
Abstract
Context:
Lateral extra-articular tenodesis (LET) and anterolateral ligament (ALL) reconstruction have been adopted by some surgeons as augmentations during anterior cruciate ligament reconstruction (ACLR) to improve anterolateral rotatory instability.
Objective:
The objective of this study was to assess the statistical robustness of outcomes reported in randomized controlled trials (RCTs) assessing the clinical significance of LET and ALL reconstruction in ACLR.
Methods:
PubMed, Embase, and MEDLINE were systematically searched. RCTs published January 1, 2010 to December 31, 2024 assessing LET and ALL reconstruction during ACLR were included. Fragility index (FI) or reverse FI (rFI) was calculated for each outcome, representing the number of event reversals required to alter statistical significance for significant and nonsignificant outcomes, respectively. The fragility quotient (FQ) was determined by dividing the FI or rFI by sample size.
Level of Evidence:
Level 1.
Results:
Of 112 RCTs screened for inclusion, 17 were included for analysis, resulting in 51 total outcomes. The median FI across the 51 outcomes was 4 [interquartile range (IQR), 2-7] with an associated median FQ of 0.031 (IQR, 0.014-0.049). Statistically significant outcomes were more fragile (median FI, 3.5; median FQ, 0.015) than statistically nonsignificant outcomes (median rFI, 5; median FQ, 0.038). In 60.8% of all outcomes (31 of 51), the number of patients lost to follow-up was greater than the outcome’s respective FI or rFI. In the 7 RCTs assessing LET, the median FQ was 0.015 (IQR, 0.012-0.042) across 23 outcomes. In the 10 RCTs assessing ALL, the median FQ was 0.035 (IQR, 0.019-0.051) across 28 outcomes. Graft failure, pivot shift, and Lachman/anterior laxity were the most common outcome categories reported, with median FQs of 0.017, 0.035, and 0.048, respectively.
Conclusion:
Outcomes reported in RCTs for LET and ALL reconstruction as augments of ACLR are statistically fragile, emphasizing the need for additional robust and adequately powered RCTs to better understand the impact of anterolateral augmentation on ACLR outcomes.
Keywords
Although anterior cruciate ligament reconstruction (ACLR) is increasingly being performed, 31 graft failure rates remain a major concern, occurring in up to 20% of patients.20,30 In recent years, there has been a heightened focus on rotational instability, with anterolateral rotatory laxity emerging as a potential contributing factor in up to 25% of ACLR failures.21,30,38 To address this, some surgeons have adopted lateral extra-articular tenodesis (LET) and anterolateral ligament (ALL) reconstruction as augments to ACLR to provide rotatory stability to the anterolateral complex.19,21,43 In a recent systematic review of randomized controlled trials (RCTs) by D’Ambrosi et al, 8 ACLR + ALL and ACLR + LET were both independently found to decrease graft failure rates significantly compared with ACLR alone without increasing complication rate. A systematic review by Bosco et al 2 similarly reported that ALL or LET procedures are independently associated with significantly improved pivot-shift tests, patient-reported outcome measures, and graft failure rates. In contrast, however, RCTs by Sonnery-Cottet et al 37 and Mogos et al 28 reported no significant difference in graft failure rates for ACLR + ALL compared with ACLR alone. Furthermore, RCTs by El-Azab et al, 10 Hamido et al, 15 and Rezansoff et al 34 report no significant differences in pivot shift for ACLR alone compared with ACLR with an anterolateral augment procedure. While recent RCTs have assessed the clinical significance of LET and ALL reconstruction in providing rotatory stability for ACLR,16,23,28,34 the conflicting findings in the literature highlight the uncertainty surrounding the clinical benefit of anterolateral augment procedures.
RCTs represent the highest level of evidence in guiding surgical decision-making for ACLR. 24 ACLR RCTs evaluating LET and ALL reconstruction ubiquitously utilize P values to convey the statistical significance of their results with considerable clinical implications. However, P values have received criticism as they do not convey effect size, indicate clinical significance, or take into account important study design elements such as attrition rate.1,24,41 Recent studies in the orthopaedic literature have highlighted a lack of statistical robustness in RCTs by delineating that statistically significant study outcomes can be reversed by altering just a few outcome events.4,5,7,22,26,27,32,44 -47 These analyses have utilized the fragility index (FI), which is a concept that was first introduced by Feinstein et al 12 in 1990 to supplement the P value’s limitations. The FI represents the “fragility” of an outcome and is calculated as the number of outcome event reversals required to reverse statistical significance. 12 The reverse fragility index (rFI) was similarly defined as the number of outcome event reversals required for a nonsignificant outcome to obtain statistical significance.3,18,25,35 The fragility quotient (FQ) takes sample size into consideration and is calculated as the FI divided by the sample size.14,33,42
The purpose of this study was to evaluate the statistical fragility of RCTs reporting on LET and ALL reconstruction as augments for ACLR. We hypothesized that statistical outcomes in RCTs assessing LET and ALL reconstruction for rotational stability would be fragile. We further hypothesized that statistically significant outcomes would demonstrate greater fragility than nonsignificant outcomes and that fragility would be identified for outcomes relating to graft failure, pivot shift testing, and anterior laxity.
