
Abstract
Context:
Visual training (VT) is used increasingly in sports rehabilitation to enhance visuomotor integration after lower extremity injuries. However, its effectiveness in improving balance and functional recovery remains unclear, with inconsistent findings across studies.
Objective:
To determine whether VT improves balance control and functional recovery in people with lower extremity injuries compared with standard rehabilitation or other active controls.
Data Sources:
Eight databases (PubMed, Web of Science, Embase, Scopus, MEDLINE, CINAHL, SPORTDiscus, and Cochrane Library) were searched from inception to September 17, 2025.
Study Selection:
Randomized controlled trials (RCTs) evaluating VT as the primary intervention and reporting balance- or function-related outcomes were included. Of 1186 records screened, 18 RCTs (n = 707) met eligibility criteria.
Study Design:
Systematic review and meta-analysis of RCTs.
Level of Evidence:
Level 1.
Data Extraction:
Data on participant characteristics, intervention protocols, balance outcomes (static and dynamic), and functional outcomes (subjective function, physical function, sport performance) were extracted.
Results:
VT improved static balance significantly (standardized mean difference [SMD] = 0.46; 95% CI, 0.10-0.81; P = 0.01) and dynamic balance (SMD = 0.88; 95% CI, 0.31-1.44; P = 0.002). No significant effects were found for subjective functional recovery, physical function, or sport performance. Larger effects were observed in men, chronic ankle instability populations, and with stroboscopic VT.
Conclusion:
VT may provide meaningful benefits for balance rehabilitation after lower extremity injuries, especially for dynamic balance. However, it does not enhance subjective function, physical function, or sport performance significantly. Despite its potential as an adjunct to rehabilitation, overall certainty of evidence is very low, highlighting the need for high-quality RCTs with standardized protocols.
With the widespread participation in both elite and recreational sports, lower extremity injuries remain one of the most prevalent and severe types of sports-related injuries.72,75 Numerous epidemiological studies have demonstrated that the lower extremities, particularly the ankle and knee, play a predominant role in sports-related injuries. For instance, acute ankle sprains account for approximately 15% of all sports injuries among collegiate athletes in the United States. 30 In basketball, lower-limb injuries constitute 63.7% of all reported cases, with ankle injuries alone comprising 21.9%. 6 Moreover, structural knee injuries, such as ligament and cartilage damage, are also common, with an incidence rate ranging up to 21% in certain athletic populations. 67 Lower-limb injuries not only result in decreased athletic performance and interruption of training and competition but also frequently lead to long-term functional deficits. Some studies have indicated that these deficits are associated primarily with impairments in balance control and proprioceptive function,42,46 both of which are critical for athletes’ successful return to sport and for preventing reinjury.2,10 Without effective intervention, residual balance deficits after injury may increase the risk of reinjury substantially, creating a vicious cycle that not only impairs athletic performance but also reduces quality of life and potentially compromises career longevity. Therefore, enhancing balance control and functional recovery during rehabilitation has become a critical focus in sports medicine and rehabilitation research.
Conventional rehabilitation approaches focus typically on restoring muscle strength, improving joint range of motion, and rebuilding fundamental functional movements. These methods have shown certain effectiveness in enhancing joint stability and basic motor function.50,76 However, an increasing number of studies have revealed that conventional rehabilitation methods are often limited in addressing the complex sensorimotor deficits that occur after injury.70,74 This limitation may stem, to some extent, from the fact that traditional rehabilitation training fails to fully account for the synergistic interaction among multiple sensory systems involved in motor control. Postural control and dynamic stability during movement rely on the coordinated integration of multiple sensory systems, including vision, vestibular input, and proprioception. 12 When injury occurs, proprioceptive pathways may be disrupted, leading to deficits in joint position sense, kinesthesia, and force perception. 4 Under such circumstances, visual information becomes increasingly important for maintaining postural and movement stability. Consequently, people tend to rely more heavily on visual input for motor control after injury, providing new insights for rehabilitation interventions.
In recent years, with the advancement of rehabilitation science and motor neuroscience, visual training (VT) has increasingly attracted the attention of researchers and clinical practitioners.24,39 VT refers to a category of interventions that use targeted visual stimuli and task-specific training to enhance visual processing efficiency and visuomotor integration, thereby supporting sensorimotor coupling.7,43 The primary forms of VT include visual coordination training,1,39 stroboscopic vision training,41,68 and visual tasks performed in virtual reality environments.62,63 The core concept of VT lies in strengthening the visual system to optimize its role in motor control and functional performance, particularly to compensate for sensory deficits resulting from impaired proprioceptive or vestibular input.13,52
Existing research has provided encouraging evidence supporting the application of VT in the field of rehabilitation. Several trials have demonstrated that implementing VT among people with lower-limb injuries can significantly improve postural stability, enhance dynamic balance, and yield favorable outcomes in functional performance tests.24,38 The underlying mechanism involves primarily improving multisensory integration efficiency through training, thereby promoting better coordination among visual, proprioceptive, and vestibular inputs. In addition, VT enhances anticipatory postural adjustments, enabling people to perform more effective feedforward control during movement. Moreover, it strengthens the functional connectivity between visual processing areas and motor control networks in the brain, thereby facilitating motor function recovery at the neural level. 54 However, some studies have reported considerable inconsistencies in findings and conclusions: while certain research has demonstrated significant benefits of VT on balance and functional recovery, 25 others have shown limited, or even nonsignificant, effects. These discrepancies may stem from methodological variations, including differences in participant characteristics, intervention protocols, outcome measures, and parameters such as training frequency and duration. Furthermore, there is still no consensus on the optimal VT implementation protocol, including aspects such as intervention duration, frequency, session length, and specific training formats. This high degree of heterogeneity not only fuels ongoing debate among researchers but also leaves clinical practice without clear evidence-based guidance for the application of VT.
To date, no systematic review or meta-analysis has focused specifically on the effects of VT on balance and functional recovery during rehabilitation after lower-limb injuries. Existing reviews are often restricted to specific injury types or single populations, or emphasize primarily emerging technologies such as virtual and augmented reality, while lacking a systematic synthesis of evidence regarding VT in broader lower-limb injury populations.46,64,66,69 Therefore, this study aims to conduct a meta-analysis to evaluate the effects of VT on rehabilitation outcomes in people with lower-limb injuries. As an emerging rehabilitation intervention, VT holds considerable theoretical value and practical potential; however, evidence regarding its efficacy and optimal application remains insufficient. This study not only addresses the limitations of existing reviews concerning VT but also provides more targeted evidence-based insights into balance and functional recovery among people with lower-limb injuries, thereby advancing the development of sports medicine and rehabilitation in the domains of visuomotor integration and functional recovery.
Methods
This review followed the methodological guidance of the Joanna Briggs Institute for systematic reviews and was prepared in line with the updated Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 checklist (Supplementary Appendix 1, available in the online version of this article). 55 The protocol has been registered prospectively in PROSPERO (ID: CRD420251141343).
Search Strategy
A systematic search of the literature was undertaken to identify studies exploring how VT influences balance and functional recovery after lower extremity injuries. Searches were carried out in several major electronic databases, including PubMed, Web of Science (Core Collection), Embase, Scopus, MEDLINE, CINAHL, SPORTDiscus, and Cochrane Library covering all available years up to September 17, 2025. The strategy incorporated both subject headings and free-text keywords, combining terms for VT methods with those describing lower extremity injuries, and Boolean operators were used to optimize both recall and precision.
Keywords for VT included a wide spectrum of intervention-related terms (such as “visual training,” “perceptual training,” “eye training,” “vision training,” “visual skill* training,” “visuomotor training,” “visual motor training,” “perceptual skill* training,” “perceptual-cognitive training,” “visual-perceptual training,” “visual enhancement,” “vision improvement,” “ocular training,” “visual exercise*,” “video-based training,” “temporal occlusion training,” “strobe training,” “stroboscopic training,” “virtual reality training,” “VR training,” “visual-spatial training,” “visual search training,” and “multiple object tracking training”). These were combined with injury-related terms (e.g., “sports injury,” “athletic injury,” “exercise-related injury,” “musculoskeletal injury,” “musculoskeletal trauma,” “sports trauma,” “orthopedic injury,” “lower extremity injury,” “lower extremity trauma,” “lower extremity disorder,” “lower limb injury,” “lower limb trauma,” “leg injury,” “leg trauma,” “hip injury,” “hip fracture,” and “hip dislocation”). The complete search formula is reported in Supplemental Appendix 2, available online.
In addition, the reference lists of all included studies and related reviews were screened manually to capture potentially overlooked articles.46,64,66,69 Only English-language papers published in peer-reviewed journals were considered eligible. Duplicates were removed using EndNote software (Version 20.5, Clarivate Analytics). Two reviewers assessed titles and abstracts independently according to predefined criteria, and any discrepancies were resolved through discussion with a third investigator. Full-text articles were retrieved for all studies judged potentially relevant. If the full manuscript could not be obtained, the corresponding author was contacted directly. The overall flow of study selection is illustrated in Figure 1.
