
Abstract
Background:
Basketball-related fractures involving the lower extremities frequently present to emergency departments (ED) in the United States (US). This study aimed to identify the primary mechanisms, distribution, and trends of these injuries.
Hypothesis:
We hypothesize that (1) lower extremity fracture frequency will decrease from 2013 to 2022, (2) the ankle will be the most common fracture site, and (3) noncontact twisting will be the most common injury mechanism.
Study Design:
Descriptive epidemiological.
Level of Evidence:
Level 3.
Methods:
The National Electronic Injury Surveillance System (NEISS) was queried for lower extremity fractures from basketball presenting to US EDs from January 1, 2013 to December 31, 2022. Patient demographics, injury location, and disposition were recorded. The injury mechanism was characterized using the provided narrative. National estimates (NEs) were calculated using the NEISS statistical sample weight. Injury trends were evaluated by linear regression.
Results:
There were 6259 cases (NE: 185,836) of basketball-related lower extremity fractures. Linear regression analysis of annual trends demonstrated a significant decrease in lower extremity fractures over the study period (2013-2022: P = 0.01; R2 = 0.64). The most common injury mechanism was a noncontact twisting motion (NE: 49,897, 26.9%) followed by jumping (NE: 39,613, 21.3%). The ankle was the most common fracture site (NE: 69,936, 37.6%) followed by the foot (NE: 49,229, 26.49%). While ankle and foot fractures decreased significantly (P < 0.05), fractures of the lower leg, knee, toe, and upper leg showed no significant trends (P = 0.09, 0.75, 0.07, and 0.85, respectively).
Conclusion:
Basketball-related lower extremity fractures decreased from 2013 to 2022, with the ankle being the most common fracture site and most fractures arising from a noncontact twist. Increasing utilization of outpatient clinics may have contributed to the decline, particularly for ankle and foot fractures. The prevalence of ankle fractures and twisting-related injuries reinforces the importance of protective footwear and targeted strengthening protocols.
Basketball is a popular sport worldwide among players of all ages and skill levels. 23 Given the sport’s popularity, a notable injury burden exists, especially involving the lower extremities. 22 From 58% to 66% of all basketball-related injuries involve the lower extremities with 25% of injuries involving the ankle. 7 The mechanism of injury differs in basketball compared with other sports, with an average of 35 to 46 jumping and landing movements per game. 34 There is also a high degree of abrupt acceleration and deceleration as well as pivoting and rotational movements for changing direction. 34
Though sprains remain the most common form of basketball-related injuries, 22 fractures from basketball are a common presentation to emergency departments (EDs) in the United States (US), especially those of the foot, ankle, and knee.3,20,21 In a previous study, it was determined that, from 2005 to 2013, there were an estimated 20,241,049 sports-related admissions to EDs across the US, which equates to an incidence of 7.35 ED visits per 1000 people annually. 21 Fractures made up approximately 20.6% of those admissions, equating to an incidence of 1.51 ED visits per 1000 people annually. 21 After extrapolation, of the estimated 4,159,764 fractures, approximately 799,328 were due to basketball (19.2%). 21 Thus, basketball had the second-highest incidence of fractures among all 18 sports queried. 21
In a 2021 study, Moore et al 22 further described the high frequency of basketball-related ankle injuries, with sprains and fractures being highly prevalent. In addition, the team emphasized that further research is needed to ensure appropriate clinical management of lower extremity basketball injuries, especially of the ankle. 22 In another study, it was determined that basketball accounted for 16.3% of all pediatric fractures that presented to US EDs between 2011 and 2020. 13 Interestingly, the study noted that the COVID-19 pandemic led to an increase in pediatric fractures across all age groups, but it did not stratify basketball-related fractures by body part or mechanism. 13
The burden of basketball-related fractures presenting to US EDs is alarmingly apparent, especially of the lower extremities. Yet, no study has evaluated the distribution of lower extremity fractures from basketball presenting to US EDs and characterized the mechanisms contributing to these injuries. The purpose of this study was to evaluate the frequency, mechanisms, and distribution of basketball-related lower extremity fractures presenting to EDs across the country. The authors hypothesized that (1) the frequency of lower extremity fractures will show a decrease from 2013 to 2022, (2) the ankle will be the most common fracture site, and (3) a noncontact twisting movement will be the most common injury mechanism.
Methods
Database
The National Electronic Injury Surveillance System (NEISS) is a deidentified, publicly available database maintained by the US Consumer Product Safety Commission. 6 Data are collected from a stratified probability sample of approximately 100 hospitals with a minimum of 6 beds and a 24-hour operating ED. The hospitals are grouped into 5 strata: 4 represent hospital EDs of various sizes and 1 represents EDs from children’s hospitals. A statistical sample weight is assigned for each ED based on the inverse of the probability of selection, thus allowing for national estimates (NEs) of injuries to be calculated across the US using the NEISS cases.
Data Extraction
The NEISS database was queried retrospectively for all lower extremity fractures related to basketball (product code 1205) from January 1, 2013 to December 31, 2022. There were 6300 cases of lower extremity fractures due to basketball identified during the study period. The patient’s demographic information (age, race, sex), ED visit date, injury location, and a brief ED narrative were provided for each case extracted.
A narrative describing the injury is available in the NEISS dataset for each patient case. This narrative is not defined by any set parameters but rather is a free text entry pulled from the medical record. The narrative of each case was reviewed by the authors (AY, JJC, and KSN) to code the mechanism of injury. The primary mechanism of injury was defined as the main mechanism that initiated and contributed most significantly to the injury process. When applicable, a secondary mechanism was recorded that contributed to the injury but was not considered the main cause. Mechanisms of injury were coded into predefined categories. “Player-player contact” refers to any injury caused by or involving another player and takes precedence over all other mechanisms. “Jump” injuries were defined as occurring before, during, or after landing from a jump. “Twisting/Rolling” exclusively refers to fractures due to twists, rolls, or inversions. “Fall/Impact with ground” fractures were defined as slips, trips, or collapses resulting in contact with the ground. “Collision/Impact with Object” represents injuries due to hitting walls, metal poles, bleachers, etc. “Running/Pivoting” injuries occurred either while running or when patients accelerated, decelerated, or changed direction. “Other” includes patients stubbing their toe, hyperextension of the body, or any other injuries not clearly defined by the aforementioned mechanisms. Injuries were classified as “Not Specified” if no mechanism was included in the narrative report.
