
Abstract
Context:
Physical activity (PA) interventions improve well-being and positive mental health in children and adolescents, but the results of previous systematic reviews included participants with chronic medical conditions and did not accurately assess the multidimensional nature of health-related quality of life (HRQoL).
Objective:
The aims of this meta-analysis were to (1) evaluate the effects of PA interventions on several domains of HRQoL in healthy <18-year-olds and (2) examine the effectiveness of interventions on HRQoL according to whether they were successful in increasing PA, the type of intervention delivered, and the duration of the intervention.
Data Sources:
PubMed (Medline), EMBASE, the Cochrane Library, SCIELO, SPORTDiscus, and PEDro databases were systematically searched from inception to September 30, 2022.
Study Selection:
Experimental studies that examined the effectiveness of PA interventions on HRQoL participants aged <18 years.
Study Design:
Systematic review with meta-analysis and meta-regression.
Level of Evidence:
Level 1.
Methods:
Random-effects models were used to calculate pooled effect size (ES) for total HRQoL score and its dimensions. Subgroup analyses were conducted to examine the effect of PA program characteristics.
Results:
A total of 17 studies were included. Pooled ES (95% CI) estimations were as follows: 0.179 (0.045, 0.002) for total HRQoL score, 0.192 (0.077, 0.306) for physical well-being, 0.158 (0.080, 0.237) for psychological well-being, 0.118 (0.044, 0.192) for autonomy and parent relation, 0.135 (0.043, 0.227) for social support and peers, and 0.129 (-0.013, 0.270) for school environment. Subgroup analyses suggested there were no differences in the effectiveness of the interventions by category of PA increase or by type and duration of intervention.
Conclusion:
Exercise interventions are an effective strategy for improving overall HRQoL and its most significant domains in children and adolescents.
Keywords
Quality of life (QoL) is the combination of objectively and subjectively indicated well-being in multiple domains of life considered salient in one’s culture and time, while adhering to universal standards of human rights. 39 QoL is a broad and hierarchically structured construct composed of several domains. One of the most representative domains is health-related QoL (HRQoL). HRQoL refers to the physical, psychological, and social domains of health, seen as distinct areas that are influenced by a person’s experiences, beliefs, expectations, and perceptions. 37 In children and adolescents, these domains are different from those in adults. Children and adolescents are embedded within multiple social contexts, including the family, their peer group, the classroom, and the community. Each of these contexts is likely to contribute to HRQoL. 28
In healthy children and adolescents, HRQoL measures may serve as a framework to identify and develop preventive medicine strategies and health promotion. 16 However, despite its widely accepted importance, findings have suggested that HRQoL has significantly declined in children and adolescents. 10 One of the factors to improve HRQoL in childhood and adolescence could be ensuring an adequate level of physical activity (PA), which may positively influence HRQoL through biological, psychological, and social mechanisms.11,21
Thus, several systematic reviews suggest a direct association between PA and HRQoL in children and adolescents, but these reviews included participants with chronic conditions 26 , or the results came exclusively from observational studies and did not allow cause-effect relationships between engaging in PA and better HRQoL to be established. 40 Moreover, a recent umbrella review, whose objective was to examine the relationship between PA, HRQoL, and well-being in a general population across lifespan and in persons with psychiatric and neurologic conditions, concluded that the evidence in youth is limited, mainly because of an insufficient number of studies and the low quality of studies included in the reviews. 27 Furthermore, previous systematic reviews and meta-analyses in children and adolescents have suggested that PA interventions improve self-esteem, self-concept, 24 well-being, 11 or positive mental health, 3 concepts closely related but different from the multidimensional HRQoL construct.
To the best of our knowledge, no meta-analytic approach has provided a comprehensive synthesis of the effectiveness of PA interventions on HRQoL for children and adolescents, distinguishing between whether or not they increased the amount of PA, whether or not they consisted of only PA or were multicomponent, and analyzing the effectiveness by duration of the intervention. Therefore, the aims of this systematic review and meta-analysis were to (1) evaluate the effects of PA interventions on several HRQoL domains in healthy subjects aged <18 years and (2) examine the effectiveness of interventions on HRQoL, according to whether they were successful in increasing PA, the type of intervention delivered (PA-only or multicomponent), and the duration of the intervention.
Methods
Protocol and Registration
This meta-analysis was performed according to the PRISMA (Preferred Reporting Items for Systematic Reviews and Meta-Analysis) statement and the Cochrane Collaboration Handbook.18,32 The protocol was registered on PROSPERO (registration number: CRD42015025823) and published elsewhere. 6
Information Sources and Search Strategy
The following electronic bibliographic databases were searched by 2 reviewers to identify relevant studies from their inception to September 30, 2022: Medline (via PubMed), EMBASE, the Cochrane Library, SCIELO, SPORTDiscus, and PEDro. The search strategy was applied to all the titles, abstracts, and keywords of the studies and combined the following keywords: “physical activity” OR “exercise” OR “sport.” These terms were combined with “health-related quality of life” OR “HRQoL” OR “quality of life” OR “well-being” OR “positive health” OR “psychological health” OR “mental health” and with “children” OR “adolescent” OR “young children” OR “schoolboy” OR “schoolgirl” OR “school children.” In addition, the terms “physical activity intervention” and “school-based intervention” were added to the search (Online Appendix Table A1). References were imported into Endnote (Thompson Reuters). Reference lists of relevant studies and previous systematic reviews and meta-analysis were also identified to review the list of included studies.