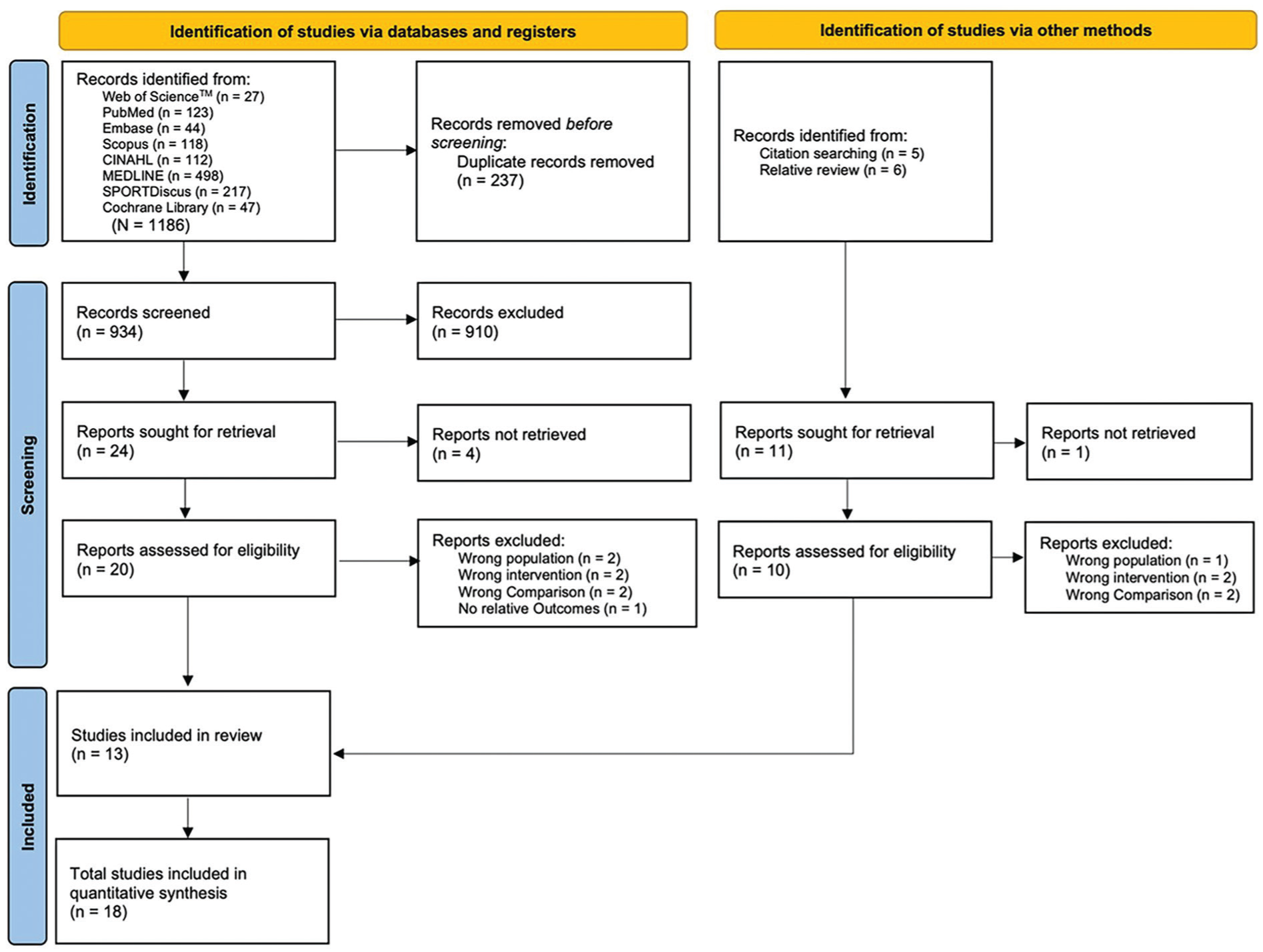
PRISMA flowchart of search process. PRISMA, preferred reporting items for systematic reviews and meta-analyses
Inclusion and Exclusion Criteria
Inclusion and exclusion criteria were established using a revised population, intervention, comparison, and outcome (PICOS) framework. 5 Studies were included if they met the following criteria:
Type of Population
The target population focused on athletes and people with lower extremity musculoskeletal injuries, such as chronic ankle instability (CAI), anterior cruciate ligament (ACL) reconstruction (ACLR), functional ankle instability (FAI), ankle sprain, and Achilles tendon rupture. 48 Considering the maturation of visual development and the potential decline in visual function with aging, participants were restricted to an age range of 10 to 60 years. 26 There were no restrictions on sex or athletic experience, allowing findings to be generalized across a broad athletic population. Studies were excluded if they involved nonsports related disorders (e.g., congenital neurological or ophthalmological diseases, stroke, Parkinson’s disease) or healthy populations without a history of injury.
Type of Intervention
The intervention was VT aimed at enhancing perceptual, visuomotor, or cognitive functions. 43 Eligible interventions included, but were not limited to, visuomotor coordination training, stroboscopic or temporal occlusion training, video-based training, virtual reality programs, and multiple object tracking. 7 Interventions could be delivered alone or in combination with standard rehabilitation programs, provided that VT was the primary experimental component. Studies were excluded if the intervention did not include a clearly defined VT protocol, if VT was only a minor component of a multimodal program without separate analysis, or if the intervention targeted unrelated domains (e.g., purely strength or cardiovascular training without a visual component).
Type of Comparison
Eligible comparisons included control groups receiving standard rehabilitation, sham or placebo interventions, or no additional treatment beyond usual care. Studies comparing VT with alternative nonvisual-training methods (e.g., balance training, or general physical therapy) were also included, provided that VT was the primary intervention under investigation. Trials without a comparator group or those in which both arms received VT-based interventions were excluded.
Type of Outcome
Eligible studies were required to report at least 1 quantitative outcome related to balance or functional recovery after lower extremity injuries. Balance outcomes referred to measures of static and dynamic postural control, including single-leg stance tests, force plate assessments such as center-of-pressure sway, and functional balance tasks such as the star excursion balance test and Y-balance test. 45 Functional recovery outcomes were further subdivided into 3 domains: (1) subjective functional recovery, assessed by validated clinical functional scales such as the IKDC, Lysholm, and FAAM 77 ; (2) physical functional recovery, including proprioception measures such as coordination tests 34 ; and (3) sport performance, evaluated through performance-based motor tests such as hop tests, agility tests, and sport skill assessments. 59 Studies that assessed only unrelated domains, such as isolated visual acuity without motor components, purely cognitive outcomes, or general fitness measures, were excluded.
Type of Study Design
Only randomized controlled trials (RCTs) were eligible for inclusion, as they provide the highest level of evidence for evaluating intervention effectiveness. All other study designs, including quasi-experimental studies, cohort studies, case-control studies, case reports, conference abstracts, and reviews, were excluded.
Data Extraction Procedures
Two reviewers extracted all relevant data independently using a tailored Excel sheet (Microsoft Corp). Discrepancies between the 2 reviewers were addressed through detailed discussion; if consensus could not be achieved, a third reviewer adjudicated to reach a final decision. The extracted dataset encompassed the following categories: (1) study identification—including the authors’ name, year of publication; (2) participant characteristics—including sample size, sex distribution, age (means and standard deviations), and injury type; (3) group allocation—sample size in each intervention and control group, as well as the number of groups per study; (4) intervention characteristics—type of training (e.g., virtual reality, stroboscopic), frequency of sessions, duration of each session, and total intervention length; (5) testing characteristics—including the outcome domains assessed, specific measurement tools (e.g., star excursion balance test, Y-balance test, joint position sense error, hop tests); (6) outcome data—pre- and postintervention results expressed as mean values and measures of variability (standard deviation or standard error), absolute or relative changes, and, where reported, statistical significance levels and effect sizes.
Risk of Bias and Certainty of Evidence
The risk of bias for randomized controlled trials was assessed independently by 2 reviewers using the revised Cochrane risk-of-bias tool for randomized trials (RoB Version 2.0). 65 The following 5 domains were evaluated: (1) bias arising from the randomization process; (2) bias due to deviations from intended interventions; (3) bias due to missing outcome data; (4) bias in measurement of the outcome; and (5) bias in selection of the reported result. Each domain was judged as “low risk of bias,” “some concerns,” or “high risk of bias,” leading to an overall risk-of-bias judgment for each study. Discrepancies between reviewers were resolved through discussion, and unresolved disagreements were adjudicated by a third reviewer.
In addition, the certainty of evidence across outcomes was appraised using the Grading of Recommendations Assessment, Development and Evaluation (GRADE) framework,27,61 considering risk of bias, inconsistency, indirectness, imprecision, and publication bias. Evidence quality was classified into 4 levels: high, moderate, low, or very low certainty.
Statistical Analysis
Effect Size Calculation
To evaluate the effectiveness of VT on balance and function recovery, effect sizes were expressed as standardized mean differences (SMDs) with 95% CIs to ensure comparability across studies employing different measurement tools. Hedges’ g correction was applied to reduce potential small-sample bias. 28 To quantify intervention effects, the mean difference of pre-post changes between intervention and control groups (MDdiff) was calculated, along with the corresponding standard deviation of the difference (SDdiff). The SDdiff was determined using established formulas that incorporate the within-subject correlation (Corr) between pre- and post-test scores. When Corr values were not reported explicitly, they were either derived through correlation analysis of raw data or obtained by contacting the original study authors. If these approaches were not feasible, a conservative Corr of 0.5 was assumed, as recommended by the Cochrane Handbook, 18 to balance potential under- or overestimation of variability.
