
Abstract
Background:
Shoulder function asymmetries are common in adolescent volleyball players, yet evidence beyond glenohumeral range of motion (ROM) is limited, and few studies jointly examine sex and attack form.
Hypothesis:
Shoulder asymmetries would differ by attack form, with bow-and-arrow hitters showing greater dominant-nondominant internal rotation (IR) strength and dynamic-stability asymmetry than straight-arm hitters. Second, we expected typical dominant-arm ROM and strength adaptations and greater strength and stability in boys than girls.
Study Design:
Cross-sectional study.
Level of Evidence:
Level 3.
Methods:
We evaluated 108 high school volleyball players (49 boys, 59 girls). Bilateral shoulder ROM, isometric strength, joint position sense, acromiohumeral distance, and dynamic stability (upper quarter Y-balance test [UQYBT]) were assessed. Asymmetry was defined as dominant minus nondominant. Exploratory logistic regression examined associations between attack form (straight vs bow-and-arrow/circular) and shoulder asymmetry, with an additional exploratory female-only subgroup analysis.
Results:
Both sexes showed marked dominant-side adaptations: reduced IR ROM (boys −20.3°, girls −17.6°; both P < 0.001) and increased external rotation (ER) ROM (boys 11.7°, girls 7.7°; both P < 0.001), with decreased total rotational motion. Boys had higher normalized IR and ER strength (P < 0.001) and superior UQYBT performance (P < 0.001), except inferolateral. In exploratory logistic regression, greater IR strength asymmetry (odds ratio [OR], 1.18; 95% CI, 1.01-1.40; P = 0.04) and smaller inferolateral reach asymmetry (OR, 0.92; 95% CI, 0.86-0.98; P = 0.01) were associated with using a bow-and-arrow/circular swing; however, no significant attack-form differences were observed in the exploratory female-only subgroup analysis.
Conclusion:
Characteristic overhead-shoulder profiles - IR loss, ER gain, and preserved ER/IR ratios - are already present in high school volleyball players. Associations between attack form and shoulder asymmetry should be interpreted cautiously and considered exploratory.
Clinical Relevance:
Clinicians may monitor IR ROM, strength balance, and upper-quarter stability to characterize shoulder function in adolescent volleyball players and to identify extreme or symptomatic asymmetries that may warrant individualized conditioning.
Shoulder injuries are common in volleyball due to repetitive, high-force overhead movements, particularly during spiking and serving, which increase the risk of both acute and chronic conditions.6,18,22,26 Understanding the biomechanical factors underlying these injuries is essential for prevention.
In overhead athletes, including volleyball players, shoulder joint function is often asymmetric between the dominant and nondominant arms.3,4,14,17,21 These asymmetries - especially in internal (IR) and external rotation (ER) range of motion (ROM) - are recognized widely as normal adaptations to repetitive overhead motions and may support sport-specific performance.13,28 However, excessive or unbalanced asymmetries may exceed physiological adaptation and have been linked to shoulder pain or dysfunction in some populations, such as baseball pitchers. 28 The distinction between adaptive and maladaptive asymmetries remains unclear in volleyball athletes. Moreover, most previous studies have targeted professional or collegiate athletes and have focused primarily on ROM and strength.14,15,19,21 Although recent work has begun to describe shoulder ROM adaptations and the prevalence of IR deficit in adolescent or high school volleyball players,15,21 comprehensive assessments that also include joint position sense, acromiohumeral distance (AHD), and dynamic stability remain scarce in this age group.
Sex differences in shoulder function are another important consideration. Men and women may differ in ROM, strength, and stability due to variations in biomechanics, muscle mass, and training patterns.5,14,21 These differences highlight the need for sex-specific injury-prevention strategies.21,31 Yet few studies have directly compared male and female athletes, especially in parameters such as AHD, joint position sense, and dynamic stability, which may influence both injury risk and performance.
Attack form - such as straight-arm, bow-and-arrow, and circular swings - may further affect shoulder function and injury risk. While most forms share similar acceleration and follow-through phases, the wind-up and cocking phases differ. 25 For example, the bow-and-arrow swing, characterized by greater trunk rotation, may impose higher demands on the shoulder than the straight-arm swing.11,22 Thus, clarifying the relationship between attack form and shoulder asymmetry is important.