Exclusion Criteria
Cases were excluded if the injury was not a fracture of the lower extremity, was not acquired while playing organized basketball or playing basketball recreationally (ie, at a court, driveway, hoop, etc), or was not sustained directly while playing the sport of basketball (ie, gunshot wound while standing on a basketball court, spectator hit by a basketball or player, playing trampoline basketball, etc).
Statistical Analysis
IBM SPSS Statistics Version 28.0 was used for data analysis. Descriptive statistics were reported as both “raw” numbers (representing the number of cases) and NEs (calculated using statistical weights provided by the Consumer Product Safety Commission). The distribution of fractures between male and female subjects was evaluated using Pearson’s chi-squared testing. Linear regression analysis was employed to identify annual trends in lower extremity fractures from basketball throughout the study period. The independent variable was the year of injury, and the dependent variable was the frequency of basketball-related lower extremity fractures. Annual fracture trends were also stratified by body part. Key assumptions were assessed to ensure the validity of the model: linearity through scatterplots, independence of observations, homoscedasticity via residual plots, and normality using the Shapiro-Wilk test. Benjamini-Hochberg correction was applied to control for the false discovery rate. Adjusted P values, R2, regression coefficient (β), and a 95% CI are reported with statistical significance set at P < 0.05.
Results
There were 6259 cases (NE: 185,836) of lower extremity fractures due to basketball that presented to US EDs from January 1, 2013 to December 31, 2022. A total of 88.7% of injuries were sustained by male patients. The average age was 19.5 ± 9.6 years (range, 2-80 years) with injuries occurring more commonly in the pediatric (≤18 years) population (63.5%) and among White patients (35.3%) (Table 1).
Demographics of all patients assessed in the study
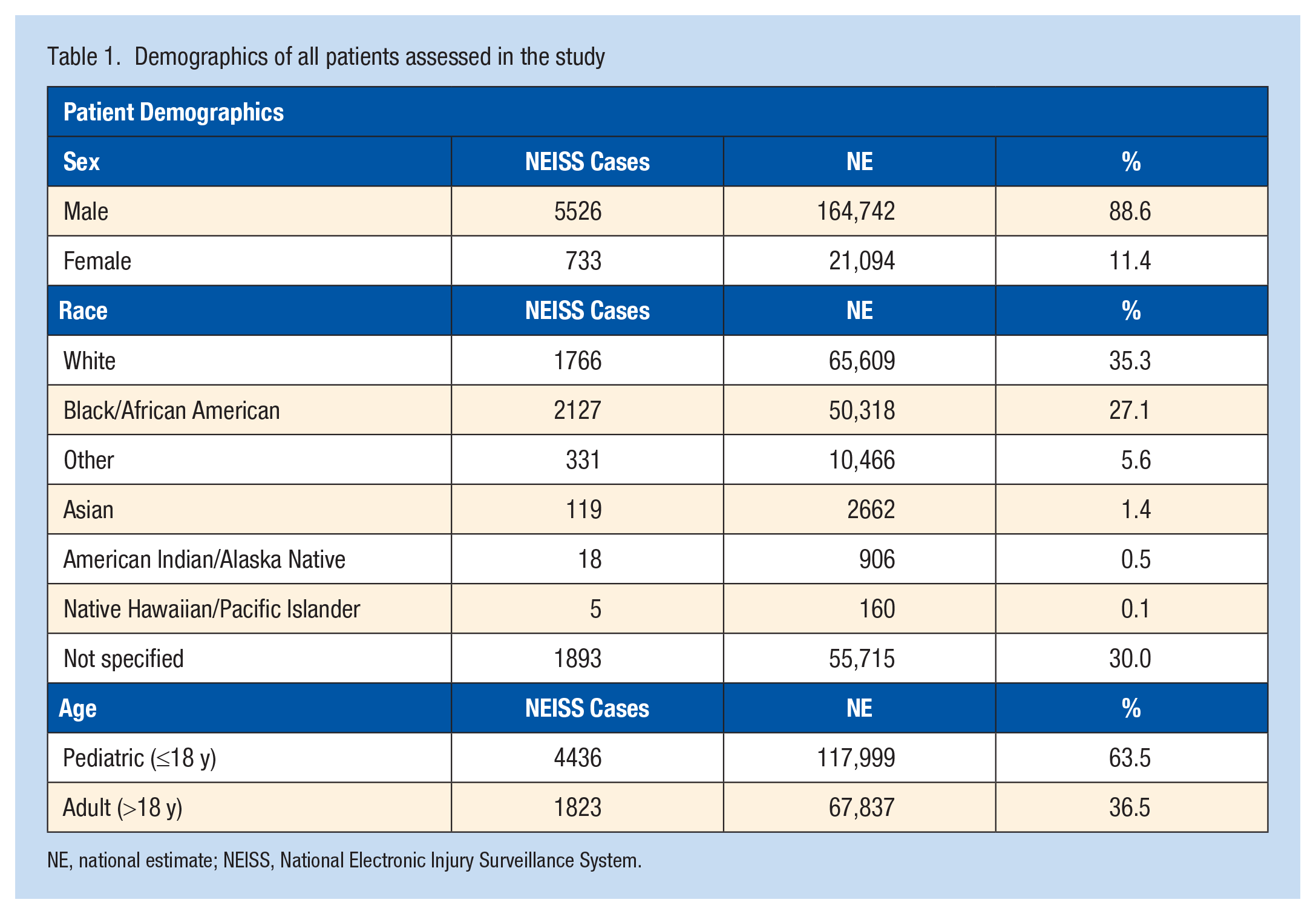
NE, national estimate; NEISS, National Electronic Injury Surveillance System.
