
Abstract
Context:
The effectiveness and optimal exercise-based physical therapy interventions for sport-related concussion (SRC) remain controversial, and a systematic synthesis of the evidence is lacking.
Objective:
To conduct a network meta-analysis (NMA) of randomized controlled trials (RCTs) evaluating exercise-based physical therapy interventions for SRC recovery and provide best-practice recommendations.
Data Sources:
MEDLINE (PubMed), Web of Science, and Cochrane databases were searched from inception through December 2024.
Study Selection:
RCTs assessing exercise-based physical therapy interventions for SRC that reported symptom or recovery outcomes were included. Animal studies, observational studies, and studies with nonextractable data were excluded. All records were screened independently and blindly by 2 reviewers.
Study Design:
NMA using a random-effects model. Study quality was assessed with the Cochrane Risk of Bias tool (PROSPERO registration: CRD420251011941).
Level of Evidence:
Level 1.
Data Extraction:
Two reviewers independently extracted data. Outcomes included clinical recovery time and symptom- or scale-based measures.
Results:
A total of 20 RCTs with 1320 participants (age, 12 to 60 years; 57% female) reporting acute or persistent SRC were included; details on sport types and levels were limited. Interventions comprised subthreshold aerobic exercise protocol (SAEP), usual care exercise protocol (UCEP), multidisciplinary interventions, stretching, strict rest, vestibular rehabilitation therapy (VRT), and combined VRT plus SAEP. Multidisciplinary interventions achieved the greatest improvements (standardized mean difference [SMD] = –2.06; P = 0.002), followed by combined VRT plus SAEP and VRT alone. Subgroup analyses showed similar patterns: multidisciplinary interventions were most effective in participants <30 years old (SMD = –2.42) and in patients with persistent symptoms (SMD = –2.999). Risk of bias was low in 13 studies, moderate in 3, and high in 4.
Conclusion:
Multidisciplinary interventions and the combination of VBT and SAEP are the most effective treatments for SRC recovery, particularly for patients with persistent symptoms and for those <30 years.
Sport-related concussion (SRC) is a mild traumatic brain injury caused by external forces in sport. 33 In the United States, SRC accounts for an estimated 2.2 million emergency department visits annually. 23 The 2022 International Consensus Statement on Concussion in Sport describes SRC as a transient disturbance in brain function, usually without structural injury on conventional neuroimaging. 36 Although symptoms are often mild and self-limited, some patients develop persistent postconcussion symptoms (PPCS) beyond 4 weeks, including headache, dizziness, and cognitive or mood disturbances, with neurocognitive impairment in more severe cases.22,25 In adolescents, SRC may cause memory and executive function deficits that persist for months compared with noninjured controls. 9
Given the heterogeneity of SRC presentations and risk of PPCS, contemporary guidelines emphasize early medical assessment and individualized rehabilitation. 41 Prompt evaluation and appropriate guidance appear to shorten recovery and reduce the likelihood of chronic symptoms. In contrast to earlier recommendations of strict physical and cognitive rest, prolonged inactivity may worsen symptoms and delay recovery. 26 Current practice favors relative rest during the first 24 to 48 hours, followed by a gradual, symptom-limited resumption of daily, academic, and sport activities. 36 Within this framework, nonpharmacologic interventions such as subthreshold aerobic exercise, behavioral management (e.g., sleep and stress regulation), vestibular rehabilitation, and multidisciplinary interventions have emerged as safe and effective options. 27
Hutchison et al 11 developed subthreshold aerobic exercise protocol (SAEP) based on the Buffalo Concussion Treadmill Test to prescribe safe, symptom-limited aerobic training, supported by feasibility and efficacy work from Micay et al, 34 and Leddy et al.27,28 In the usual care exercise protocol (UCEP), patients are advised to observe brief relative rest followed by a gradual return to physical and cognitive activities, often without a structured aerobic prescription. 36 Vestibular rehabilitation therapy (VRT) can reduce dizziness and improve balance, with reports of accelerated recovery and better quality of life in youth with SRC and PPCS.35,47 Multidisciplinary programs that target dominant symptom domains and integrate physical, vestibular, and psychological care also reduce symptom burden and improve function.2,41
Systematic reviews and meta-analyses suggest that SAEP reduces concussion symptom severity and that individualized multidisciplinary interventions may expedite recovery, particularly in PPCS.37,39 However, the comparative effectiveness of different exercise-based physical therapy approaches remains uncertain, and clinicians lack clear guidance on which strategies are most beneficial. To address this gap, we will conduct a network meta-analysis (NMA) of randomized controlled trials (RCTs) evaluating exercise-based physical therapy interventions for SRC across age groups and symptom durations, enabling comparisons among SAEP, UCEP, VRT, and other modalities. We hypothesize that exercise-based interventions differ in therapeutic efficacy and that multidisciplinary interventions will rank among the most effective strategies for optimizing SRC recovery.
Methods
Protocol and Registration
The NMA was conducted in accordance with the PRISMA-NMA guidelines and the Cochrane Handbook for Systematic Reviews of Interventions. 12 The study protocol has been registered with PROSPERO (registration no.: CRD420251011941).
Search Strategy and Study Selection
We conducted a systematic search of MEDLINE (PubMed), Web of Science, and the Cochrane Library to identify RCTs assessing exercise-based physical therapy interventions for recovery from acute or persistent SRC. Only RCTs were included to ensure the highest level of evidence. The literature search encompassed all available studies published in the databases from their inception through December 2024 and was supplemented by a manual review of references from relevant systematic reviews and meta-analyses. Search terms included “brain concussion,” “sport-related concussion,” “mild traumatic brain injury,” and “post-concussion syndrome.” The full search strategy is presented in Supplementary Table S1 (available in the online version of this article).
Two independent reviewers screened titles and abstracts, followed by full-text assessment conducted independently and blindly based on predefined eligibility criteria. Disagreements were resolved by discussion or consultation with a third reviewer.