For studies reporting multiple related outcomes within the same construct (e.g., the 3 reach directions of the star excursion balance test), these were first aggregated into a single effect size by averaging their means and calculating a pooled standard deviation, assuming a correlation of 0.5 among outcomes. 11 This combined estimate was then entered into the meta-analysis to avoid unit-of-analysis errors. In trials comparing multiple intervention groups against a shared control, the sample size of the common comparator group was divided evenly across comparisons to prevent double counting and to maintain statistical independence.31,57 In this meta-analysis, SMDs were calculated as Hedges’ g, which represents a bias-corrected SMD. Hedges’ g values were classified as small (< 0.50), medium (0.50-0.80), and large (≥0.80). 29
Meta-Analyses and Heterogeneity Testing
The meta-analysis and data visualization were conducted using the “meta” and “metafor” packages in R software (Version 4.3.3, R Core Team). A conventional 2-level meta-analysis approach was applied within a random-effects framework, estimated with the DerSimonian-Laird method. 20 The random-effects model assumes that study-specific effect sizes are sampled from a distribution of true effects rather than a single common value, thereby incorporating between-study heterogeneity and yielding more generalizable pooled estimates. 18 A positive effect size indicated greater improvements in the intervention group compared with the control group.
Heterogeneity was evaluated using the I2 statistic and the Cochrane Q (chi-squared) test. The degree of heterogeneity, as indicated by I2, was categorized as low (<25%), moderate (25% to 50%), high (50% to 75%), or considerable (≥75%) in accordance with established guidelines. 32 A P value of <0.10 for the Q test was taken to suggest statistically significant heterogeneity.
Subgroup Analysis and Meta-Regression
Subgroup analyses were performed to explore potential sources of heterogeneity. The χ² test was used to compare effect sizes between the following categorical variables: (1) intervention type; (2) participant characteristics, and (3) injury type (ACLR vs CAI vs other injuries).
Meta-regressions were performed to explore the influence of potential continuous moderators on the effects of VT interventions on primary outcomes. The following moderator analyses were explored: (1) intervention duration (weeks), (2) training frequency (sessions per week), and (3) session length (minutes per session). Meta-regression analyses were conducted only when >10 studies were available for inclusion. 23
Publication Bias Assessment and Sensitivity Analysis
Potential publication bias was examined through the use of contour-enhanced funnel plots, 56 supplemented by Egger’s regression test when ≥10 studies were available for analysis. 21 A nonsignificant result (P > 0.05) from Egger’s test was interpreted as an absence of substantial publication bias. These complementary procedures provided both a visual and a quantitative means of evaluating asymmetry in effect size distributions, thereby enhancing confidence in the reliability of the pooled estimates.
To assess the robustness of the findings, a sensitivity analysis was performed using a leave-one-out approach. In this procedure, each study was removed sequentially from the meta-analysis to assess whether any single study exerted a disproportionate influence on the overall effect size. Stability of the pooled estimates across these iterations was interpreted as evidence of the reliability of the synthesized findings.
Results
Study Selection and Characteristics
A total of 1186 records were identified through electronic database searching: Web of Science (n = 27), PubMed (n = 123), Embase (n = 44), Scopus (n = 118), CINAHL (n = 112), MEDLINE (n = 498), SPORTDiscus (n = 217), and Cochrane Library (n = 47). After removal of 279 duplicates, 907 records remained for title and abstract screening. Of these, 883 records were excluded as they did not meet the eligibility criteria. Four full-texts could not be retrieved despite extensive searching. Subsequently, 20 full-text articles were assessed for eligibility, of which 9 were excluded for reasons such as irrelevant population, inappropriate intervention, absence of relevant outcomes, or 2-arm VT intervention design. In addition, 11 records were identified from other sources. After screening, 5 studies met the eligibility criteria. Finally, 18 RCTs fulfilled the inclusion criteria and were included in the final analysis (Figure 1).
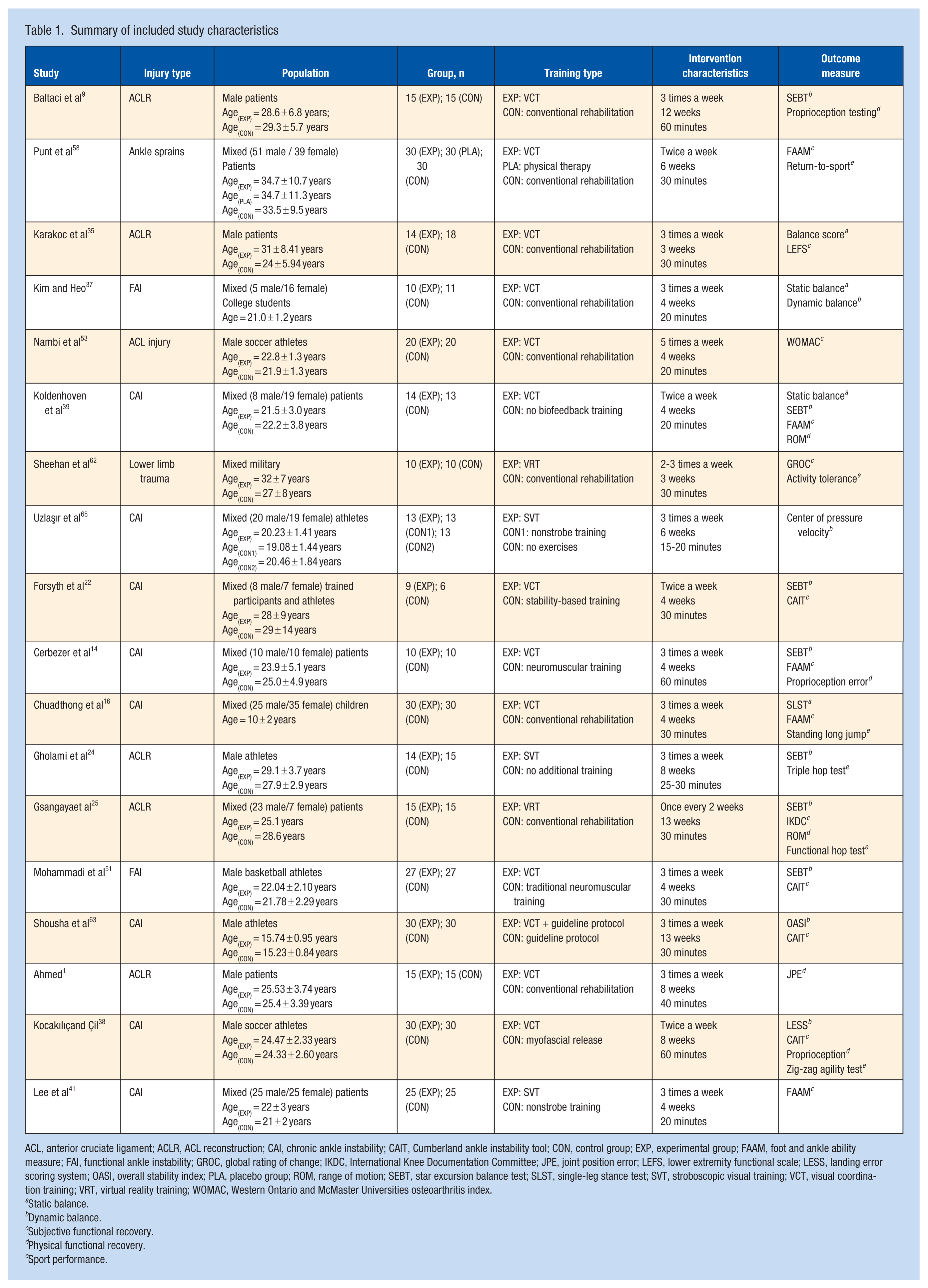
Of the RCTs, 18 were published between 2013 and 2024, involving participants with a range of sports-related lower-limb injuries, including ACL injuries,1,9,24,25,35,53 CAI,14,16,22,38,39,41,63,68 FAI,37,51 ankle sprains, 58 and lower limb trauma. 62 Across all studies, a total of 707 participants were enrolled. The study populations consisted of ordinary patients,1,9,14,16,25,35,39,41,58 competitive athletes,22,24,38,51,53,63,68 college students, 37 and military personnel, 62 with both male-only and mixed-gender cohorts. Participant age ranged from 10 years in pediatric cohorts to approximately 32 years in adult athletic or patient groups, with group sample sizes varying from 15 to 90 participants.
The majority of interventions (13 trials) employed visual coordination training,1,9,14,16,22,35,37 -39,51,54,58,63 whereas 3 trials applied stroboscopic visual training,24,41,68 and the other 2 trials implemented virtual reality training.25,62 Control groups typically received conventional rehabilitation, neuromuscular or stability-based training, or no additional training. The intervention protocols varied considerably, with frequencies ranging from once every 2 weeks to 5 sessions per week, durations spanning from 3 to 13 weeks, and session lengths between 15 and 60 minutes. The detailed characteristics of the included studies are presented in Table 1.
Summary of included study characteristics
ACL, anterior cruciate ligament; ACLR, ACL reconstruction; CAI, chronic ankle instability; CAIT, Cumberland ankle instability tool; CON, control group; EXP, experimental group; FAAM, foot and ankle ability measure; FAI, functional ankle instability; GROC, global rating of change; IKDC, International Knee Documentation Committee; JPE, joint position error; LEFS, lower extremity functional scale; LESS, landing error scoring system; OASI, overall stability index; PLA, placebo group; ROM, range of motion; SEBT, star excursion balance test; SLST, single-leg stance test; SVT, stroboscopic visual training; VCT, visual coordination training; VRT, virtual reality training; WOMAC, Western Ontario and McMaster Universities osteoarthritis index.