Linear regression analysis of annual trends demonstrated a significant decrease in lower extremity fractures over the study period (2013-2022: P = 0.01, R2 = 0.64, β = -1151.02, 95% CI: [-1858.69 to -443.35]) and before the COVID-19 pandemic (2013-2019: P = 0.04, R2 = 0.68, β = -1034.64, 95% CI: [-1842.28 to -227.01]) (Figure 1). The year 2020 represented the lowest frequency, with 10,024 lower extremity fractures presenting to US EDs, which was a 51.5% decrease from prepandemic (2013-2019) levels. In 2021, there were 13,907 injuries, which was an increase of 38.7% from 2020, but this frequency was still below the prepandemic levels by 32.7%. Similarly, the frequency in 2022 was 16.9% lower than prepandemic levels.
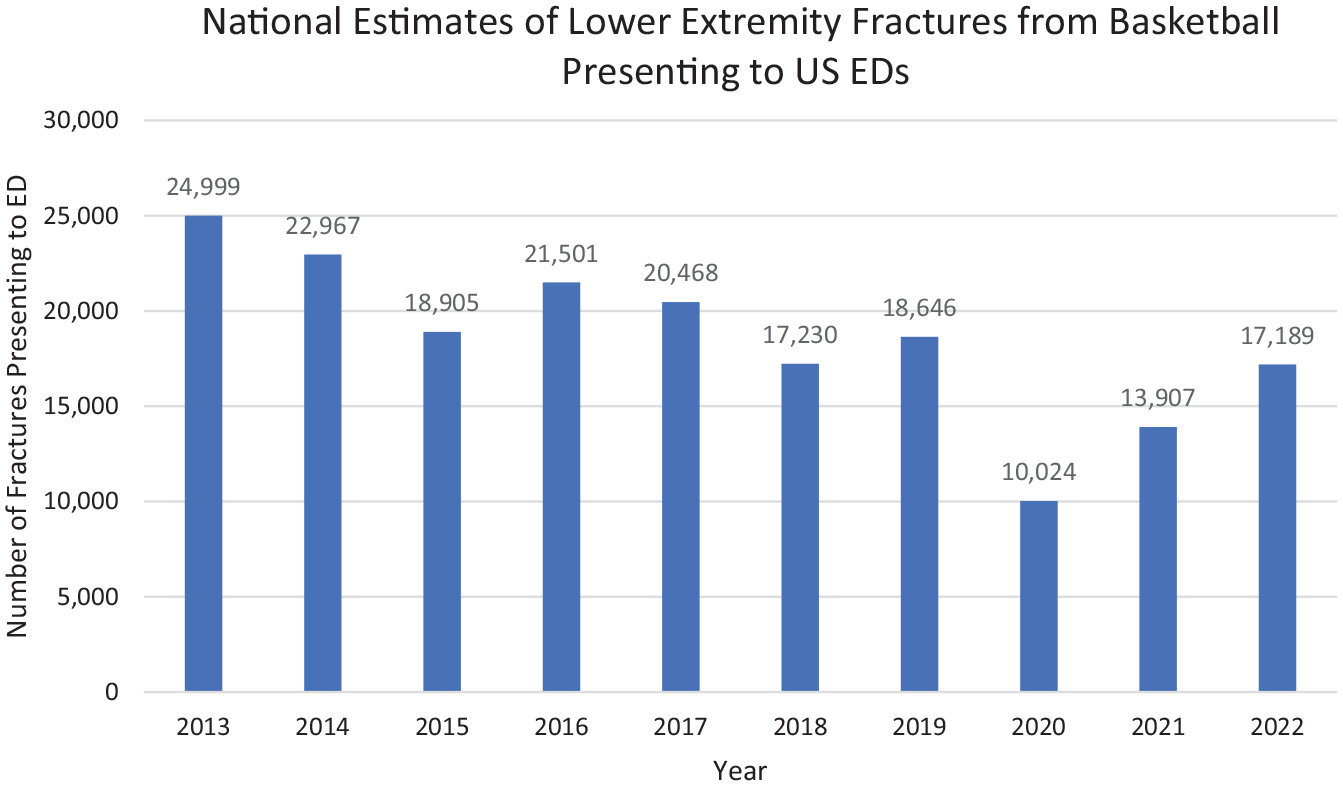
NEs of basketball-related lower extremity fractures presenting to US EDs between January 1, 2013 and December 31, 2022. ED, emergency department; NE national estimate; US, United States.
The most common primary injury mechanism was a noncontact twisting motion, making up 26.9% of injuries (NE: 49,897) (Table 2). Of these twisting injuries, 5.1% secondarily involved a fall (NE: 2559). Jumping was the next most common primary injury mechanism, making up 21.3% of injuries (NE: 39,613). In this group, 24.6% of fractures sustained during jumping involved a twisting motion (NE: 9744), and 9.1% of jumping injuries were associated with a fall (NE: 3598).