Methods
Literature Review
The Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines were utilized for this systematic review (Figure 1). PubMed, Embase, and MEDLINE were queried for RCTs published from January 1, 2010, to December 31, 2024, using the following search terms: ((lateral extra-articular tenodesis OR LET) OR (anterolateral ligament OR ALL)) AND (anterior cruciate ligament OR ACL). RCTs written in English that reported dichotomous, categorical outcomes related to LET and ALL reconstruction in ACLR were included. Meta-analyses, case reports, papers without full-text availability, proposals, in vitro studies, and animal studies were excluded. Duplicates were removed after the initial review. Abstract screening and full-text review were performed by 2 independent authors (N.H.K. and A.R.L.) in parallel. Any disagreements or conflicts between the 2 primary screeners were resolved by a third, independent author (A.Y.) for ultimate inclusion or exclusion. Interrater reliability was assessed using Cohen’s kappa statistic. Bias assessment was conducted using the revised Cochrane Risk of Bias tool for evaluating bias in randomized trials by A.C. 40 A second independent author (A.Y.) subsequently performed bias assessment of all included RCTs using the revised Cochrane Risk of Bias tool blinded to the primary author’s assessment. A third independent author (C.G.) consolidated the risk of bias assessments from the 2 authors (A.Y. and A.C.) for all RCTs and resolved any discrepancies.
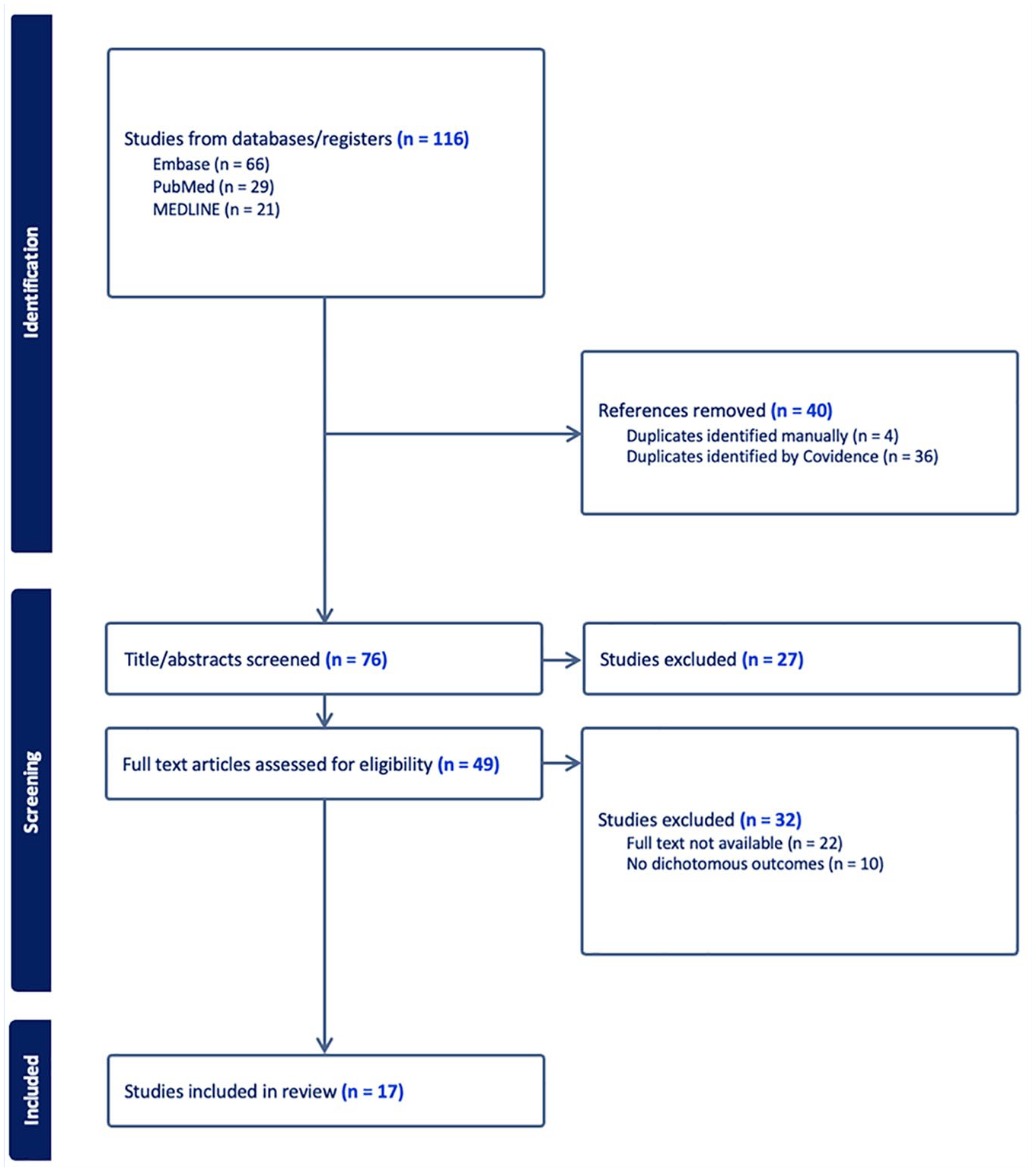
PRISMA flow diagram showing identification, screening, and inclusion, of eligible articles from PubMed, Embase, and Medline.
Data Extraction
Author name, publication year, study title, journal of publication, and intervention studied were extracted and included in Table 1. Study interventions, outcomes measured, number of patients per intervention with each outcome, number lost to follow-up, and reported P values were also extracted from each article. This study focused on the statistical significance of outcomes rather than evaluating the efficacy of interventions and, thus, did not qualify for PROSPERO international registration.