Static balance.
Dynamic balance.
Subjective functional recovery.
Physical functional recovery.
Sport performance.
According to the RoB 2 tool, none of the 18 included trials was judged to be at overall low risk of bias (Supplementary Appendix 3, available online); 7 studies (39%) were rated as having a high overall risk of bias, while the remaining 11 studies (61%) were rated as having “some concerns.” The primary driver of high-risk judgments was missing outcome data (D3), due particularly to high attrition rates or imbalanced dropout between groups. In some studies, inadequate randomization procedures (D1) or the presence of “some concerns” across multiple domains also led to high overall risk ratings. With respect to randomization (D1), only 8 studies were judged as low risk, whereas the majority were downgraded due to insufficient information on allocation concealment. For deviations from intended interventions (D2), nearly all trials were rated as “some concerns,” reflecting the inherent difficulty of blinding participants and therapists in rehabilitation interventions. Measurement of outcomes (D4) was typically low risk when objective tools were used, but “some concerns” were noted when outcomes relied on self-reported scales or when assessor blinding was not specified. For selective reporting (D5), 15 studies were rated as “some concerns,” due largely to the lack of prospective trial registration or protocol-analysis consistency. Overall, the body of evidence demonstrated notable methodological limitations, particularly in handling missing data and ensuring transparency in outcome reporting, which should be considered when interpreting and generalizing the findings.
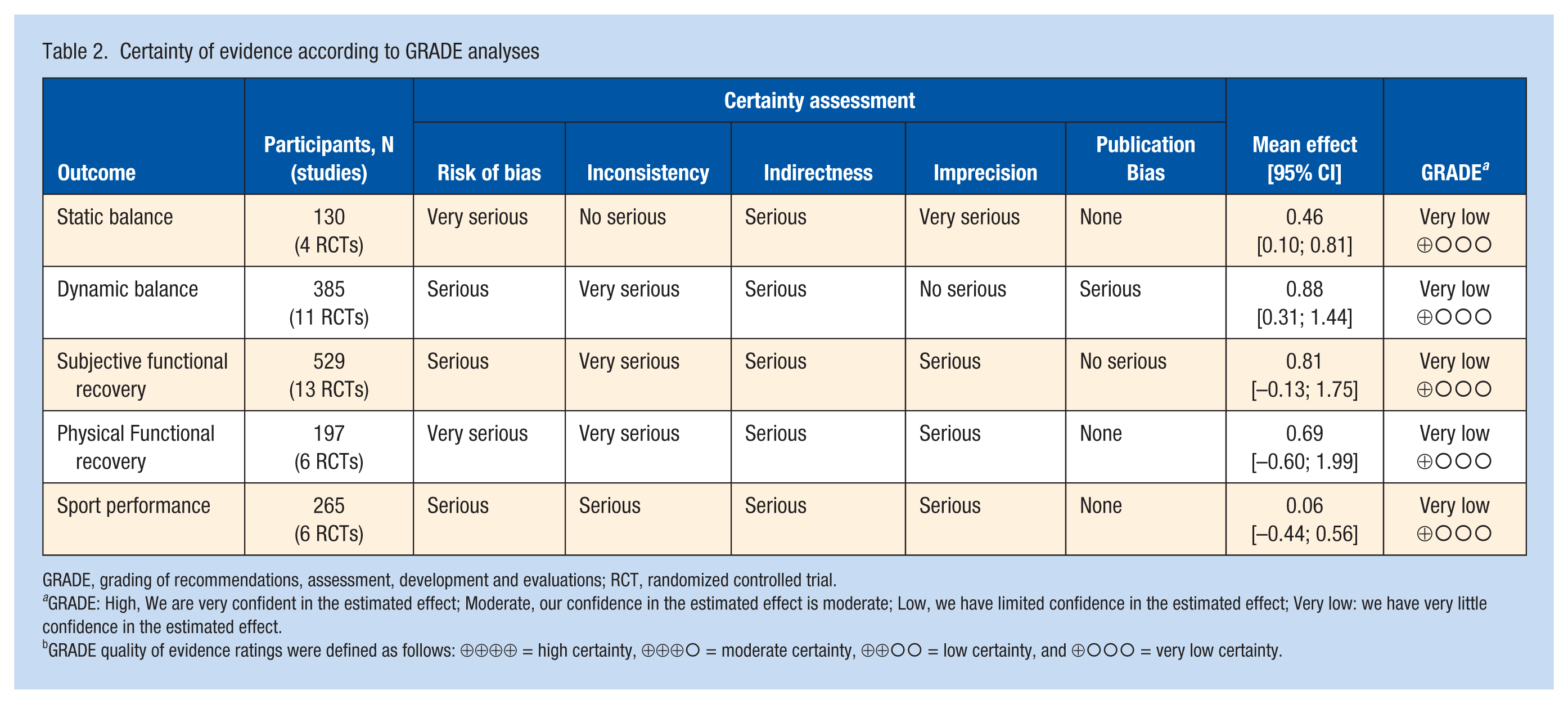
According to the GRADE assessment (Table 2), the certainty of evidence for all 5 outcomes was rated as very low, due primarily to high risk of bias, inconsistency across studies, indirectness of evidence, and imprecision of effect estimates. For static balance, the certainty was downgraded primarily due to very serious risk of bias and imprecision, reflecting the small number of included trials (n = 4) and limited sample sizes, despite low statistical heterogeneity (I2 = 0%). In contrast, for dynamic balance, the very low certainty was driven mainly by very serious inconsistency, as evidenced by substantial heterogeneity across studies (I2 = 84%), despite a larger body of evidence (n = 11). For subjective functional recovery, although a moderate number of trials were included, the certainty was downgraded due to very serious inconsistency and indirectness, as the outcome measures varied considerably and may not fully capture overall functional recovery. Similarly, the evidence for physical functional recovery and sport performance was downgraded because of a combination of serious risk of bias, inconsistency, indirectness, and imprecision, further limiting confidence in the estimated effects.
Certainty of evidence according to GRADE analyses
GRADE, grading of recommendations, assessment, development and evaluations; RCT, randomized controlled trial.
GRADE: High, We are very confident in the estimated effect; Moderate, our confidence in the estimated effect is moderate; Low, we have limited confidence in the estimated effect; Very low: we have very little confidence in the estimated effect.
GRADE quality of evidence ratings were defined as follows: ⊕⊕⊕⊕ = high certainty, ⊕⊕⊕○ = moderate certainty, ⊕⊕○○ = low certainty, and ⊕○○○ = very low certainty.
Meta-Analyses
Regarding the effects of VT on static balance (Figure 2), 4 studies comprising 4 intervention groups and a total of 130 participants were included. The meta-analysis revealed a statistically significant improvement (SMD = 0.46; 95% CI, 0.10-0.81; I2 = 0%; P = 0.01), indicating a small-to-modest effect size. Low heterogeneity was observed. Egger’s test indicated no publication bias in the primary pooled effect size (P = 0.51), supported by symmetry in the funnel plot (Figure 7a). Sensitivity analysis confirmed the robustness of the pooled estimate (Supplementary Appendix Figure 4.1, available online).
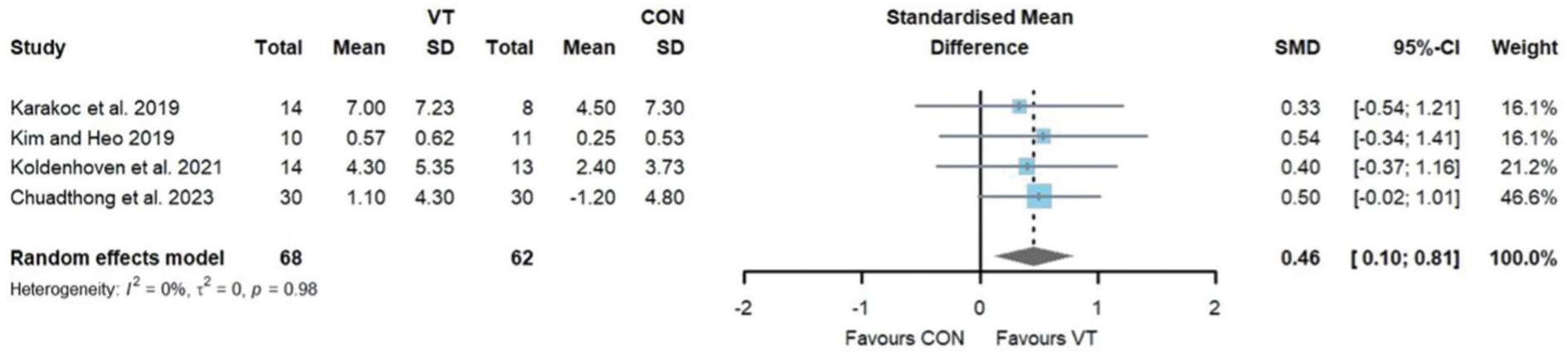
Forest plots depicting the total effect size on static balance. CON, control; VT, visual training.
Regarding the effects of VT on dynamic balance (Figure 3), 11 studies comprising 12 intervention groups and a total of 385 participants were included. The meta-analysis revealed a statistically significant improvement (SMD = 0.88; 95% CI, 0.31-1.44; I2 = 84%; P = 0.002), indicating a moderate-to-large effect size. Considerable heterogeneity was observed. Egger’s test indicated no publication bias in the primary pooled effect size (P = 0.78), supported by symmetry in the funnel plot (see Figure 7b). Sensitivity analysis confirmed the robustness of the pooled estimate (Supplementary Appendix Figure 4.2, available online).