Breakdown of fractures by primary mechanism a
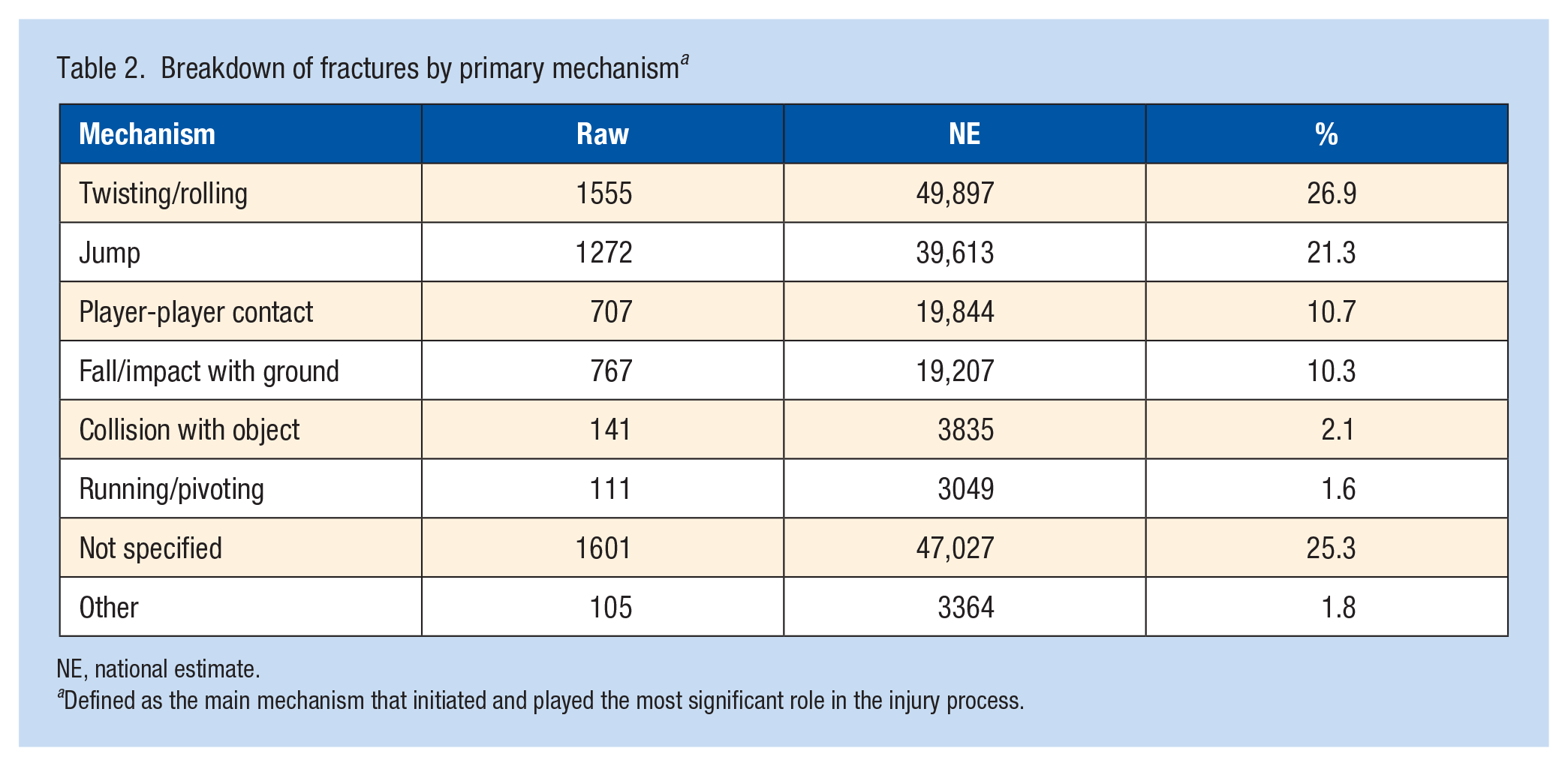
NE, national estimate.
Defined as the main mechanism that initiated and played the most significant role in the injury process.
Player-player contact injuries resulted in 10.7% of fractures (NE: 19,844). Among these contact-related injuries, 24.2% (NE: 4793) occurred while the player was in the act of jumping, 16.5% (NE: 3282) secondarily led to twisting injuries, and 5.0% (NE: 996) involved falls. Fall/impact with the ground was responsible for 10.3% of all injuries (NE: 19,207). Collisions with objects and injuries while running/pivoting accounted for just 2.1% and 1.6% of injuries, respectively.
The ankle was the most common fracture site, making up 37.6% of lower extremity basketball fractures (NE: 69,936) (Figure 2). The foot accounted for 26.5% of fractures (NE: 49,229) and the lower leg made up 21.9% (NE: 40,701). The knee, toe, and upper leg were less commonly injured, making up just 6.6%, 5.8%, and 1.6% of lower extremity fractures from basketball, respectively. Interestingly, there were significant decreases across the study period (2013-2022) for fractures of the ankle (P = 0.02, R2 = 0.52, β = -533.3, 95% CI: [-911.4 to -155.2]) and foot (P < 0.01, R2 = 0.70, β = -415.9, 95% CI: [-621.8 to -209.9]). However, no significant trends were seen for fractures of the lower leg (P = 0.09), knee (P = 0.75), toe (P = 0.07), or upper leg (P = 0.85) (Figure 3).
