
Abstract
Context:
There is significant interest in jugular venous compression (JVC) devices from multiple parties, including sports physicians, athletic trainers, athletes, and parents.
Objective:
To examine the effects of JVC on repetitive head impacts and evaluate their effectiveness in reducing brain injury and concussion risk in sport.
Data Sources:
Embase, Cochrane Central Register of Controlled Trials, CINAHL Plus, SPORTDiscus, Web of Science Core Collection - SCI-EXPANDED, SSCI, AHCI, ESCI, American Psychological Association, PsycInfo, WHO International Clinical Trials Registry Platform (ICTRP), ProQuest Dissertations and Theses Citation Index (Web of Science), Europe PMC, and PubMed.
Study Selection:
Full-text, peer-reviewed manuscripts of primary research, published between 2010 and 2024.
Study Design:
Scoping review.
Level of Evidence:
Level 5.
Data Extraction:
A total of 22 articles met the inclusion criteria. These articles were categorized into 4 groups: animal models (n = 4), biomechanics in humans (n = 4), evidence in athletes (n = 11), and evidence in Special Weapons and Tactics Breacher Training (SWAT) (n = 3). Several of the athlete articles used the same cohort of athletes.
Results:
There was no difference in concussion rates in athletes between collared and noncollared groups during a season, while evidence from animal and tactical populations was limited to mechanistic and imaging outcomes. In both athletes and SWAT personnel, there were no clinically significant differences in neurocognitive performance between groups. There are statistically significant imaging changes between collared and noncollared groups; however, the imaging changes were not consistent and are of uncertain clinical significance. Furthermore, 6 out of 11 studies in athletes are currently under investigation. The available evidence supports that JVC can increase intracranial pressure, but it remains unknown if this results in any clinically meaningful benefit.
Conclusion:
Although no adverse outcomes are reported with collar use, current research does not support the effectiveness of JVC collars for concussion reduction and use for mitigation of repetitive head impact. Additional studies from diverse research teams with independent funding sources are required.
Repetitive head impacts, also termed subconcussive impacts, are head contacts that do not result in the clinical manifestation of a concussion. 3 However, some authors suggest that the aggregation of such contacts over an athlete’s career may have deleterious neurophysiological impacts, including cognitive effects.14,20 Moreover, some neuroimaging studies indicate that a single season of contact sports involving repetitive head impacts can alter brain networks as measured by diffusion tensor imaging (DTI).2,7 Studies have shown that DTI metrics are sensitive to changes in white matter microstructure and can be altered after a concussion. 28
A specialized neck collar has been developed (Q-Collar, Q30 Westport) and is United States Food and Drug Administration (FDA) approved to aid in protection of the brain from the effects of repetitive subconcussive head impacts. 36 There is debate regarding the clinical effectiveness of such devices, 13 and a more recent summary by the FDA was more measured in its support. The summary highlighted limitations including that the Q-Collar has not been demonstrated to prevent long-term cognitive function deficits, ultimate impact on clinical outcomes has not been evaluated, use of imaging studies as a future indicator of brain injury has not been validated, and data do not demonstrate that the device can prevent concussion or serious brain injury. 35 In addition, 6 studies that were submitted to the Journal of Neurotrauma are currently under investigation.24,29,38,40,41,43
These devices apply pressure to the bilateral jugular veins and are proposed to provide brain “cushion” by increasing venous volume. This increase is intended to limit brain movement and lessen the impact of rapid acceleration/deceleration and tissue deformation.4,15 This scoping review provides a comprehensive analysis of studies examining the effects of jugular venous compression (JVC) on repetitive head impacts in sports, as well as animal, biomechanical, and tactical-athlete studies. Specifically, it aims to determine whether a JVC collar reduces deleterious effects of repetitive head trauma, as observed through neuroimaging and neurocognitive task performance, and whether use of neck collars influences the frequency of head impacts as well as concussion rate.
Methods
This review was intended originally to be a systematic review, with the authors developing a protocol and registering it with PROSPERO. However, after conducting an initial screening of the studies and identifying gaps in the existing literature, there was insufficient literature to support a systematic review, so the project was transitioned to a scoping review format. This scoping review has now been registered with Open Science Framework and was carried out in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses extension for Scoping Reviews (PRISMA-SCr) guidelines. 33
Search Strategy
The search strategy was created by a health sciences librarian using relevant seed studies related to JCV, repetitive head impact, and concussion outcomes provided by the authors. The search strings used controlled vocabulary and free text terms to increase search sensitivity in multiple databases. Databases used were Embase, Cochrane Central Register of Controlled Trials, CINAHL Plus, SPORTDiscus, Web of Science Core Collection-SCI-EXPANDED, SSCI, AHCI, ESCI, American Psychological Association, PsycInfo, WHO International Clinical Trials Registry Platform (ICTRP), ProQuest Dissertations and Theses Citation Index (Web of Science), Europe PMC, and PubMed. The search strategy for each database can be found in Supplemental Appendix I (available in the online version of this article). The search was limited to the years 2010 to 2024. Publications in languages other than English were excluded.
Study Selection
Searches were uploaded into Covidence, where they were de-duplicated. Inclusion criteria were studies examining the effect of JVC head injury, including repetitive head impact in English in animal models, athletes, and other groups where repetitive head impact is a concern (military/police). Studies were included if they discussed mechanisms or outcomes. Subsequently, the titles and abstracts were screened manually by 2 authors for relevance. Disagreements were resolved through discussion. Full-text screening was performed by both authors to see whether inclusion criteria were met, and disagreements were again resolved through discussion. Animal and tactical athlete studies were included to provide mechanistic context and were analyzed separate from studies conducted in athletes.
Data Extraction
Before data extraction, the authors agreed on information to be extracted. Extracted information included year of study, country of study, study participants, study type, study design, results, interpretation of findings, study funding, imaging outcomes, cognitive tests outcomes, and concussion rate.