High school athletes represent a unique population, as ongoing physical maturation may interact with training loads to shape shoulder adaptations and injury risk. Taken together, shoulder function asymmetries and sex differences are well documented in overhead athletes. However, to our knowledge, no study has systematically examined these domains in high school volleyball players while also considering specific attack forms. Furthermore, previous work has not adequately addressed how different spiking techniques influence shoulder adaptations or imbalances.10,20,22
Therefore, the primary aim of this study was to examine whether shoulder functional asymmetries are associated with attack form (bow-and-arrow vs straight) in high school volleyball players. We hypothesized that players using a bow-and-arrow swing would show greater dominant-to-nondominant asymmetry in IR strength and dynamic stability than those using a straight-arm swing. As secondary aims, we sought to (1) describe shoulder functional asymmetries between the dominant and nondominant arms and (2) explore sex differences in these adaptations. Clarifying these relationships may help clinicians and coaches design individualized training and injury-prevention strategies tailored to sex and attack form.
Methods
Study Design and Ethical Considerations
This cross-sectional study combined a questionnaire to obtain demographic and volleyball-specific information with a series of shoulder joint function assessments. Data were collected in the gymnasiums of participating high school volleyball teams between March and July 2023. The study adhered to the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) guidelines and complied with the Declaration of Helsinki. Ethical approval was granted by the Institutional Review Board of Saitama Medical University (approval no. 2022-019).
Before data collection, principals and coaches received detailed explanations of the study’s objectives, procedures, and potential implications, and written institutional approval was obtained. Players and their parents or legal guardians were also provided with comprehensive information and given the opportunity to ask questions. Written informed consent was then obtained from both athletes and their parents or guardians, confirming voluntary participation.
Participants
Participants were volleyball players aged 15 years to 18 years from the top 32 schools in the Saitama Prefecture High School Volleyball League, Japan. Nine teams agreed to participate, yielding 108 players (49 boys and 59 girls). To reflect real-world playing conditions, players with pain in the dominant shoulder were eligible if their pain was not severe enough to prevent participation in regular practice. Current shoulder symptoms were recorded using a self-report questionnaire; players were asked whether they currently experienced pain in the dominant shoulder during volleyball activities (yes/no).
Exclusion criteria were: (1) history of spine or limb surgery, (2) current absence from practice due to injury, and (3) history of glenohumeral dislocation. To minimize selection bias, all eligible players on each team, regardless of position, skill level, or pain status, were invited to participate. All 108 players met the inclusion criteria and completed the assessments, and no adverse events occurred during testing (Figure 1).
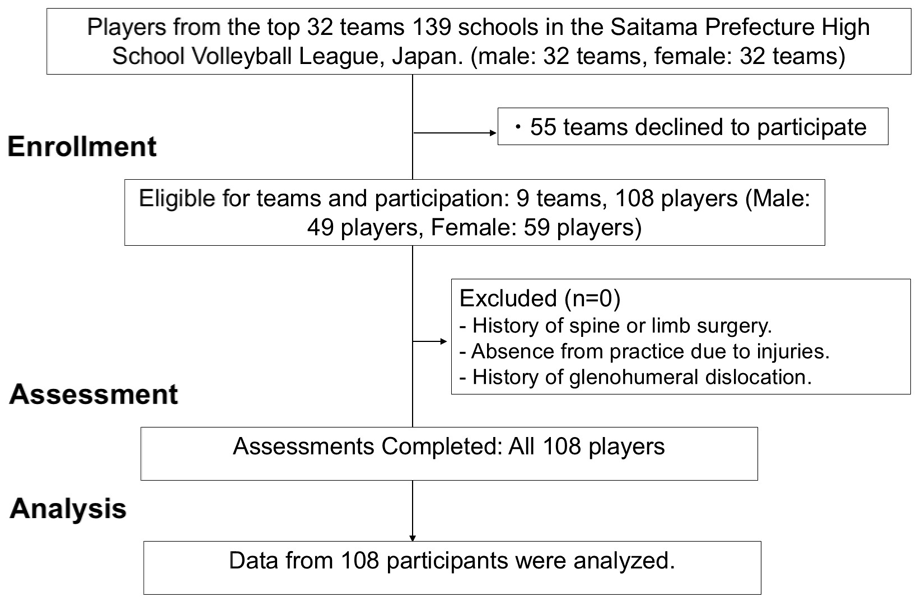
Guideline flow diagram.
