
Abstract
Background:
Delayed-onset muscle soreness (DOMS) has been widely examined in the peripheral muscles; however, studies showing the potential effects of DOMS on respiratory function are limited.
Hypothesis:
DOMS in trunk muscles has a negative effect on respiratory function parameters, respiratory muscle strength, respiratory muscle endurance, and exercise capacity.
Study Design:
Prospective cohort study.
Level of Evidence:
Level 2.
Methods:
In 24 healthy participants with a mean age of 21 ± 2 years, DOMS was induced for the trunk muscles with a load equal to 80% of the maximum repetitive voluntary contraction. Pulmonary function parameters, respiratory muscle strength and endurance, exercise capacity, pain, fatigue, and dyspnea perception severity were recorded before DOMS and at 24 and 48 hours after DOMS.
Results:
After DOMS, decreases were observed in respiratory function parameters, namely, forced vital capacity, forced expiratory volume in the first second, vital capacity, and 25% to 75% flow rate value of forced expiratory volume (25% to 75%) (P = 0.02, P = 0.02, P < 0.01, P = 0.01, respectively). Maximal inspiratory pressure and exercise capacity also decreased (P = 0.02, P < 0.01, respectively). No difference was observed between all 3 measurements of maximal expiratory pressure (MEP) and MEP% values (P1 = P2 = P3 ≥ 0.99). The results of the respiratory muscle endurance tests did not reveal a significant difference in terms of load and time in all 3 conditions (P > 0.05).
Conclusion:
After DOMS, there was a 4% to 7.5% decrease in respiratory function parameters, and a 6.6% decrease in respiratory muscle strength.
Clinical Relevance:
The occurrence of DOMS before a competition can have a detrimental impact on pulmonary performance. Hence, it is imperative to consider this factor when devising training and exercise programs. In addition, the development of treatment protocols becomes crucial if DOMS arises.
Respiration is a physiological event that occurs with muscular activity. At rest, inspiration is accomplished by the contraction of the diaphragm, the external intercostal muscles, and the scalene muscles. These muscles are called the primary inspiratory muscles. 1 The sternocleidomastoid, sternohyoid, sternothyroid, serratus anterior, pectoralis major, and serratus posterior superior muscles are accessory respiratory muscles. Since they are forced inspiration muscles, they do not function in “at-rest breathing,” but function especially in physiological and pathological conditions where the tidal volume must be increased.4,10 Expiration has no primary muscles. At the end of an inspiration, the activity of the nerves that stimulate the diaphragm and other inspiratory muscles decreases and these muscles relax. Therefore, expiration is passive. 4 However, to overcome the resistance to air flow, active/forced expiration may be required via the forced expiratory muscles such as rectus abdominis, external and internal oblique muscles, and abdominal wall muscles such as transversus abdominis and internal intercostal muscles. 10
Delayed-onset muscle soreness (DOMS) is a condition characterized by pain and tenderness after unusually excessive exercise, mostly involving eccentric contraction. 19 In DOMS, although pain and tenderness are more prominent in the muscle groups used during activity, functional disorders including decreased range of motion, edema, stiffness, and decreased muscle strength also occur. 15 DOMS increases in skeletal muscles in the first 24 hours after exercise and progresses to a peak after 24 to 48 hours, with symptoms and pain subsiding within 5 to 7 days after exercise. 11
There is a direct relationship between the amount of lactic acid accumulated depending on the intensity of the exercise and the muscle pain felt. 7 However, studies have suggested that delayed muscle soreness after exercise is caused by microtears in muscle fibers or connective tissues. Tears in muscles or connective tissues occur after exercises for unconventional muscle groups or with overload. Microscopic tears seen after exercise cause the fluid in the muscles to pass into the surrounding tissues, as a result of which interstitial edema may occur. 12
Most of the studies examining delayed muscle pain in humans are on the peripheral muscles. 14 Studies showing that cardiac and pulmonary system parameters are affected after delayed muscle pain in various parts of the body are limited. 13 Although there is a study examining the effect of DOMS on respiratory function, DOMS was created in inspiratory muscles directly by airflow in the study. 21 However, considering that the muscles used during forced expiration and inspiration are mostly trunk muscles, delayed muscle pain that may occur in these muscles has the potential to affect the power and efficiency of respiratory function. Considering that core muscle, spine, and spinal stabilization training are performed intensely in almost all sports and physical activity programs, 20 possible loss of function as a result of DOMS of the trunk muscles gains importance. Given that very small variables in performance are major success factors in elite athletes, this can be vital for performance loss in athletes.
The aim of the study was to evaluate how respiratory parameters are affected after DOMS induced in trunk muscles. We hypothesized that DOMS in trunk muscles has a negative effect on respiratory function parameters, respiratory muscle strength, respiratory muscle endurance, and exercise capacity.
Methods
Participants
A total of 24 (n = 11 female, n = 13 male) healthy university students with a mean age of 21 ± 1 years without regular exercise habits were included in the study (Figure 1).
