
Abstract
Context:
This study aimed to evaluate the effects of concurrent strength and aerobic exercise training (CET) on cognitive function in middle-aged and older adults with physiological conditions (e.g., type 2 diabetes, metabolic syndrome, cardiovascular disease, chronic obstructive pulmonary disease, frailty, fibromyalgia) or neurocognitive disorders (e.g., mild cognitive impairment, dementia, Alzheimer’s disease [AD]).
Evidence Acquisition:
Two independent reviewers conducted a systematic search of PubMed, EMBASE, Cochrane Library, Web of Science, Scopus, SPORTDiscus, CNKI, WanFang, and Google Scholar from inception to July 2024. Randomized controlled trials (RCTs) examining CET (≥4 weeks) in clinical populations, reporting global cognition via validated tools (e.g., Mini-Mental State Examination [MMSE], Montreal Cognitive Assessment [MoCA]). Non-RCTs, acute interventions, healthy populations, and lack of control were excluded. Two reviewers performed study selection, data extraction, and risk of bias assessment independently using the Cochrane Risk-of-Bias 2.0 tool; discrepancies were resolved by a third reviewer. Standardized mean differences (SMD) with 95% CI were calculated using random-effects models.
Study Design:
Systematic review and meta-analysis.
Level of Evidence:
Level II.
Results:
A total of 22 RCTs involving 3463 participants (age range, 43.9-92.1 years; 48% female) were included. Of these, 714 participants had physiological disorders (e.g., diabetes, fibromyalgia, frailty) and 2442 had neurocognitive disorders (e.g., dementia, AD). CET significantly improved global cognitive function compared with controls (SMD = 0.34; 95% CI, 0.18 to 0.50; P < 0.001; I2 = 67%). Subgroup analyses demonstrated significant improvements in both physiological disorders (SMD = 0.29; 95% CI, 0.09 to 0.49; P < 0.01) and neurocognitive disorders (SMD = 0.37; 95% CI, 0.14 to 0.55; P < 0.01). No publication bias was detected (Egger’s test P = 0.62).
Conclusion:
CET is an effective nonpharmacological intervention for enhancing cognitive health in middle-aged and older adults with physiological or neurocognitive disorders.
Strength-of-Recommendation Taxonomy (SORT):
Moderate.
Keywords
Cognitive health refers to maintained cognitive capacities (e.g., memory, executive function, attention) essential for daily functioning and adaptation across the lifespan.7,41 As global population growth decelerates and the aging population expands, the prevalence of cognitive decline and dementia has emerged as a major public health challenge. 76 Currently, approximately 50 million people worldwide live with dementia, projected to rise to 152 million by 2050.1,50 A report by Alzheimer’s Disease International estimates that the global cost of dementia was approximately US $1.3 trillion in 2019, with projections indicating it will double by 2030. 75 This increasing prevalence underscores the need for effective interventions to promote cognitive health and mitigate the risk of cognitive decline.
Physical exercise has emerged as a promising nonpharmacological intervention. Specifically, aerobic exercise improves cerebral blood flow and levels of brain-derived neurotrophic factor (BDNF),53,54 while strength training enhances executive function through muscle-derived myokines (e.g., irisin) and insulin-like growth factor 1 (IGF-1) pathways,11,31,39 and reduces systemic inflammation.12,38,77 Concurrent exercise training (CET) has garnered attention for its physiological interference, which is the attenuation of strength or endurance adaptations when aerobic and strength training are combined.23,30,55 However, a growing body of evidence indicated that these training interactions may enhance brain plasticity and cognitive function synergistically.29,60 Despite this, long-term CET effects in population with clinical conditions remained understudied. Therefore, this meta-analysis aimed to evaluate the effects of CET on cognitive function in middle-aged and older adults with physiological conditions (e.g., diabetes, metabolic syndrome, fibromyalgia) or neurocognitive disorders (e.g., mild cognitive impairment [MCI], dementia, Alzheimer’s disease [AD]). CET was compared with active comparators (aerobic-alone or resistance-alone training), 79 and passive controls (e.g., no intervention, health education, or routine care). 47 We hypothesized that CET modalities would yield superior cognitive benefits in these high-risk populations.
Methods
Study Design and Objectives
The systematic review and meta-analysis was conducted following Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA 2020) guidelines, 37 and was registered prospectively with the International Prospective Register of Systematic Reviews (PROSPERO ID: CRD42024587940).
The primary objective was to evaluate the effect of CET on global cognitive function in middle-aged and older adults with physiological or neurocognitive disorders.
Secondary objectives were to compare the magnitude of CET effects between participants with physiological disorders (e.g., diabetes, cardiovascular disease, frailty) versus neurocognitive disorders (e.g., MCI, dementia, Alzheimer's disease), and to examine whether the order of exercise (aerobic-first vs strength-first) moderates cognitive outcomes.
Search Strategy
A comprehensive search was conducted across 9 electronic databases: PubMed, EMBASE, Cochrane Library, Web of Science, Scopus, Google Scholar, SPORTDiscus, China National Knowledge Infrastructure (CNKI), and WanFang Database from their inception to July 2024, without language restrictions. For Google Scholar, we screened the first 400 most relevant results due to high overlap with other databases. 25 We also used artificial intelligence (AI)-assisted search tools (Elicit and Consensus) to identify potentially relevant studies. The search strategy combined controlled vocabulary terms and keywords related to CET and cognitive health (see Supplementary Table S1, available in the online version of this article). Boolean operators, proximity searches, and truncation were employed to capture a wide range of terminologies. In addition, we performed backward citation tracking (screening key reference lists of included studies and relevant systematic reviews and/or meta-analyses) and forward citation tracking to identify potentially eligible studies missed by database searching.
Two independent reviewers screened all titles and abstracts. Full-text articles were retrieved for potentially eligible studies and independently assessed by the same reviewers. Conflicts were resolved through discussion or by consulting a third reviewer when consensus could not be reached.
Eligibility Criteria
Studies were included if they (1) investigated middle-aged and older adults (≥40 years old) with physiological or neurocognitive disorders, (2) employed concurrent strength and aerobic exercise training interventions lasting at least 4 weeks, (3) included a control group (passive or active control), and (4) measured global cognitive function using validated tools. Only randomized controlled trials (RCTs) were included because they establish causal relationships between interventions and outcomes, minimize selection bias through randomization, and allow for robust meta-analytic pooling of effect sizes. Conversely, studies were excluded if they (1) employed nonrandomized designs, (2) included healthy populations without clinical diagnoses, (3) investigated acute (single-bout) exercise rather than chronic training programs, (4) lacked a control group, (5) did not report cognitive outcomes, and (6) had overlapping participant populations with already included studies.