Characteristics of Included Studies a
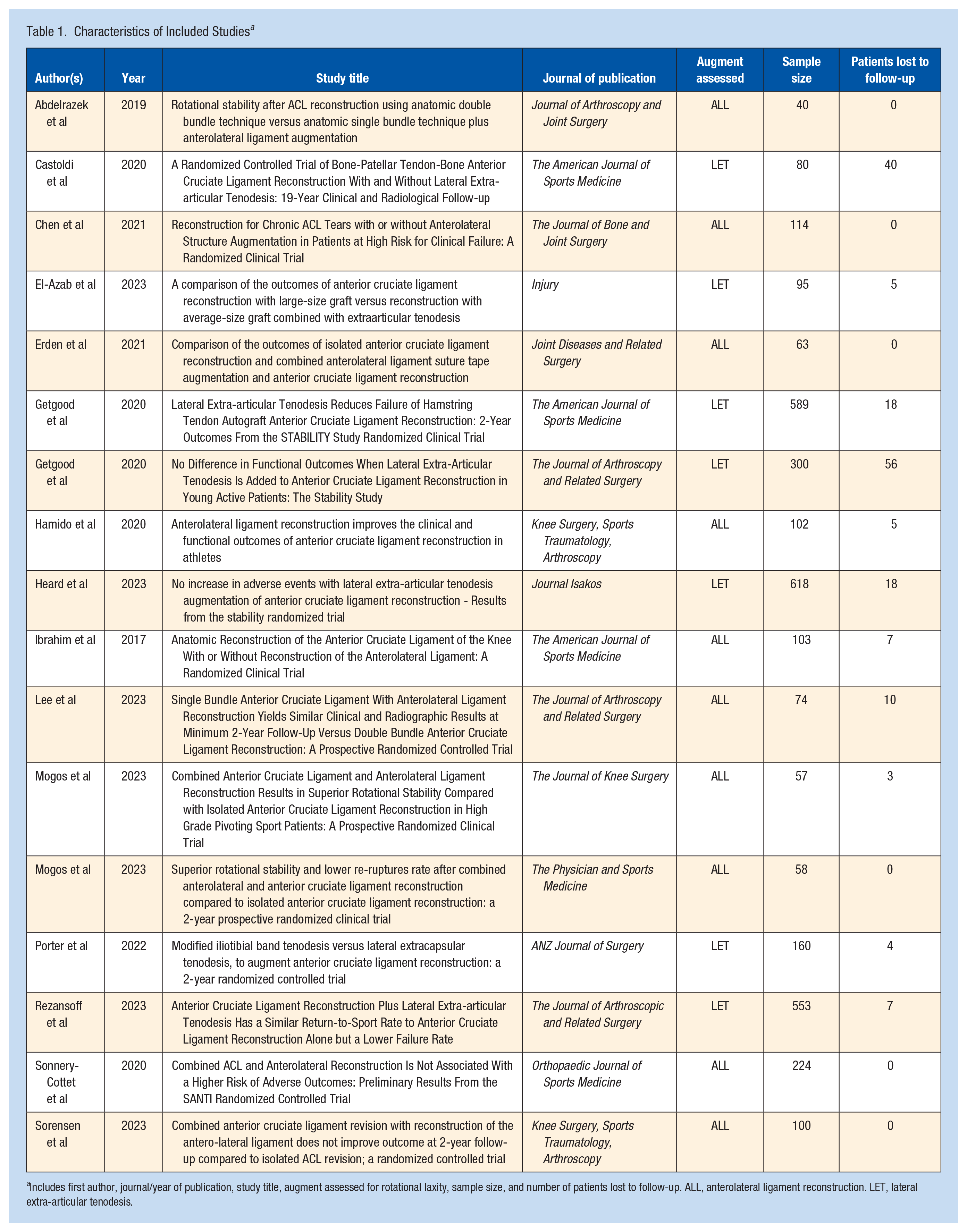
Includes first author, journal/year of publication, study title, augment assessed for rotational laxity, sample size, and number of patients lost to follow-up. ALL, anterolateral ligament reconstruction. LET, lateral extra-articular tenodesis.
Statistical Analysis
Reported P values for all included outcomes were verified using the 2-tailed Fisher exact test, and values less than 0.05 were considered significant. A 2 × 2 chi-square table was then generated for each included outcome. Iterative outcome event manipulations were performed until outcome significance was altered, either from significant to nonsignificant (FI), or from nonsignificant to significant (rFI). Figure 2 outlines the methodology utilized for significance reversal. The FQ was determined by dividing the FI or rFI by the respective sample size. Summary statistics are reported as median (IQR [interquartile range]). All outcomes were pooled to report the summary median and IQR for FI and FQ across all RCTs. Summary statistics were subsequently calculated for significant outcomes (FI/FQ) and nonsignificant outcomes (rFI/FQ). Pooled (significant and nonsignificant outcomes) fragility assessment was also performed, stratifying ALL and LET RCTs. Outcomes were then assigned to and analyzed in 6 subgroups: graft failure, positive pivot shift test, positive Lachman/anterior laxity, return to sport, progression to osteoarthritis, and other. The “other” subgroup included outcomes such as International Knee Documentation Committee (IKDC) improvement, surgical complications, contralateral rupture, and postoperative pain. The subgroup analysis by outcome type was performed by pooling significant and nonsignificant outcomes for the respective subgroup and analyzing them collectively.