Procedure
Demographic Details and Environmental Factors
Demographic variables included age, height (cm), weight (kg), body mass index (BMI, kg/m2), dominant hand, weekly sleep duration, number of sports played during elementary school (≤1 sport vs ≥2 sports), and current dominant-shoulder pain during volleyball activities (yes/no). Dominant hand was defined as the arm used for attack and serve. Sport-specific factors were also assessed: years of volleyball experience; court position (outside hitter, middle blocker, opposite, setter, or libero); number of positions played (1, 2, or ≥3); serve type (float, jump, or hybrid); and attack form (straight, bow-and-arrow, or circular). Self-reported technical factors included single-leg landing during attacks, behind-the-head ball contact, and frequent mistimed hits.
Attack form was verified by video analysis of practice sessions and classified as straight, bow-and-arrow, or circular by a physical therapist and Japan Sport Association-certified volleyball coach.10,25 The primary form used in >80% of attacks was recorded. Definitions of the arm swing techniques were based on previous biomechanical descriptions in elite volleyball players.10,25 In the straight-arm swing, the hitting arm remains relatively extended during the cocking phase with limited trunk rotation, and the wrist of the hitting arm does not rise markedly above shoulder level. In the bow-and-arrow swing, the hitting arm is abducted and externally rotated with the elbow and wrist at or above shoulder height during the cocking phase, while the nonhitting arm is drawn in the opposite direction, resembling a drawn bow. Circular swings are characterized by a more pronounced circumduction of the hitting arm: after an initial elevation to approximately shoulder height, the elbow moves downward and follows a looping path around the shoulder without a distinct stop in the final cocking position before accelerating toward ball contact. Setters and liberos were included in the study because, at the high school level, positional roles are often not strictly divided, and these players frequently practice spikes and serves in a manner similar to attackers during training.
Shoulder Function Assessment
Shoulder function was evaluated bilaterally, including AHD, passive glenohumeral ROM, isometric strength, joint position sense, and the upper quarter Y-balance test (UQYBT) (Figure 2). Asymmetry was defined as the dominant minus the nondominant value. All assessments were performed in a standardized, nonrandomized order by experienced physical therapists. Specifically, AHD, passive glenohumeral ROM, and joint position sense were assessed first, followed by isometric strength and the UQYBT. This sequence was selected to minimize the potential influence of fatigue or exertion from higher-load tasks on the static and lower-load assessments. To minimize measurement bias, examiners were not provided with players’ questionnaire responses (e.g., pain status, attack form, and training history) during testing.