Results
From 239 articles found using the searches, 22 were deemed relevant and included in this scoping review, as illustrated in the flow diagram in Figure 1. Of these 22 studies, 8 provide insight into the mechanism of action of JVC, 11 investigate Q-collar use in athletes, and 3 examine JVC in special weapons and tactical personnel.
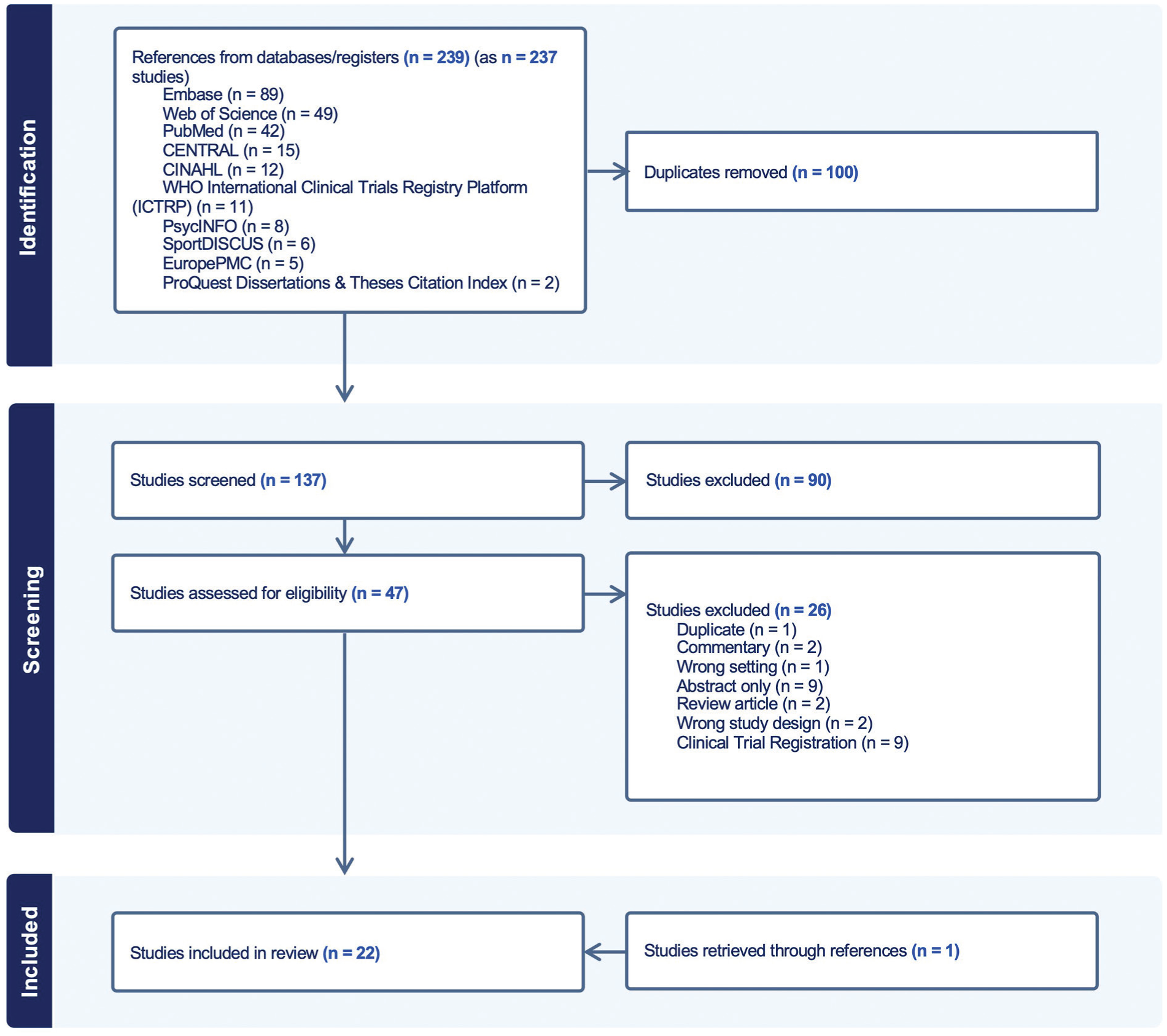
PRISMA-SCr flow diagram for this scoping review, created using Covidence. PRISMA-SCr, preferred reporting items for systematic reviews and meta-analyses extension for scoping reviews.
Animal models
Search results identified 4 studies in rats and swine that explored the mechanism of action of JVC and its potential to mitigate the effects of head impact. Two studies investigated the effects of JVC on brain injury using rat mild traumatic brain injury (TBI) models.30,34 Smith et al 30 and Turner et al 34 reported a mean 31% increase in intraocular and intracranial pressures with the use of JVC, supporting the proposed mechanism of action. Both papers examined the effects of impact-acceleration TBI on rats with and without JVC. The studies found an 80% reduction in the number of amyloid precursor protein-positive (b-APP) axons, 30 a 48.7% to 59.1% reduction in degenerative neurons, a 36.8% to 45.7% decrease in reactive astrocytes, and a 44.1% to 65.3% reduction in microglial activation among rats with JVC compared with controls. 34 Although both studies had a small sample size, with only 10 experimental and 10 control animals, and assessed histological markers only 7 days post-TBI, their findings indicate potential protective effects of JVC for single impact head injury in a controlled setting.
Other studies used swine models to investigate the effect of JVC on TBI markers.19,29 Mannix et al 19 used a model allowing for neck rotation at impact and reported a reduction of histological markers after TBI, specifically the phosphorylated tau epitope AT8 and the inflammatory microglial marker IBA1. Conversely, Sindelar et al, 29 using a fixed-head TBI model with the intent to create brain hemorrhage, found no statistical difference in b-APP, neuronal degeneration, cerebral edema, or inflammatory infiltration in animals with JVD compression compared with controls, but did observe a reduction in total subarachnoid and intraparenchymal hemorrhage scores.