Data Items
The primary outcome of interest was global cognitive function, measured by validated neuropsychological tests including: Mini-Mental State Examination (MMSE), Montreal Cognitive Assessment (MoCA), Alzheimer’s Disease Assessment Scale-Cognitive Subscale (ADAS-Cog), Paced Auditory Serial Addition Task (PASAT), Addenbrooke’s Cognitive Examination-Revised (ACE-R), and Global Composite Scores (GCS). Secondary outcomes included domain-specific cognitive functions (executive function, memory, attention) where available.
Study Selection and Data Extraction
Titles and abstracts were evaluated independently by 2 reviewers. Full texts of studies identified as potentially eligible were retrieved for comprehensive assessment. Discrepancies in study selection were resolved through discussion or consultation with a third reviewer. Data extraction was conducted meticulously by 2 reviewers utilizing a standardized form that captured essential study characteristics (e.g., author, publication year, objectives, and findings), participant demographics (e.g., sample size, sex, and age), training modalities and sequences, intervention conditions (types, frequency, session duration, length of intervention, and comparator information), data characteristics (relevant data for assessing effect sizes, including means and standard deviations, CIs, and corresponding measurement tools). In instances where multiple articles stemmed from the same population, only the article with the longest follow-up or largest sample size was included to avoid duplicate participant data. Studies with overlapping populations were not included in the meta-analysis. However, if the same study presented separate statistical analyses for healthy and clinical populations, data specific to each population were extracted for meta-analysis. When cognitive outcomes were measured at both postintervention and follow-up, only data from the postintervention period were retained for analysis.
Risk of Bias Assessment
Two independent reviewers assessed the risk of bias using the Cochrane Risk-of-Bias tool Version 2.0. These guidelines evaluated distinct domains as follow: random sequence generation, allocation concealment, participant and personnel blinding, outcome assessment blinding, incomplete outcome data, selective reporting, and potential sources of bias. 28 Each domain was evaluated using 7 items, and the overall risk of bias for each study was categorized as ‘low,’ ‘high,’ or ‘some concerns’ based on the detected level of bias. Discrepancies between reviewers were resolved through discussion or by consulting a third reviewer.
Data Synthesis and Analysis
Statistical analyses were conducted using Stata software (Version 18.0; StataCorp.) and Review Manager software (Version 5.4.1) provided by the Cochrane Collaboration. The fixed-effect or random-effects model was used for pooling data when heterogeneity was not significant (I2 < 50%); otherwise, the random-effects model was applied to account for the variability among studies. Standard errors, ranges, within-group CIs, and statistical P values were transformed and integrated. 28 Standardized mean differences (SMDs) with 95% CIs were calculated for continuous outcomes. Heterogeneity was assessed using the Higgins I2 statistic and the Q test. The pooled effect size was calculated using a fixed-effect model when data were available and heterogeneity was minimal. In cases where high statistical heterogeneity was detected, as assessed by the χ2 test, the Higgins I2 statistic, and the Q test. I2 values of 25%, 50%, and 75% were considered low, moderate, and high heterogeneity, respectively. Subgroups were determined based on potential sources of heterogeneity, such as differences in cognitive assessment tools (e.g., global cognitive ability being measured by MMSE, ADAS-Cog, MoCA, PASAT) and measurement units. Given the differing directional interpretations of cognitive test scores, a separate analysis was conducted for tests with positive score benefits (e.g., MMSE, MoCA, PASAT), where higher scores indicate better cognitive function, and tests with negative score benefits (only ADAS-Cog), where lower scores indicate better cognitive outcomes. For each type of test, the data were pooled separately to ensure that the interpretation of effect sizes remained consistent with the directionality of the outcome measures. In the Galbraith plot, each study is represented by a data point where the x-axis denotes the precision (1/standard error) and the y-axis represents the standardized effect sizes, calculated as Hedges’s g. The 95% CI for each study is depicted to provide an indication of the uncertainty around the effect size estimates. Studies located at the extremes of the plot, particularly those far from the no-effect line, may exert a significant influence on the overall meta-analysis outcome. Publication bias was assessed using funnel plots and Egger’s test. 19
Results
Study Identification
The systematic search yielded 13,533 from 9 electronic databases and supplementary sources. After removing duplicates (n = 7665) and screening titles and abstracts, 491 full-text articles were assessed for eligibility. One study was excluded because its intervention design focused on the combination of aerobic exercise and cognitive training rather than on concurrent training. 48 Two studies employed the single-group pre-post study design.36,44 Ultimately, 22 studies fulfilled the inclusion criteria (Figure 1).2 -4,13 -15,21,22,24,26,34,35,40,43,46,56 -59,63,66,73
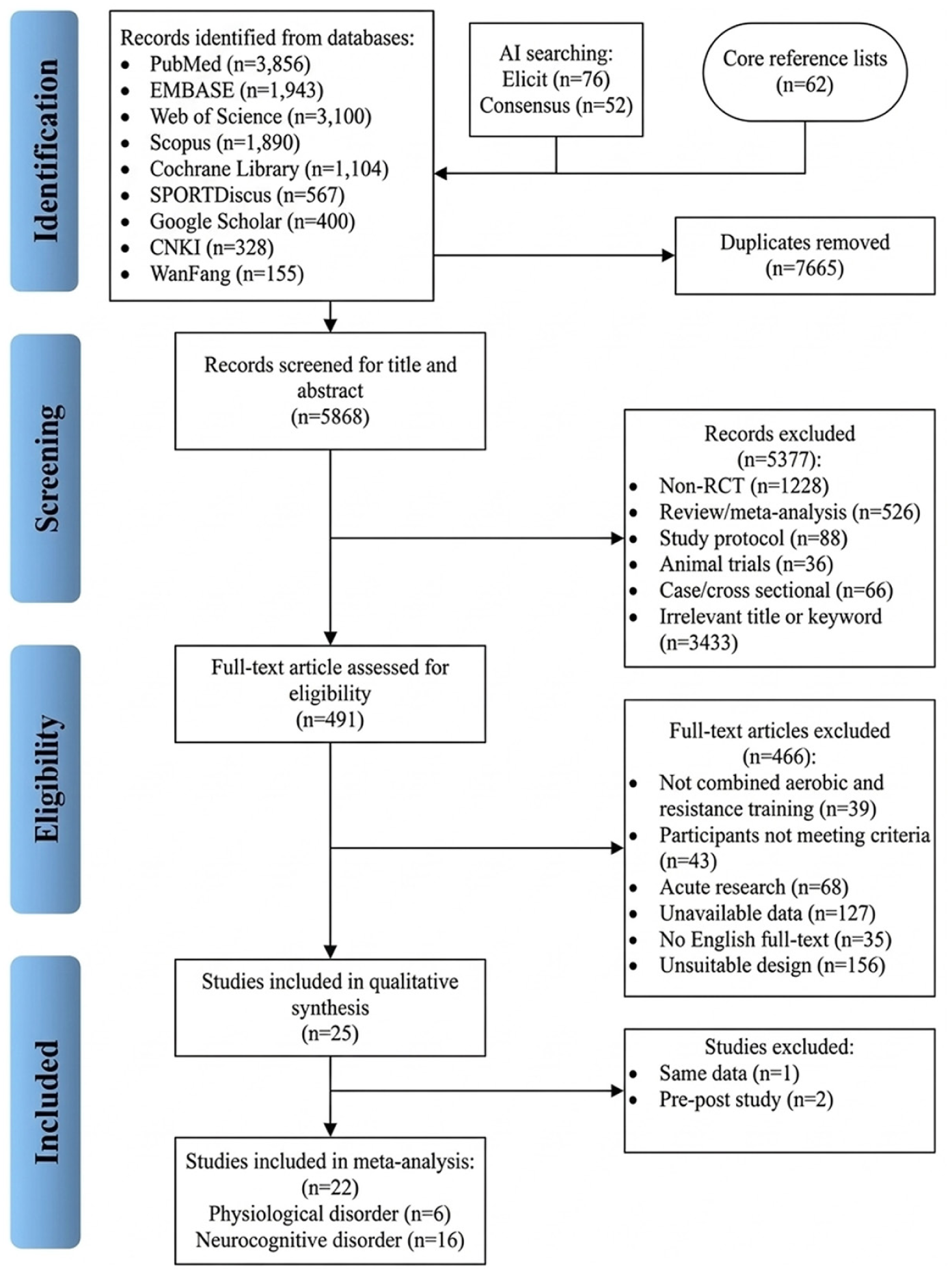
PRISMA flowchart of the study selection process. AI, artificial intelligence; PRISMA, preferred reporting items for systematic reviews and meta-analyses; RCT, randomized controlled trial.
