cohorts, from geographically diverse regions, and include a more explicit definition of sports specialization, considering the age of choosing a specialization pathway. Furthermore, some athletes in the moderate specialization group reported only ever playing 1 sport, thus they answered no to the question on quitting other sports. This may have incorrectly classified them as moderately specialized when truly they were likely highly specialized. Again, this highlights the need for a more explicit way to classify each athlete’s level of sports specialization.
Lastly, no difference was found in FMS proficiency between male and female athletes in this study. This contrasts with other works which have found female athletes to have lower levels of motor competency (specifically object control skills) compared with male athletes.20,25 It was conceptualized that sex differences in motor proficiency may exist as a result of female children being provided with fewer opportunities to be physically active. In the current study; however, there was no difference in level of physical activity between male and female participants, which may be a novel finding since it highlights gender equality in the domain of physical activity. More studies are warranted to ensure that we close the gender gap and provide equal opportunities in the domain of physical activity.
Limitations
This study has limitations to note. Importantly, we did not perform reliability testing for individual raters between days or to evaluate reliability between raters scoring the TGMD-2. In addition, investigators were not blinded to each athlete’s specialization level. This might have led to bias as the investigators completed the TGMD-2 assessment. However, given the relatively low proficiency exhibited across participants in all 3 specialization groups, this is unlikely to have impacted the outcomes of the study. In this study, 75.9% of athletes were moderately to highly specialized. Given their high levels of physical activity, this study may not be generalizable to all middle school children as their activity levels are likely different from those in this study. This study does not account for potential differences in access to specialized sport training, sport participation characteristics (recreational vs competitive sports participation), socioeconomic status, or race and ethnicity as these datapoints were not collected in this study. The variability in the aforementioned variables likely contributed to participants’ motor skill proficiency. In addition, the TGMD-2 has been validated for use only in children aged 3 to 11 years. In this study, we used the TGMD-2 to assess movement in athletes up to an age of 13 years. Thus, percentile ranks for children older than 11 years were calculated with reference to normative data for children that are aged 11 years. This likely led to an underestimation of motor skill deficiency for athletes aged 12 and 13 years. However, despite the potential for underestimating motor skill deficiency, the athletes in this study still performed poorly. Furthermore, the TGMD-2 assesses only the physical domain of physical literacy. Using a tool that assesses all domains of physical literacy may have been more sensitive to differences in our cohort.
Conclusion
The results of this study suggest that motor skill proficiency is low amongst highly active middle school athletes, and there were no motor skill proficiency differences by sex and level of sports specialization. Future studies should aim to identify training or interventions that effectively address the low motor skill proficiency in pediatric athletes.
Footnotes
The authors report no potential conflicts of interest in the development and publication of this article.