Eligibility Criteria
Studies were included if they met the following criteria: (1) designed as an RCT; (2) enrolled participants of whom >50% sustained SRC; (3) investigated the effects of physical therapy interventions (e.g., VRT, SAEP) on SRC recovery; (4) reported primary outcomes such as the Post-Concussion Symptom Inventory (PCSI), Rivermead Post-Concussion Symptoms Questionnaire (RPQ), or clinical recovery duration.
Exclusion criteria were as follows: (1) animal studies, cross-sectional or case-control studies, conference abstracts, and study protocols; (2) studies that did not include any participants with SRC; (3) studies not involving physical therapy interventions; and (4) studies lacking extractable data for analysis.
Quality Assessment and Data Extraction
The risk of bias in included studies was assessed using the Cochrane Risk of Bias tool, covering 7 domains: randomization method, blinding of participants and personnel, blinding of outcome assessors, allocation concealment, completeness of outcome data, selective reporting, and other potential biases.
Two independent reviewers extracted data from eligible studies. Any discrepancies were resolved through discussion or consultation with a third reviewer. Extracted data included the first author, publication year, sample size, mean participant age, sex distribution, time since injury at study inclusion, intervention details, and outcome measures.
Data Items
The outcomes of interest included: clinical recovery duration (CRD) (time to return to baseline or full activity) and symptom severity, assessed using validated scales: (1) PCSI, (2) RPQ, (3) Vestibular/Ocular Motor Screening (VOMS), (4) Sports Concussion Assessment Tool 3 (SCAT3), (5) Dizziness Handicap Inventory (DHI), and (6) Short-Form Health Questionnaire (SF-36).
Statistical Analysis
Data were analyzed using RStudio with relevant statistical packages, including netmeta, ggplot2, bayesmeta, and forestplot. Given the variability in outcome measures across studies, standardized mean differences (SMDs) were used to estimate effect sizes. The surface under the cumulative ranking curve (SUCRA) was employed to rank intervention effectiveness, with higher values indicating superior outcomes.
A network evidence diagram was constructed to visualize direct and indirect treatment comparisons. Nodes represent interventions, and edges indicate direct comparisons, with line thickness proportional to comparison frequency.
To assess the consistency of NMA results, node-splitting analysis was performed to evaluate local inconsistency, comparing direct and indirect estimates for specific comparisons. A significant difference between direct and indirect estimates indicated local inconsistency.
For studies reporting only medians and interquartile ranges, means and standard deviations were estimated using the method proposed by Luo et al. 30 This approach accounts for small sample sizes and non-normal distributions, enhancing estimation precision. All hypothesis tests were 2-tailed, with a significance level of α = 0.05.
Results
Study Selection and Characteristics