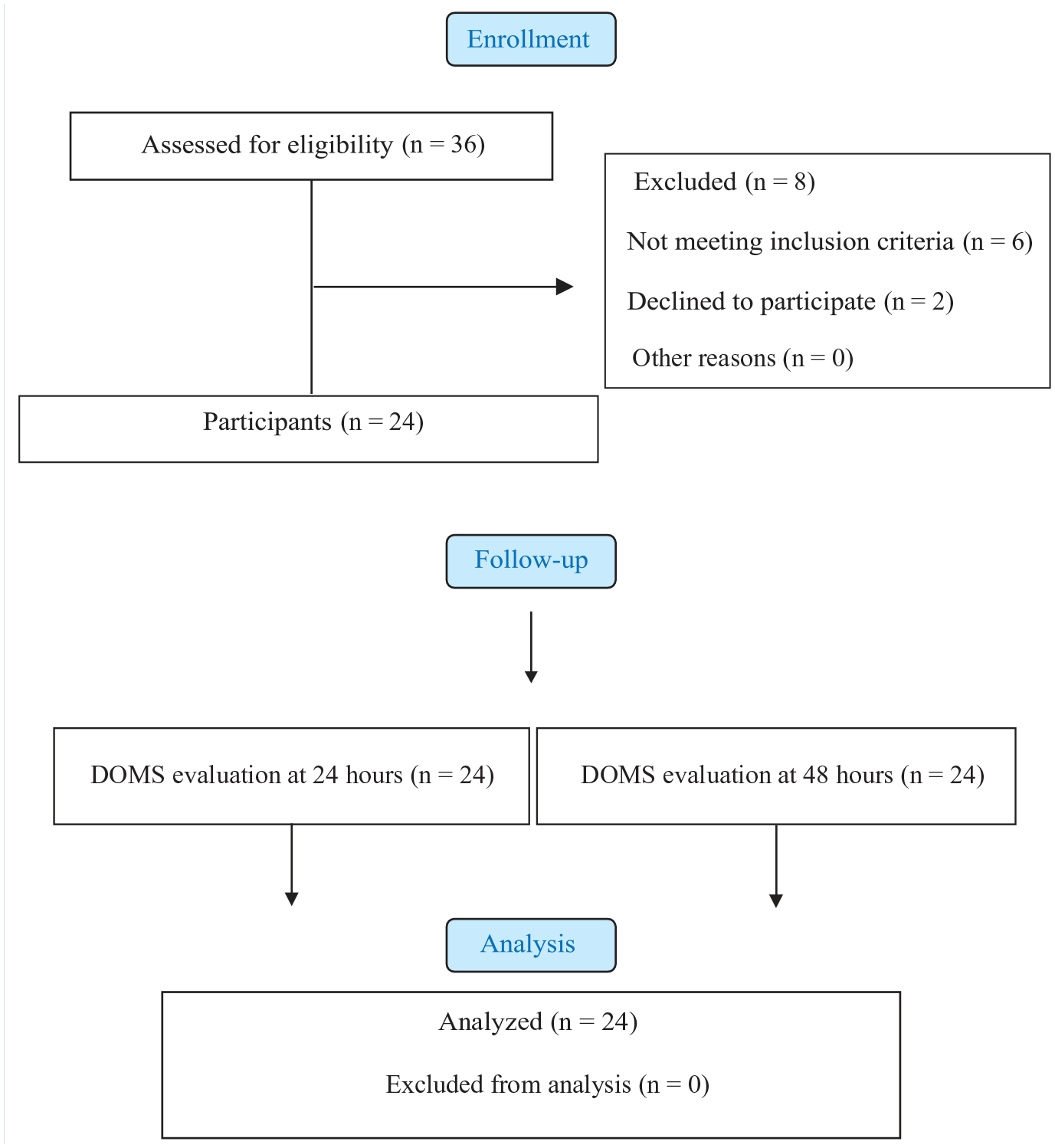
Flowchart of the study. DOMS, delayed-onset muscle soreness.
Ethical approval of the study was obtained from the Ethics Committee of Cyprus International University (No. 100-4466). In addition, after participants were given general information about the study, their declaration that they accepted to participate in the study voluntarily was taken with an “Informed Consent Form.” This study was carried out in accordance with the Declaration of Helsinki.
Participants visited the laboratory 3 times. At the first visit, DOMS was induced by performing eccentric-concentric trunk flexion exercise for 5 sets of 10 repetitions at 80% of maximal voluntary contraction (MVC) on the trunk muscles. Pulmonary function parameters, respiratory muscle strength and endurance, exercise capacity, pain, fatigue, and dyspnea perception severity were recorded before DOMS and at 24 and 48 hours after DOMS.
The inclusion criteria of the study were to be a healthy person aged 18 to 25 years. Exclusion criteria were having a lung, cardiovascular, neurological, systemic, or orthopaedic disease.
DOMS Protocol
A digital dynamometer (Model-01165, Lafayette Instrument Co) was used to measure the maximum repetition force of the trunk flexors. Trunk flexion strength was measured by a handheld dynamometer with a good reliability (between ICC [2,1] = 0.9 and ICC [2,1] = 0.67). 9 Before inducing DOMS, jogging for 10 minutes from low speed to medium speed level and stretching movements for upper and lower extremities were performed for warm-up. The participant was placed in the supine position with a towel in the lumbar region so as not to increase the lumbar cavity. The head was extended in the midline with the knees flexed at 90° and the arms at the sides. The base of the dynamometer was placed by detecting the middle part of the sternum, and the subject was asked to lift their scapula from the bed. Isometric muscle strength was determined by applying counterforce during trunk flexion by the physiotherapist. For a maximum repetition of the trunk muscles, 2 measurements were made with a 45-second rest interval. The values were recorded in pounds by taking the maximum value of the 2 repetitions measured. DOMS was induced by eccentric contraction with 80% of this determined value.
To generate DOMS in the trunk, participants were seated on the bench with the knees flexed at 90° and the soles of the feet in full contact with the floor, keeping the weight at 80% of the predetermined maximum repetition. Participants performed 5 seconds of eccentric contraction and 3 seconds of concentric contraction for the trunk extensor muscles with 80% of the MVC load for 5 sets of 10 repetitions (Figure 2).1,6,14 A voice command was given so that they could follow the tempo; 2-minute rests between sets and 45-second rests between repetitions were given. Participants were requested to rate delayed muscle soreness on a scale ranging from 0 to 10 at 24 and 48 hours.