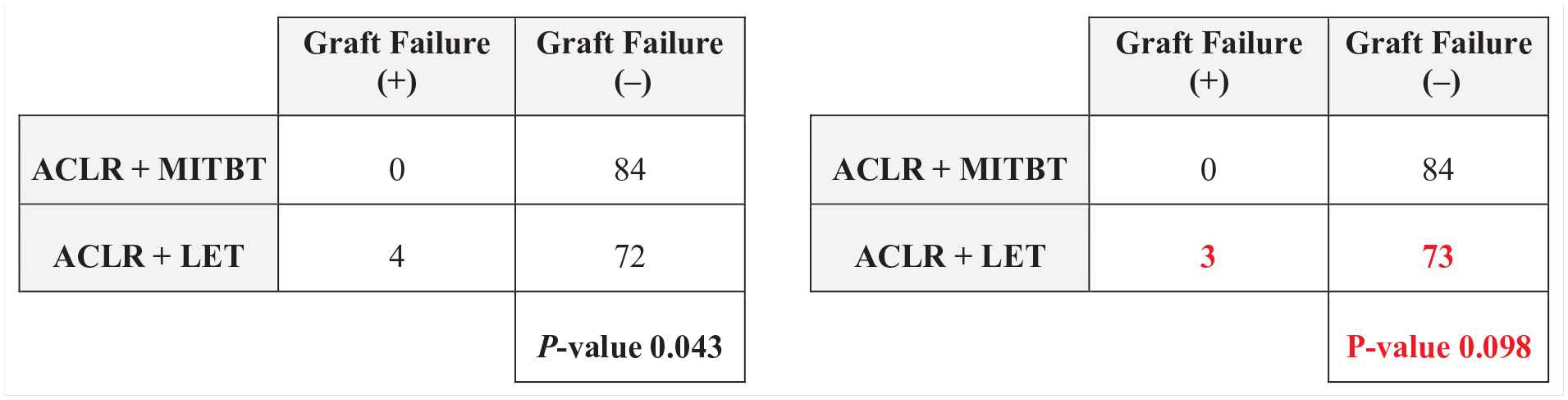
Demonstration of statistical significance reversal using a 2 × 2 contingency table with a resulting fragility index (FI) = 1.
Results
Of 116 RCTs screened for inclusion, 17 were ultimately included for analysis, comprising a total of 3330 patients. The interrater agreement for title and abstract screening was 89.5%. The interrater agreement for full-text review was 79.5%. In 7 of the included RCTs, LET was assessed as an augment for ACLR and, in 10 included RCTs, ALL reconstruction was assessed (Table 1).
The median FI across all 51 total outcomes was 4 (IQR 2-7), indicating that a median of 4 outcome event reversals may alter the significance of the RCTs assessing LET and ALL reconstruction as augments for ACLR (Table 2). The median FQ across all outcomes was 0.031 (IQR 0.014-0.049). Thus, an outcome event reversal in just 3.1% of patients may be sufficient to alter outcome significance across the 17 RCTs. For 14 outcomes denoted in the RCTs as primary outcomes, the median FI was 4.5 (IQR 2.25-6.75) with an associated FQ of 0.018 (IQR 0.015-0.035). In 60.8% of all outcomes (31/51), the number of patients lost to follow-up was greater than the respective outcome’s FI.
Fragility Data Based on Trial and Outcome Characteristics
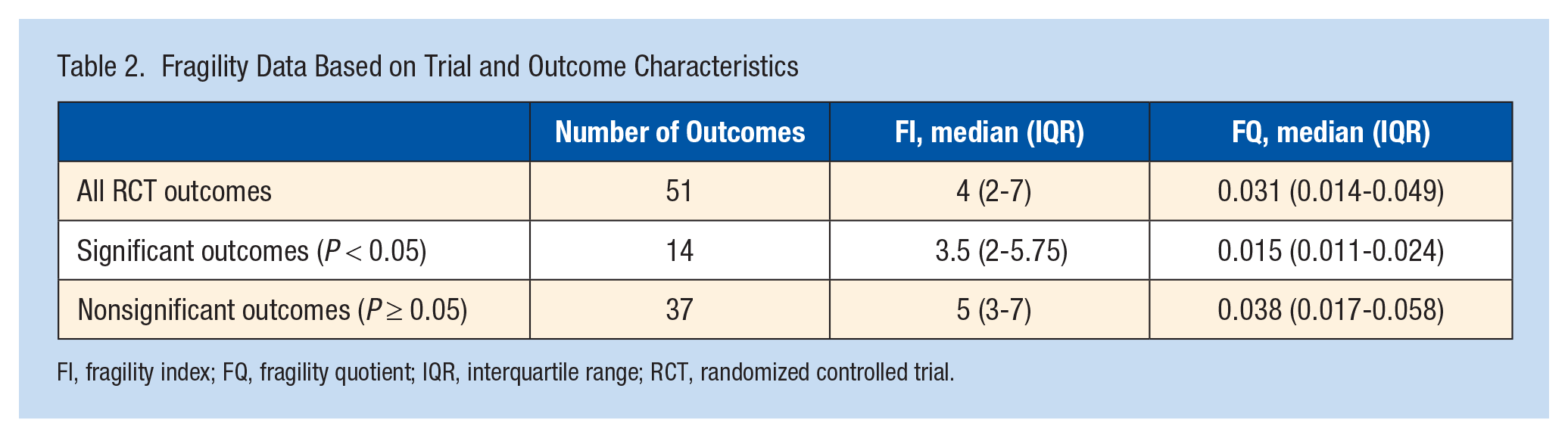
FI, fragility index; FQ, fragility quotient; IQR, interquartile range; RCT, randomized controlled trial.