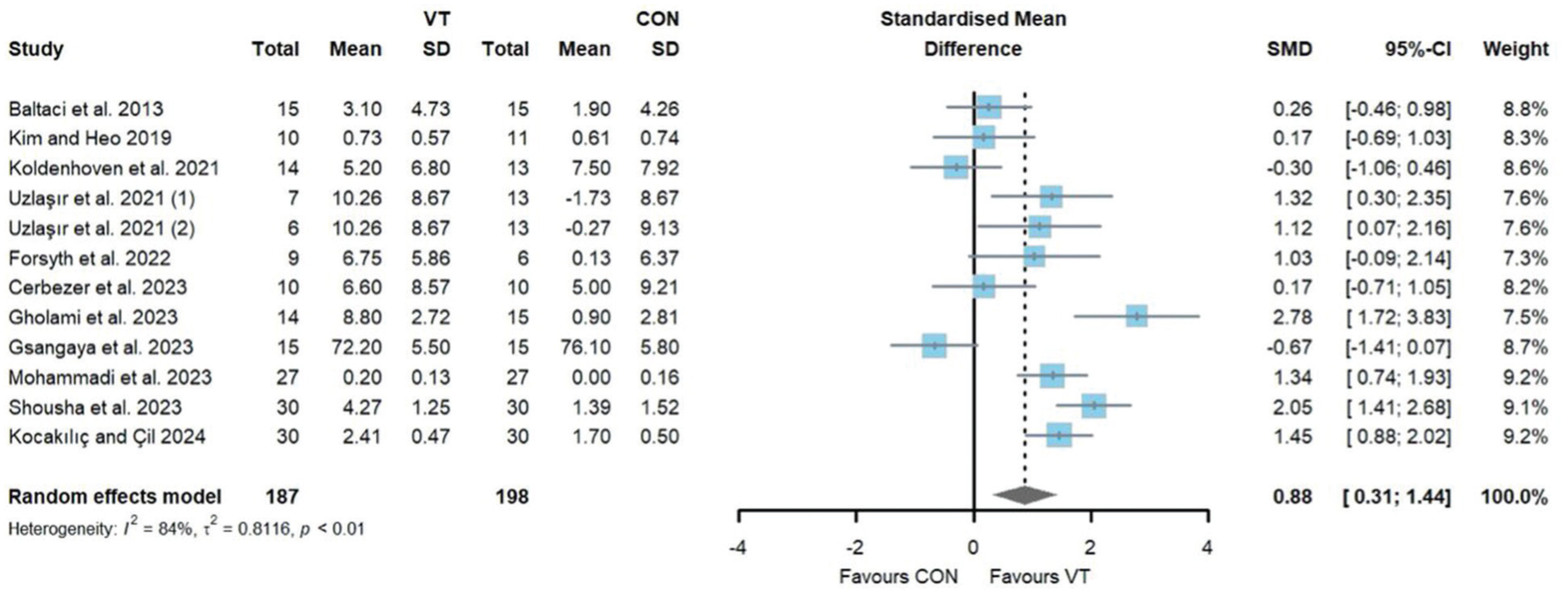
Forest plots depicting the total effect size on dynamic balance. CON, control; VT, visual training.
Regarding the effects of VT on subjective functional recovery (Figure 4), 13 studies comprising 14 intervention groups and a total of 529 participants were included. The meta-analysis revealed no statistically significant improvement (SMD = 0.81; 95% CI, –0.13 to 1.75; I2 = 89%; P = 0.09). Considerable heterogeneity was observed. Egger’s test indicated no publication bias in the primary pooled effect size (P = 0.25), supported by symmetry in the funnel plot (see Figure 7c). Sensitivity analysis confirmed the robustness of the pooled estimate (Supplementary Appendix Figure 4.3, available online).
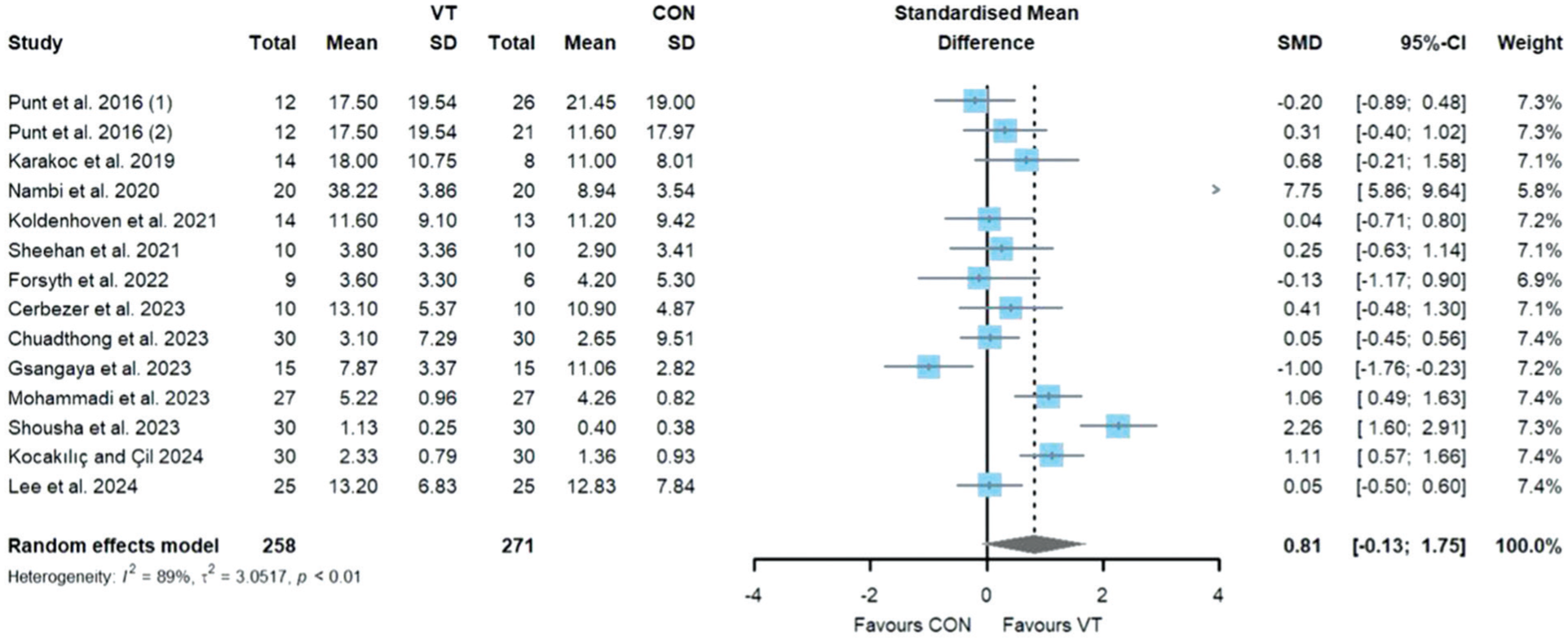
Forest plots depicting the total effect size on subjective functional recovery. CON, control; VT, visual training.
Regarding the effects of VT on physical functional recovery (Figure 5), 6 studies comprising 6 intervention groups and a total of 197 participants were included. The meta-analysis revealed no statistically significant improvement (SMD = 0.69; 95% CI, –0.60 to 1.99; I2 = 89%; P = 0.29). Considerable heterogeneity was observed. Egger’s test indicated no publication bias in the primary pooled effect size (P = 0.98), but the funnel plot showed slight asymmetry with a tendency toward the right side (see Figure 7d). Sensitivity analysis confirmed the robustness of the pooled estimate (Supplementary Appendix Figure 4.4, available online).
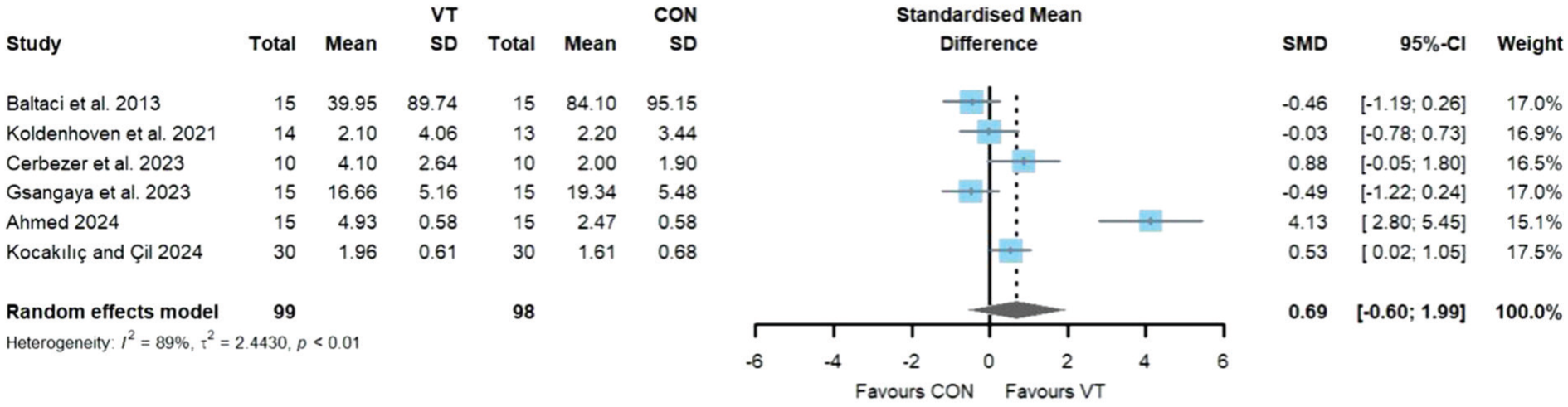
Forest plots depicting the total effect size on physical functional recovery. CON, control; VT, visual training.