Characteristics of Included Studies
Table 1 summarizes the study characteristics. The 22 RCTs included middle-aged and older adults (age range, 43.9-92.1 years; sample sizes, 21-1476). Regarding participants, 1712 engaged in CET, while 1751 were assigned to the control group. Of the included studies, 6 (n = 714) included people with specific physiological disorders, such as diabetes, fibromyalgia syndrome, and frailty,21,24,34,43,46 and 16 (n = 2442) enrolled participants with neurocognitive disorders, including MCI, dementia, AD, and MS.2,3,13 -15,21,22,26,35,57,58,63,66,73 Four studies (9%) involved participants with mixed clinical statuses,21,34,46,63 while 3 studies included patients with both MCI and AD.14,22,66 Two studies reported data concurrently from populations with distinct neurological conditions.14,22
Characteristics of the studies included in the meta-analysis
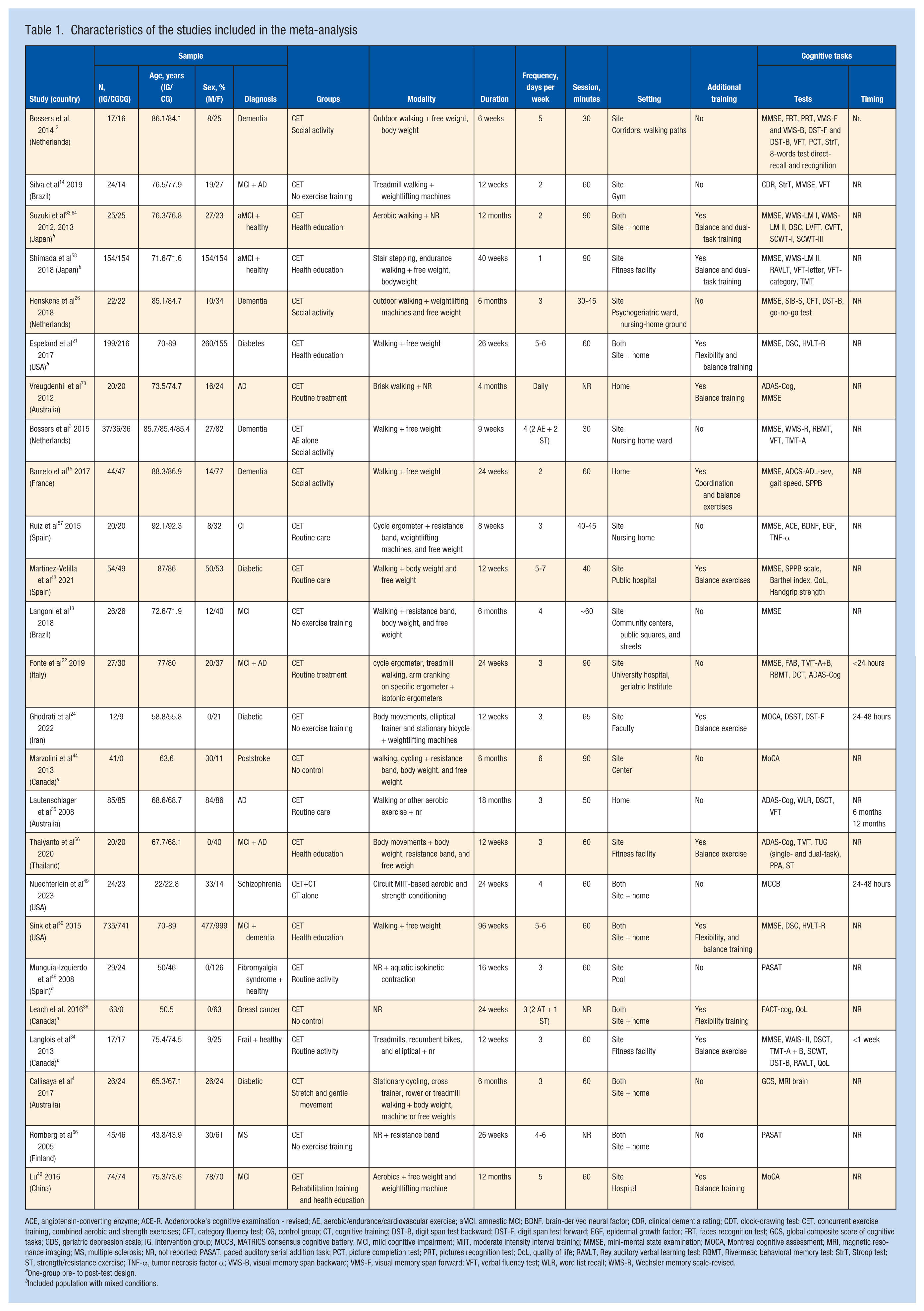
ACE, angiotensin-converting enzyme; ACE-R, Addenbrooke’s cognitive examination - revised; AE, aerobic/endurance/cardiovascular exercise; aMCI, amnestic MCI; BDNF, brain-derived neural factor; CDR, clinical dementia rating; CDT, clock-drawing test; CET, concurrent exercise training, combined aerobic and strength exercises; CFT, category fluency test; CG, control group; CT, cognitive training; DST-B, digit span test backward; DST-F, digit span test forward; EGF, epidermal growth factor; FRT, faces recognition test; GCS, global composite score of cognitive tasks; GDS, geriatric depression scale; IG, intervention group; MCCB, MATRICS consensus cognitive battery; MCI, mild cognitive impairment; MIIT, moderate intensity interval training; MMSE, mini-mental state examination; MOCA, Montreal cognitive assessment; MRI, magnetic resonance imaging; MS, multiple sclerosis; NR, not reported; PASAT, paced auditory serial addition task; PCT, picture completion test; PRT, pictures recognition test; QoL, quality of life; RAVLT, Rey auditory verbal learning test; RBMT, Rivermead behavioral memory test; StrT, Stroop test; ST, strength/resistance exercise; TNF-α, tumor necrosis factor α; VMS-B, visual memory span backward; VMS-F, visual memory span forward; VFT, verbal fluency test; WLR, word list recall; WMS-R, Wechsler memory scale-revised.