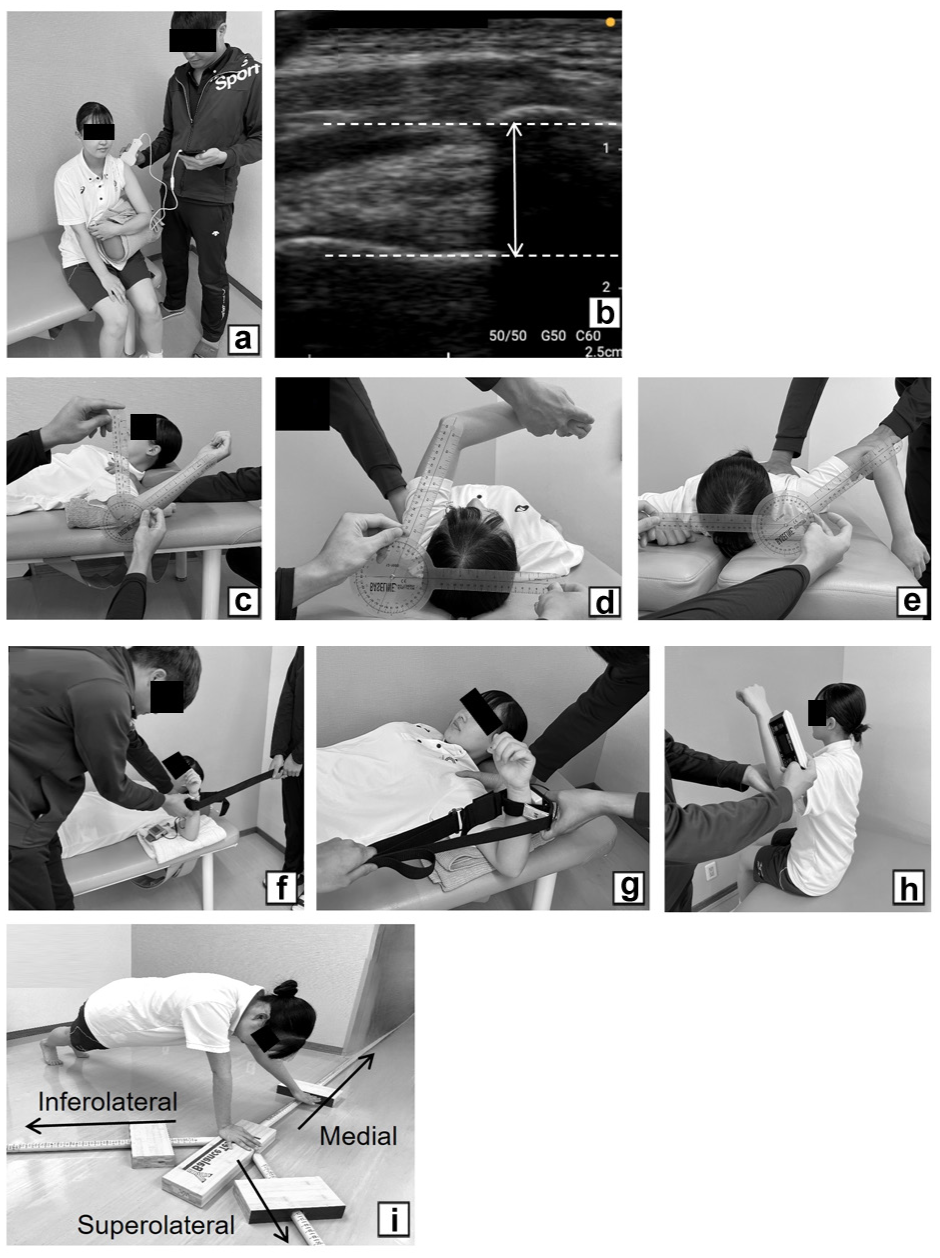
Shoulder joint function assessments. (a) AHD assessment position. (b) Measurement of the AHD on ultrasound image. (c) IR and ER ROM. (d) HAD ROM. (e) HAB ROM. (f) IR strength. (g) ER strength. (h) Joint position sense. (i) UQYBT. AHD, acromiohumeral distance; ER, external rotation; HAB, horizontal abduction; HAD, horizontal adduction; IR, internal rotation; ROM range of motion; UQYBT, upper quarter Y-balance test.
AHD, defined as the distance between the humeral head and the inferior aspect of the acromion, 2 was measured using ultrasound (miruco, NIPPON SIGMAX Co, Ltd) (Figure 2a,b). Participants were seated with the shoulder in 60° abduction, elbow at 90° flexion, and forearm in neutral, resting on a cushion. After palpating the acromion, its midpoint was identified as the landmark for probe placement. The transducer was then positioned over the lateral shoulder in the coronal plane and adjusted until the inferior aspect of the acromion and the superior aspect of the humeral head were clearly visualized in the same image. Three images were obtained from the lateral side, stored, and analyzed with ImageJ. 24 The shortest distance was measured, and the average of 3 trials was used. Previous studies report excellent intrarater reliability (intraclass correlation coefficient [ICC] > 0.90). 2 All AHD measurements were conducted by a physical therapist with >15 years of clinical experience, who had previously completed formal musculoskeletal ultrasound training under the supervision of a sports medicine physician.
Passive ROM was measured bilaterally for IR, ER, horizontal adduction (HAD), and horizontal abduction (HAB) using a Baseline plastic goniometer (12-1000; Fabrication Enterprises Inc; 1° increments) (Figure 2c-e). 8 The shoulder was positioned at 90° abduction. IR, ER, and HAD were measured in supine, and HAB in prone. The scapula was stabilized to prevent compensatory motion. Total rotational motion (TROM) was calculated as the sum of IR and ER. Previous reports indicate good to excellent intrarater reliability for these measurements (ICC 0.85-0.99; variability 4°-7.5°). 8 In the present study, ROM measurements were performed by 1 physical therapist, while scapular stabilization was provided by K.S. for male participants and by S.H. for female participants. Although single-examiner assessments are common in clinical practice, this 2-examiner setup was adopted to enhance measurement accuracy.
