
Abstract
Background:
Sacral stress fractures are a rare cause of low back pain in athletes. Given the low incidence of these fractures, there is a scarcity of data on symptomatology, risk factors, and clinical outcomes.
Hypothesis:
Patients diagnosed with sacral stress fractures would be athletes presenting with low back pain.
Study Design:
Case series of 13 patients with sacral stress fractures.
Level of Evidence:
Level 4.
Methods:
We conducted a retrospective review of medical records to identify patients diagnosed with sacral stress fractures at a single academic institution. Fractures were diagnosed on noncontrast T2-weighted magnetic resonance imaging scans and categorized using the Bakker classification system. Subjects were administered an electronic survey that asked about (1) the onset, time course, and location of pain and other symptoms; (2) time to treatment and treatment modalities pursued; (3) sports performance and time to return to sport; and (4) risk factors for stress fractures.
Results:
Of 18 eligible patients, 13 (72.2%) completed the survey with mean follow-up of 49.6 months (range, 1-144 months). Mean age was 28.0 years (range, 18-52 years); 9 patients (69.2%) were female, of whom 7 (77.8%) were premenopausal. The most common fracture type was Bakker type B (8 patients; 61.5%). Most patients presented with acute lumbosacral back pain in the setting of running/jogging activities. All patients underwent nonoperative treatment for an average of 3.8 months (range, 0-8 months) and three-quarters reported pain resolution at last follow-up. Rate of return to sport was 83.3%, but most patients reported ongoing deficits in running performance.
Conclusion:
Sacral stress fractures commonly present as acute lumbosacral back pain provoked by running sports. While the pain associated with these fractures prevents most athletes from participating in sports, nonoperative management appears to be an effective treatment modality with a high rate of return to sport.
Sacral stress fractures are rare injuries resulting from repetitive, submaximal loading of the sacrum. 20 There are 2 distinct types of sacral stress fractures: fatigue fractures resulting from abnormal stresses applied to normal bone, and insufficiency fractures resulting from normal stresses applied to abnormal bone.10,13 Fatigue fractures typically occur in young athletes with demanding training schedules and have been found to be particularly prevalent among runners. 4 In contrast, insufficiency fractures tend to occur in older patients with osteoporosis and are more common in postmenopausal women than in men. 17 While the incidence of sacral fatigue and insufficiency fractures in the US population is unknown, 10 Weber et al 17 report that 1.8% of women admitted to a rheumatology unit were found to have sacral insufficiency fractures.
Both fatigue and insufficiency sacral stress fractures typically present with diffuse pain in the low back, buttock, or pelvis. 10 These fractures frequently go undiagnosed or are mistaken for other injuries due to the diffuse nature of the pain and the relative lack of knowledge regarding sacral stress fractures.3,10,14,18 Furthermore, diagnosing sacral stress fractures may be challenging; plain radiographs are typically unrevealing, while magnetic resonance imaging (MRI) and computed tomography are far more sensitive and specific.3,13,20 Common treatments for sacral stress fractures include rest and gradual return to activity, although there is extensive variability in the literature regarding duration of rest and the specifics of rehabilitation protocols. 3 Due to their uncommon nature, the difficulty in diagnosis, and the scarcity of literature addressing sacral stress fractures, these injuries remain poorly understood. To properly diagnose, advise, and treat patients presenting with sacral stress fractures, it is crucial to characterize the risk factors associated with this entity, as well as the presentation and clinical course of patients with sacral stress fractures.
The purpose of our study was to assess the injury presentation, course, and outcomes among athletes diagnosed and treated for sacral stress fractures. Our specific aims were to (1) characterize presenting symptoms and treatment modalities used; (2) evaluate preinjury, postinjury, and posttreatment sports performance; and (3) identify known risk factors for stress fractures in this group.
Methods
Subject Identification and Eligibility Criteria
After receiving institutional review board approval (22-00291), we retrospectively reviewed patients diagnosed and treated for sacral stress fractures at a single urban academic medical center between January 1, 2010 and December 31, 2021. Patients were identified through a search of the electronic medical record system of the institution using the following International Classification of Diseases, 10th Revision, Clinical Modification (ICD-10-CM) codes: M48.48XA, S32.10XA, and M84.350A. Once an initial list was obtained, patients were screened individually for eligibility. Inclusion criteria were diagnosis of sacral stress fracture, age 16 years or older at the time of diagnosis, and willing and able to provide informed consent to participate in the study (for patients ≥18 years old) and/or assent with parental permission (for patients <18 years old). Exclusion criteria included sacral fractures of traumatic or pathologic etiology, age <16 years, inability to provide informed consent and/or refusal of parental permission, and inability to communicate in English.