One-group pre- to post-test design.
Included population with mixed conditions.
A total of 18 studies delivered strength and aerobic components in the same session. Of these, 15 explicitly reported exercise intensity, ranging from light to high relative load. Data on the order of exercise modalities were extracted when available, with 55% of the studies providing this information. The sessional frequency ranged from 1 to 7 times per week, with durations spanning 30 to 90 minutes. Furthermore, all studies involved chronic exercise interventions lasting from 6 to 96 weeks (cumulative volume, 900-34,560 minutes). Passive controls (routine care, health education, wait-list) were used in 18 studies, while active controls (aerobic-only, alternative exercise) were used in 4 studies. Cognitive outcomes were assessed using MMSE (n = 13), ADAS-Cog (n = 5), MoCA (n = 2), PASAT (n = 2), and GCS (n = 2).
Of the 22 trials, 17 (68%) were conducted exclusively on-site (e.g., hospital, gym, fitness facility, community center, nursing home, or public corridors), 5 (20%) were conducted solely at participants’ homes, and 3 (12%) followed a hybrid schedule (initial on-site instruction followed by home-based sessions). Eight on-site studies explicitly mentioned group-based or supervised in pairs sessions, while all home-based interventions relied on telephone or video support from caregivers or researchers.
Effects of CET on Global Cognition
Among the included trials, 4 studies reported postintervention cognitive assessment within 24 to 48 hours of the final exercise bout,22,24,34,49 and the remaining studies did not specify testing intervals. The meta-analysis indicated that CET improved global cognitive function significantly compared with controls (SMD = 0.34, 95% CI 0.18 to 0.50; P < 0.001; I2 = 67%; random-effects model; Figure 2a). Moderate heterogeneity was observed among the studies (P < 0.01). Analysis of ADAS-Cog scores showed significant improvements with CET (SMD = –0.44; 95% CI, –0.65 to –0.22; P < 0.001; I2 = 0%; fixed-effects model; Figure 2b).
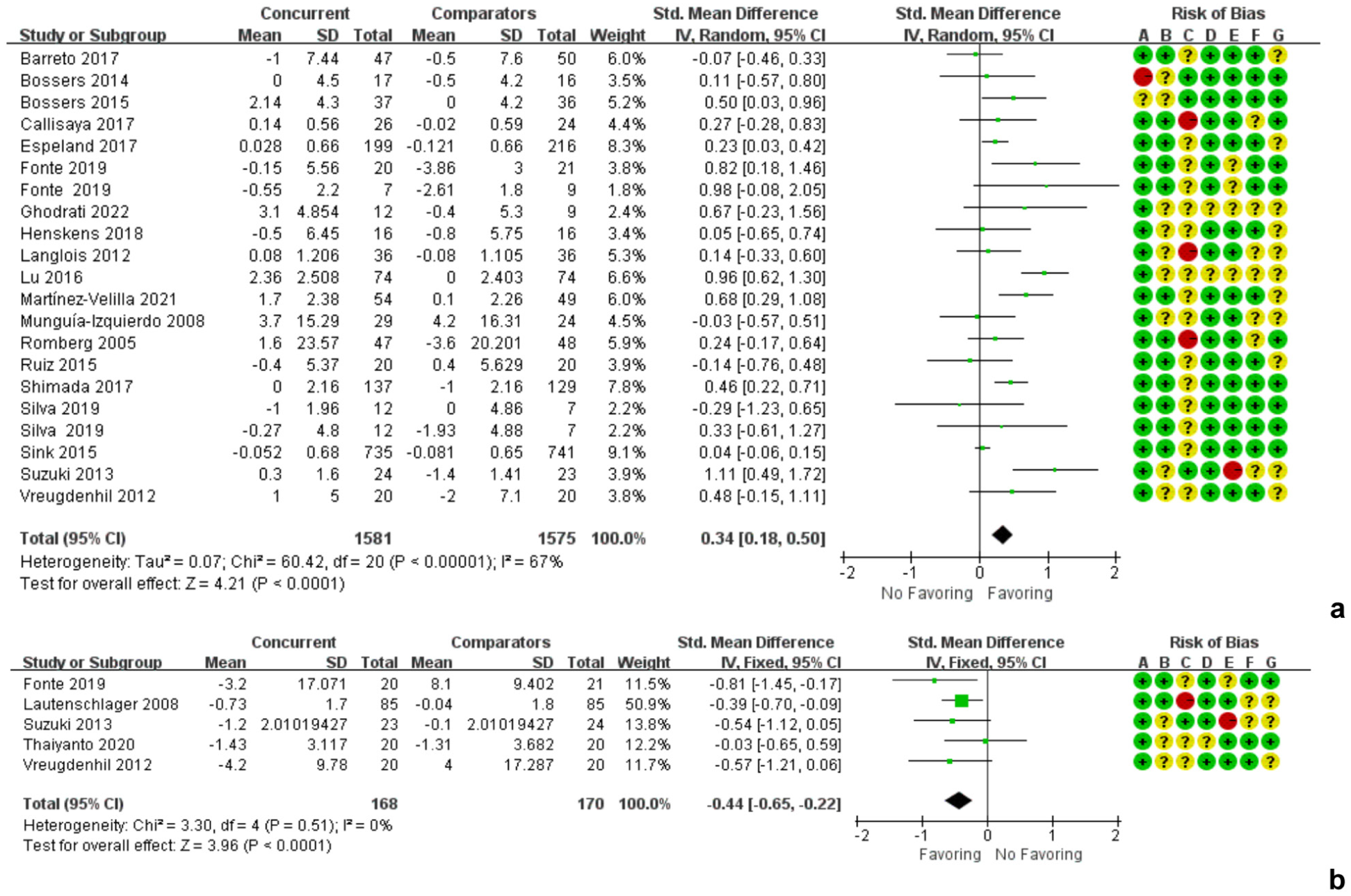
Forest plot of the effects of CET on global cognitive function. Global cognitive function was assessed using (a) MMSE, MoCA, PASAT, GCS, or (b) ADAS-Cog. Risk of bias elements are highlighted in the legend below the forest plot and bias is indicated as low (green), unclear (yellow), or high (red). ADAS-Cog, Alzheimer’s disease assessment scale-cognitive subscale; CET, concurrent exercise training; GCS, global cognition scores; IV, inverse variance; MMSE, mini-mental state examination; MoCA, Montreal cognitive assessment; PASAT, paced auditory serial addition task; Std, standard.