Overall, the applicability of these studies to sport-related repetitive head impact in supporting a decrease in harm from repetitive head impact is uncertain. In sports, there are multiple degrees of freedom of the neck after a blow to the head. Only 1 animal model allowed for rotational forces, 19 and in 3 studies the neck was fixed.29,30,34 The injury models used in these studies were limited by use of a single injury paradigm (vs repetitive head impact) and the magnitude of the applied forces was likely significantly more than those that occur with typical sports-related head impacts, with 1 study creating an injury leading to brain hemorrhage. 29 In addition, the collars used for these studies differed from commercial models tested in humans (Table 1).
Animal studies of JVC
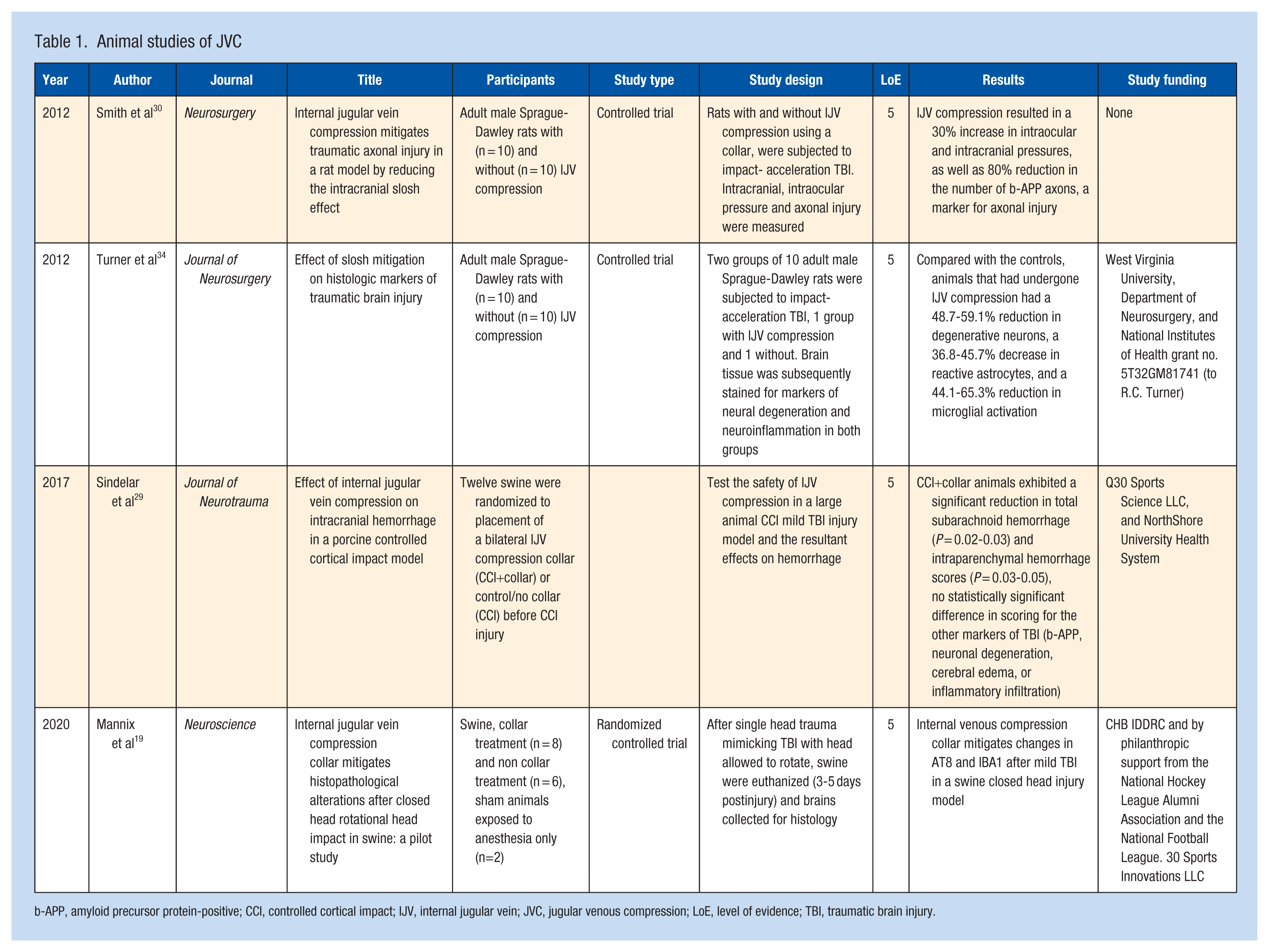
b-APP, amyloid precursor protein-positive; CCI, controlled cortical impact; IJV, internal jugular vein; JVC, jugular venous compression; LoE, level of evidence; TBI, traumatic brain injury.
Biomechanical Studies in Humans
Research in humans has demonstrated that JVC compression leads to an increase in jugular vein cross-sectional area,10,16,37 as well as increased intracranial pressure, 10 indicating the potential for decreased intracranial compliance or ability for brain deformation. Two studies used the Q-Collar,16,37 and 1 study used a Velcro collar with 2 rectangular sponge pads placed over the internal jugular vein. 10 DiCesare et al 8 investigated the effects on wearing a collar for JVC on athletic performance and found no detrimental impacts during a range of physiologic and neurologic challenges mimicking competitive sport. These studies were small but support the view that JVC collars increase intracranial pressure and appear to be safe in the short term in controlled settings (Table 2).