Eligibility Criteria and Study Selection
We selected studies that examined the effectiveness of PA interventions on HRQoL. The criteria for study inclusion were (1) children (<12 years) and adolescents (≥12-18 years) without diagnosis of any pathology (ie, general population, including samples of children with overweight/obesity); (2) planned and structured PA interventions in and out of school, where the main aim was to increase PA; (3) experimental studies (randomized controlled trials [RCTs] and non-RCTs) in which the control group (CG) received no structured type of physical exercise intervention (ie, usual daily activities or regular school curriculum); (4) an assessment of the multidimensional construct of HRQoL (self-reported and parent reported) using valid questionnaires; and (5) providing enough information to calculate effect sizes (ESs). We used the following exclusion criteria: (1) observational studies (including cross-sectional and longitudinal observational studies); (2) studies including adults and studies targeting clinical populations of children and adolescents (eg, obesity, cancer, asthma, etc); (3) studies describing interventions not including a well-defined structured PA intervention (at least duration, frequency, and type), or exclusively educational healthy lifestyle interventions; and (4) studies that reported only specific domains of HRQoL (eg, psychosocial, physical, well-being, emotional). Also excluded were studies not providing an adequate CG for comparison.
No date limits were imposed on the search, and studies were limited to those published in English or Spanish. Two authors independently screened the title, abstracts, and keywords of studies identified by the search strategy. Discrepancies between the 2 reviewers regarding study conditions were resolved by consensus with a third author.
Data Collection Process
Two reviewers extracted the following data from each included study: author, year of publication, country of study, study design, number of participants, intervention and CG size, characteristics of the PA intervention (duration, frequency, and type), details of additional intervention (eg, sleep, nutrition, instruction or parental involvement), and HRQoL questionnaire used. A third author arbitrated unresolved disagreements regarding data extraction.
Risk of Bias in Individual Studies
Two authors independently assessed the risk of bias for each of the included studies in accordance with the Cochrane Collaboration tool for assessing risk of bias (RoB2). 36 This tool evaluates 5 specific domains: randomization process, deviations from intended interventions, missing outcome data, measurement of the outcome, and selection of the reported result. Each list item was classified as “+” (low risk of bias), “-“ (high risk of bias), and “?” (some concerns), based on criteria for judging the risk of bias. In addition, the tool calculates an overall risk of bias value.
Data Synthesis and Statistical Analysis
The ES (Cohen d) of each study was calculated as the standardized mean difference in each HRQoL dimension. We calculated the ES of the parameters from preintervention to postintervention between groups (exercise intervention vs control) in each study and pooled these using the random-effects model (DerSimonian-Laird approach), 30 assuming a correlation coefficient of 0.5. When studies used different follow-up periods, we synthesized outcomes collected at the reported closest postintervention endpoint. In the studies with a crossover design, we included data from only the first period of the trial. When studies met the inclusion criteria but did not report the necessary data for meta-analysis, we emailed the corresponding author requesting the data. Finally, the ESs of all the studies included were combined to estimate an overall summary ES, with a 95% CI and a random-effects model, which was calculated using STATA Version 14 (StataCorp) software.