Diagnostic Criteria
All patients were diagnosed and treated by 1 of 8 sports fellowship-trained orthopaedic surgeons at a single institution. A diagnosis of sacral stress fracture was suspected on the basis of the patient’s history (eg, lower back pain without a history of trauma) and physical examination findings (eg, pelvic compression test, Gaenslen’s test, squish test, single-leg standing test, hop test) and confirmed on noncontrast T2-weighted MRI scan of the pelvis. Fractures identified on MRI scans were classified using a radiographic system previously described by Bakker et al. 1 To summarize, this system classifies fractures by 3 categories: incomplete fractures of the sacral ala (Type A), complete fractures of the sacral ala (Type B), and fractures involving the sacral corpus (Type C). Each fracture type has 3 associated subtypes (A1, A2, A3) based on the exact location and pattern of the fracture.
Patient Questionnaire
An electronic questionnaire was used to collect information on each patient’s clinical presentation and treatment history, sports performance before and after treatment, and known risk factors for stress fractures. The survey was designed and administered using the REDCap data capture instrument and distributed via email.
The clinical presentation and treatment history section assessed the location of pain before treatment using a diagram of the pelvis with 6 delineated regions: (1) groin and medial thigh, (2) anterior thigh, (3) lumbosacral region, (4) gluteal region, (5) intergluteal cleft, and (6) lateral thigh. Other variables collected included laterality of pain in each of the 6 regions, location of pain in any other region of the body besides the 6 previously described, location of any associated swelling, estimated date of pain onset, acuity of onset (sudden or gradual), symptom pattern (constant or intermittent), frequency of symptoms (ranging from less than once a year to multiple times each day), precipitating factors (sitting, standing, walking, running), palliating factors, months elapsed between onset of symptoms and initial visit, previous misdiagnoses, pharmacological and nonpharmacological therapies used, duration of treatment, changes in symptoms after treatment, and pre- and posttreatment levels of pain as measured on a 10-point visual analog scale (VAS). On the VAS, 0 corresponded to “no pain at all” and 10 corresponded to “worst possible pain.”
The sports performance section assessed the patient’s preinjury participation in sports, exercise, and/or physical activity, postinjury level of participation, presence of symptoms during sports/activities, and success and timing of return to sport after treatment. For patients who participated in recreational running/jogging or running sports (track and field, cross-country, hurdling, long-distance running, marathon running, middle-distance running, relay races, sprints, steeplechase) before injury, total miles run per week (preinjury, postinjury, posttreatment), longest distance run (preinjury, postinjury, posttreatment), and average mile time (preinjury, postinjury, posttreatment) were recorded. For runners/joggers who participated in races, the survey asked how the patient’s performance changed after injury and after treatment compared with their preinjury baseline.
The risk factors section assessed the following known risk factors for sacral stress fractures and stress/insufficiency fractures in general: previous history of stress fractures, menstrual history, and oral contraceptive (OCP) use.
Results
Patient Demographics
On initial search of the electronic medical record system, 53 patients were identified. After screening the list for eligibility, 18 patients were found to have a confirmed diagnosis of sacral stress fracture with the other 35 patients excluded due to having sacral fractures of traumatic etiology or pelvic fractures that did not involve the sacrum. Of the remaining 18 patients, 13 completed the survey.
Patient demographics are summarized in Table 1. Patient ages ranged from 18 to 52 years (mean, 28.0 years) and most were female (9 patients, 69.2%). Of the 9 female patients, 7 (77.8%) were premenopausal. Of the 12 patients with available body mass index (BMI) measurements, 10 (83.3%) were of normal weight (BMI ≥18.5 and ≤25 kg/m2). Of the 11 patients with available pelvic MRIs, most (8 patients; 61.5%) had sacral stress fractures of Bakker type B. The most common subtype was B3 (Figure 1) indicating complete fracture of the sacral ala with involvement of the neural foramina or spinal canal. Follow-up time, as defined by the time elapsed from the date of diagnosis to date of survey completion, ranged from 1 to 144 months (mean, 49.6 months).