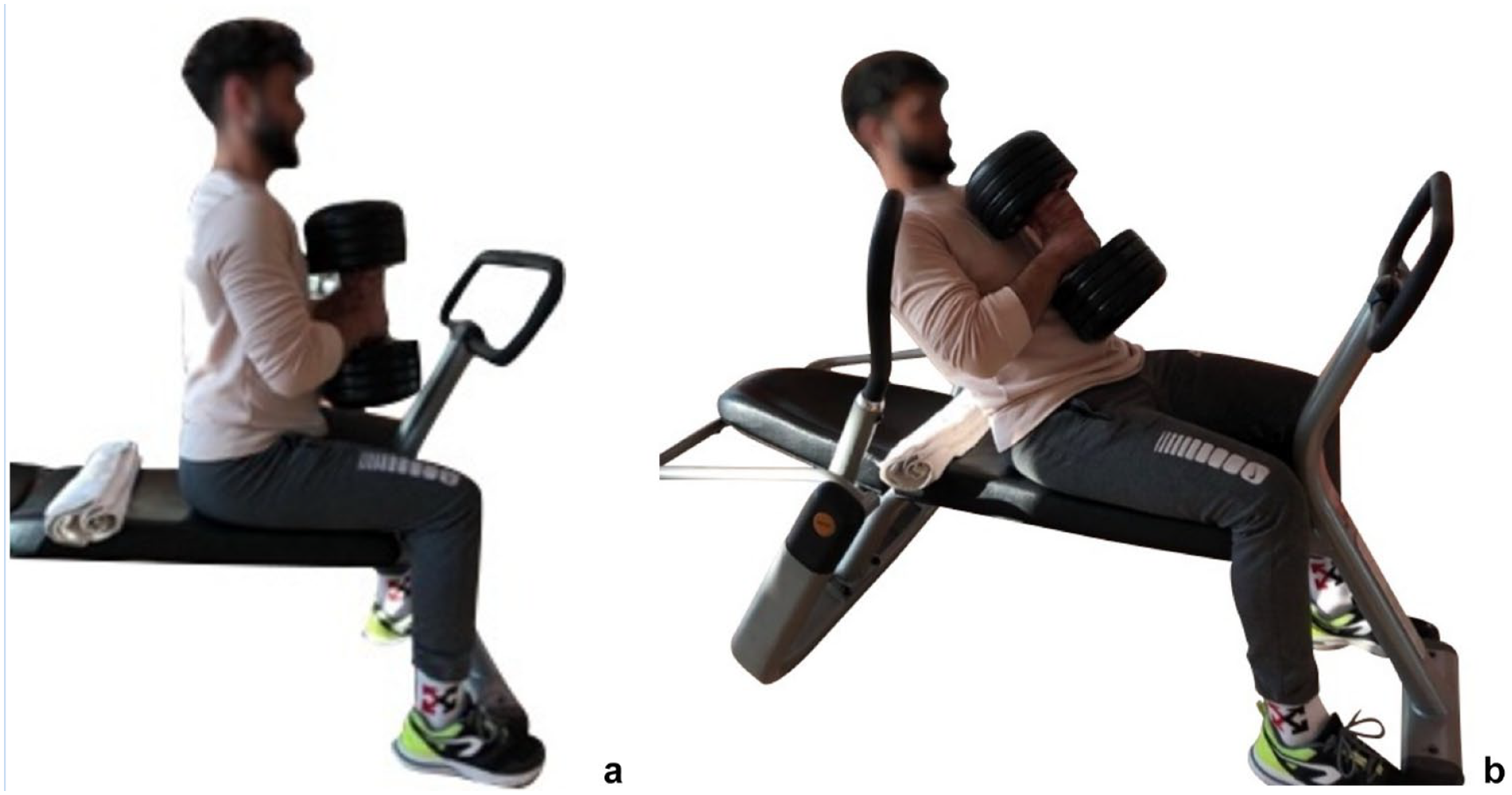
(a) Starting position for eccentric contraction. (b) Trunk extension during eccentric contraction.
Evaluations
Pulmonary function test. Tests were performed using a portable spirometer (MIR Spirolab III). During the tests, the subject was in a sitting position and a nose clip was used. The tests were repeated 3 times and the best measurement value was used. Participants were asked to make a forced expiration after maximum inspiration. From pulmonary function tests, forced vital capacity (FVC), vital capacity (VC), forced expiratory volume in the first second (FEV1), and maximal midexpiratory flow rate (FEF 25% to 75%) measurements were made.25,29 FVC%, FEV1%, and FEF 25% to 75% are also expressed as a percentage of the expected values according to age, height, body weight, and sex and were measured according to recommended standards. 22
Pulmonary function test measurements were made in all subjects at rest and at 24 and 48 hours after trunk-oriented DOMS.
Respiratory muscle strength measurement. Respiratory muscle strength validity and reliability were demonstrated (maximal inspiratory pressure [MIP] intraclass correlation coefficient [ICC] = 0.90, maximal expiratory pressure [MEP] ICC = 0.93) by measuring MIP and MEP with a portable intraoral pressure measuring device (MicroRPM Respiratory Muscle Testing). 14 Measurements were made using a nose clip that prevents nasal breathing and were performed 5 times until a difference of 5 cmH2O remained, with a 30-second rest period between measurements to record the best value, and the best result was recorded in cmH2O. 5 MIP% and MEP % were expressed as a percentage of the expected values according to age, height, body weight, and sex and were measured according to recommended standards. 22 MIP and MEP values were recorded in cmH2O. MIP and MEP measurements were repeated at least 3 times. The best value was used if the difference between the measurements was <10% or 10 cmH2O. The value is also expressed as a percentage of normal reference values calculated according to the participant’s age and sex. 28 This test was carried out at rest before and at 24 and 48 hours after DOMS.
Respiratory muscle endurance test. Respiratory muscle endurance was evaluated with a threshold-loaded (constant) respiratory muscle trainer (Power Breathe, POWERbreathe International Ltd) with proven validity and reliability (ICC = 0.96). 3 In the evaluation, the measurements were made by attaching a nose clip to the nose of a subject in a sitting position in the chair. Initial workload was applied at 60% of the MIP. Subjects performed respiratory efforts while breathing through Power Breathe’s rubber tubing for 10 minutes with a lip seal as the nose was occluded. Patients were informed that they could remove the device if they felt breathless and, in this case, the test would end. 29 The results of the test were recorded as pressure (cmH2O), time (seconds), and pressure × time (cmH2O × seconds). This test was performed at rest before DOMS, and at 24 and 48 hours after DOMS.