Biomechanical studies in humans
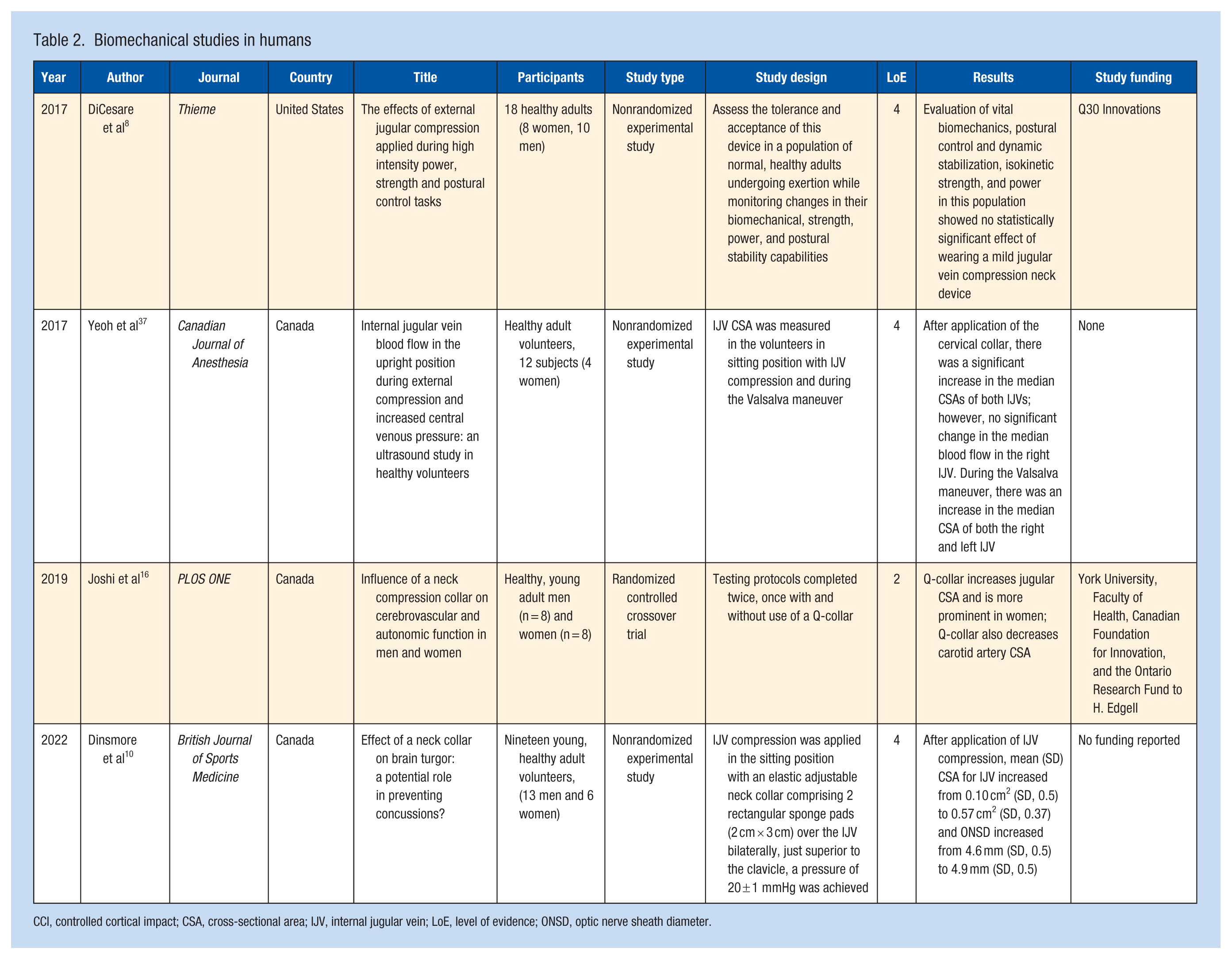
CCI, controlled cortical impact; CSA, cross-sectional area; IJV, internal jugular vein; LoE, level of evidence; ONSD, optic nerve sheath diameter.
Evidence in Athletes
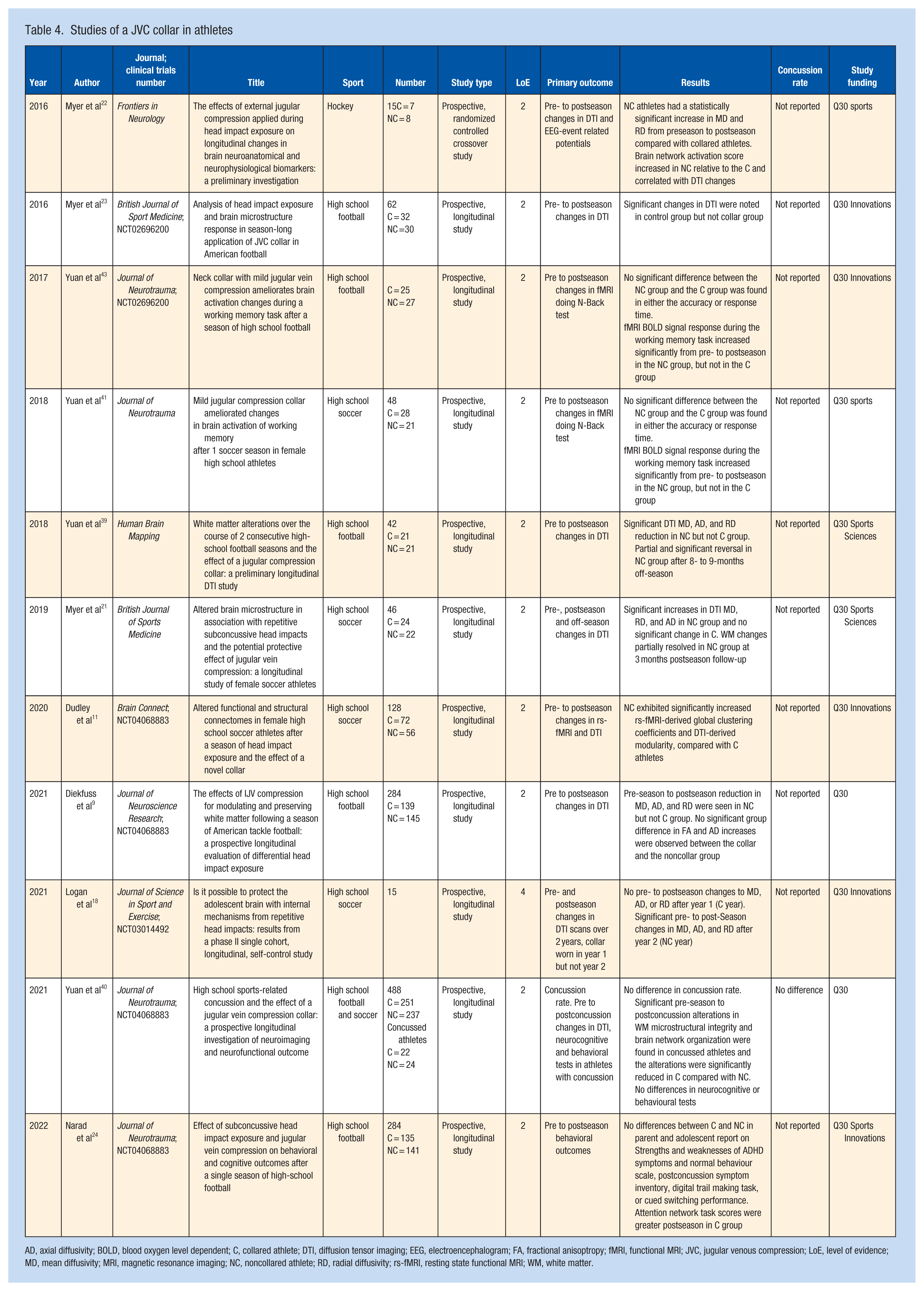
A total of 11 studies investigated the effects of wearing a collar inducing JVC on repetitive head impact in the sports of football (n = 6), women’s soccer (n = 5), and hockey (n = 1). All 11 studies were performed by similar author groups and funded by the manufacturer of a JVC collar. There appear to be overlapping cohorts with separate papers reporting different outcomes. It is unclear how many total athletes were represented. Of these studies, 4 (representing a total of 488 athletes) had the same national clinical trials registration.9,11,24,40 These studies follow a cohort of athletes across 1 or 2 seasons, focusing on longitudinal changes in brain neuroanatomy and neurophysiology using neuroimaging. Impact sensors were used to detect and quantify repetitive head impacts. While all the studies show significant differences in neuroimaging results between the athletes wearing a collar and those without, the