Patient demographics
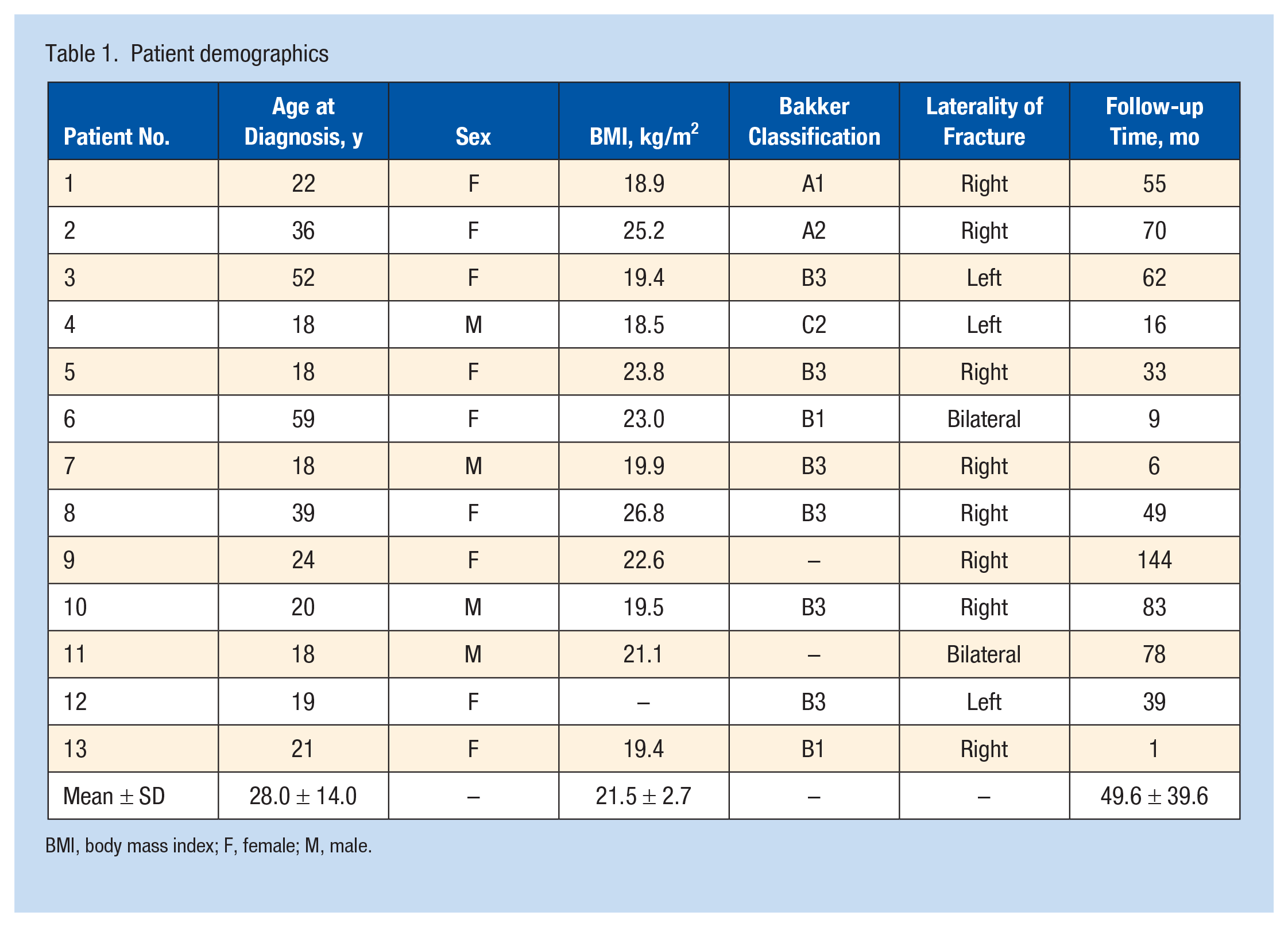
BMI, body mass index; F, female; M, male.