Exercise capacity and other tests. The exercise capacity of the subjects was evaluated with the 6-minute walk test (6-MWT) and a submaximal test with high validity and reliability (ICC = 0.94).17,27 The distance covered in a 6-minute walk was calculated from the number of laps and meters. Values were recorded as a percentage of expected values for age and sex. 27 This test was carried out at rest before and at 24 and 48 hours after DOMS.
Data Analysis
SPSS 20 for Windows (Lead Technologies Inc, SPSS Inc) was used for statistical analyses. Power analysis was carried out according to results of the pilot study of 10 participants. The mean and standard deviation values of the respiratory muscle endurance parameter were examined for sample size analysis. The effect size was calculated with 0.8 and 80% power, taking into account α = 0.05, β = 0.20 as suggested by Cohen. 8 The number of repetitions was taken as 3 for the analysis of variance (ANOVA) test (Pre, 24, 48). According to results, 24 healthy subjects were included in the study. One-way ANOVA was performed in repeated measurements for data with normal distribution (Shapiro-Wilk test) and those with normal distribution as a result of log transformation. Results are presented as means and standard deviations. Freidman’s 2-way ANOVA was applied for categorical and non-normally distributed data. Bonferroni correction was performed in all ANOVA applications. For all comparisons, type I error P < 0.05 was considered to be statistically significant.
Results
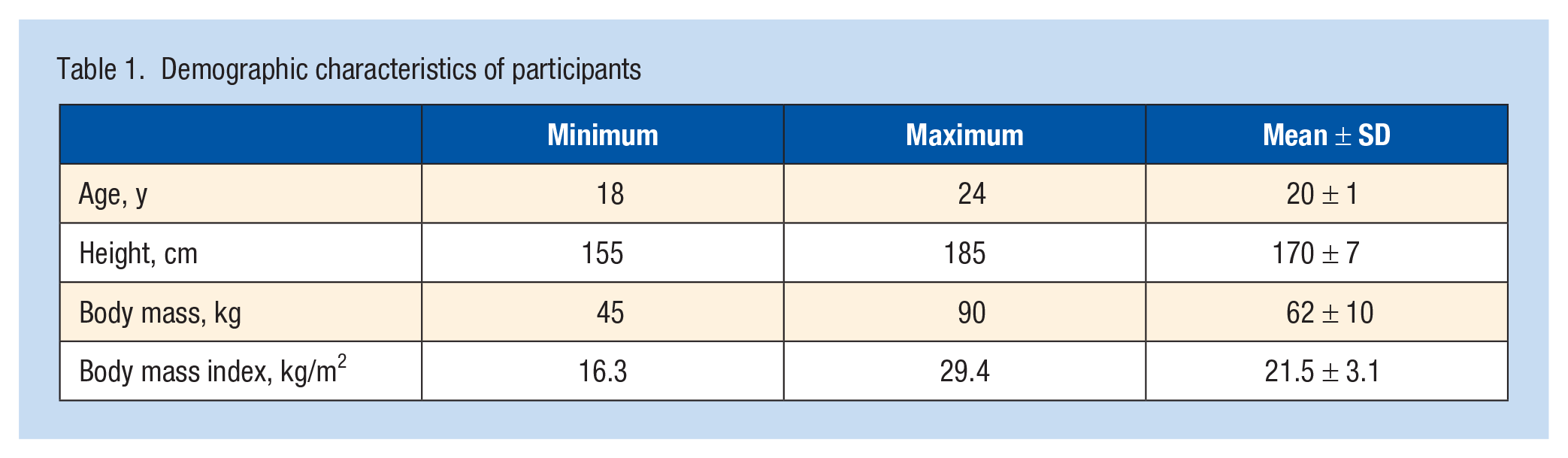
The mean age of the 24 participants whose demographic information is listed in Table 1 was 21 ± 1 years. At 24 and 48 hours after the intervention, the resting DOMS pain score of the participants was 3 ± 2 and 2.5 ± 2, respectively. Table 2 presents the comparison of pulmonary function, respiratory muscle strength, respiratory muscle endurance test, and exercise capacity before, and at 24 hours and 48 hours after, DOMS.