direction of differences in white matter DTI parameters varied (Table 3). Two studies reported on functional magnetic resonance imaging (MRI) (fMRI) blood oxygen level dependent (BOLD).41,43 These studies examine oxygen uptake on MRI while performing a cognitive task. Both studies showed no differences in performance of pre- and postseason cognitive tasks; however, in the postseason, while both the noncollared group and the collared group had increases in fMRI BOLD signal, the increase was greater in some brain areas in the noncollared athletes.41,43 Two studies included follow-up neuroimaging scans, both of which revealed a partial reversal of DTI changes observed in the noncollar group at 3 to 9 months postseason.21,39 There is a lack of consensus regarding the clinical implications and potential long-term effects of the reported neuroimaging changes on neurophysiology and neuroanatomy.
Summary of DTI findings in noncollar group and collared group after 1 season a
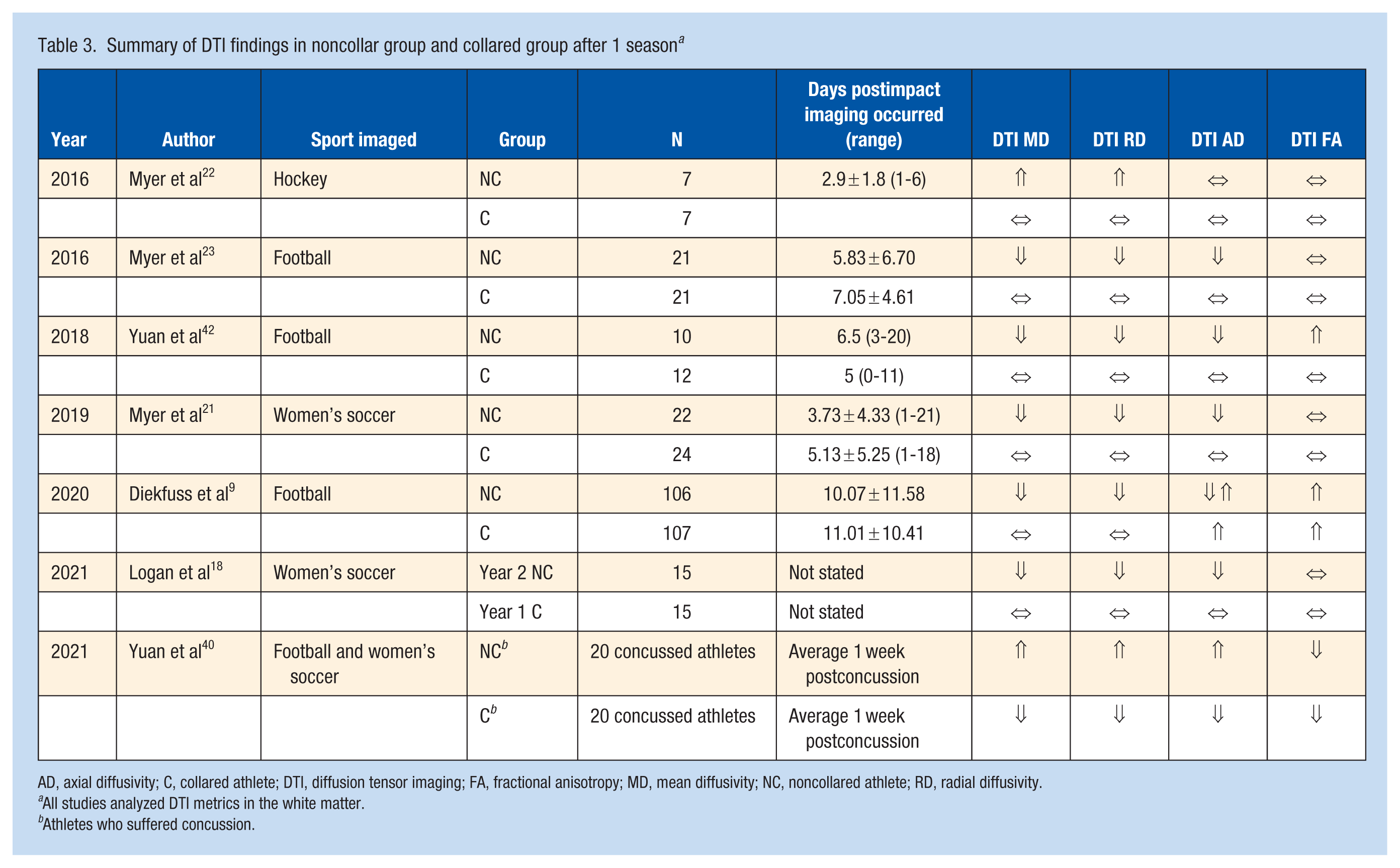
AD, axial diffusivity; C, collared athlete; DTI, diffusion tensor imaging; FA, fractional anisotropy; MD, mean diffusivity; NC, noncollared athlete; RD, radial diffusivity.