Regarding the effects of VT on sport performance (Figure 6), 6 studies comprising 7 intervention groups and a total of 265 participants were included. The meta-analysis revealed no statistically significant improvement (SMD = 0.06; 95% CI, –0.44 to 0.56; I2 = 71%; P = 0.81). High heterogeneity was observed. Egger’s test indicated no publication bias in the primary pooled effect size (P = 0.91), supported by symmetry in the funnel plot (Figure 7e). Sensitivity analysis confirmed the robustness of the pooled estimate (Supplementary Appendix Figure 4.5, available online).
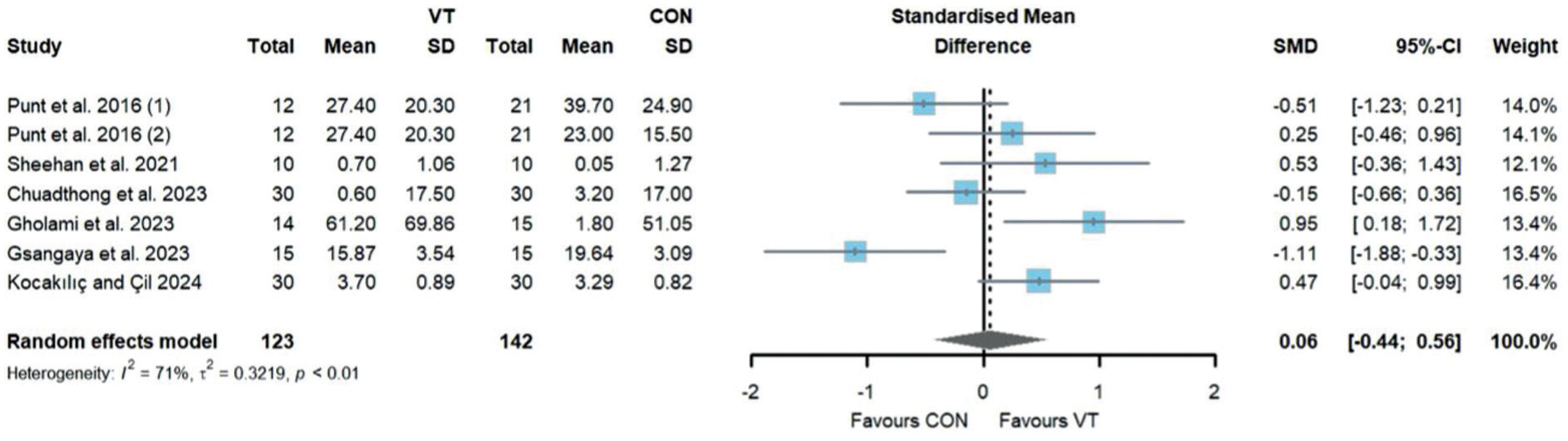
Forest plots depicting the total effect size on sport performance. CON, control; VT, visual training.
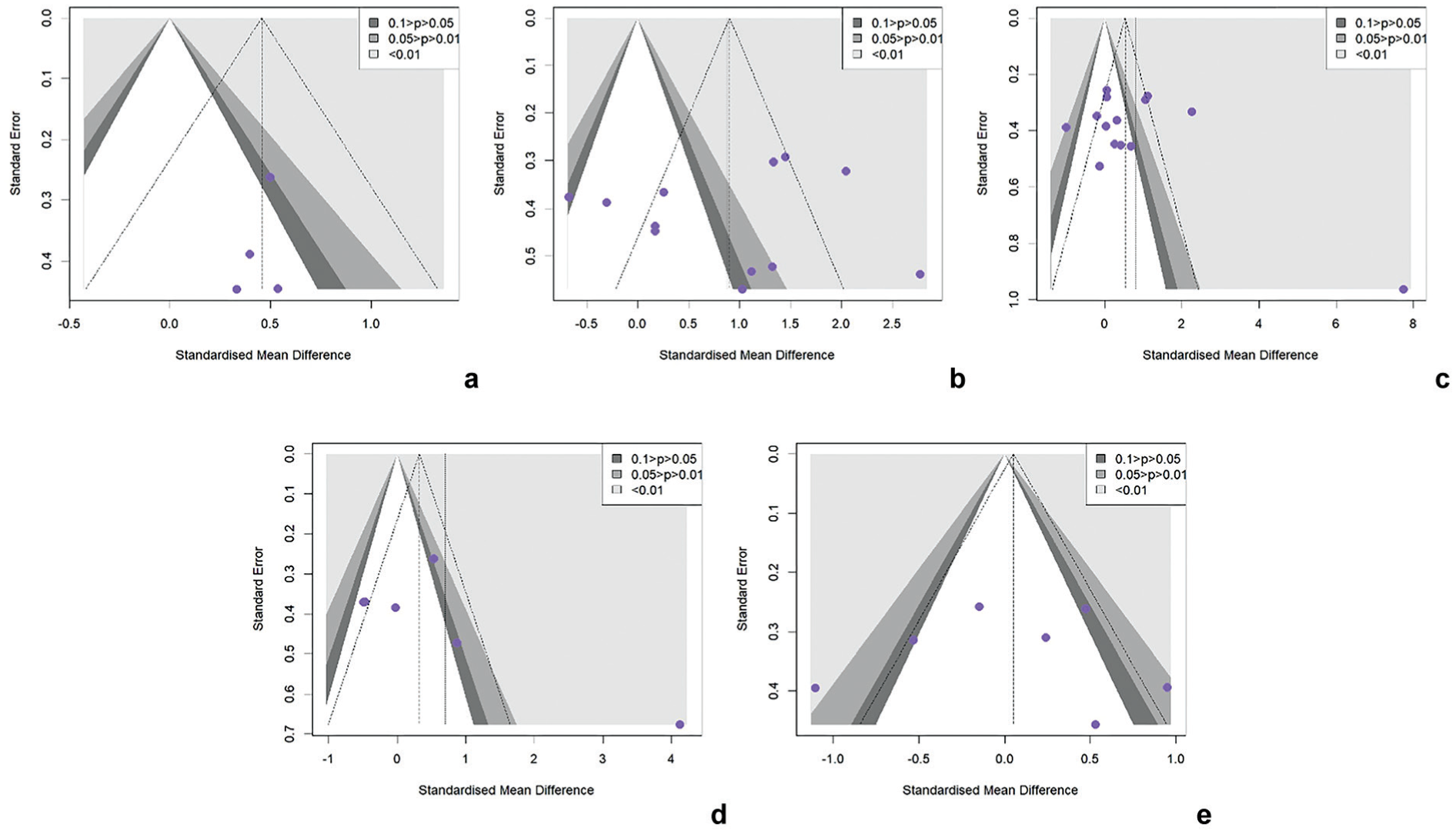
Funnel plots for studies reporting (a) static balance, (b) dynamic balance, (c) subjective functional recovery, (d) physical functional recovery, and (e) sport performance.
Subgroup Analysis and Meta-Regression
Subgroup analyses revealed significant differences between groups (Table 3). Sex was a significant moderator: male-only cohorts showed larger improvements in dynamic balance (SMD = 2.47 vs 0.33; between group, P = 0.01), subjective functional recovery (SMD = 1.34 vs –0.04; between group, P = 0.04) and sport performance (SMD = 0.62 vs –0.35; between group, P = 0.04) compared with mixed-sex cohorts. In addition, several noteworthy patterns emerged. Stroboscopic visual training demonstrated a particularly large effect on dynamic balance (SMD = 1.73; P < 0.05), suggesting its potential superiority in this domain. Within injury types, CAI populations showed robust improvements in static balance (SMD = 0.47; P < 0.05) and dynamic balance (SMD = 0.99; P < 0.05). Trials with passive controls tended to report larger improvements in dynamic balance (SMD = 1.95; P < 0.05) and sport performance (SMD = 0.58; P > 0.05) compared with active comparators, although this difference did not reach statistical between group significance (P = 0.15).