Demographic characteristics of participants
Comparison of pulmonary function, respiratory muscle strength, respiratory muscle endurance test, and exercise capacity before, 24 hours after, and 48 hours after DOMS
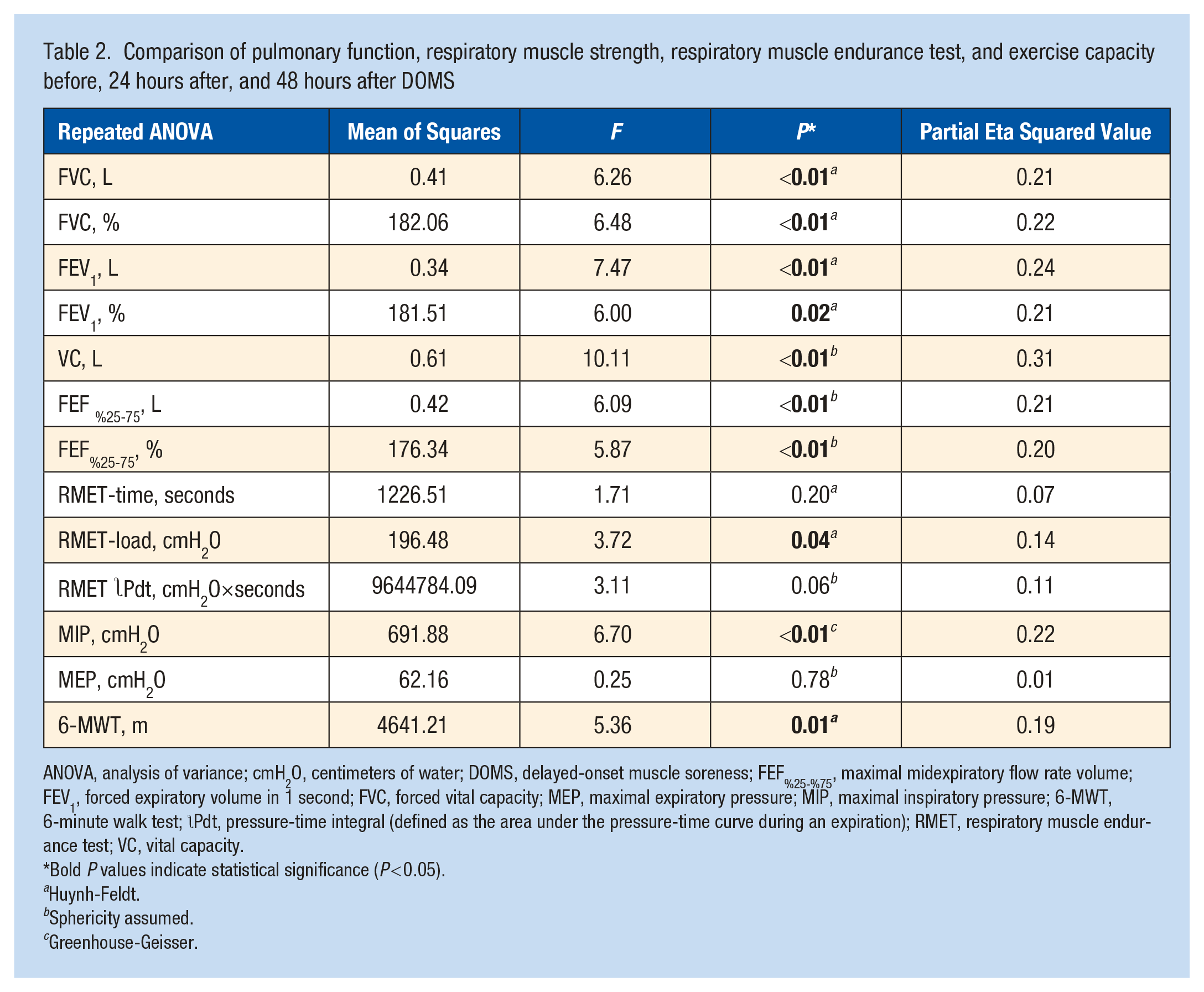
ANOVA, analysis of variance; cmH2O, centimeters of water; DOMS, delayed-onset muscle soreness; FEF%25-%75, maximal midexpiratory flow rate volume; FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity; MEP, maximal expiratory pressure; MIP, maximal inspiratory pressure; 6-MWT, 6-minute walk test;  Pdt, pressure-time integral (defined as the area under the pressure-time curve during an expiration); RMET, respiratory muscle endurance test; VC, vital capacity.
Pdt, pressure-time integral (defined as the area under the pressure-time curve during an expiration); RMET, respiratory muscle endurance test; VC, vital capacity.
Bold P values indicate statistical significance (P < 0.05).
Huynh-Feldt.
Sphericity assumed.
Greenhouse-Geisser.
Pulmonary Function
Most of the pulmonary function parameters measured decreased at 24 hours after DOMS (DOMS-24) and 48 hours after DOMS (DOMS-48) compared with pre-DOMS values. Compared with pre-DOMS, the measured FVC value in DOMS-24 decreased (P1 = 0.02). In terms of FVC measurements, no difference was found between pre-DOMS and DOMS-48, and between DOMS-24 and DOMS-48 (P2 = 0.05; P3 ≥ 0.99). Compared with pre-DOMS values, the calculated FVC-% decreased in DOMS-24 and DOMS-48 (P1 = 0.02; P2 = 0.04), but no significant difference was observed between DOMS-24 and DOMS-48 measurements in terms of FVC-% (P3 ≥ 0.99). Compared with pre-DOMS, measured FEV1 values were found to be decreased in DOMS-24 and DOMS-48 (P1 = 0.02; P2 = 0.02), but FEV1 values were found to be similar in DOMS-24 and DOMS-48 (P3 ≥ 0.99). FEV1% values were also found to have the same trend with FEV1 values (P1 = 0.04; P2 = 0.04; P3 ≥ 0.99). Whereas the differences between the pre-DOMS VC value and the VC values measured in DOMS-24 and DOMS-48 were significant (P1 < 0.01; P2 < 0.01), no significant difference was found between DOMS-24 and DOMS-48 VLC values (P3 ≥ 0.99). VC % results showed the same trend as VC (P1 = 0.02; P2 < 0.01; P ≥ 0.99). The difference between the pre-DOMS and DOMS-48 values in terms of FEF25%-75% and FEF25%-75% was statistically significant (P2 = 0.01) (Table 3).