Statistically significant outcomes demonstrated greater fragility than nonsignificant outcomes. The median FI for statistically significant outcomes was 3.5 (IQR 2-5.75) and the associated median FQ was 0.015 (IQR 0.011-0.024). Thus, an outcome event reversal in just 1.5% of patients may lead to a reversal of the significance of outcomes. There were 9 statistically significant outcomes in favor of an ACLR + an anterolateral augment compared with ACLR alone, with a median FQ of 0.17, suggesting that these outcomes may be reversed by changes in the outcomes of less than 2% of patients. There were 3 significant outcomes which favored ACLR alone compared with ACLR + LET, with 2 being related to surgical complications and 1 assessing osteoarthritis. These outcomes were particularly fragile, however, with a median FQ of 0.006. The median rFI for outcomes that were not statistically significant was 5 (IQR 3-7) with an associated median FQ of 0.038 (IQR 0.017-0.058).
In the 7 RCTs assessing LET as an augment for ACLR, the median FI was 6 (IQR 3.5-8.5) across 23 outcomes (Table 3). The associated median FQ was 0.015 (IQR 0.012-0.042). For the 10 RCTs assessing ALL reconstruction as an augment for ACLR, the median FI was 3.5 (IQR 2-5) across 28 outcomes. The associated median FQ was 0.035 (IQR 0.019-0.051). These findings indicate that an outcome event reversal in 1.5% of patients in the LET RCTs and in 3.5% of patients in the ALL reconstruction RCTs for augmenting ACLR may be sufficient to alter outcome significance.
Subgroup Analysis Based on Rotational Laxity Augment Type for Anterior Cruciate Ligament Reconstruction
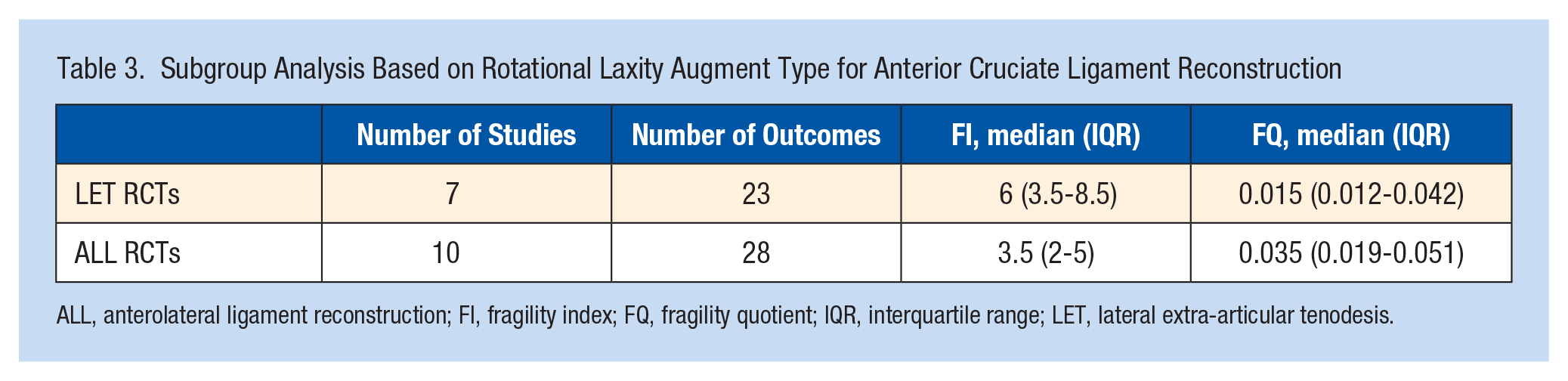
ALL, anterolateral ligament reconstruction; FI, fragility index; FQ, fragility quotient; IQR, interquartile range; LET, lateral extra-articular tenodesis.
Across 11 graft failure outcomes, the median FI was 4 (IQR 2-6.5) with an associated FQ of 0.017 (IQR 0.013-0.029) (Table 4). For the 11 pivot shift outcomes, the median FI was 3 (IQR 2-4) with an associated FQ of 0.035 (IQR 0.019-0.048). In 9 outcomes relating to anterior laxity, the median FI was 4 (IQR 3-5) with an associated FQ of 0.048 (IQR 0.013-0.033). For 4 outcomes relating to return to sport and 3 outcomes relating to progression to osteoarthritis, the median FI’s were 7.5 and 6, respectively.