Following the search strategy, an initial 3207 studies were identified across the 3 databases (Supplementary Figure S1, available online). After removing 1479 duplicates, 1047 studies were excluded based on title and abstract screening (including reviews, animal studies, and protocols). A total of 402 studies underwent full-text review, resulting in the final inclusion of 20 RCTs.5 -7,11,16,19-21,24,27,28,31,32,34,38,40,43,45,46,49 These studies involved 1431 patients, with 1320 patients included in the final analysis after accounting for loss to follow-up and other exclusions. The participants ranged in age from 6 to 60 years, with 57% being female. The included interventions consisted primarily of: SAEP (n = 11); UCEP (n = 10); multidisciplinary interventions (n = 5); stretching programs (n = 5); strict rest (n = 5); VRT (n = 3); VRT combined with SAEP (n = 2). Notably, a study by Willer et al 49 was included 3 times, as it had 2 control groups (stretching and strict rest). The frequency of exercise interventions varied significantly across studies, ranging from 1 to 7 sessions per week, with an average session duration of 20 minutes. Although we aimed to include studies in which >50% of participants had SRC, the limited number of such studies necessitated the inclusion of 5 studies with SRC proportions ranging from 18% to 30% to ensure the stability of the network plot.6,19,32,38,45 The detailed characteristics of the included studies are summarized in Table 1.
Basic characteristics of the included literature
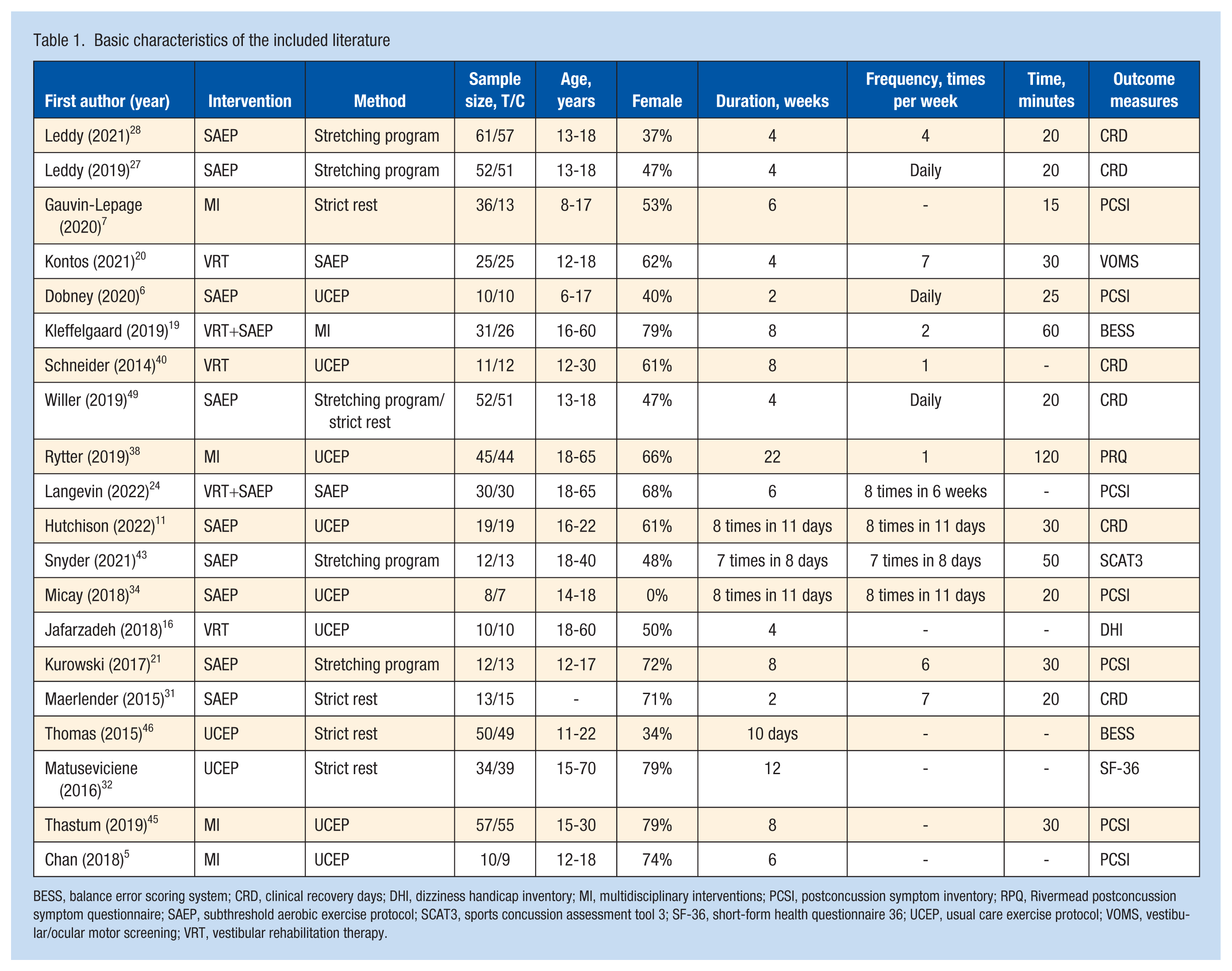
BESS, balance error scoring system; CRD, clinical recovery days; DHI, dizziness handicap inventory; MI, multidisciplinary interventions; PCSI, postconcussion symptom inventory; RPQ, Rivermead postconcussion symptom questionnaire; SAEP, subthreshold aerobic exercise protocol; SCAT3, sports concussion assessment tool 3; SF-36, short-form health questionnaire 36; UCEP, usual care exercise protocol; VOMS, vestibular/ocular motor screening; VRT, vestibular rehabilitation therapy.
Risk of Bias
Among the 20 RCTs included in this meta-analysis, 4 had a high risk of bias, 3 had some concerns of bias, and 13 had a low risk of bias. The detailed risk of bias assessment is presented in Supplementary Table S2 (available online). A funnel plot analysis (Supplementary Figure S2, available online) suggested a low likelihood of publication bias.
Efficacy of Different Postconcussion Management Strategies
This study evaluated the effectiveness of 6 distinct postconcussion management strategies, including 5 exercise-based physical interventions and standard care, compared against strict rest (F) (Figure 1). Table 2 and Figure 2a present SMDs with 95% CIs, P values, and P score values for each intervention.
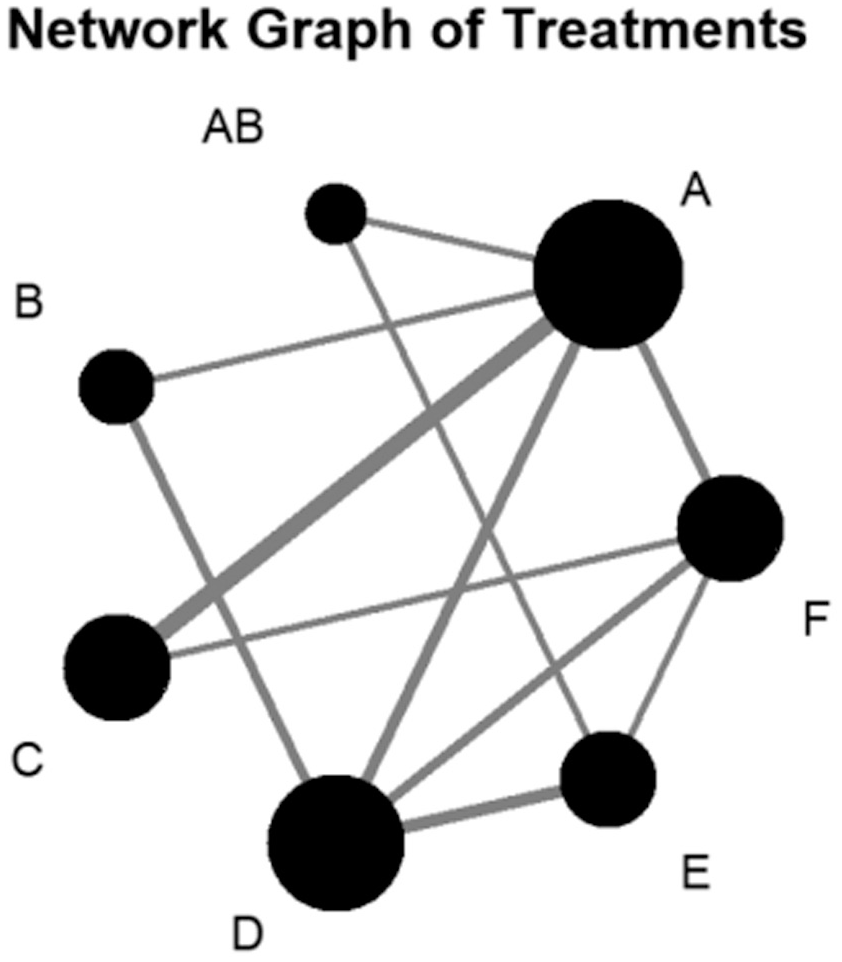
Network plots: A, SAEP; B, VRT; C, stretching scheme; D, UCEP; E, multidisciplinary interventions; and F, strict rest. Each node represents a specific type of exercise intervention. Edge thickness corresponds to the number of direct comparisons between 2 interventions. Node size reflects the total sample size per intervention. SAEP, subthreshold aerobic exercise protocol; UCEP, usual care exercise protocol; VRT, vestibular rehabilitation therapy.