All studies analyzed DTI metrics in the white matter.
Athletes who suffered concussion.
There does not appear to be a difference in overall head impact counts across the sporting season between collar and noncollar groups, with only 1 small study in hockey (n = 15) reporting more head impacts in the collar compared with the noncollar group. 22 These findings suggest little evidence for risk compensation or of players adjusting their behavior when wearing the collar (e.g., tackling with their head more because they felt protected).
Only 1 of the 11 studies in athletes reported concussion rates and found no difference between collared and noncollared groups. In this large study of 488 male football and female soccer athletes, the rate of concussion was 9.43% in the collared group compared with 10.13% in the noncollared group. 40 There were 40 athletes who underwent imaging an average of 7 days after the concussion; results showed that concussed athletes had white matter changes in axial diffusivity (AD), radial diffusivity (RD) and mean diffusivity (MD) but those wearing the collar had changes of a smaller magnitude. 40 A participant breakdown by sport and sex was not reported.
Four studies included pre- and postseason cognitive assessments and self-report questionnaires.24,40,41,43 Three of the studies included the entire enrolled study population and did not report on whether any of the athletes had sustained a concussion during the season,24,41,43 while the fourth study looked at pre and postseason cognitive assessments only in athletes who had been concussed during the season. 40 The neurocognitive tests included the N-back task assessing working memory; digital Trail Making Test assessing neuromotor control, attention and oculomotor function; the Strengths and Weaknesses of ADHD Symptoms and Normal Behavior Scale (SWAN); Cued Switching task; Post-Concussion Symptom Inventory; Attention Network Task (ANT); King-Devick (KD) test; and Flanker test assessing attention. These studies reported no significant differences between the collar and noncollar groups on most assessments.24,40,41,43 However, 1 study reported a small but significant improvement in postseason performance of the collar group in the altering network scores of the ANT compared with the noncollar group, with the caveat of a small effect size with questionable clinical significance. 24 Yuan et al 40 documented improved performance among collared athletes on the KD over the course of a season when compared with noncollared controls. However, performance for both groups improved during the course of the season; therefore, the clinical significance of a reduced practice effect in the noncollared group is unclear (Table 4).
Studies of a JVC collar in athletes
AD, axial diffusivity; BOLD, blood oxygen level dependent; C, collared athlete; DTI, diffusion tensor imaging; EEG, electroencephalogram; FA, fractional anisoptropy; fMRI, functional MRI; JVC, jugular venous compression; LoE, level of evidence; MD, mean diffusivity; MRI, magnetic resonance imaging; NC, noncollared athlete; RD, radial diffusivity; rs-fMRI, resting state functional MRI; WM, white matter.
In summary, these studies comparing groups of athletes wearing JVCs with those without show group differences in advanced neuroimaging metrics; however, the direction and magnitude of change is inconsistent and the clinical significance is unclear. All reviewed studies used a common JVC collar - the Q-Collar. Impact monitors included helmet-mounted sensors, X-patches, and G-Force sensors showed no differences in impacts, although these impact monitors have limitations which have been described previously. 25 There was no difference in concussion rate between collared and noncollared groups and there was no clinically significant difference between groups in neurocognitive testing. All of these studies were funded by the maker of the Q-Collar.
Evidence in Special Weapons and Tactics Breacher Training
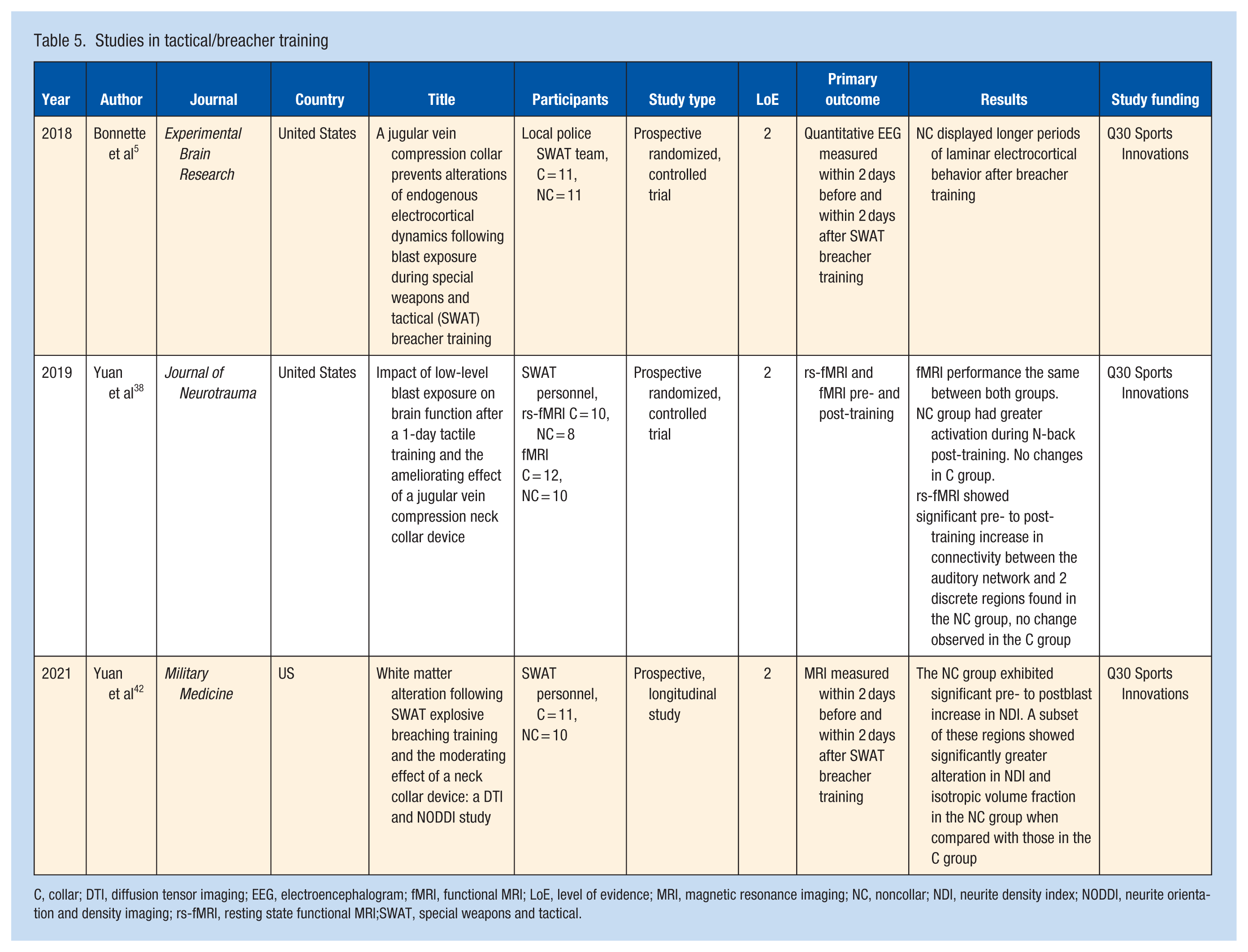
We identified 3 studies in special weapons and tactics (SWAT) breacher training.5,38,42 The studies used an impact monitor for blast exposure and evaluated a variety of imaging and cognitive outcomes in participants with and without a collar for JVC. One study conducted recurrence quantification analysis, a type of quantitative electroencephalogram (EEG), testing 2 days before and within 2 days after blast exposure, with 11 people in each group, and found participants in the noncollar group had longer periods of laminar electrocortical behavior after breacher training compared with the noncollared group. 5 Another study investigated fMRI and cognitive changes in SWAT personnel after blast exposure and found significantly increased fMRI brain activation during the N-back working memory task and fMRI activity but no significant difference in performance on the N-back working memory task. 38