Subgroup Analysis Based on Outcome Category
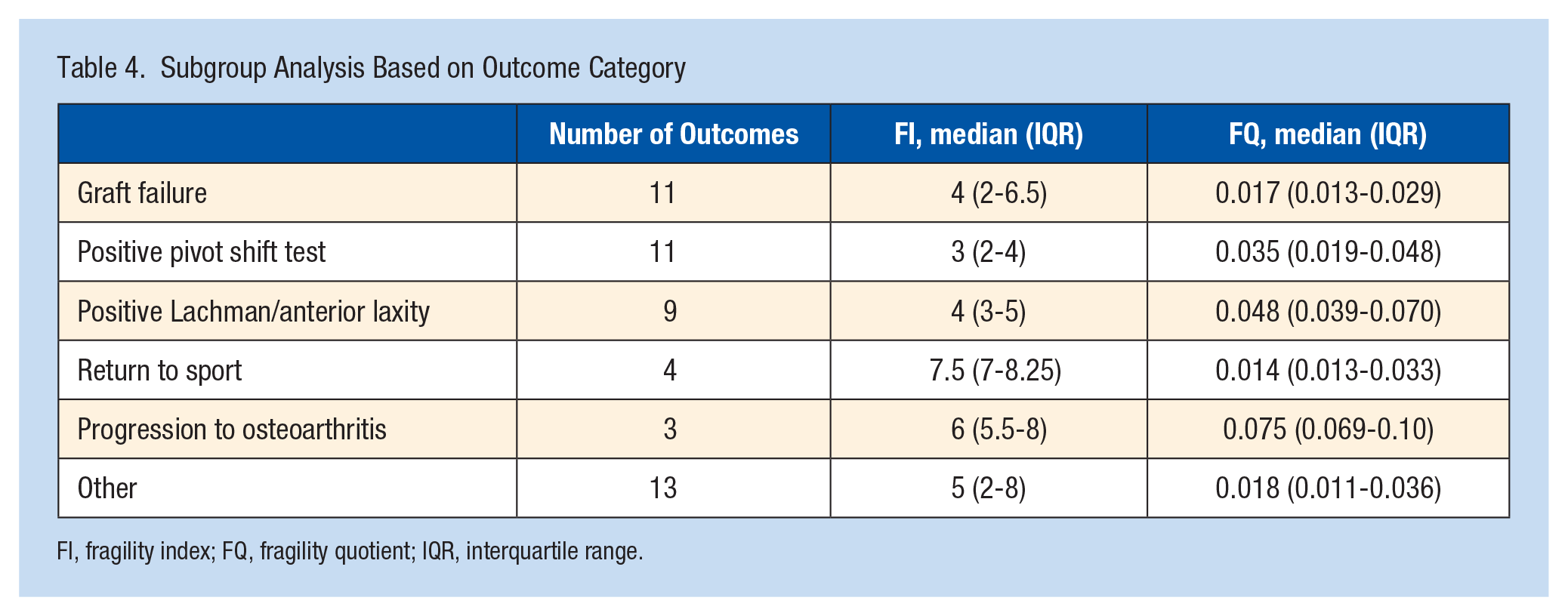
FI, fragility index; FQ, fragility quotient; IQR, interquartile range.
Bias assessment of the RCTs performed with the revised Cochrane risk-of-bias tool revealed that only 3 of 17 included studies demonstrated “some concerns” for bias. The remainder of the studies were found to have low risk of bias (Table 5). Bias was most frequently identified in domains concerning missing outcome data.
Cochrane Risk of Bias Assessment for Evaluating Randomized Controlled Trials
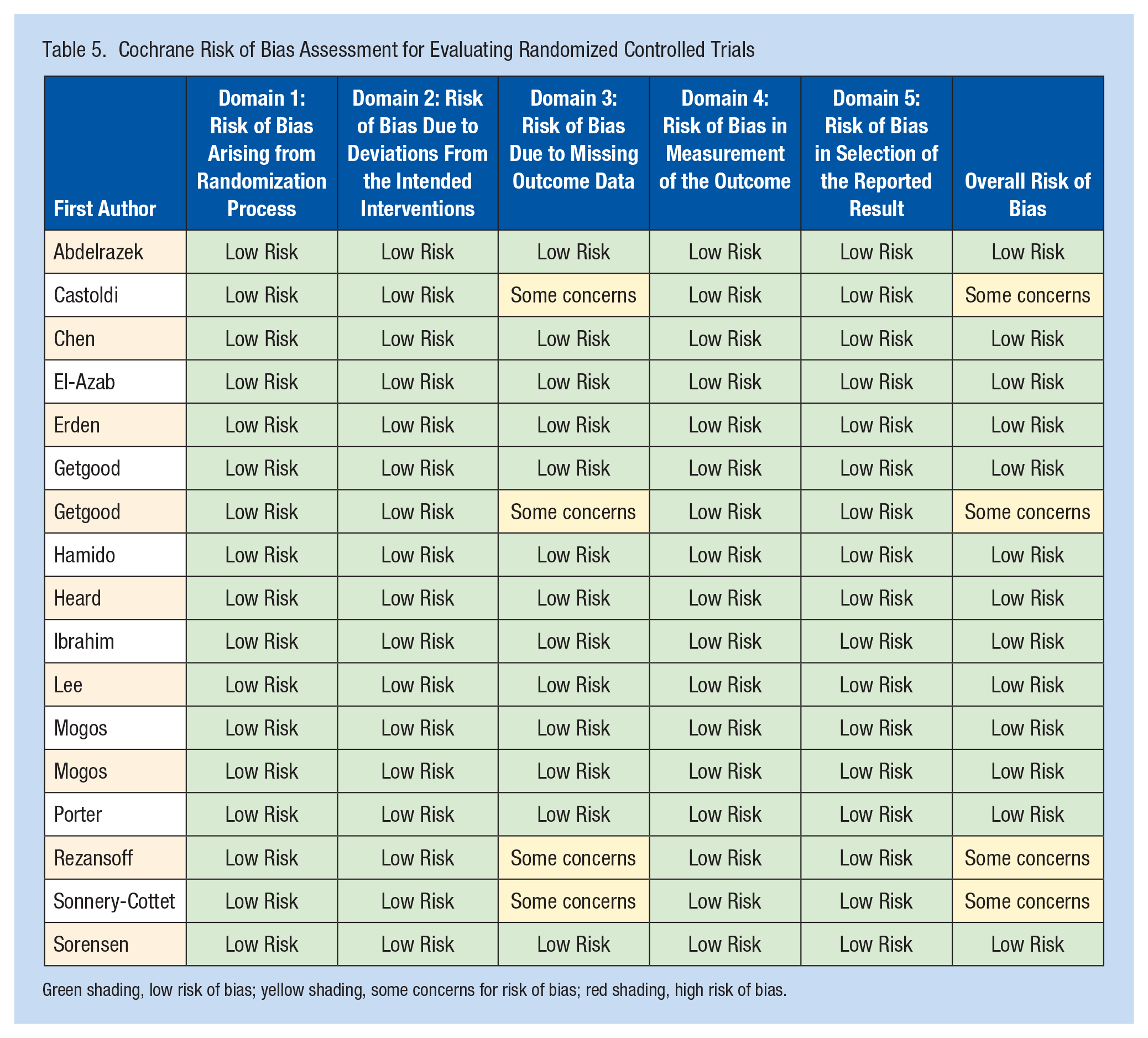
Green shading, low risk of bias; yellow shading, some concerns for risk of bias; red shading, high risk of bias.
Discussion
This study utilized the FI, rFI, and FQ metrics to assess the robustness of outcomes reported in RCTs evaluating LET and ALL reconstruction as augments for rotatory instability in ACLR. We systematically reviewed the PubMed, Embase, and Medline databases and identified 17 RCTs for inclusion that reported 51 total outcomes. The median FI for 14 significant outcomes was just 3.5 and the median rFI for 37 nonsignificant outcomes was 5. Furthermore, we found that event reversals in just 1.5% of patients could reverse the statistical significance of outcomes studied in RCTs assessing LET for ACLR. Similarly, event reversals in 3.5% of patients could reverse the statistical significance of outcomes from RCTs investigating ALL reconstruction. Finally, in 60.8% of all outcomes studied, the number of patients lost to follow-up exceeded the respective outcome’s FI or rFI.
Trials investigating LET and ALL in ACLR have led to an increase in their popularity over the last several years. However, our assessment of RCTs that investigate LET and ALL reconstruction as augments for ACLR indicates that the significance of outcomes studied may be lost if there are outcome reversals in less than 4% of patient outcome events. This highlights the potential for type-1 alpha errors in these studies, wherein the null hypothesis is wrongfully rejected with 1 treatment arm falsely being touted as clinically superior. The studies included in this systematic review reported several significant outcomes in favor of anterolateral augments in ACLR. In particular, improvements in graft failure rate and