Treatment estimate
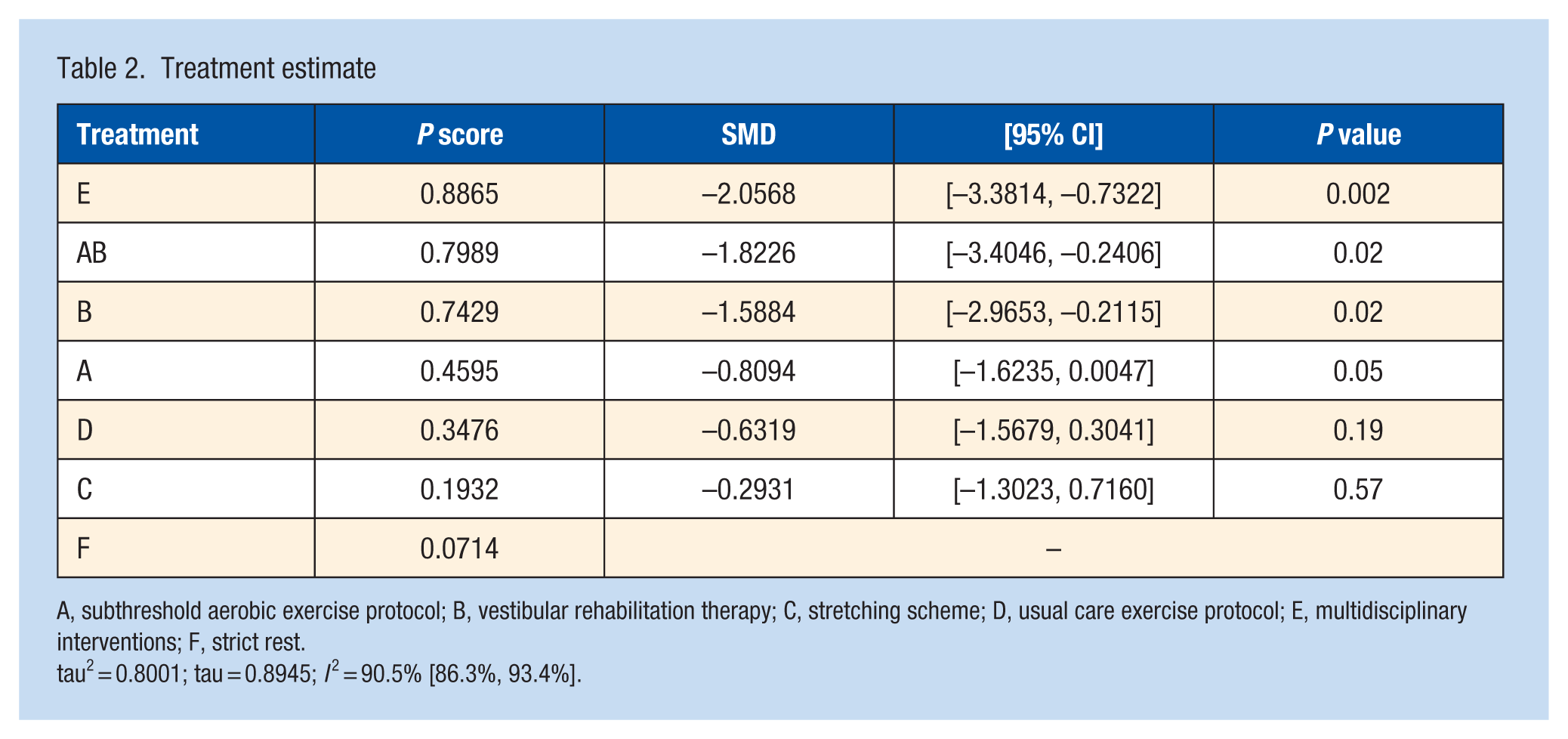
A, subthreshold aerobic exercise protocol; B, vestibular rehabilitation therapy; C, stretching scheme; D, usual care exercise protocol; E, multidisciplinary interventions; F, strict rest.
tau2 = 0.8001; tau = 0.8945; I 2 = 90.5% [86.3%, 93.4%].