In a subsequent study, Yuan et al 42 investigated MRI and neurite density index (NDI) changes using neurite orientation dispersion and density imaging (NODDI) - more sophisticated markers of grey matter change - 2 days before and 2 days after blast exposure and found a significant increase in NDI in the noncollar group from pre- to postblast exposure, but no significant difference in DTI changes between the 2 groups. These studies were limited by small samples sizes (Table 5).
Studies in tactical/breacher training
C, collar; DTI, diffusion tensor imaging; EEG, electroencephalogram; fMRI, functional MRI; LoE, level of evidence; MRI, magnetic resonance imaging; NC, noncollar; NDI, neurite density index; NODDI, neurite orientation and density imaging; rs-fMRI, resting state functional MRI;SWAT, special weapons and tactical.
Discussion
This scoping review provides a comprehensive overview of the studies investigating the potential role of external JVC for mitigating repetitive head impact across a range of exposure contexts. Out of 239 screened articles, 22 met inclusion criteria, with 11 in studies in athletes, of which many appeared to have overlapping cohorts. Other studies included in the review were animal-model studies (4), biomechanical studies in humans (4), and studies in tactical athletes (3). The nonsport studies were included to inform potential mechanisms of action and biological effects of JVC. This review led to several conclusions. First, animal-model studies support the view that JVC collars increase intracranial pressure and may protect the brain from a single-head traumatic impact; however, the applicability of the animal models to subconcussive repetitive head impact in humans is unknown. Second, biomechanical studies in humans support the ability of JVC collars to increase intracranial pressure and short-term use did not appear to cause harm. Third, studies in athletes show differences in advanced neuroimaging after a season of use between collared and noncollared athletes but no difference in concussion rate or clinically significant difference in neurocognitive testing. The clinical significance of the neuroimaging changes is unclear. Finally, very small studies in tactical athletes (breacher training), which involve blast exposure rather than sport-related impacts, show differences in quantitative EEG, white matter changes, and differences in fMRI between collared and noncollared participants. All studies were funded by the maker of a JVC collar.
Studies in animals (4), biomechanical studies in humans (4), and studies in tactical athletes (3) were included to provide a complete picture of available research. Animal and biomechanical studies suggest JVC increases intracranial pressure providing support for the proposed mechanism of action of the collar. However, the applicability of the single-injury model used in animals to sports-related repetitive subconcussive impacts is unknown. Likewise, forces from blasts experienced by tactical athletes (SWAT) are very different from repetitive subconcussive head impacts experienced by football and soccer athletes, and the ages of the cohorts were different, which can all effect imaging outcomes. Findings from studies on tactical athletes exposed to blast forces may also not be applicable to repetitive head impact in athletes.
The primary finding in 7 of the athlete studies was changes in DTI in the white matter. DTI is an advanced MRI technique that quantifies the directional movement of water molecules in brain tissue, providing sensitive markers of white and grey matter microstructural integrity. 6 MD refers to the overall magnitude of water diffusion within the brain tissue, AD quantifies diffusion along the axis of white matter tracts and is often associated with axonal integrity, RD measures diffusions perpendicular to axonal fibers and is linked to myelin integrity and fractional anisotropy (FA) reflects the degree of directionality of diffusion with higher values associated with more organized white matter and is reported for different structures in the brain. DTI studies in athletes with concussion generally show that MD, AD, and RD go up and FA goes down after concussion, and are not back to normal when symptoms have resolved and athletes have been cleared to play. Studies of contact athletes after a season of repetitive head impact have conflicting findings. 32 There is wide variability among studies, which may be due to acquisition parameters, age of athlete, time postconcussion when imaging is acquired, and wide variability in methods of analysis and interpretation making comparison and generalizations difficult. 17 All of the DTI studies on athletes without a JVC collar compared with athletes wearing the collar for a season reported some changes in white matter DTI parameters; however, the magnitude and direction of change was not always consistent and the clinical significance is unknown.