The percentage of total variation across the studies due to heterogeneity (Cochran’s Q-statistic) was used to calculate the I2 statistic, 20 considering the following thresholds: not important (0%-30%), moderate (30%-50%), substantial (50%-75%), and considerable (75%-100%) inconsistency 19 ; P values were also considered.
Subgroup analyses were performed comparing the interventions that were effective in increasing PA versus those that were not, and between the subtype of PA intervention (PA alone vs PA combined with other strategies, such as instructions to promote a healthy lifestyle) to observe which had the highest ES. In addition, random-effects meta-regression analyses were performed to determine whether the length of interventions could be related to the effectiveness of the intervention to improve HRQoL.
We conducted a sensitivity analysis to assess the influence of each study on the overall ES. Each study was removed in turn from the model, and we then recalculated the pooled analysis conducted. A funnel plot and Egger test were used to test publication bias.
Results
Study Selection
The search strategy identified 1547 potential studies. After removing 742 duplicates, 760 references were excluded based on the title and abstracts. We selected 45 studies for a more detailed evaluation of the full text. Finally, a total of 17 studies1,4,5,7,8,9,12,13,14,17,22,23,29,31,33,35,38 met the inclusion criteria (Figure 1).
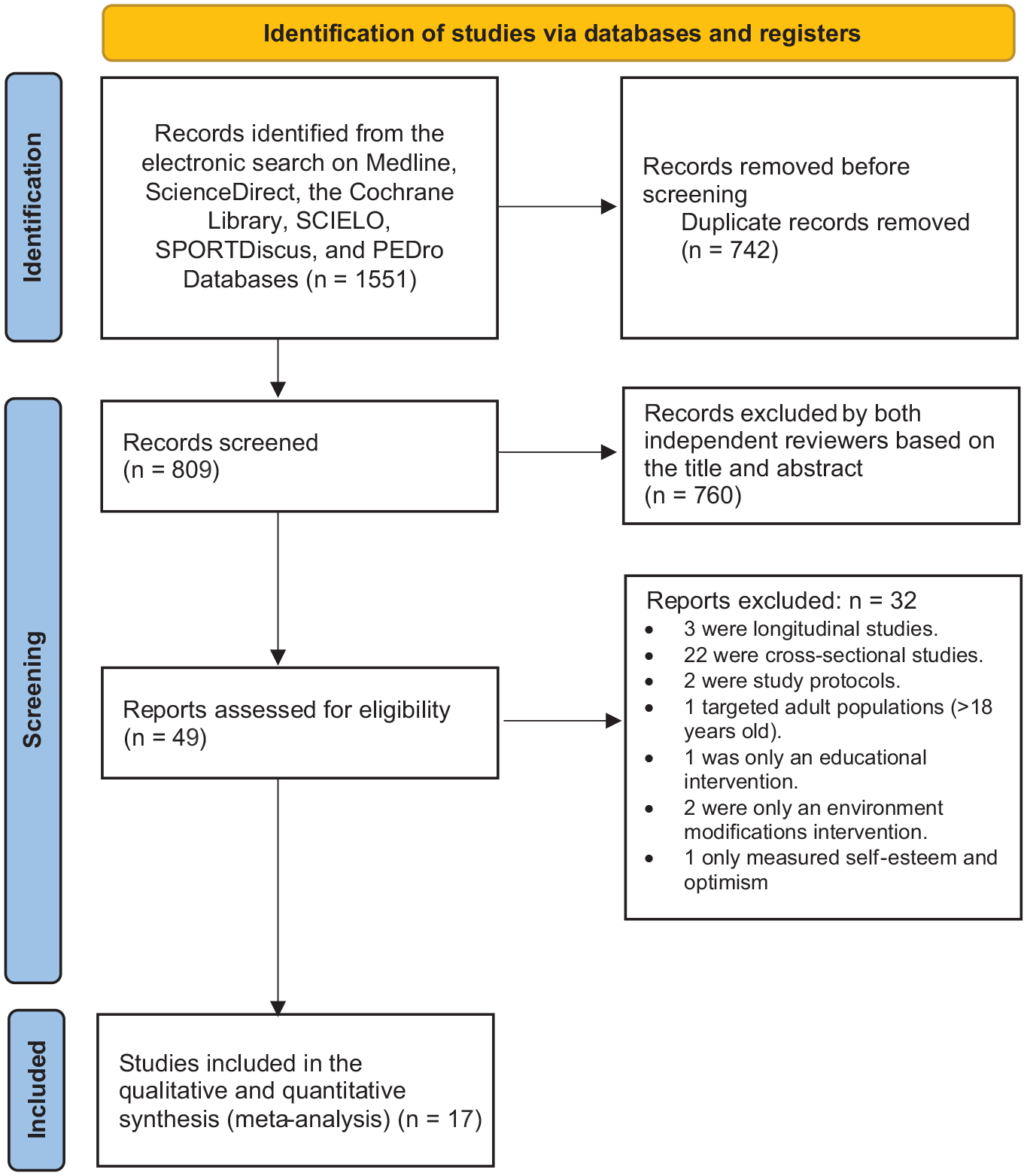
PRISMA flow diagram with the progress through the stages of study selection. PRISMA, Preferred Reporting Items for Systematic Reviews and Meta-Analysis.
Study Characteristics
Online Appendix 2 summarizes the study characteristics. The studies were published between 2010 and 2020 and were conducted in 10 countries (Ireland, England/United Kingdom, Sweden, Australia, Singapore, South Africa, Hong Kong, Switzerland, Norway, and Canada). Of the 17 studies, 15 were RCTs,1,7-9,12-14,17,22,23,29,31,33,35,38 and 2 were quasi-experimental.4,5 The total sample included 11,980 children and adolescents (6303 in the intervention group) aged 2.5 to 14 years. One study included only girls. 9 Two studies involved first and fifth grade students,7,29 but only 1 study separately showed results by grade. 17
HRQoL measurement instruments varied across studies and included the KIDSCREEN-27,5,8,13,14,23,35, Pediatric Quality of Life Inventory 4.0,1,4,9,12,31,33,38 Child Health Questionnaire,17,22,29 and The Child Health Utility 9D questionnaires. 7 The HRQoL questionnaires were self-administered in 13 studies,1,4,5,7-9,13,14,22,23,29,35,38 and parent-reported in 4 studies.12,17,31,33 PA was assessed using different methods: only with accelerometers,1,5,8,14,17,22,23,29,31,35 with accelerometers and parent-reported children’s habitual PA,33,38 with pedometers and pulsometers, 12 with a Likert-type scale for PA levels plus self-reported PA questionnaire, 9 and with a single-item question taken from the Health-Behavior of School-Aged Children survey. 3