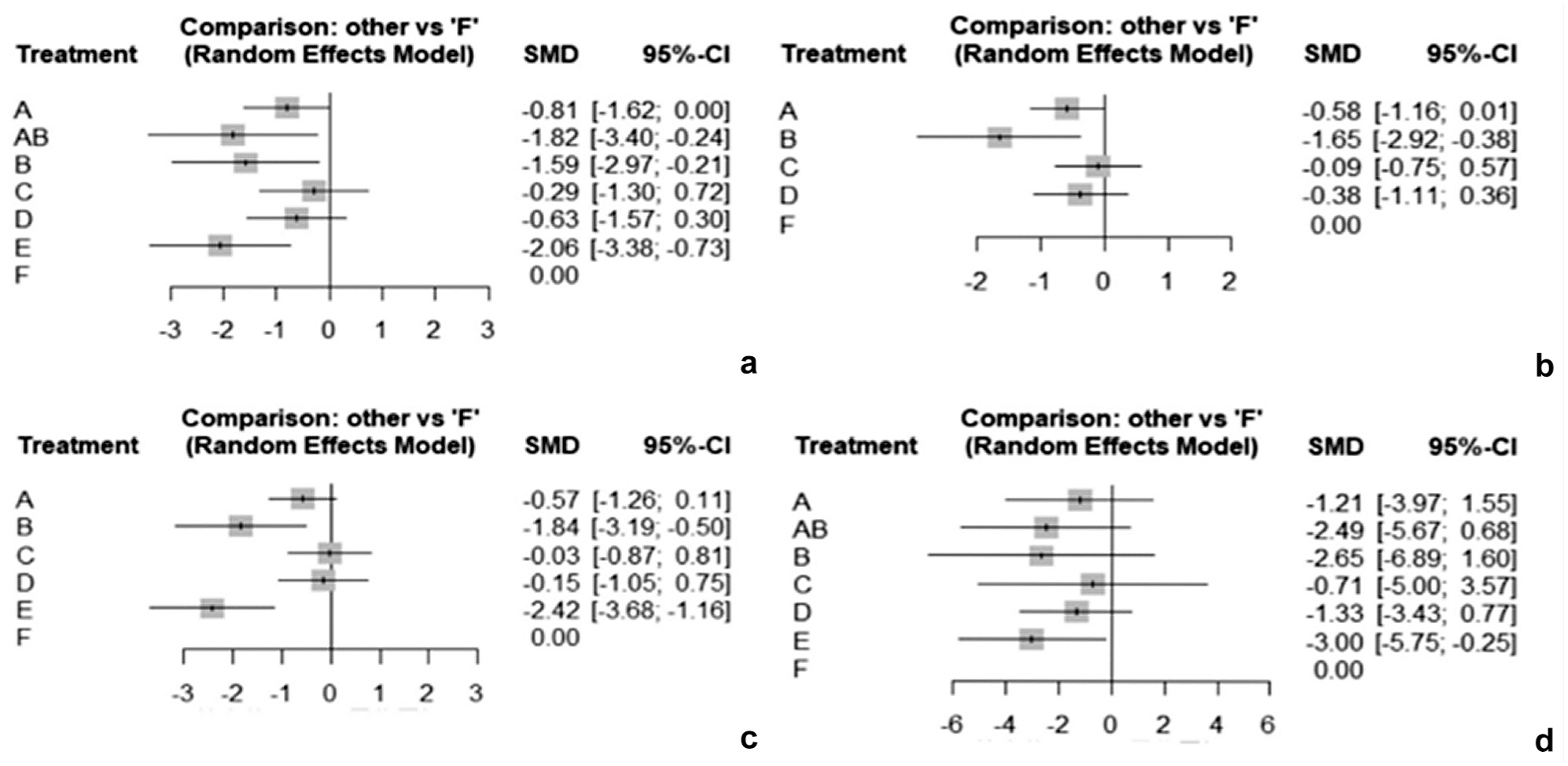
Summary of Forest plots. (a) Total forest map. (b) Included patients with acute SRC. (c) Included patients <30 years old with SRC. (d) Included patients with PPCS. Intervention types as in Figure 1. SMD, standardized mean difference; SRC, sport-related concussion.
Among all the intervention types, multidisciplinary interventions (E) demonstrated the most significant improvement in clinical outcomes (SMD = –2.0568; 95% CI, –3.3814, –0.7322; P = 0.002), with the highest P score (0.8865). VRT combined with SAEP (AB) also exhibited substantial efficacy (SMD = –1.8226; 95% CI, –3.4046, –0.2406; P = 0.02; P score = 0.7989). Similarly, VRT (B) demonstrated a significant therapeutic effect (SMD = –1.5884; 95% CI, –2.9653, –0.2115; P = 0.02), with a P score (0.7429) comparable with VRT combined with SAEP (AB).
SAEP (A) approached statistical significance (SMD = –0.8094; 95% CI, [–1.6235, 0.0047]; P = 0.05; P score = 0.4595), while UCEP (D) failed to show significant efficacy (SMD = –0.6319; 95% CI, –1.5679, 0.3041; P = 0.19; P score = 0.3476). Stretching protocols (C) exhibited the least effect (SMD = –0.2931; 95% CI, –1.3023, 0.7160; P = 0.57; P score = 0.1932).Given the substantial heterogeneity (τ² = 0.8001, τ = 0.8945; I2 = 90.5%; 95% CI, 86.3% to 93.4%), subgroup analyses were conducted (Figure 2b-d).
Subgroup Analyses
Acute-phase patients (Figure 2b): VRT (B) exhibited the highest efficacy (SMD = –1.6505; 95% CI, –2.9207, –0.3802), emerging as the most effective intervention; SAEP (A) demonstrated a moderate effect (SMD = –0.5771; 95% CI, –1.1623, 0.0080), ranking second; UCEP (D) showed limited impact (SMD = –0.3755; 95% CI, –1.1093, 0.3583); stretching protocols (C) had the lowest effect size (SMD = –0.0908; 95% CI, –0.7546, 0.5730).
Patients <30 years old (Figure 2c): multidisciplinary interventions (E) demonstrated the strongest effect (SMD = –2.4205, 95% CI, –3.6825, –1.1586), followed by VRT (B) (SMD = –1.8420, 95% CI, –3.1873, –0.4968); SAEP (A) had a moderate impact (SMD = –0.5737, 95% CI, –1.2562, 0.1087), while UCEP (D) (SMD = –0.1534, 95% CI, –1.0532, 0.7465) and stretching (C) (SMD = –0.0262, 95% CI, –0.8656, 0.8131) had minimal efficacy.
Patients with persistent symptoms (Figure 2d): interdisciplinary intervention (E) was the most effective strategy (SMD = –2.9990, 95% CI, –5.7478, –0.2502); VRT combined with SAEP (AB) (SMD = –2.4948, 95% CI, –5.6722, 0.6826) and VRT (B) (SMD = –2.6451, 95% CI, –6.8911, 1.6008) showed similar levels of effectiveness; UCEP (D) (SMD = –1.3304, 95% CI, –3.4284, 0.7676) and SAEP (A) (SMD = –1.2100, 95% CI, –3.9709, 1.5509) had moderate effects, while stretching (C) exhibited the lowest efficacy (SMD = –0.7137, 95% CI, –5.0003, 3.5729).