Subgroup analysis by clinical population revealed significant cognitive improvements in both physiological disorders (n = 714; SMD = 0.29; 95% CI, 0.09 to 0.49; P < 0.01; I2 = 21%) and neurocognitive disorders (n = 2442, SMD = 0.37; 95% CI, 0.14 to 0.55; P = 0.001; I2 = 74%; Figure 3). Two studies from the subgroup analysis of neurocognitive disorders may represent potential sources of heterogeneity (I2, 74% to 41%).40,59 In another subgroup analysis, 12 studies focusing on the order of exercise modalities demonstrated a significant improvement in global cognition (n = 2734; SMD = 0.32; 95% CI, 0.14 to 0.50; P < 0.001; Figure 4). No significant subgroup differences were observed among the clinical populations (P = 0.63) and the order of exercise modalities (P = 0.18).
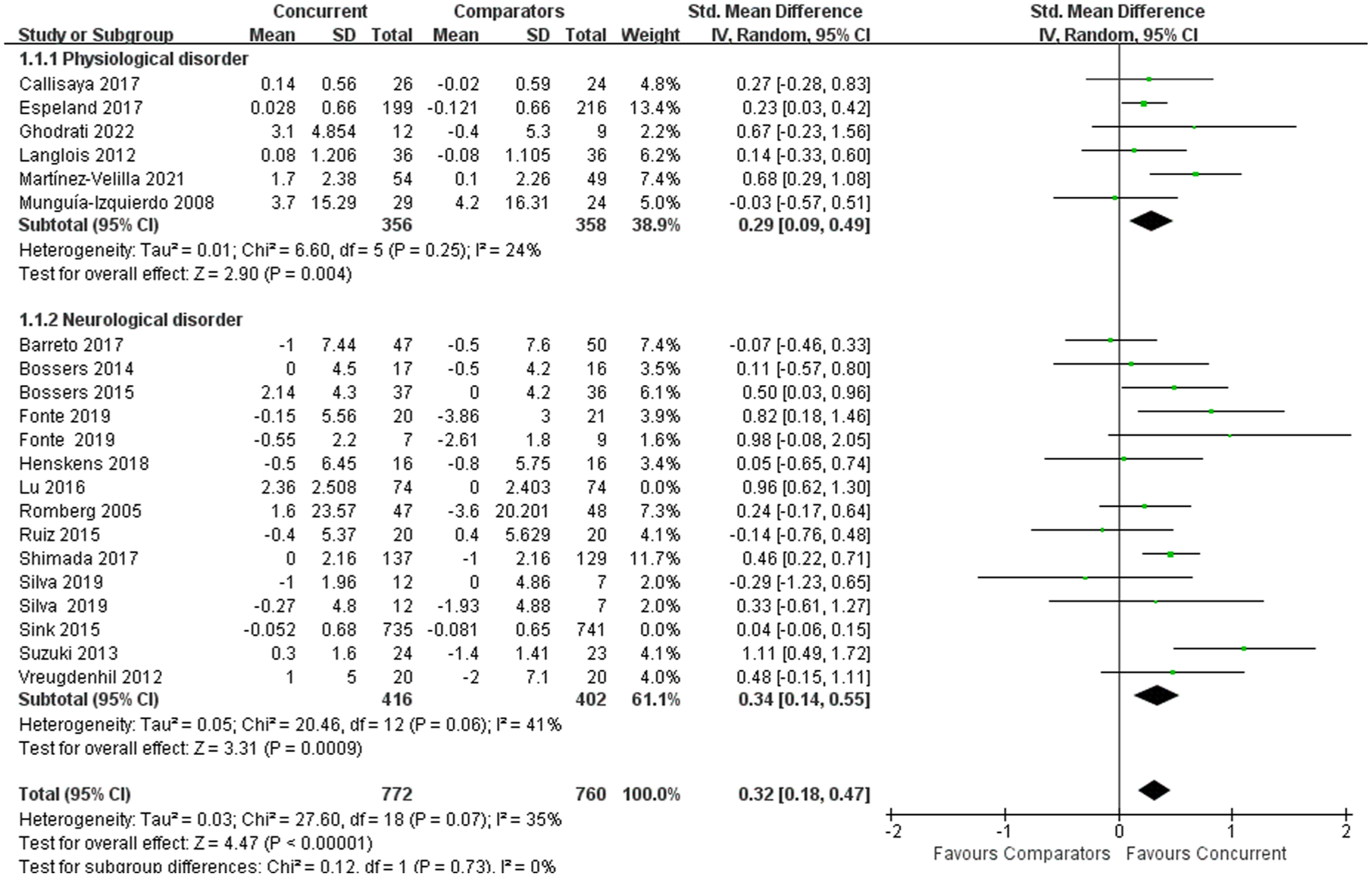
Forest plot of studies comparing differences on global cognitive function with CET between patients with physiological disorder and neurological disorder. Physiological disorder included diabetes, fibromyalgia syndrome, or frail symptoms. Neurological disorder included MCI, dementia, AD, or multiple sclerosis. AD, Alzheimer’s disease; CET, concurrent exercise training; IV, inverse variance; MCI, mild cognitive impairment; Std, standard.