Subgroup effects of visual training on balance and functional recovery
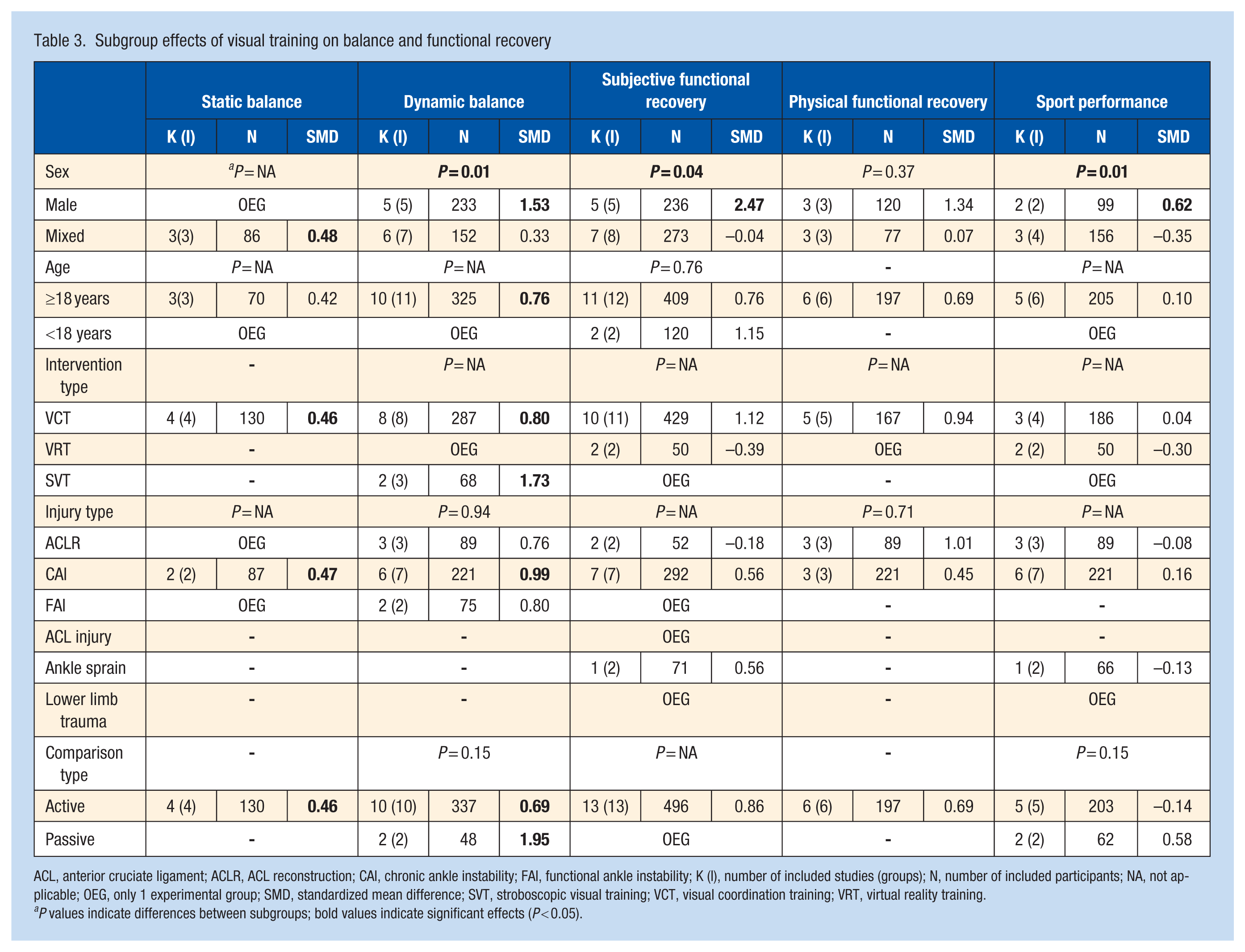
ACL, anterior cruciate ligament; ACLR, ACL reconstruction; CAI, chronic ankle instability; FAI, functional ankle instability; K (I), number of included studies (groups); N, number of included participants; NA, not applicable; OEG, only 1 experimental group; SMD, standardized mean difference; SVT, stroboscopic visual training; VCT, visual coordination training; VRT, virtual reality training.
P values indicate differences between subgroups; bold values indicate significant effects (P < 0.05).
Meta-regression analyses were conducted only for dynamic balance (n = 12) and subjective functional recovery (n = 14), as these were the only outcomes with >10 eligible trials. For subjective functional recovery, however, training frequency emerged as a significant predictor (β = 1.46; 95% CI, 0.79-2.12; P < 0.001; Supplementary Appendix Figure 6.5, available online), indicating that higher intervention frequency was associated with greater improvements in functional recovery. For dynamic balance, no significant moderators were identified. Nevertheless, training frequency showed a positive but nonsignificant trend (β = 0.65; 95% CI, –0.01 to 1.32; P = 0.06; Supplementary Appendix Figure 6.2, available online), suggesting that higher training frequency may contribute to larger improvements in dynamic balance, although the association did not reach statistical significance.
Discussion
This systematic review and meta-analysis included 18 RCTs, revealing that VT improves balance among people with lower-limb injuries significantly, with particularly large effects observed in dynamic balance. However, no statistically significant improvements were observed in subjective functional recovery, physical function, or sport performance outcomes. Subgroup and meta-regression analyses further indicated that training frequency may be a key determinant of intervention efficacy, whereas sex, injury type, and training modality also moderated the effects to varying degrees.
Effects of Visual Training on Balance
This study demonstrates that VT exerts a significant positive effect on balance recovery after lower-limb injuries. VT produced a small-to-modest yet statistically significant improvement in static balance (SMD = 0.46; P = 0.01, borderline large effect), indicating that it effectively enhances static postural stability. A moderate-to-large effect and statistically significant improvement was observed in dynamic balance (SMD = 0.88; P = 0.002, borderline large effect). As dynamic balance represents a critical indicator of motor function recovery and return to sport,15,49 VT can serve as a promising rehabilitation strategy that markedly enhances balance control in people with lower-limb injuries by optimizing visuomotor integration.38,46,51
According to the theory of multisensory integration,40,78 balance control relies on the coordinated interaction among the visual, vestibular, and proprioceptive systems. Lower-limb injuries are often accompanied by proprioceptive deficits. 8 VT can compensate partially for the loss of proprioceptive input by strengthening visuomotor coupling and recalibrating the multisensory integration process.3,19 This compensatory effect can be explained by central sensory reweighting, whereby the central nervous system dynamically adjusts the relative weighting of visual, proprioceptive, and vestibular inputs according to their reliability and contextual demands. 12 When proprioceptive input is degraded after injury, its reduced signal reliability promotes an increased reliance on visual information to maintain postural stability. However, this adaptation is constrained by temporal characteristics of sensory processing, as visual feedback involves longer processing delays (approximately 150-200 ms) compared with proprioceptive feedback (approximately 50 ms). 36 Consequently, visual compensation may preferentially support anticipatory and feedforward control rather than rapid reactive postural adjustments. Evidence from visuo-proprioceptive coupling studies further suggests that such visual dominance represents a context-dependent adaptation rather than a universally optimal strategy, as excessive visual weighting may compromise multisensory integration under certain task or environmental conditions. 19 Furthermore, VT facilitates the reorganization of functional connectivity between cortical motor and sensory regions, particularly in key areas involved in visuomotor transformation, such as the parietal and premotor cortices. 54 Such neuroplastic adaptations enhance the weighting of visual information during motor execution, thereby improving spatial orientation and postural control when proprioceptive feedback is impaired or external sensory input is insufficient. Previous research has shown that VT not only enhances sport performance, 26 but also facilitates the recalibration of multisensory integration by modulating the coupling between sensory input and motor output.7,44 Compared with traditional rehabilitation approaches, VT provides stronger neurophysiological support for postinjury recovery of lower-limb function.
The finding that VT exerts greater effects on dynamic balance than on static balance may be attributed to the task-specific nature of the intervention. Most studies included in this review employed visual coordination training, which combines dynamic visual stimuli with motor tasks. This training paradigm aligns more closely with the neural control mechanisms required for dynamic balance.24,38 Dynamic balance requires continuous visual information processing and motor regulation, and VT precisely strengthens the cognitive-motor coupling involved in this process. In contrast, static balance depends primarily on basic postural maintenance mechanisms and involves relatively minimal higher-order cognitive processing, which may explain its limited responsiveness to VT.
The subgroup analyses revealed several key moderating variables that influenced the effectiveness of VT in improving balance performance. Male participants demonstrated a significantly greater improvement in dynamic balance (SMD = 2.47 vs 0.33; P = 0.01); however, most studies included mixed-sex samples, limiting isolation of sex-specific effects. Whether observed differences reflect biological sex, sex-based activity levels, or other confounders cannot be determined from available data. Training type also demonstrated differential effects, with stroboscopic visual training showing a particularly large effect size (SMD = 1.73) for improving dynamic balance, clearly exceeding that of visual coordination training. The underlying mechanism of stroboscopic visual training lies in intermittent visual occlusion, which enhances predictive control and the formation of motor memory. By periodically restricting visual input, the nervous system is compelled to use the available sensory information more efficiently.33,71 Consequently, stroboscopic visual training improves visuomotor integration and, when combined with balance exercises, produces greater rehabilitation benefits than conventional training approaches.41,68 The injury type analysis indicated that patients with CAI exhibited significant improvements in both static and dynamic balance. This may be due to CAI-specific proprioceptive and neuromuscular control deficits, as VT can effectively compensate for the loss of sensory input resulting from impaired ankle mechanoreceptor function, thereby restoring ankle stability control strategies. 73 Meta-regression analyses for dynamic balance showed that the effect of training frequency approached but did not reach statistical significance (β = 0.65; P = 0.06). This finding suggests that the influence of training frequency on dynamic balance could potentially be overshadowed by qualitative factors such as training modality. Given the limited number of studies and variability in intervention protocols, this relationship requires confirmation in adequately powered trials.