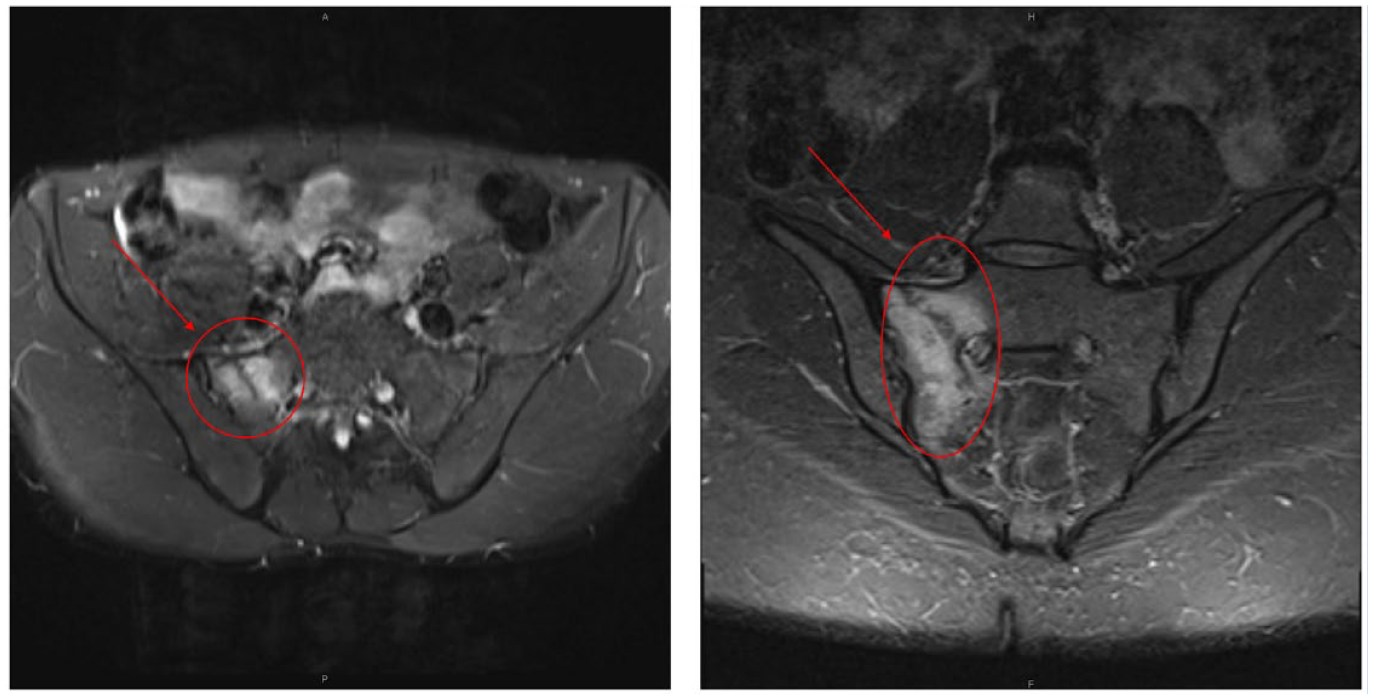
T2-weighted pelvic MRI scan of patient 5 revealing a Bakker type B3 sacral stress fracture (outlined in red and indicated with an arrow) on axial view (left) and coronal view (right). MRI, magnetic resonance imaging.
Clinical Presentation and Treatment History
The location and laterality of pelvic pain experienced by each patient is summarized in Table 2. The majority of patients (10 of 13, 76.9%) reported experiencing back pain in the lumbosacral region. A minority of the group reported having pain in other regions of the pelvis, with the most common being the lateral thigh (5 of 13, 38.5%) followed by the gluteal regions (3 of 13, 23.1%). All but 1 patient (9) reported that the pain in each pelvic region was of the same laterality as the sacral fracture confirmed on MRI scan. Three patients (Nos. 1-3) reported having pain in nonpelvic locations, with patients 1 and 3 describing pain radiating up the spine and patient 2 describing pain radiating down the lower extremity. Only 1 patient (No. 10) reported associated swelling, which he localized to the lower back and ipsilateral hip. No patients complained of paresthesias or muscle weakness in the pelvis or lower extremities.