The interventions were intended to improve the amount of PA using the following strategies: (1) adding extra physical education (PE) lessons1,8,13,17,22,23,29,33,35,38 to the regular school curriculum; (2) with extra PA, offering sport or dance activities,4,13,31 motor skills training, 31 short active breaks,13,17,22,23,29,35 breaks for walk or run, 7 or PA during recess 14 ; (3) with after-school PA programs, either through outdoor activities, 12 daily step targets, 12 or PA homework17,22,23,29,35; (4) making environmental adaptations to encourage PA practice5,13,14,17,33,38; (5) restructuring preschoolers’ outdoor playtime into shorter, more frequent periods of time 38 ; and (6) substituting the usual PE classes for sports and recreational sessions with an alternative teaching methodology. 9 In addition, 4 studies also included healthy lifestyle recommendations for participants (PA, nutrition, sleep, use of electronic media),1,8,14,33 and 1 study addressed barriers to PA participation. 9 In addition, in 5 studies, parents were trained in the benefits of PA and were involved in the development of the intervention.1,4,12,31,33 The interventions provided an increase in PA time from 57 to 325 minutes per week. Two studies offered free access to resources to promote PA, through dance mats 5 or ropes and activity zones. 14 One study set a goal of steps and a minimum of 2, 60-to-90-minute, outdoor activity sessions per month. 12 The frequency of the interventions was predominantly twice a week4,17,22,23,29 or 5 days a week.1,7,13,31,38 Other programs were implemented every day of the week,5,12,14 4 days a week, 33 and 1 day a week.8,9 One study did not specify the frequency of the intervention. 35 None of the included studies reported information on the intensity of the PA programs. The length of interventions ranged from 2 to 12 months.5,9,38 Of the 12 studies, 6 included implemented 9-month interventions, corresponding to 1 academic year.12,17,22,23,29,33 Four studies conducted long-term follow-up,1,8,29,38 ranging from 3 months to 3 years postintervention.1,29 The CG engaged in their regular PE lessons for all interventions.5,7 -9,12,13,17,22,23,29,31,33,35,38 In 1 study, 14 the CG had free access to ropes during school recess. Finally, 2 studies did not provide information on the PA performed by the CG.1,4
Of the 17 studies included in the meta-analysis, 7 studies1,5,8,9,13,14,35 reported that the interventions did not increase participants’ PA levels, and in 5 studies PA levels increased significantly in the experimental group from baseline levels,12,22,29,33,38 observing variations across studies: significant increase in PA measured by step target, 12 increases in moderate-to-vigorous PA (MVPA) and total PA, 22 increased levels of self-reported PA but not total PA measured by accelerometer, 33 and increased levels of total PA and MVPA but not light PA. 38 Five studies did not report postintervention PA values.4,7,17,23,3
Risk of Bias in Individual Studies
The risk of bias score for the included studies is reported in Figure 2. A total of 15 studies reported a process of randomization.1,7 -9,12 -14,17,22,23,29,31,33,35,38 In 2 studies,4,5 there was no randomization. Three studies were at high risk of bias due to deviations from intended interventions,4,7,8 4 studies in missing outcome data,5,7,9,29 4 studies in selection of the reported results,1,7,22,29 and 6 studies had high overall bias.4,5,7,22,29,31
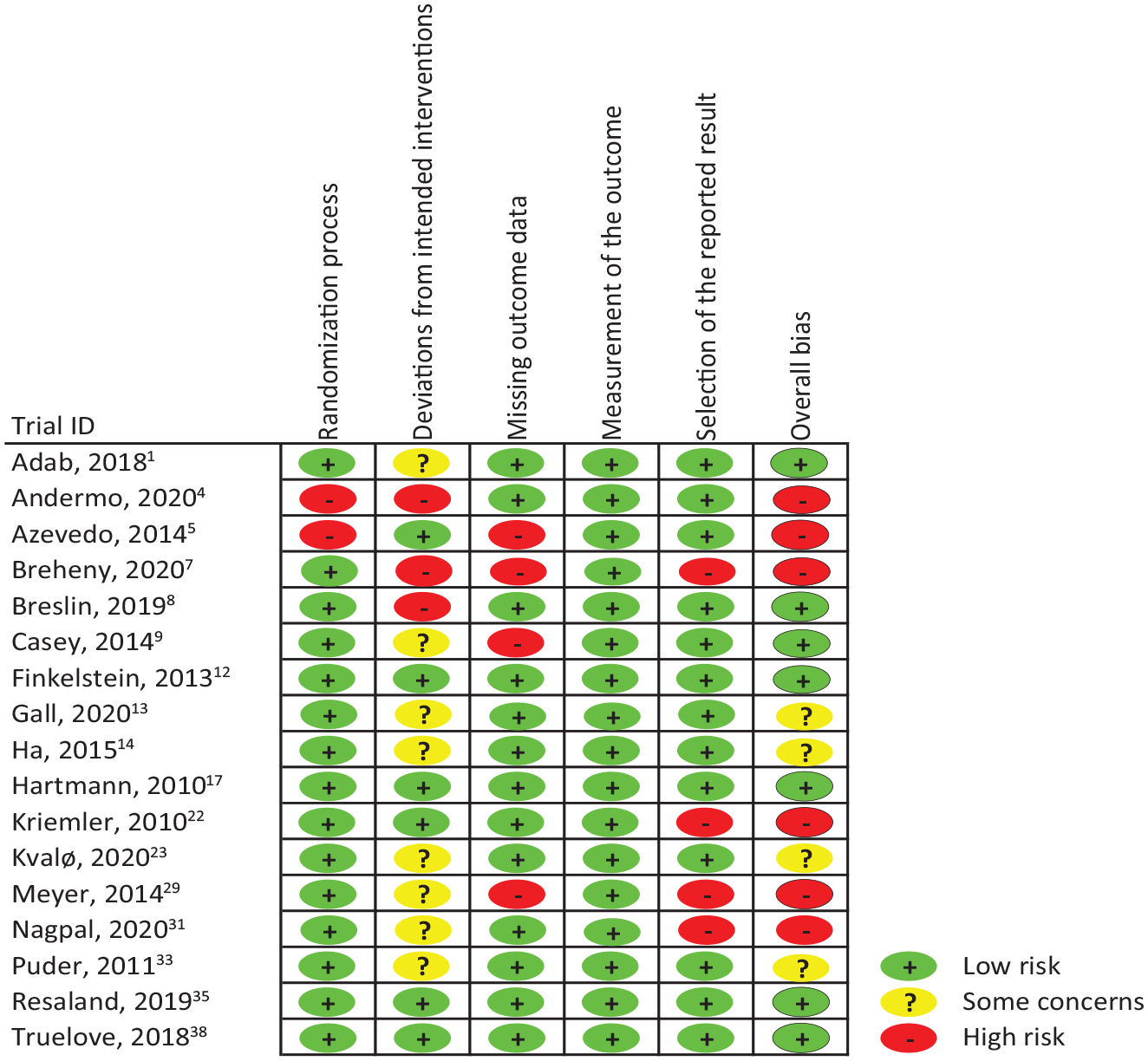
Risk of bias assessment for all included studies.