pivot shift testing were frequently reported. For example, Chen et al 6 reported a failure rate of 20.4% in the ACLR alone group compared with 3.3% in the ACLR and ALL reconstruction group. However, this outcome hinges on just 3 patient outcome events and would be reversed by outcome event reversals in less than 3% of RCT patients (FQ = 0.26). Furthermore, Mogos et al 29 evaluated ACLR and ALL reconstruction versus ACLR alone and reported a significant difference in positive pivot shift tests at 1 year postoperative follow-up in favor of ACLR+ALL (2/32 for ACLR + ALL versus 9/25 for ACLR alone). However, this finding had an FI of 2, which was found to be less than the number of patients lost to follow-up in the RCT. Considering that the median FQ across the 14 statistically significant findings was 0.015, these significant findings should be interpreted with caution, as outcome event reversals in just 1.5% of patients could reverse statistical significance.
The included studies reported 37 outcomes as not statistically significant. As Khan et al 18 highlight, a lack in statistical significance in the form of P values may not correlate with the real treatment effects of interventions. Furthermore, the group recommends that P values of study outcomes that are between 0.05 and 0.10 should be assessed thoroughly to ensure that potentially significant differences between interventions are not missed. 18 This allows for P values to be viewed in less of a dichotomous manner and for all aspects of a reported outcome to be taken into consideration when guiding clinical decision-making. Recent fragility analyses have employed the rFI to evaluate outcomes lacking statistical significance in orthopaedic RCTs. In a 2024 study, Mazzucco et al 25 employed the rFI to assess mortality endpoints for hemiarthroplasty for hip fractures and found median rFIs of 3, 6, and 7 at the 30-day, 90-day, and latest follow-up points. Furthermore, Shi et al 36 used the rFI to assess survivorship of computer-navigated versus conventional total knee arthroplasty and found a median rFI of 4. Importantly, the group recommends that when interpreting results lacking statistical significance, several factors should be considered beyond just the reported P value, including the rFI, study power, and the effect size.