Location(s) and laterality of pain associated with sacral stress fractures
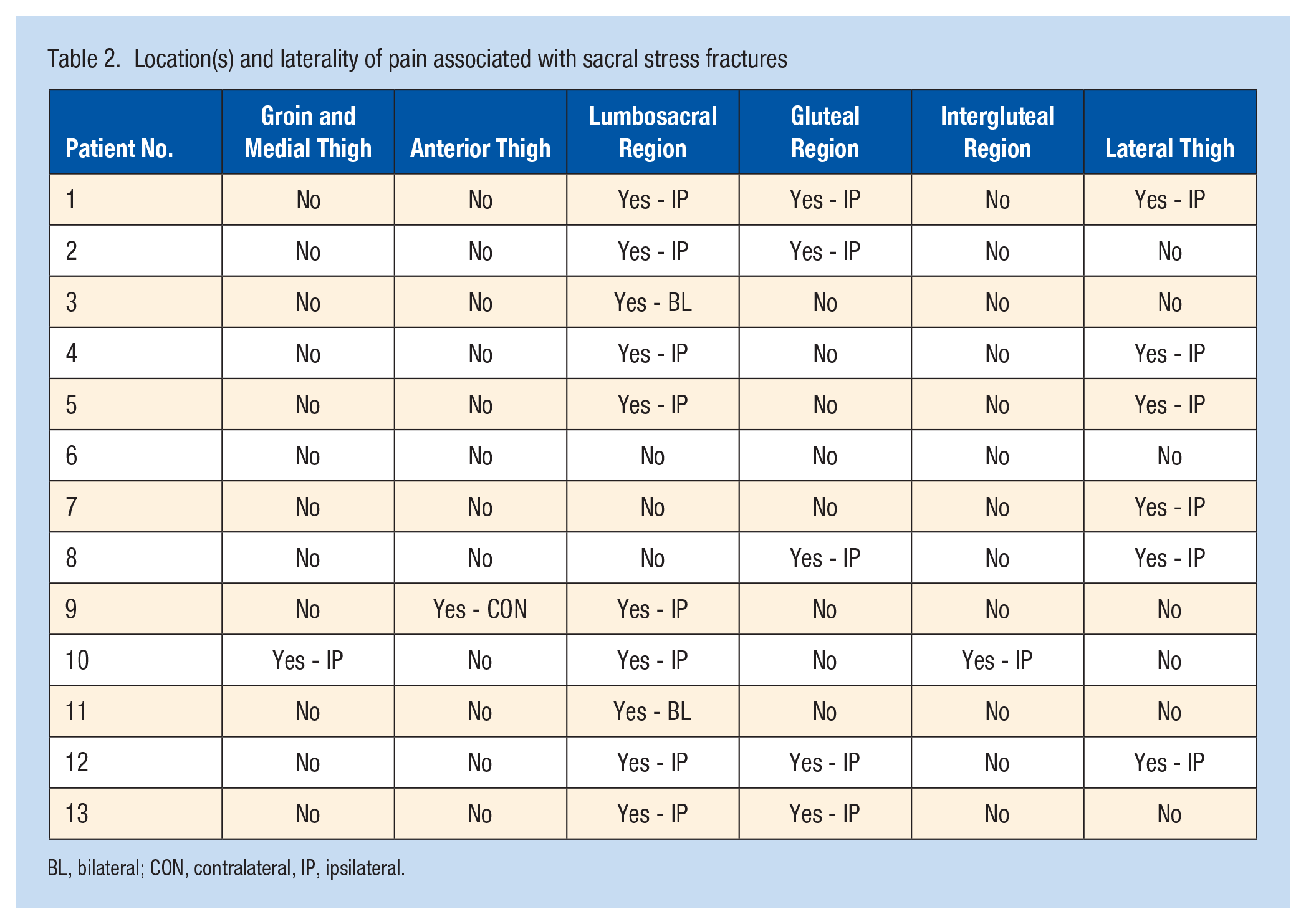
BL, bilateral; CON, contralateral, IP, ipsilateral.
With regard to the onset of pain, most patients described a sudden onset (10 of 13, 76.9%). All patients associated the onset of pain, whether sudden or gradual, with a physical activity they were doing at the time; the most common activity reported was running (9 of 13, 69.2%) followed by skiing (1 patient), horseback riding (1 patient), soccer (1 patient), and high-impact exercise (1 patient). All patients reported that their pain was provoked by walking or running, and most also reported pain with sitting (8 of 13, 61.5%) and standing (11 of 13, 84.6%). Most patients reported having constant pain (10 of 13, 76.9%). The 3 patients who reported having intermittent pain indicated that they experienced pain at least once per day and that the pain was triggered by running, single-leg standing, or strenuous activities. Most patients were unable to describe any modalities or activities that relieved their pain (8 of 13, 61.5%). The remaining 5 patients reported palliating factors such as exercise avoidance (3 patients), running on a water treadmill (1 patient), and applying ice and heat to the affected area (1 patient). Average VAS before treatment was 7.2 out of 10 (range, 1-10).