Despite the encouraging effects of VT on balance, the findings are constrained by notable methodological limitations and should be interpreted with caution. The considerable heterogeneity observed in the dynamic balance analysis (I2 = 84%) indicates meaningful between-study differences, likely arising from insufficient standardization of training protocols, variability in outcome measures, heterogeneity of study populations, and differences in intervention delivery. Although heterogeneity was low for static balance (I2 = 0%), which strengthens internal consistency, the small number of included studies (n = 4) limits the generalizability of the conclusions. According to GRADE, the certainty of evidence for both dynamic and static balance was rated very low, due primarily to the following serious issues: (1) risk of bias - frequent shortcomings in randomization procedures, lack of allocation concealment, and inadequate handling of attrition; (2) inconsistency - substantial between-study variability, especially in intervention protocols and effect sizes; (3) indirectness - several interventions deviated from routine clinical practice, reducing direct applicability; (4) imprecision - wide confidence intervals, several of which crossed the null. Collectively, these methodological weaknesses indicate that the current evidence base requires strengthening, and clinical adoption should proceed with caution.
Effects of Visual Training on Functional Recovery
The effects of VT on the 3 functional recovery outcomes were inconsistent with the clear benefits observed for balance improvement. Regarding subjective functional recovery, although the effect size reached a large magnitude (SMD = 0.81), it did not reach statistical significance (P = 0.09). This indicates uncertainty in the efficacy of VT in improving perceived functional ability and suggests it may not outperform conventional rehabilitation methods. Similarly, physical functional recovery did not show statistically significant improvement (SMD = 0.69; P = 0.29), suggesting that VT may have limited efficacy in enhancing proprioceptive joint flexibility. Most notably, VT produced no measurable effects on sport performance (SMD = 0.06; P = 0.81). For athletic populations, this lack of improvement may limit its practical value for enhancing competitive performance or reconstructing sport-specific skills. The benefits of VT may therefore be confined to directly related sensorimotor abilities, with relatively limited contribution to broader functional recovery. Although VT shows clear advantages in balance restoration, these gains do not appear to translate directly into comprehensive improvements in sport performance or functional recovery. While VT enhances visuomotor integration and balance control, these improvements may not transfer effectively to more complex functional tasks. Functional recovery involves the coordinated integration of multiple physiological systems, including muscular strength, endurance, coordination, and psychological factors, whereas VT targets primarily perceptual-cognitive enhancement and exerts limited direct influence on other system components.43,52 Therefore, future studies should further explore the complementary relationship between VT and conventional rehabilitation, such as whether combining VT with neuromuscular or task-specific training could, while maintaining balance-related benefits, promote both subjective and objective functional recovery more effectively, thereby providing more comprehensive and sustained rehabilitation support for people with sports injuries. From a neuroadaptive perspective, the neuroplastic changes induced by VT may occur primarily in specific brain networks involved in visuomotor transformation, such as the visual cortex, parietal cortex, and cerebellum. 47 However, functional recovery requires the involvement of broader neural networks, including the motor cortex, basal ganglia, and spinal motor circuits. 60 This limitation in neural adaptation may explain why VT yields significant improvements in directly related tasks such as balance but demonstrates limited effects in comprehensive functional assessments.
The subgroup analyses once again identified sex as an important moderating factor. Male cohorts showed greater improvements in subjective functional recovery (SMD = 1.34 vs –0.04; P = 0.04) and sport performance (SMD = 0.62 vs –0.35 P = 0.04). However, as no included studies examined female-only samples, these findings should be interpreted with caution and require further investigation. The analysis of control group type revealed that studies using active controls generally reported smaller effect sizes than those with passive controls, a pattern particularly evident in functional recovery outcomes. Notably, the vast majority of studies included in this meta-analysis (16 of 18) employed an active control design, in which control groups received evidence-based rehabilitation interventions such as standard physiotherapy, neuromuscular training, or balance training. Only a few studies used passive control groups without additional treatment.24,68 Active control interventions themselves have been shown to effectively improve muscle strength, joint mobility, proprioception, and functional performance. Consequently, VT must demonstrate additional improvements beyond these already effective baseline treatments to achieve statistical significance. Although this design enhances clinical relevance, it simultaneously increases the difficulty of detecting the additional benefits of VT. Therefore, VT must yield additive benefits beyond existing effective rehabilitation treatments, which undoubtedly raises the threshold for achieving statistical significance.
The meta-regression analysis revealed a significant positive association between training frequency and improvement in subjective functional recovery (β = 1.46; P < 0.01). This finding suggests that achieving significant gains in subjective functional recovery may require higher-intensity or more frequent training stimuli. High-frequency training may facilitate the transfer of training effects to functional tasks by providing more learning opportunities and reinforcing memory consolidation processes. 17
The GRADE assessment rated the certainty of evidence for all functional recovery outcomes as very low. These 3 indicators shared similar methodological shortcomings with the balance outcomes, including inadequate randomization and blinding procedures, small sample sizes, inconsistency in intervention protocols and outcome measures, and uncertainty in effect size estimation. These limitations indicate that the current evidence regarding the effects of VT on functional recovery remains insufficient. Its efficacy should be further validated through high-quality RCTs with larger sample sizes, more rigorous designs, and extended follow-up periods, to provide stronger and more reliable evidence for clinical application.
Limitations, Clinical Implications, and Future Research
Although this review and meta-analysis provides new insights into the role of VT in balance and functional recovery after lower-limb injuries, several limitations should be acknowledged. (1) The literature search was restricted to English-language, peer-reviewed randomized controlled trials, which ensured methodological rigor but may have introduced language and publication bias. (2) For certain outcomes, such as static balance and sport performance, the small number of eligible studies limited the statistical power and the robustness of subgroup analyses. (3) Although subgroup and moderator analyses were performed, data insufficiency prevented adequate examination of certain potentially important variables, such as intervention duration, injury severity, and type of VT. (4) Although female participants were included in several studies, all eligible trials employed mixed-sex samples, and none were specifically designed to investigate female-only populations or conduct sex analyses. (5) Despite the application of an age range of 10 to 60 years, age-related differences in visual development and sensorimotor function may still represent a potential source of heterogeneity, which should be considered when interpreting the findings.
Due to the very low certainty of evidence, these findings provide preliminary insights for rehabilitation after lower-limb injuries. (1) VT may serve as a valuable adjunct to conventional rehabilitation programs, particularly for enhancing dynamic balance - a critical factor for functional recovery and safe return to sport. (2) Given the limited evidence, current findings do not allow firm conclusions regarding the standalone effects of VT, suggesting that its role in multimodal rehabilitation strategies warrants further investigation. (3) Training frequency warrants further investigation, as variations in training frequency across studies may partly contribute to differences in observed effects; however, the optimal frequency and dosage of VT remain unclear and require validation in future high-quality randomized controlled trials with standardized protocols. (4) As no included studies specifically examined female participants, clinicians should recognize that current evidence may not fully capture sex-specific training responses and should tailor rehabilitation protocols to individual differences. (5) Given that most existing studies adopted relatively short intervention and follow-up periods, VT should be embedded in a longer-term rehabilitation framework and combined with proprioceptive and sport-specific skill training to maximize both short- and long-term recovery outcomes.
Although this study provides valuable evidence, further research is required to strengthen and expand the current understanding of VT. First, based on the existing evidence, future trials should adopt high-quality randomized controlled designs that adhere to rigorous methodological standards, include larger sample sizes (e.g., ≥90 participants per group), and extend follow-up durations (e.g., >12 months) to better evaluate the long-term effects of VT on injury prevention and functional recovery. Second, further research should explore sex-specific responses to VT, as no studies to date have specifically targeted female populations, and should prospectively examine individual characteristics such as age, sex, and baseline proprioceptive deficits, including aptitude-treatment interaction analyses. Future studies should also systematically compare different training frequencies, durations (e.g., ≥8 weeks), and intensities, preferably using standardized outcome measures across balance and functional domains, to clarify the optimal dose-response relationship of VT. Finally, integrating advanced neuroimaging and biomechanical techniques will be essential to elucidate the underlying mechanisms of VT and facilitate its broader implementation in clinical and athletic practice.
Conclusion
This systematic review comprehensively evaluated the effects of VT on balance and functional recovery after lower-limb injuries. The findings indicate that VT has a positive effect on improving balance, with particularly pronounced benefits for dynamic balance. However, no significant improvements were observed in subjective functional recovery, physical function, or sport performance. Subgroup analyses suggested that male participants, people with CAI, and those receiving stroboscopic visual training exhibited greater potential for improvement. Moreover, meta-regression results identified training frequency as a key determinant of subjective functional recovery. Nevertheless, the GRADE assessment rated the certainty of evidence across all outcomes as very low, due primarily to high heterogeneity, methodological limitations, and small sample sizes. Therefore, VT may be considered as a valuable adjunct in lower-limb rehabilitation, particularly during the balance restoration phase. In clinical practice, VT can strengthen visuomotor coupling, compensate for sensory deficits caused by proprioceptive impairment, and thereby enhance overall rehabilitation outcomes. Future research should focus on extending intervention duration, determining the optimal training frequency, and conducting high-quality randomized controlled trials across different sexes to elucidate the long-term effects and underlying neural mechanisms of VT in sports rehabilitation.
Supplemental Material
sj-docx-1-sph-10.1177_19417381261451826 – Supplemental material for The Effects of Visual Training on Balance and Functional Recovery After Lower Extremity Injuries: A Systematic Review and Meta-analysis
Supplemental material, sj-docx-1-sph-10.1177_19417381261451826 for The Effects of Visual Training on Balance and Functional Recovery After Lower Extremity Injuries: A Systematic Review and Meta-analysis by Kaijun Liu, Jinyu Qiu, Anqi Shi and Yuqiang Guo in Sports Health
Footnotes
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.