Joint position sense of IR and ER was assessed with a Baseline digital inclinometer (12-1057; Fabrication Enterprises Inc; accuracy 0.1°) (Figure 2h). 1 Participants sat without back support, maintaining a neutral trunk. The shoulder was at 90° abduction, elbow at 90° flexion, and forearm in neutral. With eyes closed and wearing a sleeveless shirt, the examiner passively moved the arm to 90% of maximum ROM and held it for 3 seconds. After returning to the starting position, participants actively reproduced the target position. Three trials were performed, and the absolute error was averaged. Previous studies report good reliability (mean ICC = 0.84). 1 All joint position sense assessments in the present study were conducted by a single physical therapist.
Isometric shoulder strength (IR and ER) was measured using a handheld dynamometer with belt fixation (μ-TAS F-1, Anima Inc) (Figure 2f,g). 7 Participants were seated with the shoulder at 90° abduction and the elbow at 90° flexion. A warm-up of submaximal contractions (50% and 75% effort) was performed before testing. 16 Two maximal 3-second contractions were then performed with 10-second rest intervals, and IR and ER tests were separated by 2 minutes. The mean of the 2 trials was used. Values were normalized to body weight (kg force/kg). High intra-rater reliability has been reported previously (ICC = 0.90 for IR; ICC = 0.87 for ER). 7 For isometric strength testing, 2 examiners were involved to enhance measurement consistency: one stabilized the scapula and elbow to prevent compensatory movements, while the other managed the belt fixation.
Dynamic stability was assessed using the UQYBT (FMS Professional Kit, Functional Movement Systems) (Figure 2i). 29 Participants assumed a push-up position and reached with 1 hand in 3 directions: medial, superolateral, and inferolateral. The opposite hand remained in contact with the ground, supporting the body during the test. Each direction was performed 3 times. Reach distances (cm) were normalized to upper limb length (C7 to the tip of the middle finger in 90° abduction) to yield percentage upper limb length (%LL). The composite score was calculated as the mean of the 3 normalized reach directions ×100. Reach distances were measured to the nearest 0.5 cm. Previous studies demonstrate excellent reliability (ICC > 0.99). 29 All UQYBT assessments in the present study were conducted by a single physical therapist.
To verify measurement consistency, a subsample of participants underwent repeated testing by the same examiner. Intrarater reliability in the present study was excellent for all measures (ICC 0.88-0.99); because single‑measure ICCs for passive ROM exceeded 0.90, 1 measurement was deemed sufficient in the main trial.
Sample Size
A priori sample size calculations were performed using G*Power Version 3.1.9.6 (Heinrich Heine University). IR ROM was selected as the reference outcome because it is a key indicator of shoulder adaptation in overhead athletes and the parameter reported most consistently in previous studies of adolescent volleyball players. 21 For within-subject comparisons of dominant and nondominant shoulders, IR ROM values from that study (dominant 60.4° ± 13.6°, nondominant 69.4° ± 13.8°, r = 0.547) indicated an expected mean difference of approximately 9°. Assuming a 2-tailed α of 0.05 and power (1 – β) of 0.80, the required sample size was 19 participants per group (i.e., per sex). For between-sex comparisons of IR ROM, reported values (boys 55.3° ± 14.1°, girls 65.7° ± 10.8°; mean difference ≈10°) yielded a required sample size of 22 participants per sex under the same statistical assumptions. Based on these calculations, we aimed to recruit at least 25 to 30 players of each sex to allow for potential exclusions or missing data. Ultimately, 49 boys and 59 girls were enrolled, exceeding the numbers required for the primary within- and between-sex IR ROM comparisons. We anticipated that asymmetries and sex differences in other functional outcomes (strength, joint position sense, and UQYBT performance) would be of similar or greater magnitude than those reported for IR ROM; therefore, the same sample size was expected to provide at least comparable statistical power for these secondary analyses. Logistic regression analyses examining the association between attack form and shoulder asymmetry were considered exploratory and were not used to determine the a priori sample size; in the final logistic model, the number of events per variable was adequate for an exploratory analysis.