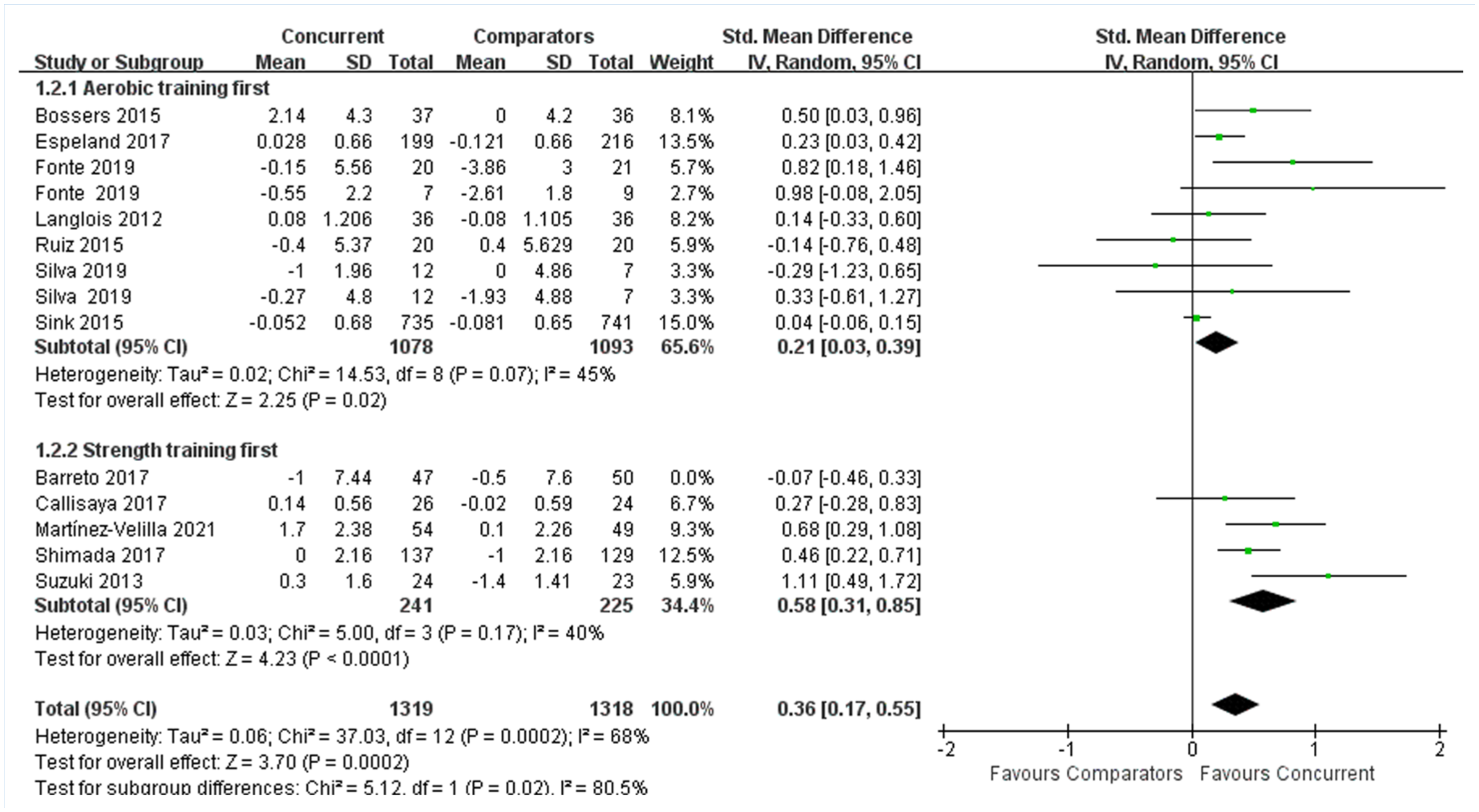
Forest plot for concurrent strength and aerobic exercise on global cognitive function according to training order. IV, inverse variance; Std, standard.
Risk of Bias
Figure 5 presents the risk of bias assessment. None of studies exhibited critical risk. Random sequence generation showed low risk in 95% of studies, although allocation concealment raised concerns in 25%. Blinding of participants/personnel was inadequate in 50% of studies, while incomplete outcome data posed low risk in the majority. Selective reporting was unclear in 50% of cases.
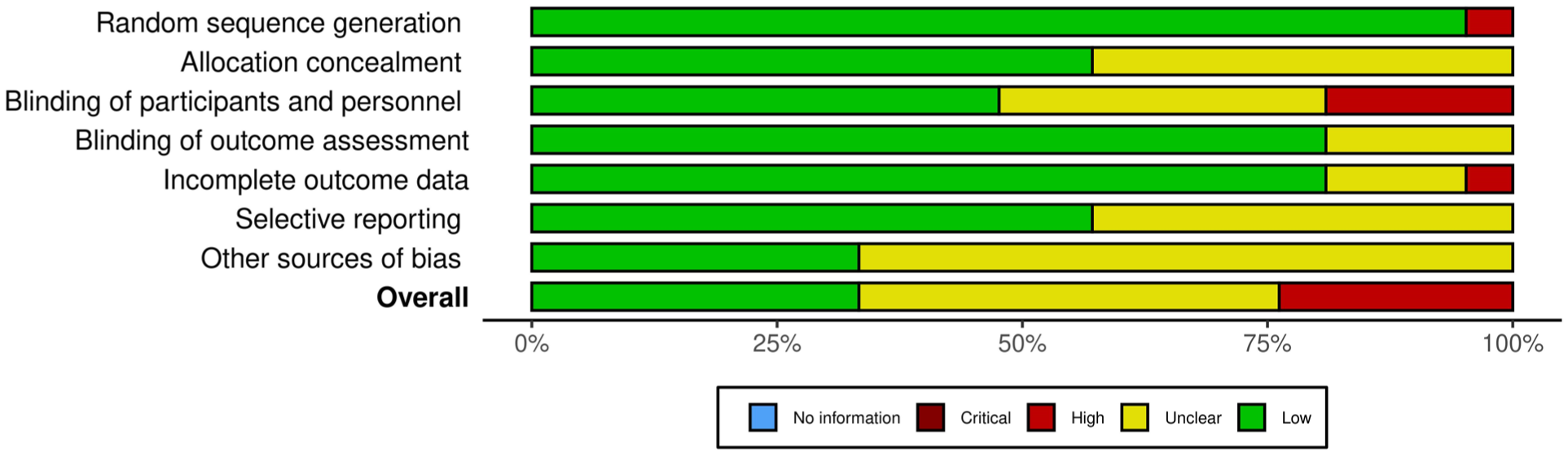
Risk of bias graph.
Publication Bias and Sensitivity Analysis
A funnel plot demonstrated symmetry (Figure 6), confirmed by nonsignificant Egger’s test (P = 0.62). A Galbraith plot indicated that no single study exerted undue influence on the pooled effect (Figure 7). Sensitivity analysis showed robust overall results. The overall results remained consistent across all deletions; however, a notable decrease in heterogeneity (I2, 67% to 35%) was observed after the exclusion of the studies by Sink et al 59 and Lu 40 in the first subgroup analysis.