Summary of Evidence
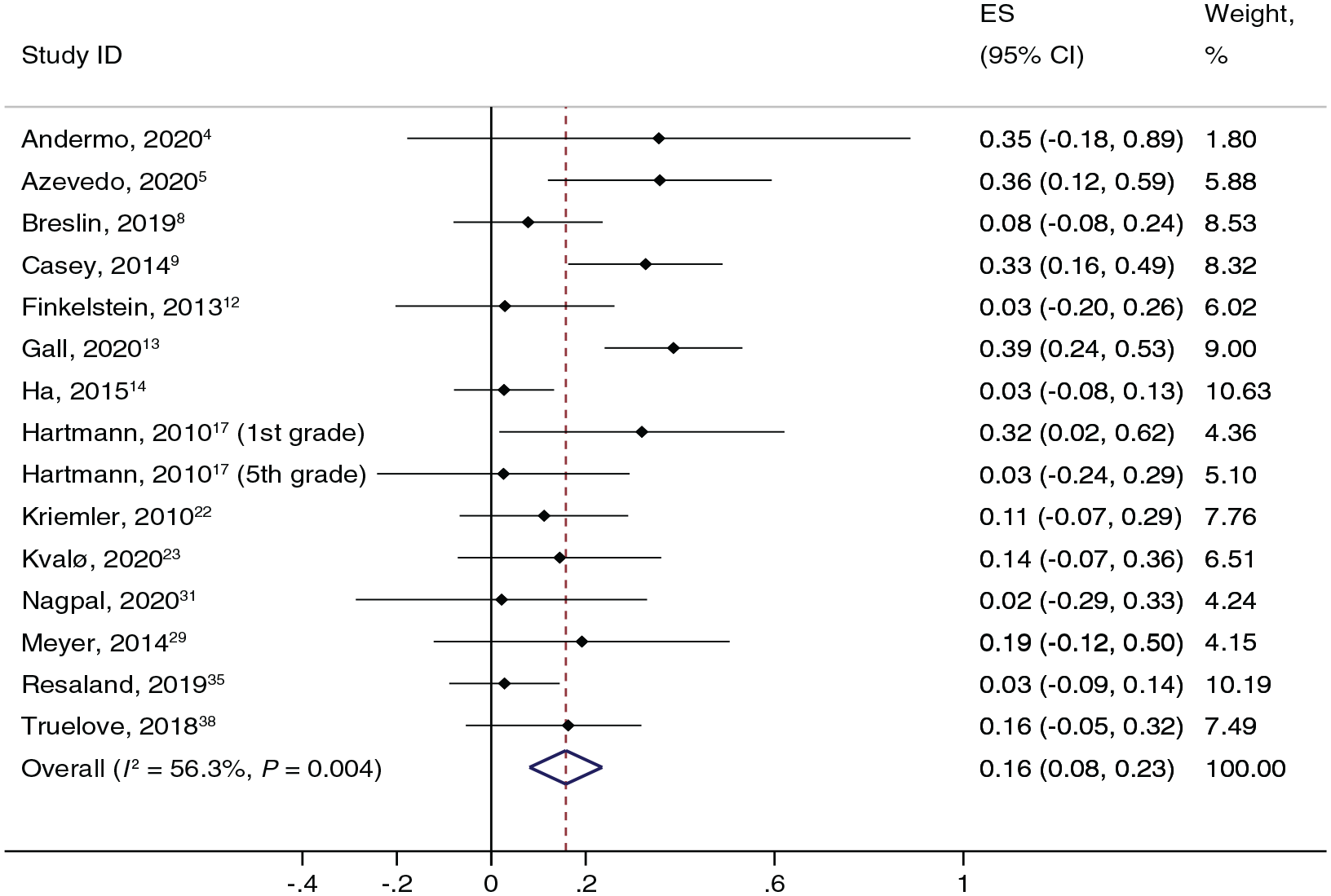
The results of the meta-analysis showed that the pooled ES (95% CI) estimates for the effect of PA on HRQoL were as follows: 0.179 (0.045, 0.002) for total HRQoL score (Figure 3), 0.192 (0.077, 0.306) for physical well-being (Figure 4), 0.158 (0.080, 0.237) for psychological well-being (Figure 5), 0.118 (0.044, 0.192) for autonomy and parent relation, 0.135 (0.043, 0.227) for social support and peers, and 0.129 (-0.013, 0.270) for school environment (Figure 6). Inconsistency among studies was moderate for autonomy and parent relation (I2 = 31.05%) and for total HRQoL score (I2 = 48.42%); substantial for social support and peers (I2 = 54.92%) and for psychological well-being (I2 = 56.31%); and considerable for physical well-being (I2 = 80.18%) and for school environment (I2 = 80.99%).
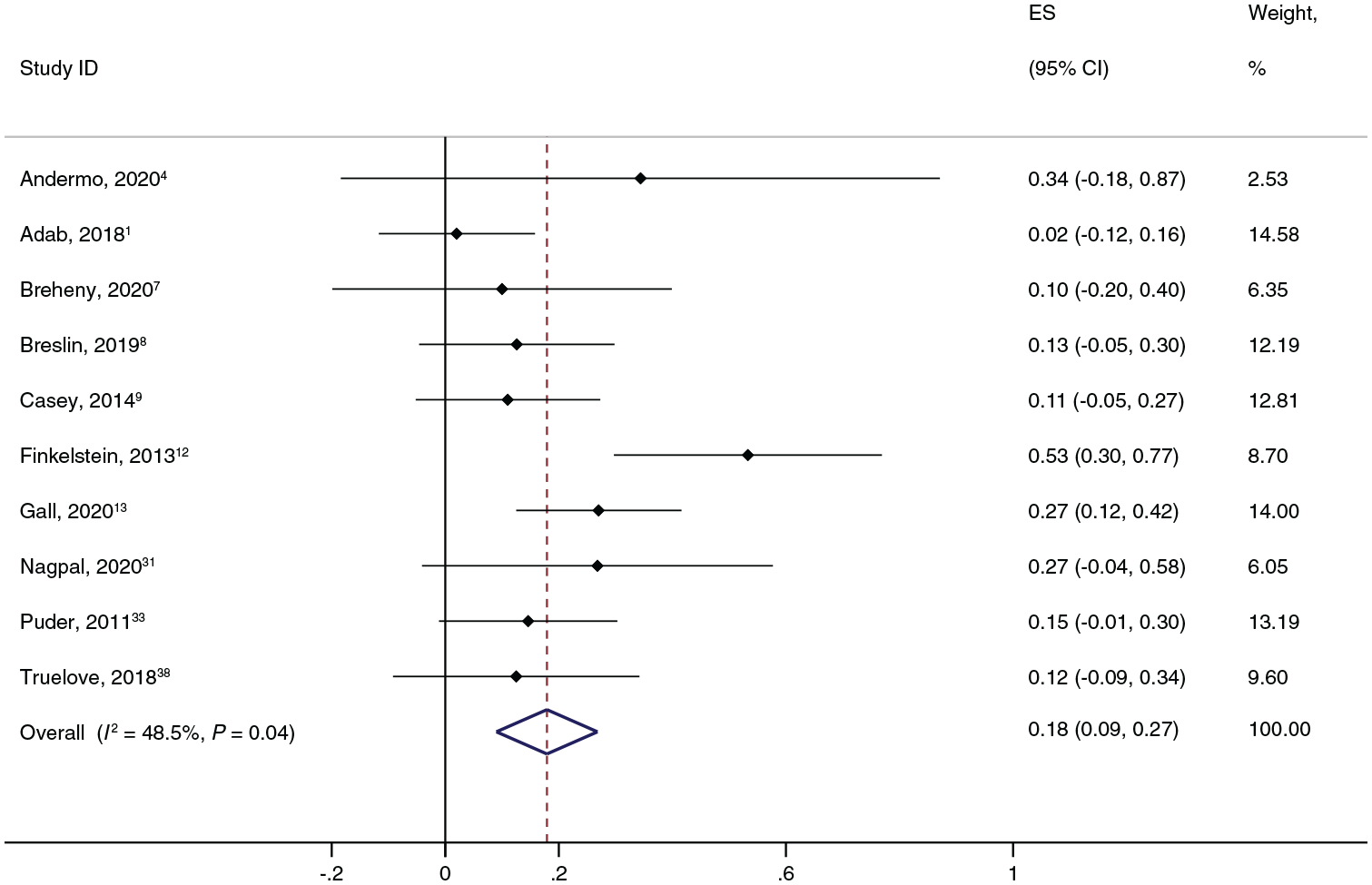
Pooled estimated effect size (ES) values of associations between PA and total HRQoL score. HRQoL, health-related quality of life; PA, physical activity.
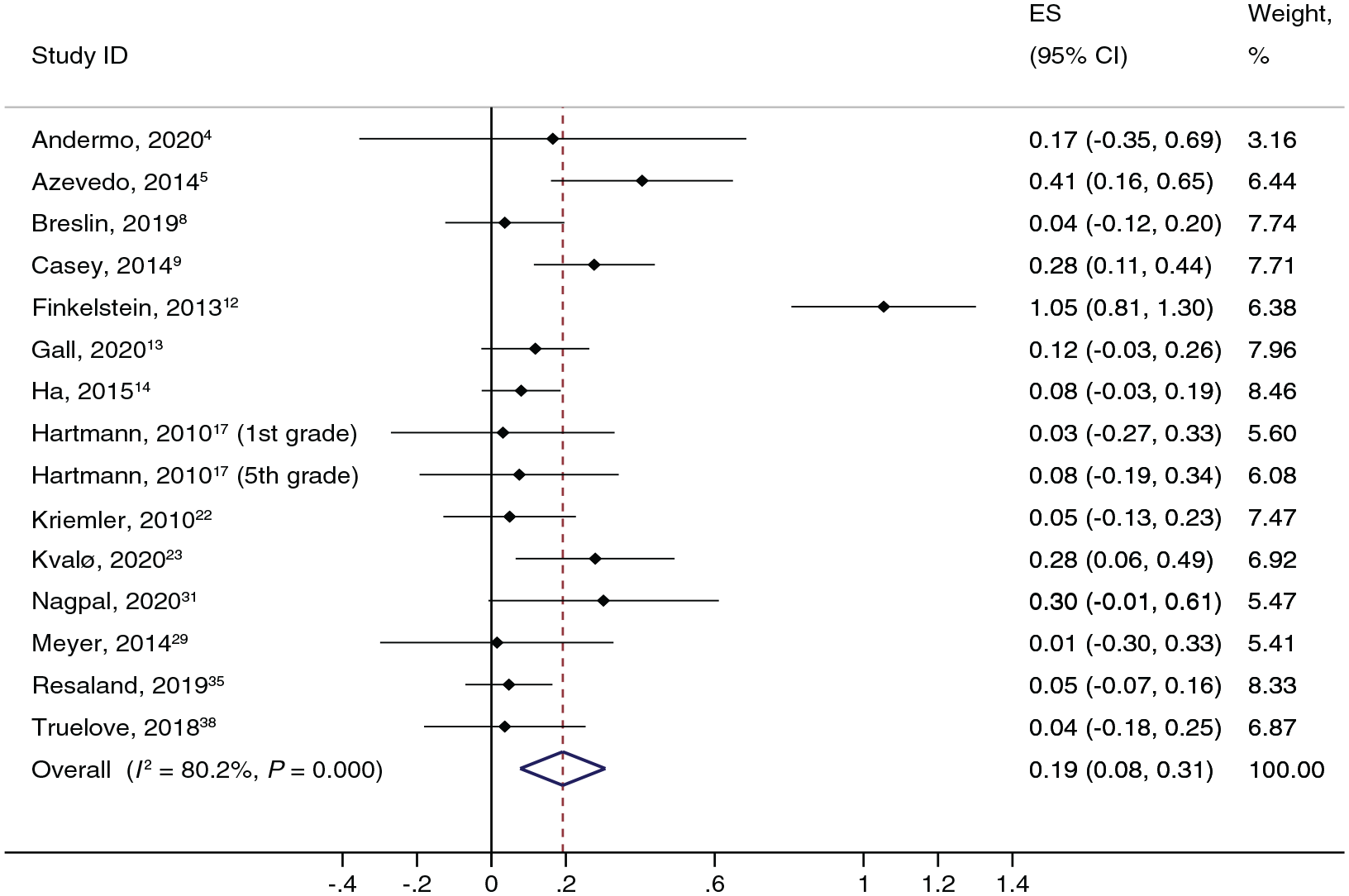
Pooled estimated effect size (ES) values of associations between PA and physical well-being. PA, physical activity.