Local Consistency Analysis of Treatment Effects
Table 3 and Supplementary Figure S3 (available online) present the results of the local consistency test under the random-effects model, comparing direct and indirect evidence. The findings indicate that the differences between most treatment modalities did not reach statistical significance. However, the comparison between SAEP (A) and UCEP (D) approached significance, while the difference between UCEP (D) and Strict rest (F) was statistically significant. Generally, an absolute z-score >1.96 (for a 2-tailed test at α = 0.05) is considered statistically significant.
Tests for regional homogeneity a
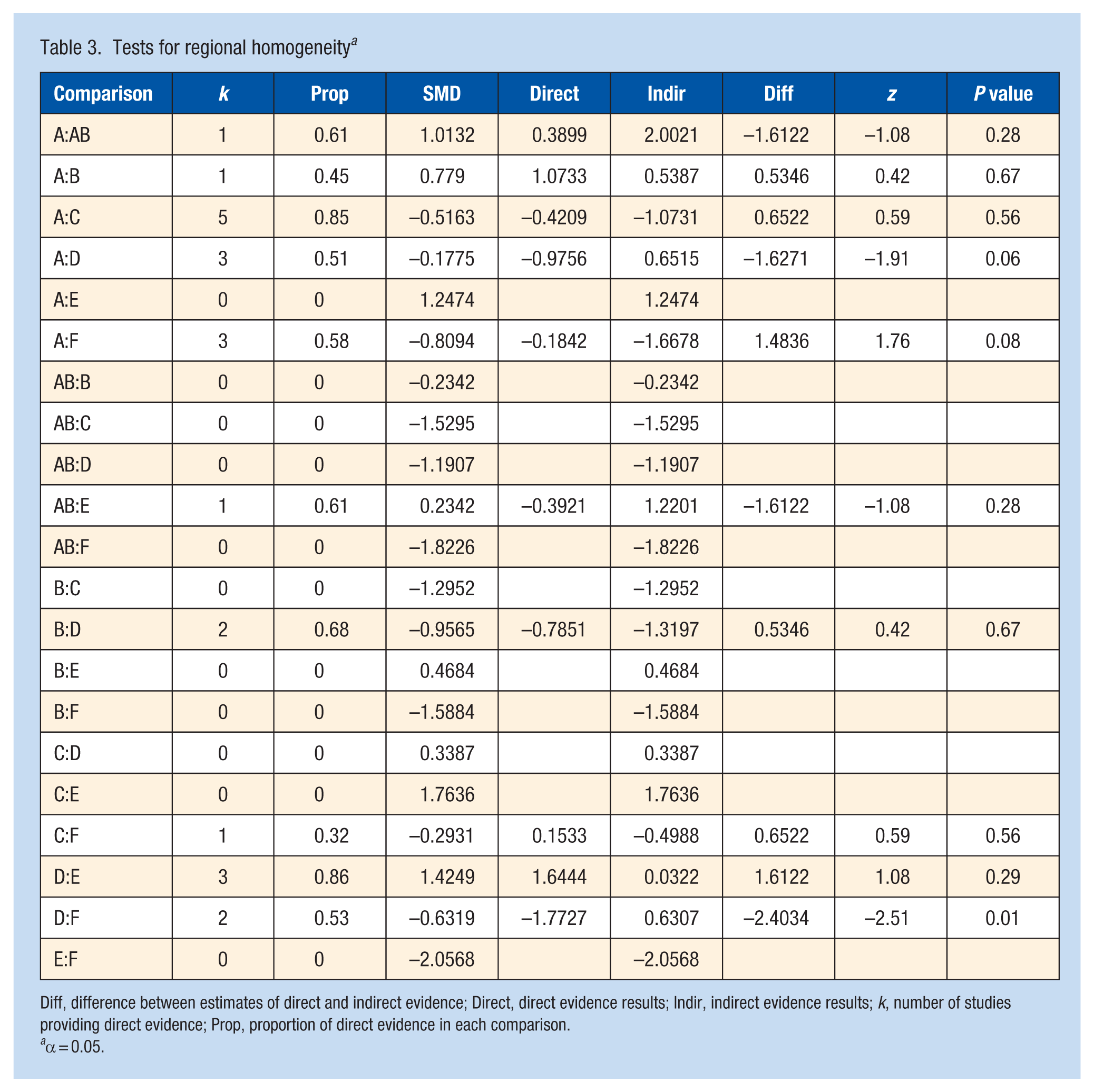
Diff, difference between estimates of direct and indirect evidence; Direct, direct evidence results; Indir, indirect evidence results; k, number of studies providing direct evidence; Prop, proportion of direct evidence in each comparison.
α = 0.05.
Specifically, the comparison between SAEP (A) and VRT combined with SAEP (AB) showed a direct effect of 1.0132 (SMD), an indirect effect of 0.3899 (SMD), and a difference of 2.0021 (SMD), with a z-score of –1.08 (P = 0.28), indicating no significant difference. Similarly, the comparison between SAEP (A) and VRT (B) yielded a direct effect of 0.7790 (SMD), an indirect effect of 1.0733 (SMD), and a difference of 0.5387 (SMD), with a z-score of 0.42 (P = 0.67), showing no significant difference. The comparison between SAEP (A) and stretching protocols (C) demonstrated a direct effect of –0.5163 (SMD), an indirect effect of –0.4209 (SMD), and a difference of –1.0731 (SMD), with a z-score of 0.59 (P = 0.56), also indicating no significant difference. The comparison between SAEP (A) and UCEP (D) revealed a direct effect of –0.1775 (SMD), an indirect effect of –0.9756 (SMD), and a difference of 0.6515 (SMD), with a z-score of –1.91 (P = 0.06), approaching significance. No direct evidence was available for the comparison between SAEP (A) and multidisciplinary interventions (E) , with an indirect effect of 1.2474 (SMD). Finally, the comparison between SAEP (A) and strict rest (F) showed a direct effect of –0.8094 (SMD), an indirect effect of –0.1842 (SMD), and a difference of –1.6678 (SMD), with a z-score of 1.76 (P = 0.08), nearing significance.