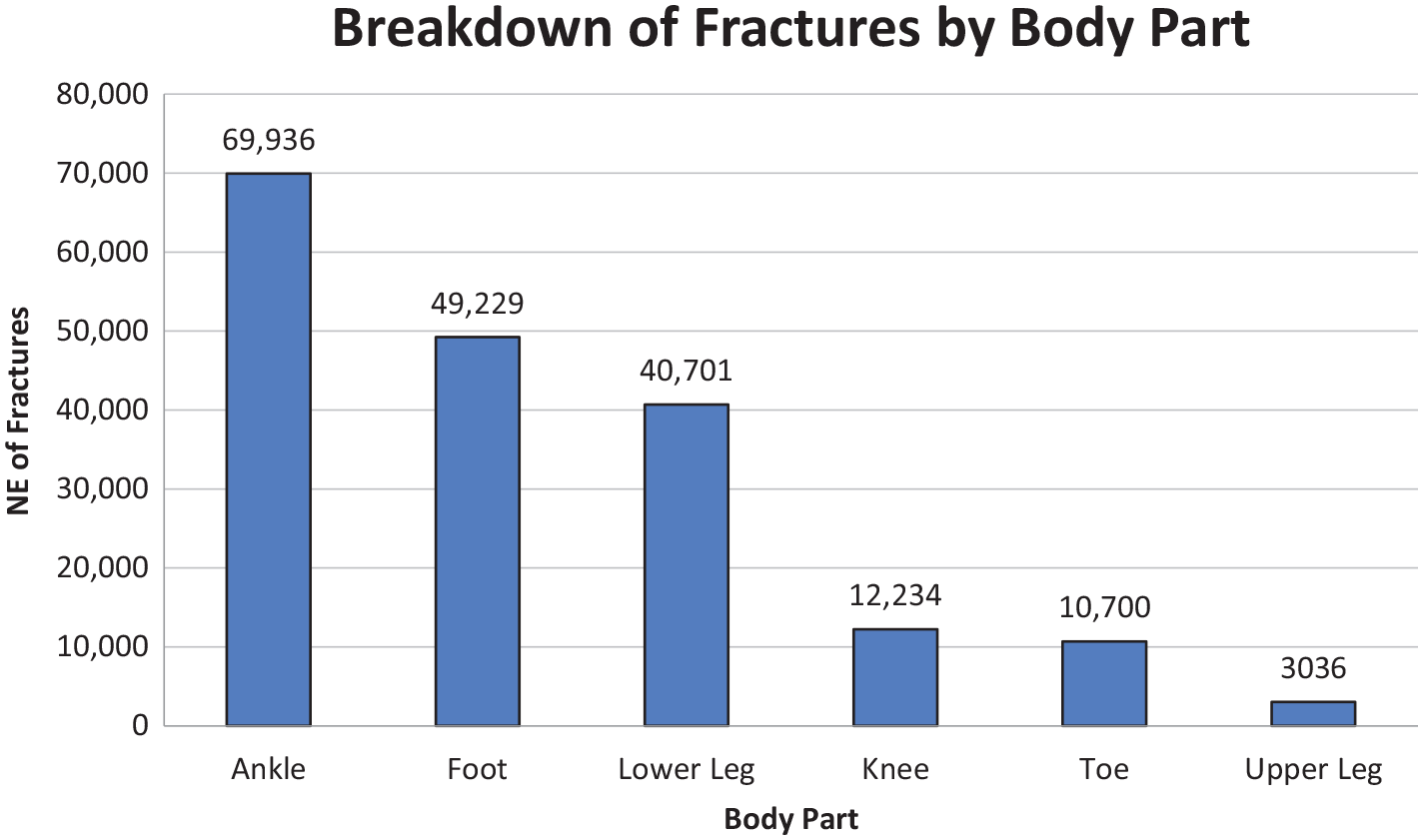
NEs of fractures based on body part. NE, national estimate.
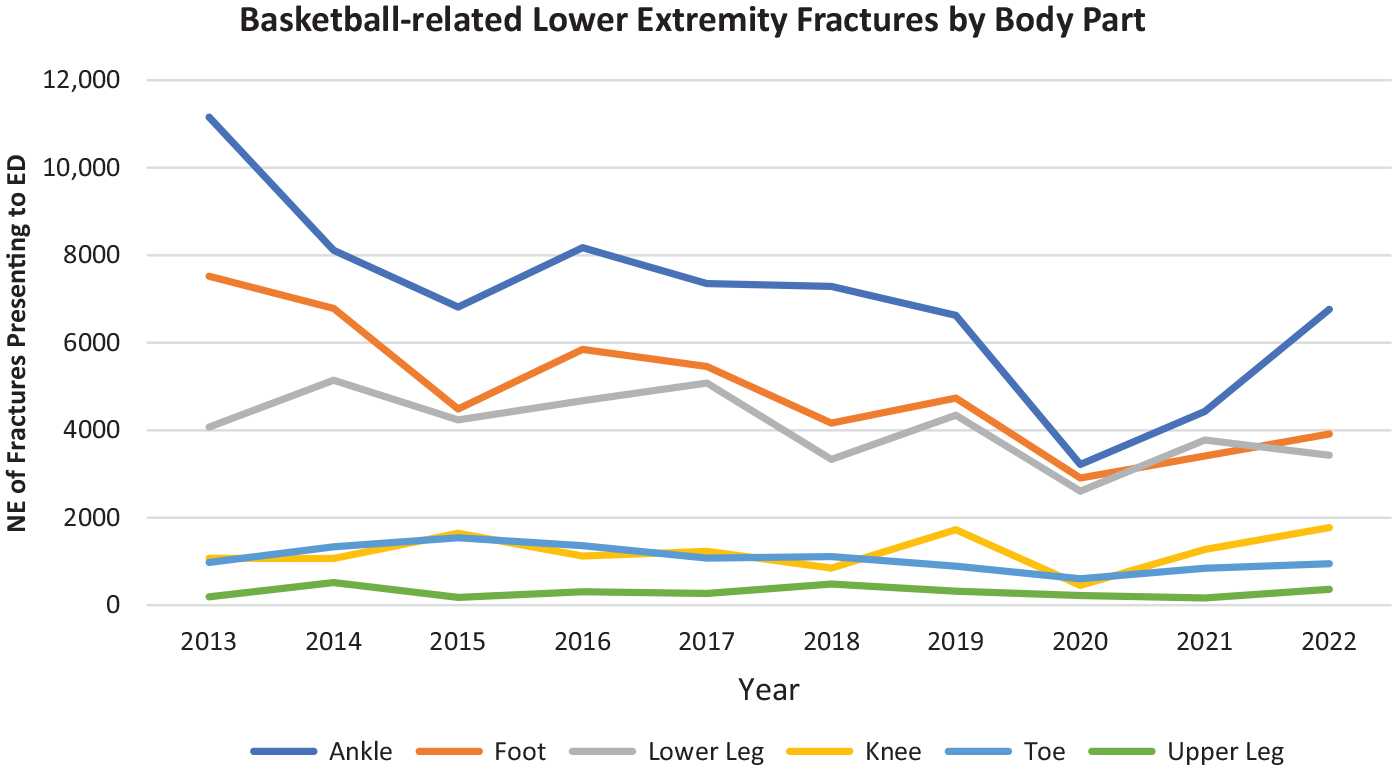
Injury trends stratified by fractured body part from 2013 to 2022. ED, emergency department; NE, national estimate.