Pooled effect size (ES) values of associations between PA and psychological well-being. PA, physical activity.
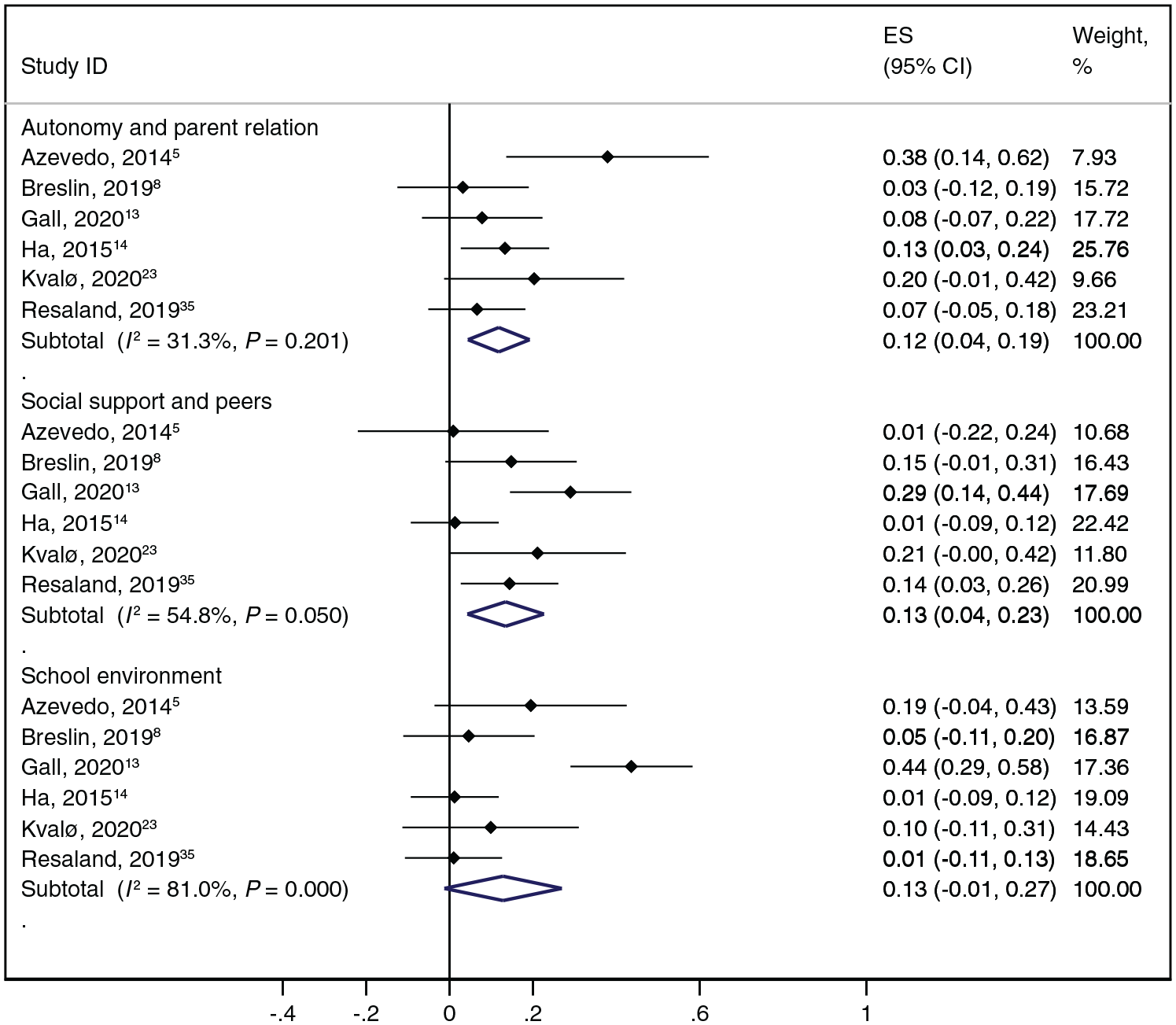
Pooled estimated effect size (ES) values of associations between PA, autonomy and parent relation, social support and peers, and school environment. PA, physical activity.
Subgroup analysis revealed no differences in the effectiveness of the interventions by category of PA increase (Online Appendix Table A2) or by type of intervention (PA alone or PA combined with other strategies) (Online Appendix Table A3). The random-effects meta-regression model showed no association between the effect of PA interventions and the length of intervention (Online Appendix Table A4).
Sensitivity analyses suggested that the pooled ES estimates for total HRQoL score, physical well-being, psychological well-being, autonomy and parent relation, social support and peers, and school environment did not change when studies were removed one by one (Online Appendix Table A5).
Funnel plot asymmetry and Egger tests show no significant publication bias for any of the outcome variables (Online Appendix Table A6).
Discussion
To the best of our knowledge, this is the first meta-analysis of the effects of PA interventions on HRQoL in healthy children and adolescents. The main finding of this systematic review and meta-analysis is that physical exercise improves overall HRQoL and several HRQoL domains, such as physical well-being, psychological well-being, autonomy and parent relation, and social support and peers. However, our findings show no positive effect of the exercise programs on the school environment domain. Furthermore, given the limited number of studies and the large heterogeneity of the interventions, the results of this review do not allow us to state whether the benefits of PA interventions on HRQoL depend on whether they manage to increase the amount of PA. Similarly, it was not possible to conclude whether the type of intervention and the duration of the programs have an influence on the benefits in HRQoL of PA interventions aimed at children and adolescents.