Recent systematic reviews by D’Ambrosi et al 8 and Bosco et al 2 have demonstrated significantly improved graft failure rates,2,8 pivot shift tests, 2 and patient-reported outcomes measures 2 favoring anterolateral augments for ACLR. However, several RCTs have also demonstrated no significant differences between ACLR alone and ACLR with an anterolateral augment. El-Azab et al, 10 for example, found no significant difference in graft failure with LET. Similarly, Erden et al, 11 Ibrahim et al, 17 and Sorensen et al 39 showed no significant differences in pivot shift for ALL augment to ACLR. In addition, no significant differences in Lachman tests were identified by Mogos et al, 28 Lee et al, 23 Hamido et al, 15 and Erden et al 11 for ALL + ACLR compared with ACLR. In our study, we identified an rFI of 5 for these nonsignificant outcomes relating to ACLR alone compared with ACLR with an anterolateral complex augment. This statistical fragility identified for nonsignificant outcomes suggests the possibility of type 2 errors in which a lack of power or an inadequate sample size may lead to statistically significant differences being missed. Thus, appropriately powered comparative trials that perform pre hoc power analysis are needed in order to reliably assess the clinical efficacy of LET and ALL reconstruction anterolateral augments for ACLR.
Outcomes in studies evaluating LET were found to hinge on outcome events in just 1.5% of trial patients, whereas outcomes from studies evaluating ALL reconstruction hinge on 3.5% of trial patients. The FQ metric serves as a valuable tool for comparing statistical fragility across RCTs with different sample sizes. The FQs identified in this study highlight the alarming level of statistical fragility in LET and ALL reconstruction RCTs. Outcome event reversals in less than 4% of patients may be sufficient to alter the statistical significance of reported outcomes, which undoubtedly raises concern over their robustness. These findings also highlight the value in standardized reporting of the FQ metric along with the FI and rFI to ensure statistical fragility of endpoints from RCTs with different sample sizes may be compared effectively.
Statistical fragility by outcome type revealed that outcomes related to return to sport, graft failure, and pivot shift testing were the most fragile (FQ = 0.014, 0.017, and 0.035, respectively). In a systematic review, Feng et al 13 reported that ACLR and LET results in a significant reduction in pivot shift and graft failure rates. In a systematic review by Lai et al, 21 patients who underwent ACLR and ALL had significantly better knee stability based on pivot shift testing as well as reduced anterior laxity and a lower incidence of graft failure. However, given that these systematic reviews are based on fragile findings from RCTs, their conclusions may be called into question.
Recent fragility analyses in the orthopaedic surgery literature have assessed the statistical fragility of outcomes relating to ACLR. Lawrence et al 22 reported a median FQ of 0.082 across 55 total outcomes in RCTs comparing bone-patellar tendon-bone versus hamstring autografts. In an analysis of RCTs comparing autograft versus allograft for ACLR, Megafu et al 26 identified a median FQ of 0.041 for statistically significant outcomes. Furthermore, Ehlers et al 9 reported a mean FQ of 0.050 for outcomes in comparative studies on single-bundle versus double-bundle autografts for ACLR. Ruelos et al utilized the reverse FQ to evaluate differences lacking statistical significance in failure rates for hamstring and bone-patellar tendon-bone autografts and found a median reverse FQ of 0.04. 35 The FQs of 0.31 across our outcomes and 0.15 for significant outcomes and the reverse FQ of 0.038 for nonsignificant outcomes in our study highlight that LET and ALL reconstruction augments for ACLR are particularly fragile compared with the broader ACLR fragility literature. Thus, additional adequately powered RCTs with power analysis may be required to further elucidate whether ALLs have a clinically meaningful benefit for patients undergoing ACLR.
Limitations
There are important limitations to consider with the present study. First, the FI and FQ are only able to be calculated for categorical, dichotomous outcomes. Some RCTs screened in this systematic review could not be ultimately included due to their failure to meet these criteria. The continuous FI has recently emerged as a potential metric that may be used to assess the statistical fragility of continuous outcomes. However, it is important to consider that the continuous FI also has limitations as it was only recently introduced, and the metric relies on the reported outcome having a mean and standard deviation reported for both intervention arms. Future studies may consider incorporating continuous fragility analyses as the metric undergoes further validation. Second, LET and ALL reconstruction augments for ACLR is a narrow topic of investigation which limited the number of RCT outcomes able to be analyzed. Finally, it is important to note that there have not been any threshold values for the FI, rFI, or FQ established for ACLR RCTs to accurately assess the reliability of the data. Threshold FI, rFI, or FQ values would serve as a benchmark for clinicians to effectively interpret the robustness of reported study findings in orthopaedic comparative trials. In addition to statistical fragility metrics, consistent reporting of clinically significant threshold measures such as the minimal clinically important difference, substantial clinical benefit, and patient acceptable symptom state may allow for study findings to be better correlated with clinically meaningful differences in reported outcome measures. 44
Conclusion
Outcomes reported in RCTs evaluating LET and ALL reconstruction as augments for rotatory instability in ACLR are statistically fragile. These findings highlight the need for additional adequately powered RCTs to better understand the effect of anterolateral augmentation on ACLR outcomes. We recommend combined reporting of P values with the FI, rFI, and FQ to aid in interpreting clinical findings of ACLR RCTs.
Footnotes
The following authors declared potential conflicts of interest: R.L.P. has received educational support from Gotham Surgical Solutions and Devices. M.J.A. has received consulting fees from DePuy Synthes, educational support from SUVON SURGICAL, and hospitality from Bodycad USA Corp. B.R.W. has received educational support from Arthrex, Vericel, and Peerless Surgical, and consulting fees from Vericel, Medical Device Business Services, and DePuy Synthes. X.L. has received consulting fees from FH Orthopedics.