The other studies in athletes looked at fMRI, resting state fMRI, and neurocognitive testing comparing collared with noncollared athletes. There were no performance differences between groups on neurocognitive tests; however, fMRI BOLD signal response during the working memory task had greater increase in some brain areas in the noncollared group in 2 studies,41,43 and in another study there was significantly increased resting state fMRI-derived global clustering coefficients and DTI-derived modularity. 11 fMRI BOLD is an indirect marker of neural activity potentially indicating more brain activity was required for the task in noncollared athletes and changes in global clustering coefficients and DTI-derived modularity may represent either adaptive reorganization or maladaptive loss of global integration. 12 In addition, 1 study found no differences in male high school football players in a variety of neurocognitive measures. 24 These studies indicate that there are no clinically significant differences in functional neurologic outcomes. The clinical significance of advanced MRI changes is unknown.
While commercial JVC collars are FDA approved and marketed to reduce the effects of repetitive head impact, media and athlete testimonials portray a decrease in concussion rate that is not supported in the literature.26,27 Only 1 study reported on concussion rate and it showed no significant difference between athletes who wore a JVC collar and those who did not. 40 This latter study was large, with 488 total athletes participating. DTI changes in 20 athletes who sustained a concussion and were not collared were more prominent than in the 20 athletes who sustained a concussion wearing a collar. 40 There are no studies comparing athletes in noncontact sports wearing collars with those without to assess whether similar differences in DTI exist secondary to collar wearing outside the setting of repetitive impact and the long-term effect of JVC collar use is untested. Finally, these studies were all relatively short-term, following athletes from preseason to postseason with a maximum follow-up 9 months postseason; therefore, potential long-term protection is speculative.
Limitations
This scoping review explores the potential of JVC collar use to mitigate the effects of repetitive head contacts in sports; it is constrained by the limited number of studies in athletes, and the studies appeared to use similar cohorts. Studies in animals and on the biomechanics in humans were included to assess the reasonableness of the proposed mechanism of action. There were no studies comparing the use of a JVC collar with noncollar wearers in noncontact sport that would offer additional insight. Most studies were conducted over a short duration, focusing only on athletes within a single sporting season. All studies involving athletes were funded by Q30 Innovation LLC - the manufacturer of the JVC collar - which raises the possibility of study bias, and all were conducted in North America, potentially limiting generalizability. The review included only studies published in English, which may have led to the omission of relevant research.
Finally, there have been concerns expressed in the literature about inconsistency and errors in the statistical interpretation of some studies, 31 and 6 studies published in the Journal of Neurotrauma are currently under investigation.1,24,29,38,40,41,43 Statistical corrections have been submitted for 3 of the articles, with the authors stating that the corrections do not alter the primary findings or conclusions.38,40,43 As of October 24, 2025, there have been no findings of wrongdoing. 1 Despite these limitations, this review offers valuable insights into the possible role of JVC in countering the effects of head impacts and identifies key areas for future research.
Conclusion
The findings from this scoping review underscore the need for additional independent research on JVC as an intervention for mitigating the effects of repetitive head impacts during sports-related activities. Animal and human studies suggest that intracranial pressure is increased with JVC compression. Yet, the available evidence in athletes does not demonstrate a reduction in concussion rate or consistent, clinically meaningful improvements in neurocognitive performance associated with JVC collar use. Although several studies report differences in advanced neuroimaging metrics between collared and noncollared athletes following a season of play, the direction and magnitude of these changes are inconsistent, and their clinical significance remains unclear. Furthermore, the studies were all relatively short-term, with a maximum follow-up of 9 months postseason. Therefore, no long-term conclusions can be drawn regarding the use of these devices.
Evidence in animals and tactical personnel provides insight into potential mechanisms of action but involves injury mechanisms and populations that differ substantially from sport-related repetitive head impact. Therefore, findings from animal and military studies may not be directly applicable to sport-related repetitive head impacts in athletes.
Future research is necessary to better understand whether the JVC is protective, especially through large-scale, randomized, long-term studies involving diverse populations and standardized outcome measures as well as studies in noncontact athletes. Until such evidence is available, thoughtful consideration of the body of evidence should be employed before the decision to use or recommend a JVC. Multidisciplinary approaches involving the traditional approach of rule changes, protective equipment, training strategies, and education remain essential in addressing both the short- and long-term consequences of repetitive head impacts in sports, while additional mitigation strategies continue to be explored.
Supplemental Material
sj-docx-1-sph-10.1177_19417381261453672 – Supplemental material for Jugular Venous Compression Collar for Prevention of Brain Injury due to Repetitive Head Impact and Concussion in Sport: A Scoping Review
Supplemental material, sj-docx-1-sph-10.1177_19417381261453672 for Jugular Venous Compression Collar for Prevention of Brain Injury due to Repetitive Head Impact and Concussion in Sport: A Scoping Review by Isabella Weber, Bridget M. Whelan, Jared M. Bruce and Kimberly G. Harmon in Sports Health
Footnotes
Acknowledgements
The authors would like to thank Teresa Jewell, librarian at the University of Washington, for her assistance with the search strategy for this study.
K.G.H. is employed as the Deputy Chief Medical Officer for the National Hockey League (NHL). J.M.B. is co-chair of the NHL concussion subcommittee and director of neuropsychology and neurobehavioral sciences at the NHL. The views and opinions expressed are soley those of the authors and do not necessarily represent those of the NHL. J.M.B. is also the neuropsychology consultant to Sporting KC. The other authors report no potential conflicts of interest in the development and publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.