Overall, our results are in line with those reported in children and adolescents in previous reviews. In this regard, Wu et al 40 and Marquez et al 27 reported that most observational studies included in their reviews concluded that higher levels of PA were associated with better HRQoL in children and adolescents. Regarding the effectiveness of PA interventions in improving different aspects of HRQoL, the available evidence showed mixed results. In line with our findings, earlier reviews and meta-analyses described how PA interventions in the school area yielded improvements in aspects such as well-being or HRQoL.3,26 In contrast, other authors found that school-based interventions had no significant effects on HRQoL or reported unclear results.3,34,15 These reviews included studies with exclusively educational interventions (healthy lifestyle information, marketing material, cognitive behavioral skills building) or exclusively environmental modifications that did not involve an increase in the participants’ habitual PA time, which could explain the differences with respect to our findings.3,34
Different mechanisms have been proposed by which PA could generate improvements in aspects related to cognition, well-being, self-esteem, or mental health. The conceptual model proposed by Lubans et al 25 establishes neurobiological, psychosocial, and behavioral mechanisms to attempt to explain these effects of PA in children and adolescents. At the neurobiological level, changes occur in the structural and functional composition of the brain, such as the growth of new capillaries, which would increase the transport of nutrients to neurons; the release of endorphins, which can relieve pain and produce a feeling of euphoria; and changes in different brain monoamines, which would increase the feeling of well-being. At the psychosocial level, PA provides an opportunity for social interaction, satisfying basic psychological needs for social connection, and positively affecting aspects, such as perceived competence, body image, and independence. At the behavioral level, participation in PA improves sleep duration and efficiency, as well as coping skills, with consequent benefits for physical and psychological well-being.
Although our results do not allow us to draw conclusions about whether interventions that increase PA are more effective in improving HRQoL than those that do not, the findings suggest that both interventions that increase PA and those that do not may have a positive effect on HRQoL in children and adolescents. It could therefore be argued that these improvements do not depend exclusively on the volume of PA but might also be related to social and psychoemotional factors (eg, social interaction, improvement of perceived motor competence and self-efficacy) inherent in the physical exercise programs included in this review. Future research should take this into account in the design of interventions aimed at improving HRQoL in children and adolescents.
Regarding the type of intervention, our data suggest that both PA-only interventions and multicomponent interventions (those including, as well as PA, other behaviors such as those related to diet, sleep, or use of electronic media) may be effective in improving HRQoL in children and adolescents. In the same vein, a recent systematic review suggested that both exclusive and multicomponent PA interventions were effective in improving aspects closely related to HRQoL, such as body image dissatisfaction and self-esteem in children aged 6 to 11 years. 15
Taking into account that the items of the school dimension are related to aspects not intentionally developed in the PA interventions included in this review, such as the children’s relationships with their teachers or how they felt at school, the lack of effectiveness in this dimension does not seem surprising. Furthermore, some studies have related improvements in cognitive aspects to the type of activity performed, arguing that cognitively demanding activities are more effective than simple, repetitive activities. 2 It is therefore likely that this has not been taken into account in the design of the interventions, although this is difficult to know due to the lack of detail on the characteristics of the activities in the programs.
Limitations
The present meta-analysis has several limitations. First, our search strategy was restricted to articles in English and Spanish. Second, few RCTs described in detail the implementation conditions of their interventions, such as the intensity of the PA or details of the process evaluation. Third, due to limited sample sizes and heterogeneity, it was not possible to conduct sensitivity analyses by age and sex. Fourth, although the different domains were assessed with valid and reliable HRQoL scales, some domains might have had the same name but measured different constructs. Fifth, most of the studies were conducted in high-income countries and therefore may not be generalizable to lower-income countries. Two studies included exclusively low socioeconomic populations with mixed results.8,9 Sixth, although an inclusion criterion of the studies was that the participants were healthy, we cannot be sure of the existence of other undetected physical, mental, or social limitations that might have influenced the relationship between PA level and HRQoL. Finally, we were unable to analyze the effect of confounding variables, mediating variables, or moderators of the effect.
Conclusion
This systematic review and meta-analysis suggests that PA interventions are an effective strategy for improving overall HRQoL, as well as its most significant domains, in children and adolescents, although the magnitude of the effect was small. Considering these findings, initiatives to increase PA should be a priority for policy makers and schools.
Supplemental Material
sj-docx-1-sph-10.1177_19417381231190885 – Supplemental material for Are Physical Activity Interventions Effective in Improving Health-Related Quality of Life in Children and Adolescents? A Systematic Review and Meta-Analysis
Supplemental material, sj-docx-1-sph-10.1177_19417381231190885 for Are Physical Activity Interventions Effective in Improving Health-Related Quality of Life in Children and Adolescents? A Systematic Review and Meta-Analysis by Alberto Bermejo-Cantarero, Mairena Sánchez-López, Celia Álvarez-Bueno, Andres Redondo-Tébar, Antonio García-Hermoso and Vicente Martínez-Vizcaino in Sports Health
Supplemental Material
sj-pdf-1-sph-10.1177_19417381231190885 – Supplemental material for Are Physical Activity Interventions Effective in Improving Health-Related Quality of Life in Children and Adolescents? A Systematic Review and Meta-Analysis
Supplemental material, sj-pdf-1-sph-10.1177_19417381231190885 for Are Physical Activity Interventions Effective in Improving Health-Related Quality of Life in Children and Adolescents? A Systematic Review and Meta-Analysis by Alberto Bermejo-Cantarero, Mairena Sánchez-López, Celia Álvarez-Bueno, Andres Redondo-Tébar, Antonio García-Hermoso and Vicente Martínez-Vizcaino in Sports Health
Footnotes
Acknowledgements
The authors would like to thank the researchers from the Health and Social Research Center for their support during the preparation of this systematic review and meta-analysis.
The authors report no potential conflicts of interest in the development and publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.