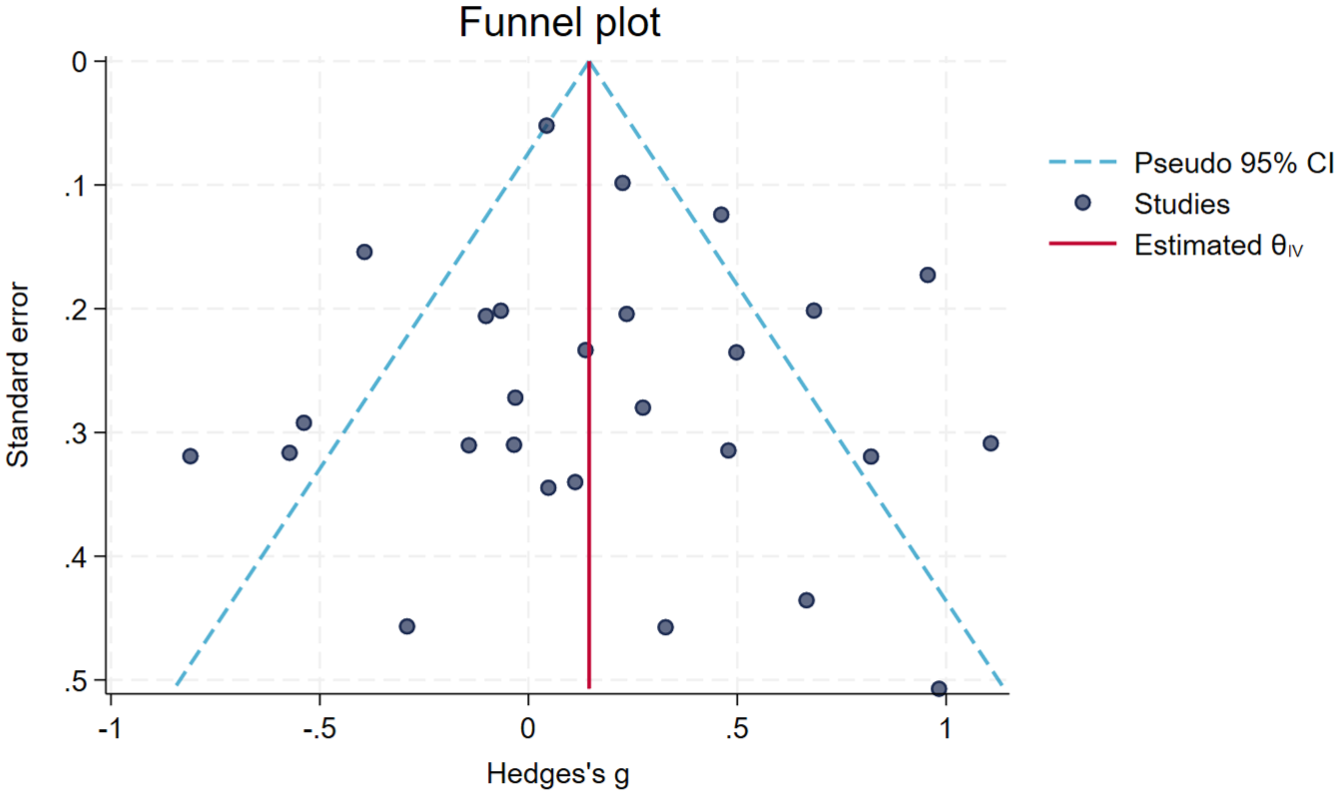
Funnel plot of included dependent effect sizes.
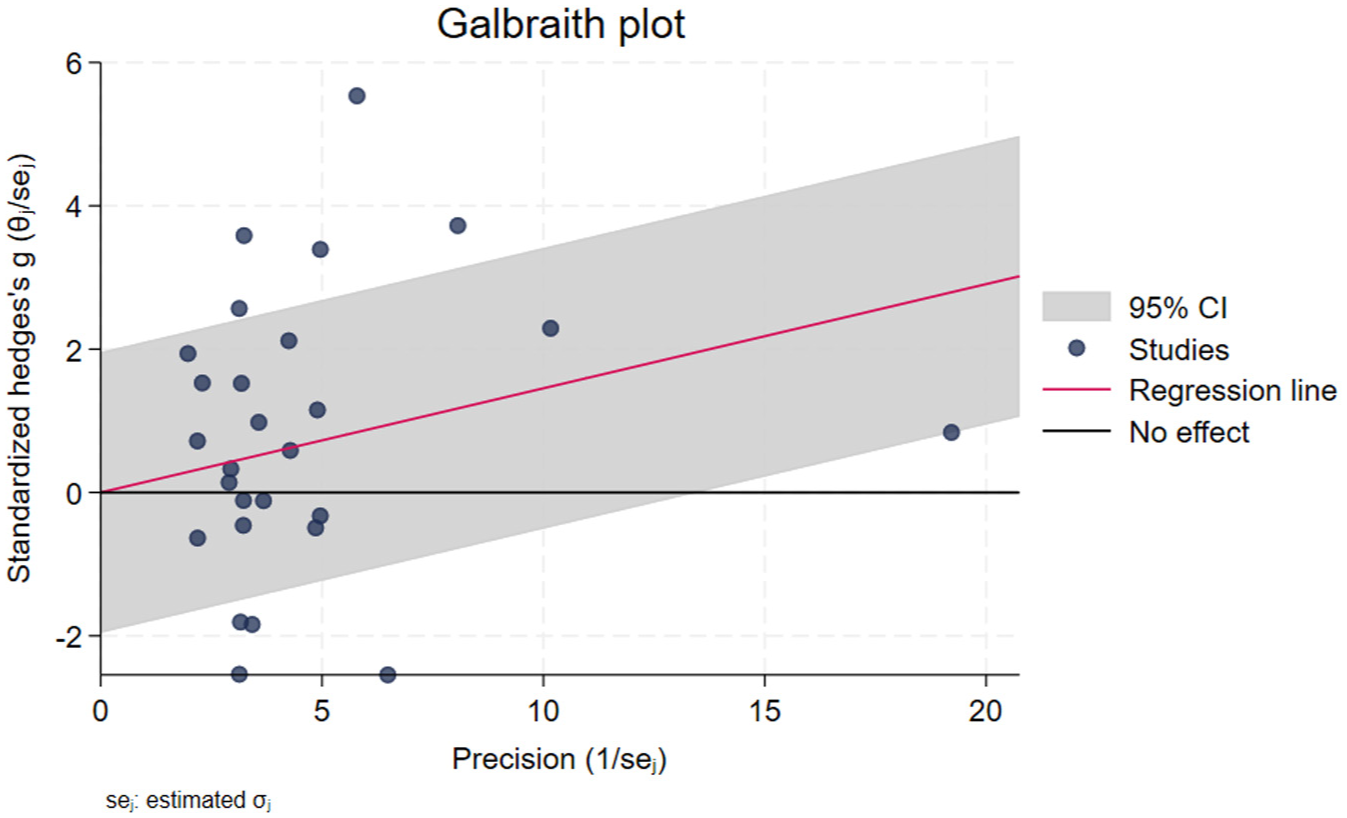
Galbraith plot assessing heterogeneity and influence of included studies.