All but 1 patient (No. 2) presented to a clinic within 1 month of experiencing symptoms. Four patients (30.8%) received misdiagnoses, of whom 3 were able to recall the specific diagnoses they received: “sciatic nerve irritation, sacroiliac joint dysfunction, and/or gluteal amnesia,” “muscle pull or strain,” and “joint misalignment.” All but 2 patients (Nos. 1 and 2) underwent medical treatment within 1 month of experiencing symptoms. The most common medications used were over-the-counter pain medications (11 of 13, 84.6%) such as ibuprofen and acetaminophen, followed by vitamin D supplements (8 of 13, 61.5%) and calcium supplements (5 of 13, 38.5%). Less commonly used medications included codeine-acetaminophen (1 patient), oral diclofenac (1 patient), muscle relaxants (1 patient), arnica herbal supplement (1 patient), and topical menthol gel (1 patient). Patients also reported using nonpharmacological therapies, most commonly rest (12 of 13, 92.3%), physical therapy (7 of 13, 53.8%), and light physical activity involving no impact or low impact (5 of 13, 38.5%). No patients underwent operative treatment but 1 patient (No. 11) reported pursuing several nonoperative treatments including laser therapy, chiropractics, electrical stimulation, dry needling, and ultrasound.
All but 1 patient (No. 13, who had only 1 month of follow-up) have completed medical treatment for their fracture. The average length of treatment was 3.8 months (range, 0-8 months). Most patients experienced symptom resolution at the conclusion of their treatment (9 of 12, 75.0%). Of the 3 patients who completed treatment but were still experiencing symptoms, 2 (Nos. 1 and 5) reported that their symptoms had improved since starting treatment while 1 (No. 11 with 78 months of follow-up) reported that their symptoms had remained the same. All 3 reported that their pain is intermittent and had pre- to posttreatment reduction in VAS pain scores (No. 1: 10-2, No. 5: 4-1, No. 11: 9-1).
Sports Performance
All patients reported participating in at least 1 type of sport, exercise, or physical activity before injury. A majority of patients listed running or a running sport as their primary activity (10 of 13, 76.9%). Other activities listed were cycling (2 patients), weightlifting (2 patients), tennis (1 patient), high-impact interval training (1 patient), skiing (1 patient), aerobics (1 patient), and swimming (1 patient). After injury but before treatment, only 3 patients (23.1%) were able to continue participating in their usual sports and physical activities; these 3 patients (Nos. 5, 11, 12) reported that they were able to continue their activities only at a lower level of intensity than their preinjury baseline and they all experienced pain during activity. The 10 patients who were unable to participate in their usual sport postinjury did not participate in any alternative sports or activities. Of the 12 patients who completed medical treatment, 10 (83.3%) were able to return to their usual sport or activity. Average time to return to sport was 5.9 months (range, 2-12 months). The 2 patients who did not return to sport (Nos. 3 and 5) cited newly diagnosed osteoporosis and chronic pain, respectively, as their reasons.
Running times for the 10 patients who participated in running or running sports before injury are reported in Table 3. Note that there are considerable differences in reported average mile times between patients according to whether the times were reported as an average during a long-distance run or reported as an isolated 1 mile run. Most patients reported a decrease in distance run per week (9 of 10, 90.0%) and longest distance run (10 of 10, 100.0%) after their injury. Among the 9 patients who completed medical treatment, only 3 (33.3%) reached or exceeded their preinjury distance run per week, and only 4 (44.4%) reached or exceeded their preinjury longest distance run. Of the 9 patients, 6 (66.7%) achieved the same or shorter average mile time after medical treatment compared with their preinjury baseline.