Statistical Analysis
Descriptive statistics were used to summarize participant characteristics. Data normality was assessed with the Shapiro-Wilk test, and parametric or nonparametric tests were applied accordingly. Within each sex, dominant and nondominant sides were compared using paired t-tests or Wilcoxon signed-rank tests. Between-sex differences in shoulder function, asymmetry, and volleyball-specific factors were evaluated using independent t-tests or Mann-Whitney U tests, and χ² tests for categorical variables. Asymmetry for each parameter was defined as the dominant minus the nondominant side.
To explore the association between attack form and shoulder asymmetry, an exploratory binary logistic regression was performed with attack form coded as 0 = straight and 1 = bow-and-arrow/circular. Because only 1 player used a circular swing, bow-and-arrow and circular swings were combined into a single category. Candidate predictors were shoulder asymmetry variables showing between-side differences with P < 0.20 in preliminary analyses; these were entered using a forward likelihood-ratio method (entry P = 0.05, removal P = 0.10). Odds ratios (ORs) with 95% CIs, model χ², Nagelkerke R2, percentage of correct classifications, and the Hosmer-Lemeshow goodness-of-fit test were reported.
To further address the potential confounding effect of sex on the association between attack form and shoulder asymmetry, an additional exploratory subgroup analysis was performed in the female cohort only, in whom the distribution of attack forms was more balanced. 21 Between-group comparisons were conducted for selected shoulder asymmetry variables relevant to the study hypothesis using independent t-tests or Mann-Whitney U tests, as appropriate.