Discussion
The findings provide evidence that CET impacts cognitive health positively in clinical populations of middle-aged and older adults. While the overall effect suggests potential advantages of combining strength and aerobic training modalities to enhance global cognition, it is important to note that the evidence for an additional benefit of CET compared with either modality alone is limited. This raises questions about the superior effects of CET versus single exercise modalities. Future research should aim to clarify these distinctions and further investigate the specific mechanisms through which CET may confer additional cognitive benefits. Furthermore, subgroup analyses revealed that the effects on cognitive benefits were influenced by participants’ cognitive status and the order of exercise modalities, resulting in distinct effect sizes. However, the observed moderate heterogeneity among studies indicates variability in outcomes, necessitating further investigation into the potential underlying mechanisms and differences in study designs.
Most previous studies on CET have focused primarily on physiological outcomes such as muscle strength, hypertrophy, cardiovascular endurance, and metabolic health,30,42 while giving less attention to its effects on neurocognitive adaptations. 17 Our pooled analysis indicates that CET is effective for improving global cognition. However, the heterogeneity (I2 = 67%) may be attributed to variations in training protocols, statistical methods, participant characteristics, and study designs. Subgroup analyses indicated that CET significantly affected both populations with physiological disorders and those experiencing neurocognitive decline, although the latter exhibited moderate heterogeneity (I2 = 41%). This variability may be due to differences in the severity of cognitive impairment among participants. For instance, 2 studies involving participants with both MCI and AD may introduce variability in the magnitude of cognitive gains, as people with more advanced neurodegenerative conditions (e.g., AD and dementia) may experience more limited benefits.22,59
CET exerts beneficial effects on cognition that may be explained by various neurobiological processes that warrant further investigation. The neurocognitive benefits of endurance and resistance training are mediated by distinct mechanisms. For instance, aerobic exercise is associated widely with increased cerebral blood flow,9,65,72 as well as upregulation of BDNF,51,69 which plays a critical role in neurogenesis and plasticity.8,20,52,71 Resistance training was linked to metabolic regulation (e.g., IGF-1 pathways) and systemic inflammation reduction.5,38,70 Nevertheless, the interaction between these 2 modalities in a CET program remains poorly understood.
The observed cognitive benefits are attributed more plausibly to synergistic increases in neurotrophic factors, cerebral perfusion, and task-specific motor learning than to competition for limited cognitive resources. These findings consistent with findings by Hertzog et al, 27 who reported greater gains from cognitive interventions among those with lower cognitive baselines.10,16,45 Furthermore, this finding aligns with the cognitive reserve hypothesis,16,61 which posits that people with lower cognitive reserve may exhibit greater adaptability and neuroplasticity in response to exercise interventions.62,74 This hypothesis further underscores the importance of sustained engagement in cognitive and physical activities. Indeed, prolonged exercise interventions, lasting from 6 to 92 weeks in the included studies, appear to enhance cognitive reserve over time, potentially protecting against cognitive decline during follow-up. Consequently, for patients with lower cognitive function, CET may represent an effective, low-risk, and cost-efficient intervention to enhance cognition in these vulnerable populations.
Another possible explanation is that exercise order may influence cognitive outcomes by modulating the acute stress response or resource allocation during exercise.6,68 For instance, performing resistance exercise before aerobic training may prioritize neuromuscular adaptations or exercise-induced arousal. 32 In a recent 24-week RCT involving older adults with MCI, Lautenschlager et al 35 observed significant cognitive improvements when aerobic and resistance components were performed sequentially, without evidence of interference. Conversely, an acute crossover study by Timmons et al 67 reported attenuated serum BDNF elevation when resistance exercise immediately preceded cycling. A 2025 meta-analysis of 35 RCTs with human participants further concluded that overall concurrent training significantly enhances global cognition (g = 0.32; 95% CI, 0.17-0.46), but insufficient data precluded firm conclusions on order-dependent effects.78,80 Thus, the hypothesis that subsequent resistance exercise ‘diminishes’ aerobic-induced brain plasticity remains speculative in humans and requires targeted trials.
The impact of exercise order in CET on physiological adaptations in elite athletes has been investigated extensively in the field of sports science.18,42 However, knowledge regarding the effects of CET on cognitive neuroadaptations remains limited. Current evidence comprises only 1 study involving animal models, 33 which demonstrated that strength training impaired the increases in β-hydroxybutyric acid and BDNF mRNA levels induced by aerobic exercise. This underscores that the order in which aerobic and strength exercises are performed may influence cognitive adaptation; however, further research is necessary to elucidate this mechanism. This area represents a promising direction for future research aimed at optimizing programs, where neuroimaging and biomarker studies could illuminate the specific pathways involved in the impact of CET on cognition.
Limitations and Future Directions
Although the findings of this meta-analysis are interesting, several limitations must be acknowledged. First, heterogeneity remains an uncertainty despite efforts to conduct subgroup analyses, and the order of exercise modalities was not reported consistently across studies, limiting the ability to fully explore its role as a moderator. In addition, all studies included participants with cognitive decline or physiological conditions, which may restrict the generalizability of the findings to healthy older adults. Finally, publication bias was not detected, but it remains a potential concern, especially given the relatively small number of high-quality RCTs in certain subgroups. Given the moderate heterogeneity observed, future research should aim to standardize exercise protocols and explore the mechanistic pathways underlying cognitive improvements. Future meta-analyses should consider more homogeneous populations or further refine subgroup analyses to better understand these differences.
Conclusion
This meta-analysis provides evidence that CET can improve global cognition in middle-aged and elderly populations with clinical conditions, compared with both active and passive control conditions. Significant diversity in study designs and populations underlies the observed heterogeneity. Importantly, our review highlights the need for further research into the neurological mechanisms underlying human concurrent training and suggests that incorporating CET programs into rehabilitation or preventative care for populations with neurocognitive and physiological disorders could potentially enhance overall health and delay cognitive decline.
Supplemental Material
sj-docx-1-sph-10.1177_19417381261451825 – Supplemental material for Effects of Concurrent Strength and Aerobic Exercise Training on Cognitive Health in Adults With Physiological or Neurocognitive Disorders: Systematic Review With Meta-analysis of Randomized Controlled Trials
Supplemental material, sj-docx-1-sph-10.1177_19417381261451825 for Effects of Concurrent Strength and Aerobic Exercise Training on Cognitive Health in Adults With Physiological or Neurocognitive Disorders: Systematic Review With Meta-analysis of Randomized Controlled Trials by Mingyang Zhang, Ruixiang Yan, Lijie Lou, Kailin Wu, Junyi Bian, Duanying Li and Jian Sun in Sports Health
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.