Comparison of pulmonary function values measured before, 24 hours after, and 48 hours after DOMS
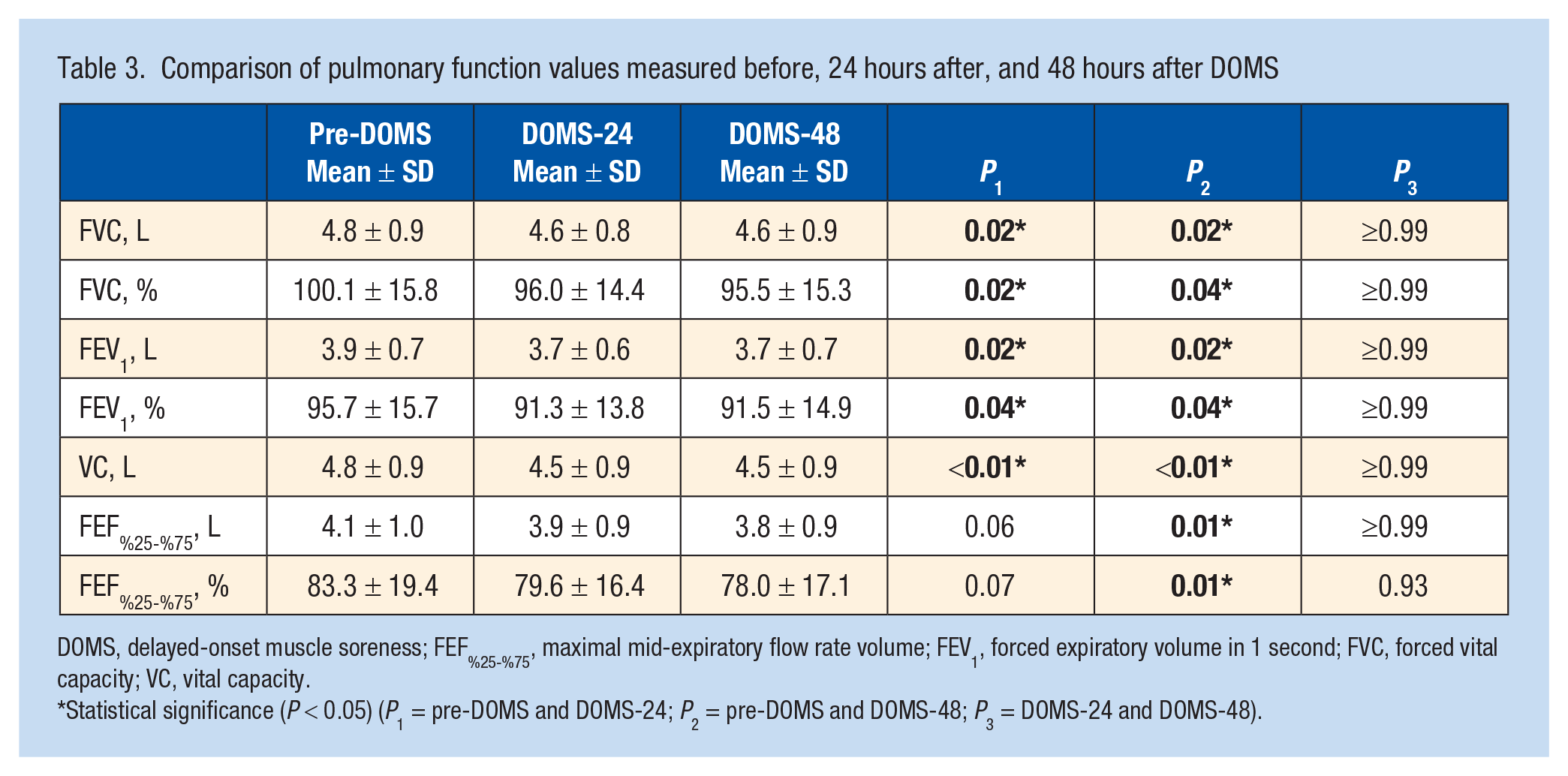
DOMS, delayed-onset muscle soreness; FEF%25-%75, maximal mid-expiratory flow rate volume; FEV1, forced expiratory volume in 1 second; FVC, forced vital capacity; VC, vital capacity.
Statistical significance (P < 0.05) (P1 = pre-DOMS and DOMS-24; P2 = pre-DOMS and DOMS-48; P3 = DOMS-24 and DOMS-48).
Respiratory Muscle Strength Measurement
When the MIP values of the respiratory muscle strength measurements made in pre-DOMS, DOMS-24, and DOMS-48 were compared, DOMS-24 measurement values were lower than pre-DOMS values (P1 = 0.02). Among the calculated MIP% values, DOMS-24 and DOMS-48 values were decreased significantly compared with the pre-DOMS values (P1 = 0.02, P2 = 0.05). No difference was observed between all 3 measurements of MEP and MEP% values (P1 = P2 = P3 = 1) (Table 4).
Comparison of respiratory muscle strength results before, 24 hours after, and 48 hours after DOMS
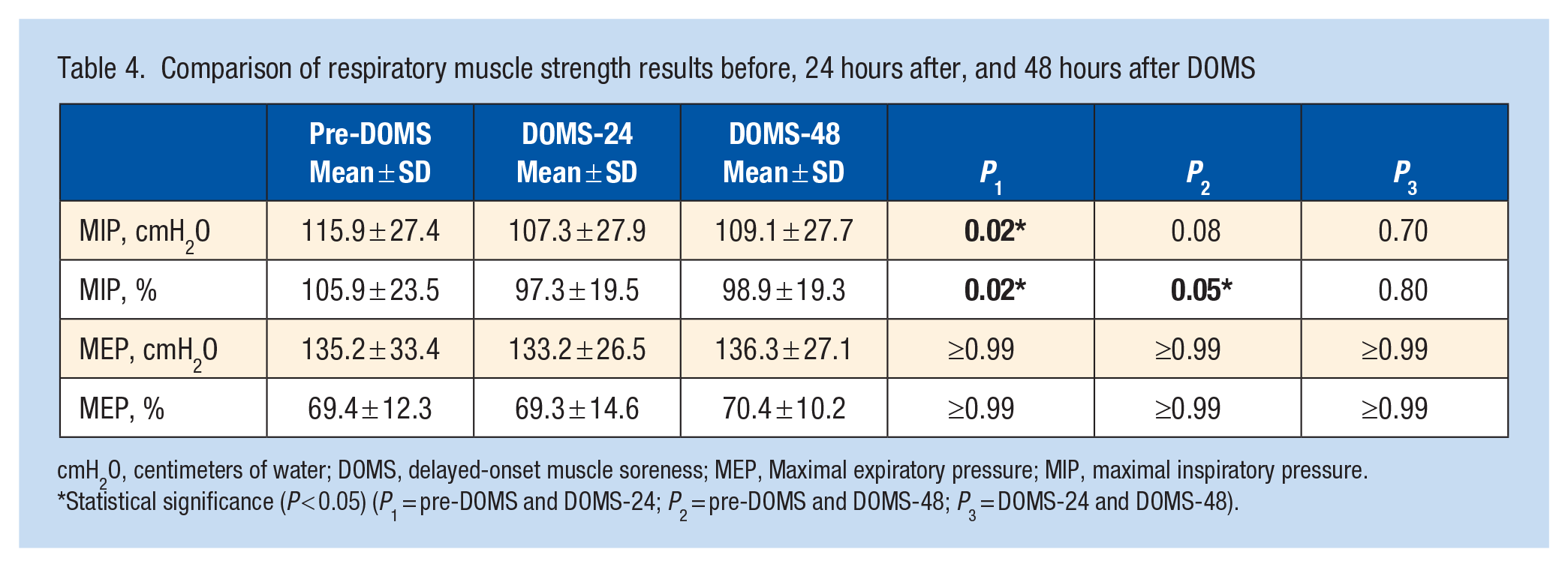
cmH2O, centimeters of water; DOMS, delayed-onset muscle soreness; MEP, Maximal expiratory pressure; MIP, maximal inspiratory pressure.