Running times and associated metrics for patients in running sports
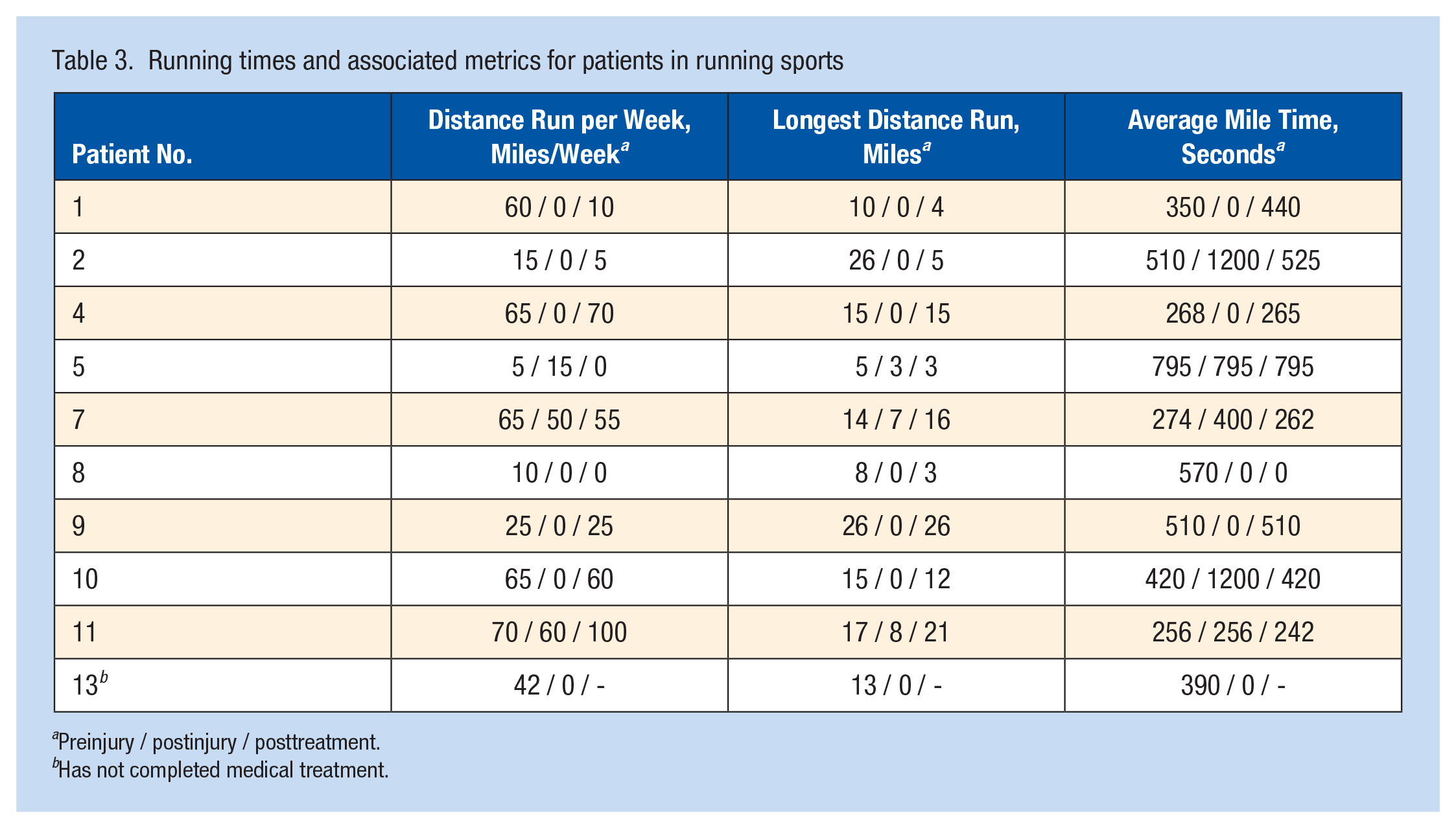
Preinjury / postinjury / posttreatment.
Has not completed medical treatment.
Of the 10 patients who participated in running or running sports, 9 (90.0%) competed in races before injury. After injury, only 1 patient (No. 11) was able to continue participating in races but he reported that his performance was worse. Of the 8 racers that completed treatment, 6 (75.0%) were able to resume competition and 5 (62.5%) were able to perform at or above their preinjury baseline.
Risk Factors for Stress Fractures
Three patients (23.1%) reported a previous history of stress fractures. Of the 9 female patients, only 3 (33.3%) were having menstrual cycles at the time of their injury. Eight female patients (88.9%) reported having regular menstrual cycles in the time preceding their injury, with an average menstrual cycle length of 32.3 days (range, 21-60 days). Of the 7 premenopausal females, 5 (71.4%) reported taking OCPs around the time of their injury.
Discussion
In this case series of 13 athletes diagnosed with sacral stress fractures, we noted several commonalities in clinical presentation, treatment modalities used, the impact of fractures on sports performance, and risk factors. Bakker type B3 fractures were the most common type identified on MRI scans and the sacral neuroforamina were frequently involved, although no patients reported neurological deficits. Most patients presented with acute-onset lumbosacral back pain in the setting of running/jogging activities. All patients underwent nonoperative treatment, primarily with rest and over-the-counter pain medications, and a majority reported resolution of pain at an average of 3.8 months after the initial visit. Rates of return to sport after nonoperative treatment were high (83.3%) although most patients continued to exhibit deficits in running performance compared with their preinjury baseline. Most premenopausal females were on OCPs around the time of their fracture, but other risk factors such as a previous history of stress fractures or irregular menses were uncommon among the cohort.