Furthermore, no direct evidence was available for the comparisons of VRT combined with SAEP (AB) versus VRT (B), VRT combined with SAEP (AB) versus stretching protocols (C), VRT combined with SAEP (AB) versus UCEP (D), or VRT combined with SAEP (AB) versus strict rest (F), and none exhibited significant differences. Similarly, comparisons between VRT (B) and stretching protocols (C), VRT (B) and UCEP (D), VRT (B) and multidisciplinary interventions (E), as well as VRT (B) and strict rest (F), did not demonstrate significant differences. Likewise, comparisons between stretching protocols (C) and UCEP (D), stretching protocols (C) and multidisciplinary interventions (E) , and stretching protocols (C) and strict rest (F) showed no significant differences, although some exhibited minor variations.
The comparison between UCEP (D) and multidisciplinary interventions (E) revealed a direct effect of 1.4249 (SMD), an indirect effect of 1.6444 (SMD), and a difference of 0.0322 (SMD), with a z-score of 1.08 (P = 0.28), indicating no significant difference. Conversely, the comparison between UCEP (D) and strict rest (F) showed a direct effect of –0.6319 (SMD), an indirect effect of –1.7727 (SMD), and a difference of 0.6307 (SMD), with a z-score of –2.51 (P = 0.01), indicating statistical significance. Finally, no direct evidence was available for the comparison between multidisciplinary interventions (E) and strict rest (F), with an indirect effect of –2.0568 (SMD).
Discussion
Study Findings
In the field of sports, the speed of concussion recovery and its long-term effects are of particular concern. Due to social and competitive pressures, athletes or patients may be compelled to return to play or duty prematurely, increasing the risk of secondary injuries. Therefore, scientifically sound rehabilitation management is crucial to mitigating the long-term consequences of concussion. The results indicate that multidisciplinary interventions (E) and VRT combined with SAEP (AB) were the most effective in SRC rehabilitation, significantly outperforming other interventions. VRT (B) and SAEP (A) also demonstrated substantial efficacy, whereas UCEP (D) and stretching protocols (C) had limited effects.
Subgroup analyses indicated that the efficacy of exercise-based interventions varied according to symptom duration and age. In acute-phase patients, VRT (B) was the most effective intervention, while SAEP (A) demonstrated moderate benefits. Considering that the brain continues developing into the mid-20s, 17 with the prefrontal cortex typically maturing around age 25 - a period accompanied by changes in physical activity, exercise habits, and rehabilitation potential - we conducted a subgroup analysis for participants younger than 30 years based on the age distribution of the included studies. 17 In this group, multidisciplinary interventions (E) produced the greatest improvements, followed by VRT (B), suggesting that early adulthood may represent a critical window for comprehensive rehabilitation strategies. Among patients with persistent symptoms, VRT combined with SAEP (AB) was most effective, whereas UCEP (D) and stretching protocols (C) demonstrated limited efficacy. These findings emphasize the importance of tailoring rehabilitation strategies according to patient characteristics, including age and symptom chronicity, to optimize recovery outcomes.
Effects of Rest and Aerobic Exercise on Concussion Recovery
Strict rest offers no advantage and may delay recovery, whereas early symptom-limited aerobic exercise is safe and supports postconcussion improvement.26,31,41,49 Hutchison et al 11 reported that SAEP (A) accelerates SRC recovery and is both safe and effective in clinical settings. Leddy et al 27 found that applying SAEP (A) within the first week post-SRC in symptomatic adolescents speeds recovery and may reduce delayed recovery. In a larger follow-up study, Leddy et al 28 used heartrate monitoring to assess adherence and intention-to-treat analysis, showing that adolescents randomized to subthreshold aerobic exercise recovered faster and had ~50% lower risk of PPCS compared with stretching. Aerobic exercise elicited higher mean heartrates (121 bpm vs 84 bpm), and patients in hospital-affiliated clinics exhibited more severe symptoms and higher delayed recovery rates. Snyder et al 43 observed symptom reduction in both aerobic and stretching groups after 7 consecutive days, although 1 participant with whiplash experienced increased symptoms, highlighting variability in exercise tolerance. Direct-impact concussions differ mechanistically from blast or penetrating injuries; however, studies indicate that the context of concussion (sports-related or motor-vehicle-related) does not significantly affect intervention outcomes.2,18 Acute-phase concussion can induce ion imbalance, disrupted energy metabolism, and impaired neural conduction, with subsequent injuries potentially exacerbating damage.3,8 Although the precise biological mechanisms remain unclear, animal studies indicate that aerobic exercise promotes neuroplasticity, stimulates neural stem cell proliferation, and inhibits apoptosis.13 -15 It also elevates serum brain-derived neurotrophic factor, supporting cognitive recovery, 29 and may gradually restore autonomic function disrupted postconcussion, enhancing physiological adaptation.4,25,42 Psychologically, aerobic exercise can reduce perceived symptom severity and improve quality of life, particularly emotional wellbeing in adolescents with slow concussion recovery. 7
These studies provide robust evidence supporting the feasibility and safety of early aerobic exercise interventions for postconcussion rehabilitation while highlighting the need for future research to establish individualized intervention strategies to optimize recovery pathways and advance personalized, interdisciplinary treatment approaches for SRC.
The Role of Physical Therapy Interventions in SRC Rehabilitation
Given the heterogeneous symptom presentation of SRC patients and the potential for some to develop persistent symptoms, exploring personalized intervention strategies remains a key research priority. Currently, no single therapy is universally effective for all patients, making patient-centered, interdisciplinary, and personalized intervention models crucial for SRC management. Interdisciplinary interventions prioritize identifying and addressing the most severe symptoms based on a patient’s symptom profile, demonstrating significant efficacy in symptom relief and prognosis improvement. 41 This intervention model relies on close collaboration among interdisciplinary teams to ensure consistency in treatment information, support long-term health management, and facilitate positive outcomes in social functioning and return to work or sport.