Statistical significance (P < 0.05) (P1 = pre-DOMS and DOMS-24; P2 = pre-DOMS and DOMS-48; P3 = DOMS-24 and DOMS-48).
Respiratory Muscle Endurance
The results of respiratory muscle endurance tests performed before and at 24 hours and 48 hours after DOMS did not reveal a significant difference in terms of load and time in all 3 conditions (P > 0.5) (Table 5).
Comparison of respiratory muscle endurance test results before, 24 hours after, and 48 hours after DOMS (1-way ANOVA in repeated measurements, Bonferroni correction)
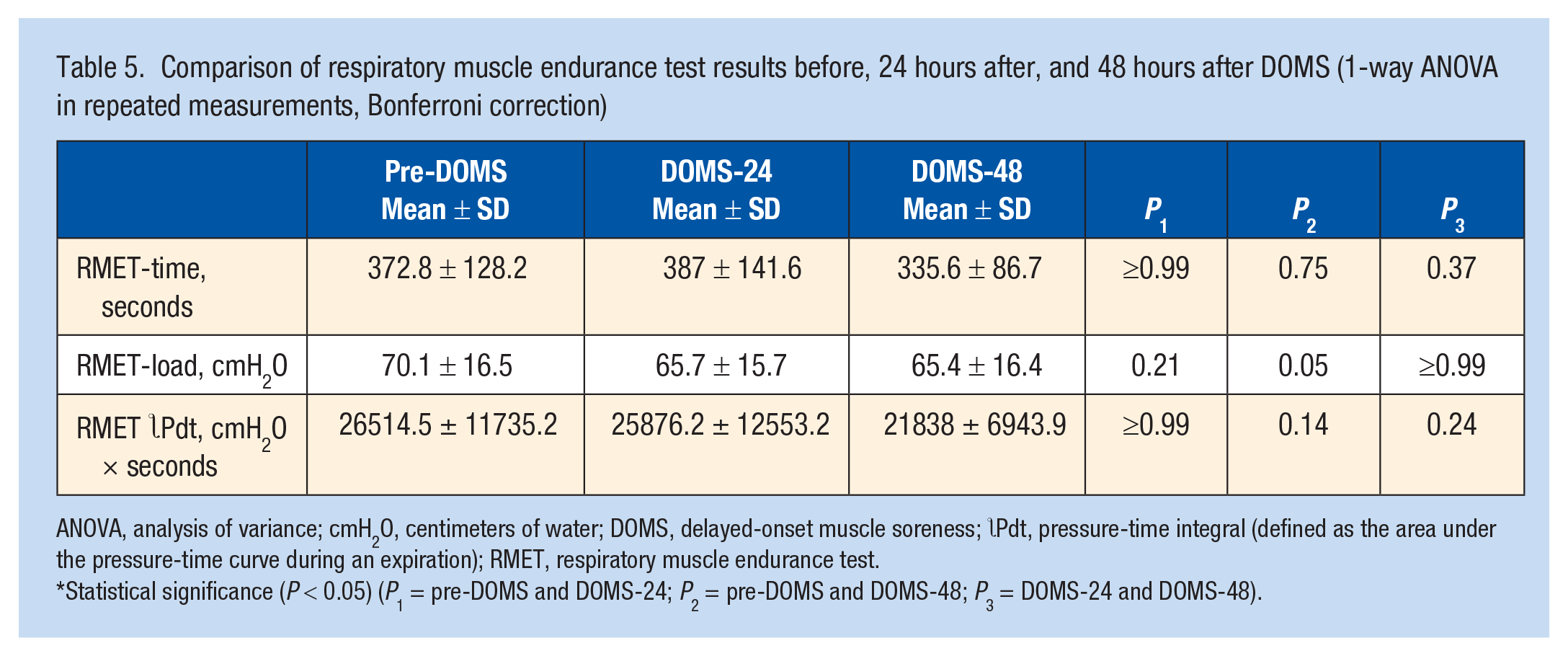
ANOVA, analysis of variance; cmH2O, centimeters of water; DOMS, delayed-onset muscle soreness; Pdt, pressure-time integral (defined as the area under the pressure-time curve during an expiration); RMET, respiratory muscle endurance test.
Statistical significance (P < 0.05) (P1 = pre-DOMS and DOMS-24; P2 = pre-DOMS and DOMS-48; P3 = DOMS-24 and DOMS-48).
Exercise Capacity
In the exercise capacity measurements made for pre-DOMS, DOMS-24, and DOMS-48, there was a significant difference between the 6-MWT distance and the expected and actual distance ratio values in the pre-DOMS and DOMS-48 measurements (P2 < 0.01). However, there was no statistically significant difference between the measurements in pre-DOMS and DOMS-24, and between DOMS-24 and DOMS-48 (P1 > 0.05; P3 > 0.05) (Table 6).