Male patients sustained significantly more fractures of the foot, lower leg, and knee than women, while female patients sustained significantly more fractures of the toe (P < 0.01) (Table 3). There were no significant differences (P > 0.05) in the proportion of ankle or upper leg fractures for male versus female patients.
Distribution of fracture locations by sex as a percentage a
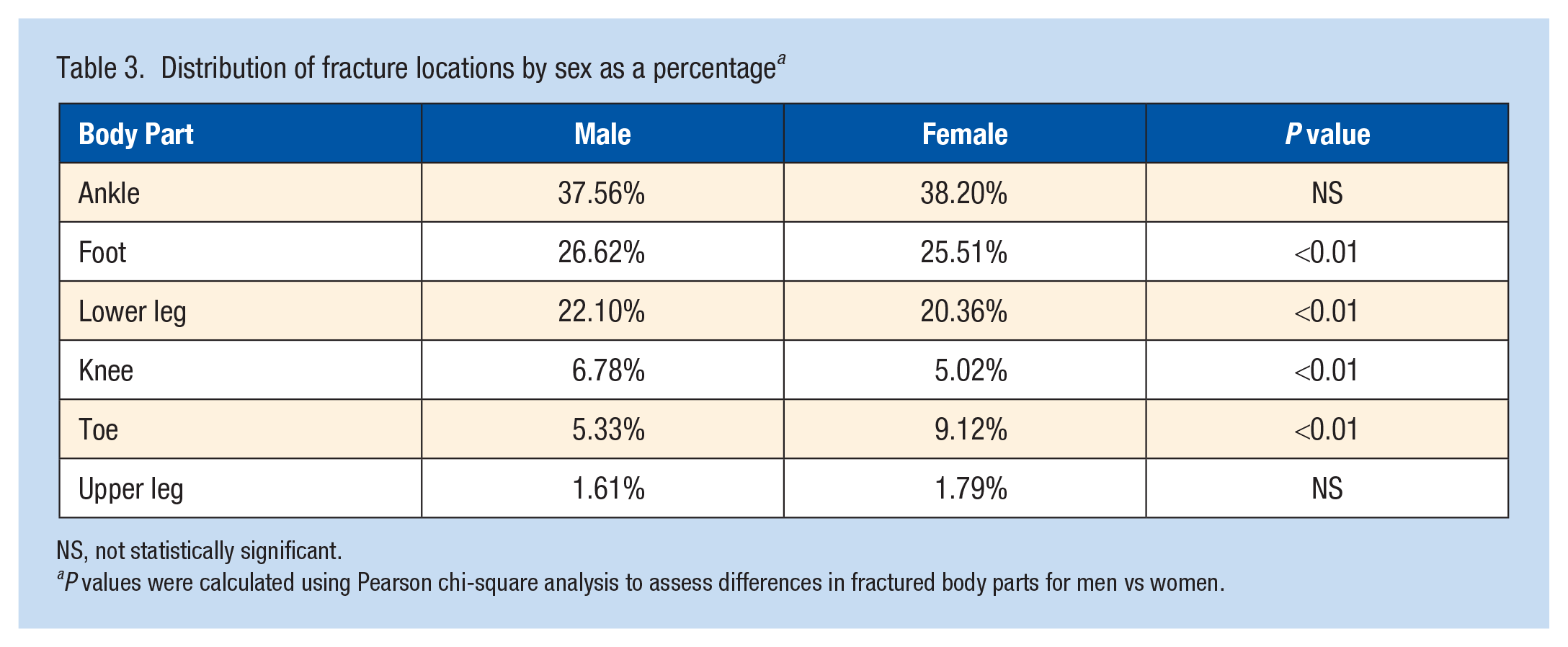
NS, not statistically significant.
P values were calculated using Pearson chi-square analysis to assess differences in fractured body parts for men vs women.
Among injuries that arose due primarily to twisting motions, jumping, and player-player contact, the ankle was most commonly fractured (Table 4). For fractures that resulted from falls or running/pivoting, the lower leg was most commonly affected. Finally, injuries after colliding with objects most frequently resulted in a fracture of the toe.