As additional exploratory analyses, we compared key shoulder asymmetry measures (IR ROM asymmetry, TROM asymmetry, IR strength asymmetry, and UQYBT inferolateral reach asymmetry) between players with and without current dominant-shoulder pain using independent t-tests or Mann-Whitney U tests, as appropriate.
All analyses were conducted with IBM SPSS Statistics for Windows, Version 29.0 (IBM Corp). Statistical significance was set at P < 0.05. Effect sizes (Cohen’s d or dz for t-tests, and ORs with 95% CIs for logistic regression) were also calculated. Given the exploratory nature of the study and the large number of comparisons, no formal adjustment for multiple testing was applied; consequently, P values should be interpreted with caution.
Results
The study included 108 participants (49 boys, 59 girls) (Figure 1). Dominant-shoulder pain during volleyball activities was reported by 51 players (47.2%; 19 boys, 32 girls), with no significant sex difference (P = 0.11). Descriptive statistics for demographic characteristics, shoulder function measures, and volleyball-specific factors are shown in Table 1.
Demographics and baseline characteristics
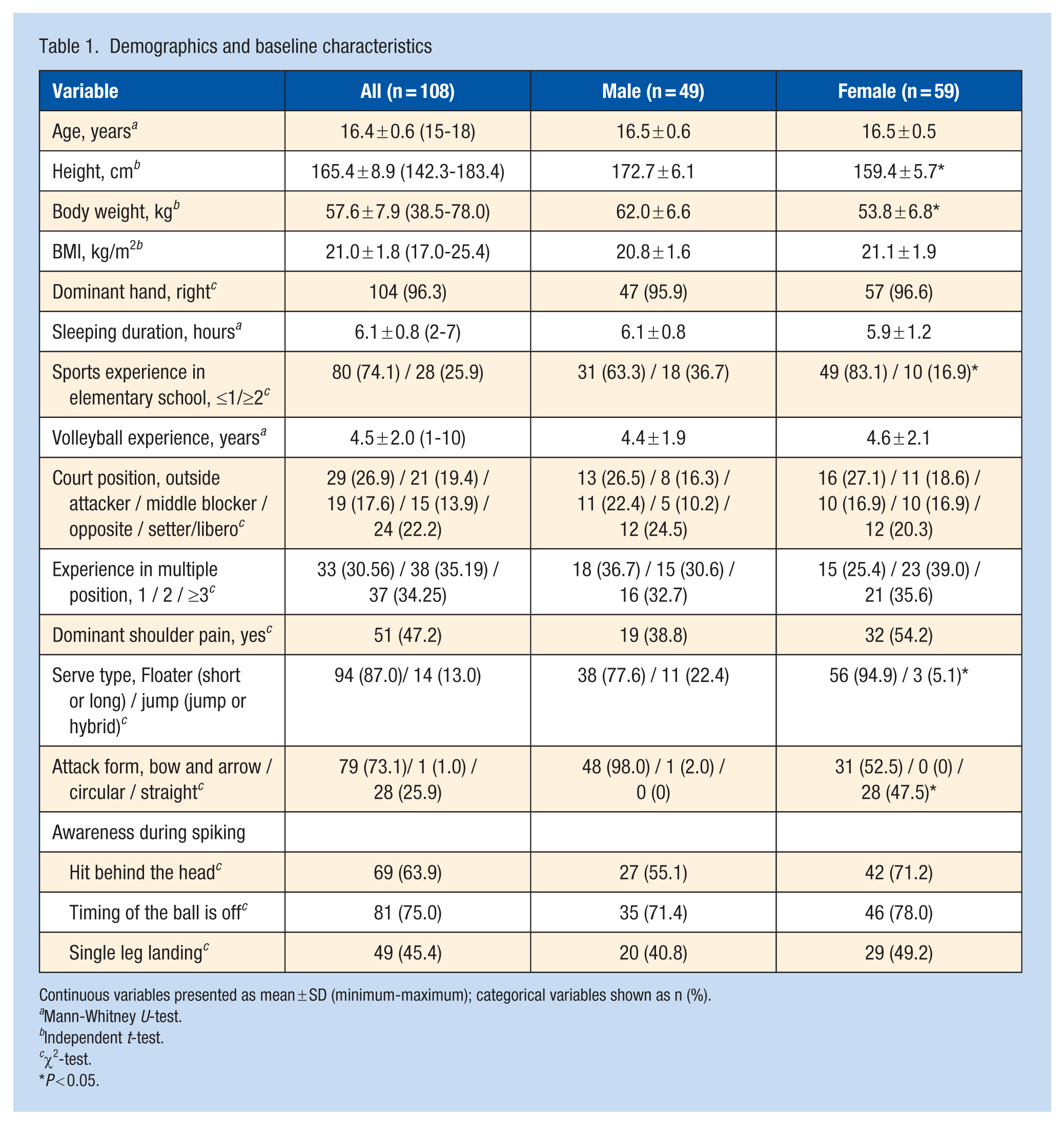
Continuous variables presented as mean ± SD (minimum-maximum); categorical variables shown as n (%).
Mann-Whitney U-test.
Independent t-test.
χ2-test.
P < 0.05.
Comparison of Dominant and Nondominant Shoulder Function by Sex
As shown in Table 2, both sexes exhibited significant dominant-side IR ROM reduction and ER ROM increase, accompanied by reduced TROM. Only boys showed a significant decrease in dominant-side horizontal adduction ROM. Both sexes demonstrated higher IR strength on the dominant side. In the UQYBT, composite scores were lower on the dominant than the nondominant side in both sexes. Boys showed dominant-side reductions in the medial and inferolateral reach directions, whereas girls showed a reduction only in the superolateral direction.