Comparison of exercise capacity results before, 24 hours after, and 48 hours after DOMS
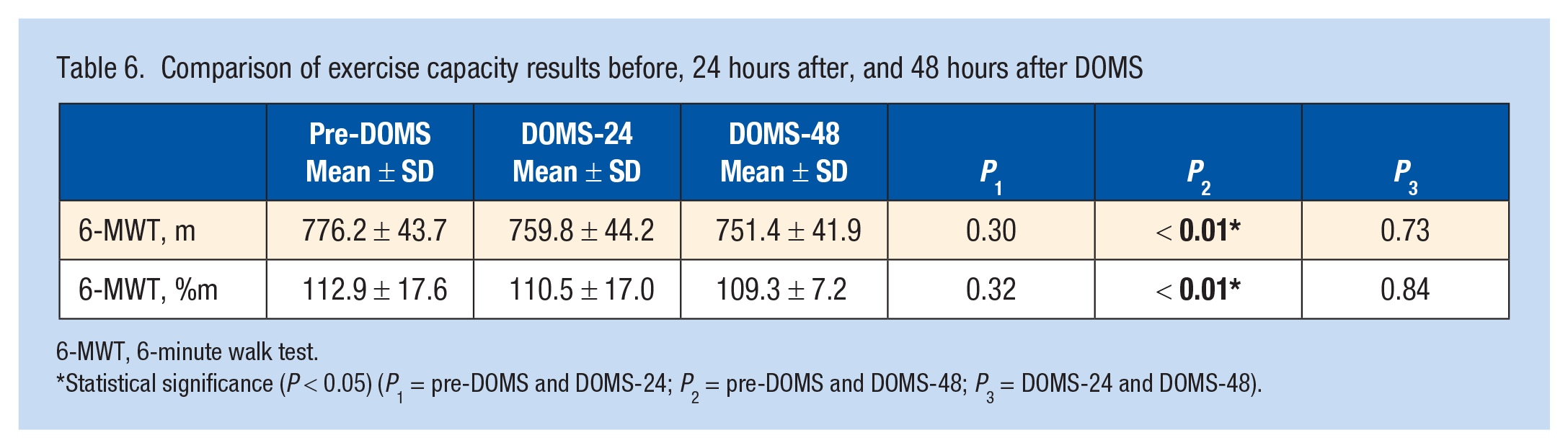
6-MWT, 6-minute walk test.
Statistical significance (P < 0.05) (P1 = pre-DOMS and DOMS-24; P2 = pre-DOMS and DOMS-48; P3 = DOMS-24 and DOMS-48).
Discussion
In this study, the effects of the delayed muscle pain induced by eccentric exercises for trunk muscles on respiratory function parameters, respiratory muscle strength, respiratory muscle endurance, and exercise capacity were investigated. As a result of the study, pulmonary function test results, inspiratory muscle strength, and exercise capacity values decreased 24 and 48 hours after DOMS in trunk muscles.
The first possible reason for respiratory function to be affected as a result of DOMS in trunk muscles may be the decrease in trunk mobility after DOMS. Restrictive type respiratory dysfunction is more common due to decreased mobility in the thorax. 30 In addition, studies on different musculoskeletal pain have reported a correlation between the chronic nature of pain and the effect on respiratory function.16,24 Since thoracic mobility is associated significantly with respiratory muscle strength and lung function, 18 decreased thoracic mobility due to pain is a parameter that can affect respiratory function directly. As stated in studies on pain in the literature,18,23,24 it is thought that there is a significant decrease in pulmonary function test values due to increased perception of pain intensity, fear of feeling pain, and decreased thoracic mobility. A possible reason for this decrease may be the functional limitation during respiratory movement due to pain in trunk muscles.
A second possible reason for the respiratory function to be affected as a result of DOMS formation in trunk muscles may be that the accessory inspiratory and auxiliary expiratory muscles fail to activate. It is thought that these results occur due to the decrease in expiration of these muscles by contracting and a decrease in allowing inspiration by stretching caused by DOMS in forced expiratory muscles (abdominal wall muscles such as rectus abdominis, external and internal oblique muscles, transversus abdominis) and internal intercostal muscles. Especially since MIP values decreased at 24 hours, we can conclude that the painful muscles involved in DOMS are more sensitive to stretching and do not allow it. These results are also compatible with studies showing that postexercise stretching protocols have no effect on DOMS at 24 hours postexercise. 2
This study also shows that DOMS pain causes a decrease in exercise capacity as indicated by negatively affected 6-MWT results. In chronic painful conditions such as low back, hip, and knee pain, the functional capacity of the person is also affected. 15 The reasons for the limitations in exercise capacity are multifactorial. Functional exercise capacity is limited mostly due to the decrease in lung gas exchange and the resulting increased ventilation need, dynamic hyperinflation, and dyspnea.26,27 In this study, it is thought that the decrease in thoracic mobility due to pain and the inability to meet the increased ventilation need required by exercise and/or dynamic hyperinflation affect the results of 6-MWT negatively.
Limitations
The most important limitation of the study was that DOMS was evaluated using the visual analog scale, and physiological methods such as the lactic acid test were not used. Although measuring the pain perception of the participants guaranteed the formation of DOMS, the fact that the parameters that create the pain were not revealed physiologically may have created a deficiency in terms of standardization of pain intensity and significant individual variation. Another limitation of our study is the inability to comprehensively identify the exact origin of the impairment in pulmonary function tests resulting from the development of DOMS in trunk muscles. Consequently, the specific inspiratory and expiratory muscle groups responsible for the impact on respiratory functions remain unknown based on the findings of our investigation.
Conclusion
In the present study, there was a 4% to 7.5% decrease in respiratory function parameters and a 6.6% decrease in respiratory muscle strength due to DOMS formation measured with a visual analog scale. Therefore, when creating training and exercise programs, it should be taken into account that delayed muscle soreness may affect respiratory functions and, thereby, athletic performance may be somewhat affected. It may be useful to determine training and competition planning in elite athletes taking this factor into account.
Footnotes
The authors report no potential conflicts of interest in the development and publication of this article.