Distribution of fracture locations by primary mechanism of injury
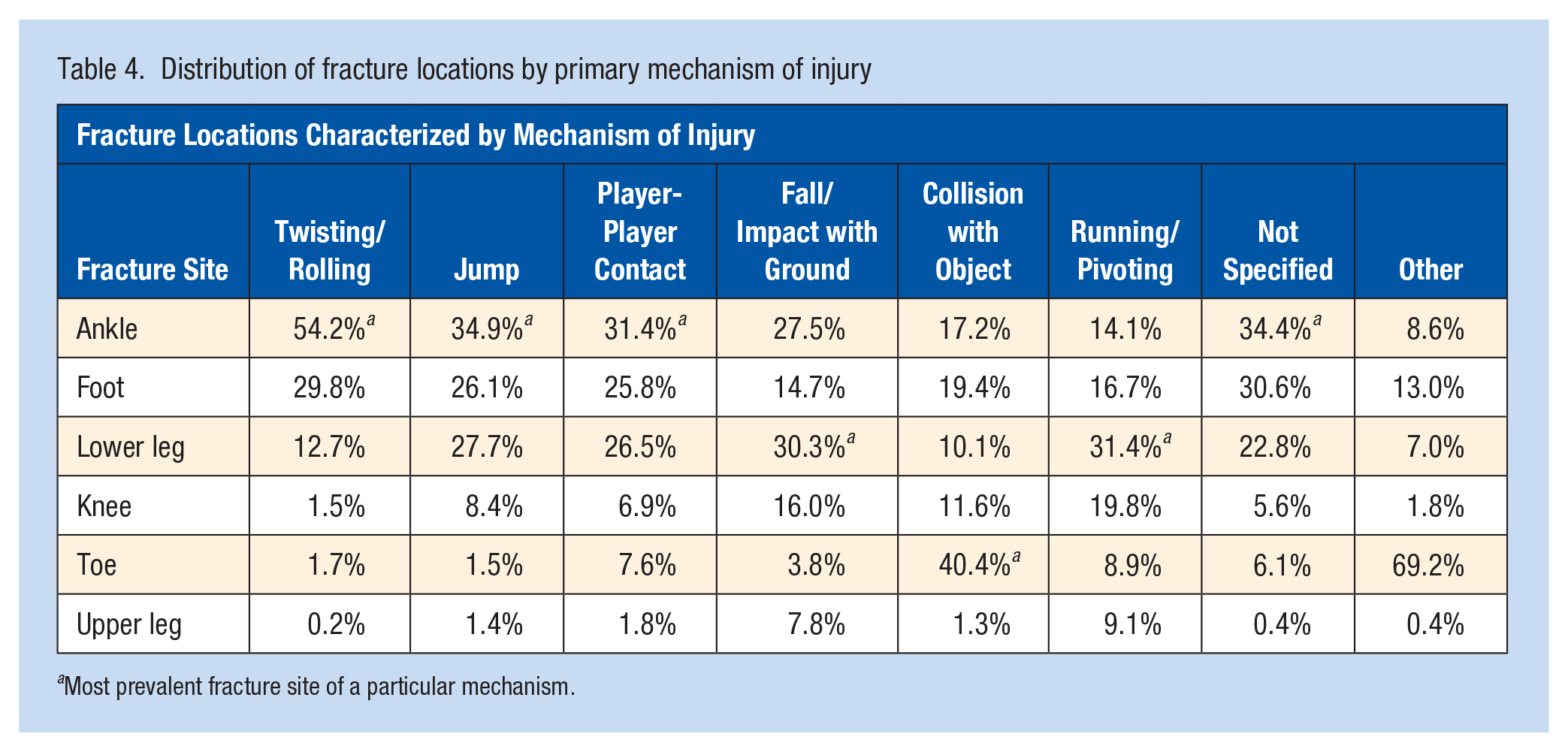
Most prevalent fracture site of a particular mechanism.
While 92.2% (NE: 171,423) of lower extremity fractures were treated/released, 5.8% (NE: 10,763) required admission. Patients who left without receiving treatment, were transferred, or were held for observation made up 2.0% (3650) of all fractures.
Discussion
The purpose of this study was to evaluate the frequency, mechanisms, and distribution of lower extremity fractures due to basketball that presented to US EDs from 2013 to 2022. This study demonstrated that basketball-related lower extremity fractures were more common in the pediatric population and among male patients, with sex-specific differences in the distribution of body parts fractured most frequently. In addition, the frequency of lower extremity fractures presenting to US EDs decreased both across the study period (2013-2022) as well as before the COVID-19 pandemic (2013-2019). The years 2020 and 2021 displayed the lowest frequency of lower extremity fractures presenting to US EDs during the study period, with a steep drop from prepandemic levels. Interestingly, while the presentation of ankle and foot fractures to US EDs declined significantly during the study period, a concomitant reduction was not appreciated in fractures of the lower leg, knee, toe, or upper leg. Finally, noncontact twisting/rolling was found to be the most common primary mechanism of lower extremity fractures, and the ankle represented the highest frequency.
This study demonstrated a high burden of basketball-related fractures occurring in the pediatric population.24,39 This finding is supported by previous literature reporting that basketball contributes a significant proportion of fractures among children 12 to 18 years old. 37 Furthermore, age-specific differences have been highlighted in previous studies with fractures sustained more commonly among younger athletes while strain/sprain injuries, inflammatory joint pain, and dislocations are common among adult athletes.8,37 Adults over 65 years, on the other hand, have been shown to commonly sustain fall-related sports injuries as well as more minor overused-related ligament/muscle injuries.15,16 In this present study, only 0.53% of lower extremity fractures were sustained by those aged 60 years and older, and only 1.5% were among those 50 years and older, which supports the available literature that fractures from basketball occur commonly among younger athletes.
According to data from the National Federation of State High School Associations, male players make up 57.5% of high school basketball players. However, this present study demonstrated a disproportionate number of male players (88.7%) presenting to US EDs with a basketball-related lower extremity fracture. 26 Although previous literature has reported that lower extremity injuries are more common among female than male players, 5 it has also been suggested that overall ED utilization for sports-related injuries may be lower among females.5,35 Previous studies have also reported a higher proportion of sprains and ligamentous injuries among female players,14,36 and a higher odds (1.21) of sports-related fractures among male players. 21 The fracture distributions in this study may thus be attributable to a higher propensity for fracture among male players and lower ED utilization for sports injuries among female players.33,37 Nonetheless, the stark difference in sex-specific ED presentations identified in this study has significant clinical implications. The potential for delayed care and underdiagnosing of sports-related fractures among female subjects warrants additional research surrounding sex-specific differences in ED presentations for fractures.