Previous literature has shown that pain associated with sacral stress fractures tends to occur in a diffuse distribution surrounding the sacral spine and at risk patients are those who follow intense training programs, particularly those involving long-distance running.11,15,16,19 Our study is consistent with previous findings as 10 out of 13 patients experienced pain in the lumbosacral region, while another 10 out of 13 were runners who ran an average of 42 miles per week and a minimum of 5 miles per week before injury. The 3 nonrunners participated in other physically demanding sports such as skiing, tennis, and soccer.
Young female patients presenting with sacral stress fractures often possess components of the female athlete triad, which is defined as a combination of nutritional deficiency, irregular menstrual cycles, and low bone mineral density. 6 Vajapey et al 16 published a case series of 3 female patients diagnosed with sacral stress fractures and noted that all 3 had at least element of the female athlete triad, while Klossner et al 8 reported a case of sacral stress fracture in a female distance runner who had both low body weight and amenorrhea. Conversely, 8 of the 9 female patients in our study reported normal menstrual cycles around the time they began experiencing symptoms and none of the female patients were underweight (BMI <18.5 kg/m2). However, we note that 5 of the 7 premenopausal women in our study were taking OCPs at the time of their injury, which may have masked any underlying menstrual irregularities. 5
The MRI-based classification system developed by Bakker et al 2 may serve to guide treatment decisions for patients with sacral stress fractures, particularly when deciding between operative versus nonoperative interventions. Bahadir et al 1 reported a series of 19 patients with fracture patterns spanning several different Bakker types. Among their cohort, all Bakker type A fractures were treated conservatively (3 of 3), most type Bs were treated with either sacroplasty or percutaneous sacroiliac fixation (8 of 11), and all type Cs were treated with lumbosacral fusion (5 of 5). In contrast to the Bahadir et al 1 cohort, all 11 patients in our cohort with Bakker-typeable fractures (2 type As, 8 type Bs, 1 type C) underwent nonoperative management. Furthermore, nonoperative treatment of type B and C fractures was associated with good return-to-sport outcomes, with 5 of the 8 patients with Type B fractures and the 1 patient with a type C fracture all returning to sport after medical treatment. These results provide tentative evidence that nonoperative management of type B and C fractures is a viable treatment option and that the Bakker classification system should not be the sole decision-making tool for determining indications for operative management.
It has been reported that sacral stress fracture patients managed conservatively experience complete recovery within 6 to 12 months, 10 but our series suggests that the typical recovery time may be even shorter. In our study, 9 of 12 patients who had completed medical treatment by the time of survey had experienced pain resolution at an average posttreatment time of 3.8 months. However, we also found that a speedier recovery did not equate to a return to the preinjury level of sports performance. Among the running athletes in our cohort, most reported decreased mileage after treatment as compared with before their injury, though most were able to achieve the same or faster average mile times after treatment. While these changes in running performance may be a result of deconditioning during the months-long recovery process, they may also reflect a conscious decision on the athlete’s part to scale back their running activities to avoid future stress injuries. In any case, most (6 of 9) of the competitive runners in our series returned to competition after completing treatment. Our positive return-to-sport outcomes are echoed by 3 previous case reports that found that runners with sacral stress fractures were able to return to competition after completing their rehabilitation programs, despite any residual deficits in running performance.7,8,12
Limitations
We note several limitations of this study. First, as this is a retrospective study with significant variation in follow-up time, patient responses to our survey may have been affected by recall bias. Patients self-reported their own clinical presentation, treatment course, sports performance, and menstrual history, and this information could be subject to additions, omissions, or changes depending on the accuracy of the patient’s recollection. Second, our study features a small sample size and this may limit the generalizability of our results to the broader population of sacral stress fracture patients. Third, this study was unable to distinguish between fatigue and insufficiency fractures among our patient sample. However, we note that this would be possible only with the use of bone density data obtained via dual-energy x-ray absorptiometry or bone densitometry, but these procedures are generally not indicated in patients <65 years of age, and especially not in women of reproductive age. 9
Clinical Recommendation
Sacral stress fractures most commonly present as acute lumbosacral back pain provoked in the setting of running sports and frequently involve the sacral neuroforamina. While the pain associated with these fractures prevents most athletes from participating in sports activities, nonoperative management appears to be an effective treatment modality with a high rate of return to sport.