This study integrates evidence from 3 studies,5,38,45 highlighting the benefits of interdisciplinary interventions incorporating VRT and aerobic exercise. For example, Rytter et al 38 implemented an interdisciplinary intervention program that provided comprehensive support for mTBI patients, significantly improving symptoms and quality of life. In addition, Vikane et al 48 evaluated the effect of a multidisciplinary outpatient follow-up program compared with follow-up by general practitioners in patients with mild traumatic brain injury. The results showed that, although it did not significantly accelerate return to work, it helped alleviate long-term postconcussion symptoms.
VRT, as a standalone intervention, also demonstrated considerable efficacy. Storey et al 44 reported that VRT improved postconcussion symptoms and visuovestibular function in children. In a retrospective study, Alsalaheen et al 1 found that adolescents undergoing vestibular home exercises showed significant improvements in VOMS scores. However, given the retrospective design and lack of control groups in some studies, further research is needed to enhance evidence quality. Schneider et al 40 found in an RCT that cervico VRT shortened recovery time for adolescents and young adults experiencing persistent dizziness, neck pain, or headaches post-SRC, with more participants receiving medical clearance to return to play within 8 weeks. Kontos et al 20 further confirmed that VRT may accelerate concussion recovery by reducing symptom severity and duration through controlled symptom exposure.
Limitations and Future Directions
This study did not impose restrictions on age and injury duration, although subgroup analyses were conducted later. The elderly population is more likely to have associated mental health issues (e.g., anxiety and depression), which are less common in adolescent and younger groups, potentially influencing the results. Nevertheless, most of the treatment comparisons in this study maintained good consistency between direct and indirect evidence, supporting the robustness of the NMA results. The comparison between conventional treatment and strict rest showed significant differences. This may be due to the fact that many studies did not monitor participants throughout the entire process. While structured subthreshold aerobic exercise is not part of conventional treatment, some patients may have still engaged in some degree of physical activity after a brief period of physical and cognitive rest. Therefore, some participants may have unknowingly engaged in additional exercise. For other studies comparing physical therapy with conventional treatments, if participants had additional exercise, this effect is more likely to weaken rather than enhance the effect of aerobic exercise, thus making it less likely to exaggerate the research results.
The NMA revealed substantial heterogeneity among the included studies, with tau 2 = 0.8001, tau = 0.8945, and I 2 = 90.5% [86.3%; 93.4%]. While the overall reporting quality was generally good, some studies lacked key information (e.g., intervention frequency or duration). Variation in intervention frequency (1 to 7 sessions per week), session duration (15 to 120 minutes), participant age, symptom severity, and the proportion of SRC cases likely contributed to this heterogeneity and may limit the external validity of the findings. More intensive or longer-duration interventions tended to produce greater benefits, whereas less intensive protocols yielded weaker effects. Therefore, the results should be interpreted with caution, and future studies should aim to standardize intervention protocols and fully report key study characteristics to reduce heterogeneity and improve comparability. Howell et al 10 found that compliance with exercise prescriptions is crucial for concussion recovery, and differences in exercise volume or intensity could lead to varying recovery outcomes. Participants who exercised >160 minutes per week in the first month of the study experienced significantly better symptom relief than those who exercised <100 minutes per week. 10 This result suggests that higher exercise volume may be associated with symptom relief. Some studies have pointed out that the severity of initial symptoms is an important factor in predicting recovery time and recommended that future studies improve research designs, such as controlling for initial symptom severity, monitoring exercise volume, and optimizing medical clearance standards. 34 Due to the current lack of a gold-standard test for accurately diagnosing SRC (despite advanced neuroimaging, fluid-based biomarkers, genetic testing, and emerging technologies providing important tools for concussion research, these are not yet applicable in clinical routine practice), clinicians typically rely on patient-reported symptoms and clinical signs to diagnose concussions. As a result, it is somewhat difficult to determine whether a patient has symptoms or whether symptoms are not reported.33,36 In this context, the placebo effect is particularly noticeable, as patients may report fewer symptoms based on external expectations (such as hoping for symptom reduction or faster recovery). Therefore, a standardized definition of “recovery” needs to be established to avoid inconsistencies across studies. In addition, physiological recovery time may be longer than clinical recovery time (i.e., symptoms may disappear on the surface, but the brain may not yet be fully recovered). 25 Hence, future prospective cohort studies should track patients long-term until both physiological indicators and clinical symptoms are completely resolved, to further optimize SRC treatment strategies and rehabilitation pathways.
Conclusion
This NMA supports multidisciplinary interventions and VRT combined with SAEP as the preferred treatments for sports-related concussions. In addition, multidisciplinary interventions demonstrated strong effects in patients with persistent symptoms and those <30 years of age, while VRT also showed significant benefits in patients during the acute phase and those <30 years old.
Supplemental Material
sj-docx-1-sph-10.1177_19417381261442593 – Supplemental material for Physical Therapy for Sport-Related Concussion: A Network Meta-analysis and Systematic Review
Supplemental material, sj-docx-1-sph-10.1177_19417381261442593 for Physical Therapy for Sport-Related Concussion: A Network Meta-analysis and Systematic Review by Huangyan Li, Jiangxi Yang, Yeting Zhang, Chang Qu and Shiliang Hu in Sports Health
Supplemental Material
sj-docx-2-sph-10.1177_19417381261442593 – Supplemental material for Physical Therapy for Sport-Related Concussion: A Network Meta-analysis and Systematic Review
Supplemental material, sj-docx-2-sph-10.1177_19417381261442593 for Physical Therapy for Sport-Related Concussion: A Network Meta-analysis and Systematic Review by Huangyan Li, Jiangxi Yang, Yeting Zhang, Chang Qu and Shiliang Hu in Sports Health
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.