One of the key findings of this study was the significant decrease in lower extremity fractures presenting to EDs between 2013 and 2022. The pandemic likely played a key role in reducing the number of fracture visits in 2020 due to the cancellation of organized sports activities and patient hesitancy to visit hospitals.11,31 In the present study, there were just 10,024 lower extremity fractures that presented to US EDs in 2020, a drastic decrease of 46.2% from 2019 and 51.5% from prepandemic levels (2013-2019). While the frequency increased from 2020 to 2021, 2021 levels were still 25.4% lower than in 2019. With the recovery of organized sports in 2022, 17,189 lower extremity fractures presented to US EDs, which approached the 2019 frequency of 18,646. However, the 2022 frequency was still 16.9% below the 2013 to 2019 average of 20,674. These findings represent a disproportionate decrease (51.5%) in presentation to US EDs in 2020 compared with the 34.6% decrease in sports-related ED visits from prepandemic levels reported by the Sabbagh et al 30 study. Given the increasing rates of lower extremity fractures in 2021 and 2022, the authors recommend increased prevention and strengthening protocols to ensure injury frequency does not reach prepandemic levels. This strengthening, exercise, and mobility training has been studied widely in the sports medicine literature and will be imperative in ensuring lower extremity fracture prevention in athletes.9,17,28,29 More specifically, neuromuscular training, strengthening programs, and balance or proprioceptive-based injury prevention programs might be effective, especially in the prevention of ankle and foot injuries.22,34
While the drop-off due to the COVID-19 pandemic is apparent, the etiology of the prepandemic decrease in fractures is likely more complex and multifactorial. Efforts to redirect patients to outpatient clinics and orthopaedic urgent care centers may have contributed to the preexisting decline in fractures presenting to US EDs.25,32 This is supported by a 2022 study by Henry et al, 12 which reported a substantial increase in visits to orthopaedic urgent care centers between 2014 and 2019, especially for complaints related to the foot/ankle, lower leg, knee, and back. By monitoring the types of patients that benefit from an ED visit versus those effectively treated in an outpatient urgent care setting, delivery of timely patient care can be optimized. 12 Furthermore, given that 92.2% of patients in the present study were treated without admission, this suggests that the majority of basketball-related lower extremity fractures may be managed adequately on an outpatient basis. This finding is supported by numerous studies that report that foot and ankle injuries constitute a significant portion of primary care office visits each year as well as visits to outpatient foot and ankle clinics.1,6
When trends in lower extremity fractures were stratified by the specific injury location, significant decreases were observed for fractures of the ankle and foot. However, fractures involving the lower leg, knee, upper leg, and toe showed no significant trend over the study period. A study by Fletcher et al 10 noted that athletes with fractures of the lower leg presented more often to the ED, whereas minor fractures, such as of the hand, were addressed in an athletic training setting. This suggests that, although some fractures can be managed without an ED visit, more serious or complex fracture patterns likely still require workup at an ED. Furthermore, they emphasize that understanding the distribution of injuries presenting to EDs versus outpatient settings will ensure cost-effective care for sports-related injuries. 10 This is particularly important given that a study by Boyce and Quigley 4 reported that around 25% of sports injuries included were referred to outpatient clinics, whereas just 3% were admitted to the hospital. In this study, a slightly higher admission rate of 5.8% was identified across the study period. This discrepancy may be attributable to the variety of sports and body regions included in their analysis while this present study focused only on basketball-related lower extremity fractures.
Another important clinically relevant finding of this study was that lower extremity fractures from basketball occurred most commonly at the ankle (37.6%). Among the different mechanisms contributing to lower extremity fractures, a noncontact twisting/rolling motion was the most common mechanism, followed by injuries sustained from jumping and player-player contact. Moreover, 24.6% of the fractures sustained during jumping and 16.5% of fractures sustained from player-player contact involved a twisting motion. This further substantiates the prevalence of twisting-related lower extremity basketball fractures. Notably, the ankle was the most frequently affected body part across the top 3 primary mechanisms. This is consistent with a 2011 study by Pappas et al 24 that reported that 21.7% of pediatric basketball-related injuries were of the ankle. Similarly, a more recent 2022 study by Zynda et al 39 demonstrated a similarly high prevalence of ankle injuries among youth basketball players. The high frequency of fractures of the foot and ankle reinforces the importance of utilizing appropriate protective footwear with adequate support. This is supported by several studies that have similarly emphasized the vital role proper footwear plays in ensuring ankle stability given the complex biomechanical movements involved in basketball.2,18,19,27,38
The findings from this study have several clinical implications. The significant decrease in lower extremity fractures presenting to the ED suggests the importance of identifying the types of sports-related injuries that may be addressed through timely management in an outpatient setting. Although strains and minor fractures of the ankle and foot likely can be managed in the outpatient setting, more serious fractures involving long bones likely still require an ED visit and workup given the potential need for admission and subsequent fracture fixation. The distribution of basketball-related lower extremity fractures as well as the contributing mechanisms described in this study will be valuable in guiding cost-effective care for sports-related injuries. Finally, the high frequency of foot and ankle fractures supports previous studies that have emphasized the importance of protective footwear to provide adequate ankle stability and support.
Limitations
While the results of this study provide valuable insights into the frequency, mechanisms, and management of basketball-related lower extremity fractures, there are limitations to consider. The study relied on data from the NEISS, which may not capture all cases of basketball-related fractures. In addition, while the NEISS dataset serves as a representative sample of all EDs in the US, there remains the possibility of sampling error. Furthermore, the study only included fractures presenting to EDs, excluding cases managed in other healthcare settings, which may skew the injuries included in this analysis toward more serious injuries. Another important shortcoming is that, given the succinct nature of the narrative reports, the exact mechanism of injury could not be determined clearly for all entries. This resulted in about 25% of injuries being classified as “not specified,” which may have impacted the distribution of contributing mechanisms of injury. Finally, the narratives do not provide specific details regarding the fracture patterns or specific bony regions involved, making it difficult for the authors to assess management practices based on the fracture type/pattern.
Conclusion
The pediatric population and male basketball players constitute a high proportion of lower extremity fractures presenting to US EDs. Increasing utilization of outpatient clinics and orthopaedic urgent care centers may have contributed to the decline in basketball-related lower extremity fractures presenting to EDs in the US. In addition, while minor fractures of the ankle and foot can be treated in outpatient settings, more serious injuries may still require an ED evaluation and workup. The high prevalence of injuries arising from a noncontact twisting/rolling motion of the foot and ankle reinforces the importance of utilizing appropriate protective footwear and incorporating targeted injury prevention and strengthening programs.
Footnotes
The following authors report potential conflicts of interest: R.L.P has received educational support from Gotham Surgical Solutions and Devices. J.D.K. has received educational support from Paladin Technology Solutions and hospitality from Baxter Healthcare. D.P.T. has received educational support from Gotham Surgical Solutions and Devices and Arthrex.