Comparison of dominant and nondominant shoulder function
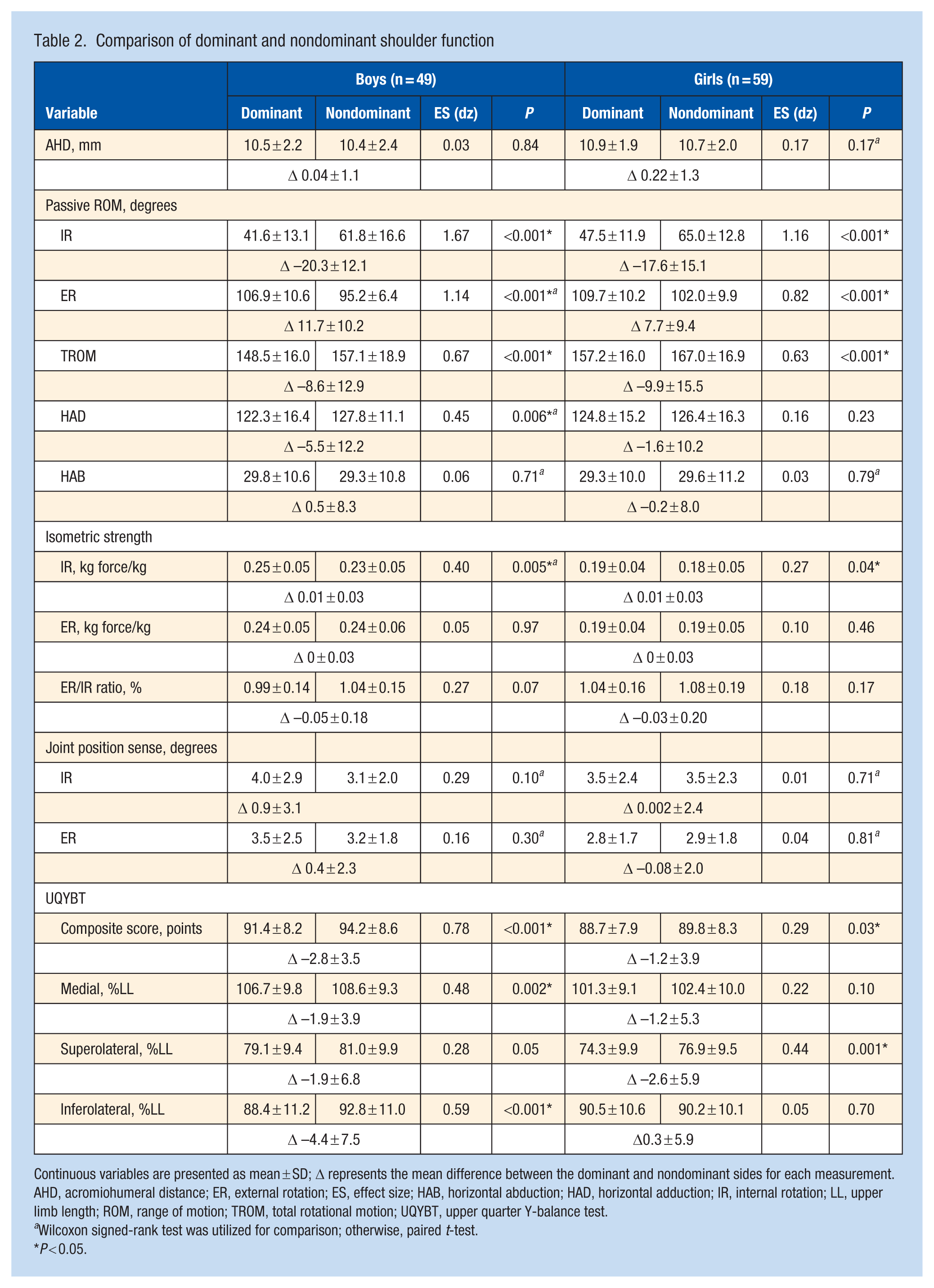
Continuous variables are presented as mean ± SD; Δ represents the mean difference between the dominant and nondominant sides for each measurement. AHD, acromiohumeral distance; ER, external rotation; ES, effect size; HAB, horizontal abduction; HAD, horizontal adduction; IR, internal rotation; LL, upper limb length; ROM, range of motion; TROM, total rotational motion; UQYBT, upper quarter Y-balance test.
Wilcoxon signed-rank test was utilized for comparison; otherwise, paired t-test.
P < 0.05.
Sex Differences in Shoulder Function and Sports-Specific Factor
Table 3 summarizes sex differences. Compared with girls, boys had lower IR ROM on the dominant side, lower ER ROM on the nondominant side, and reduced TROM bilaterally, as well as greater ER ROM asymmetry. Boys also demonstrated higher normalized IR and ER strength on both sides, but there were no significant sex differences in strength asymmetry or ER/IR ratio. In the UQYBT, boys showed higher nondominant composite scores and greater medial and superolateral reach distances bilaterally, whereas inferolateral reach was similar between sexes; however, boys exhibited more negative inferolateral asymmetry, indicating lower dominant‑side reach relative to the nondominant side. Regarding sport-specific factors, boys used jump serves more often and predominantly preferred the bow‑and‑arrow swing, whereas girls more frequently used a straight‑arm swing (Table 1).
Sex difference in shoulder function
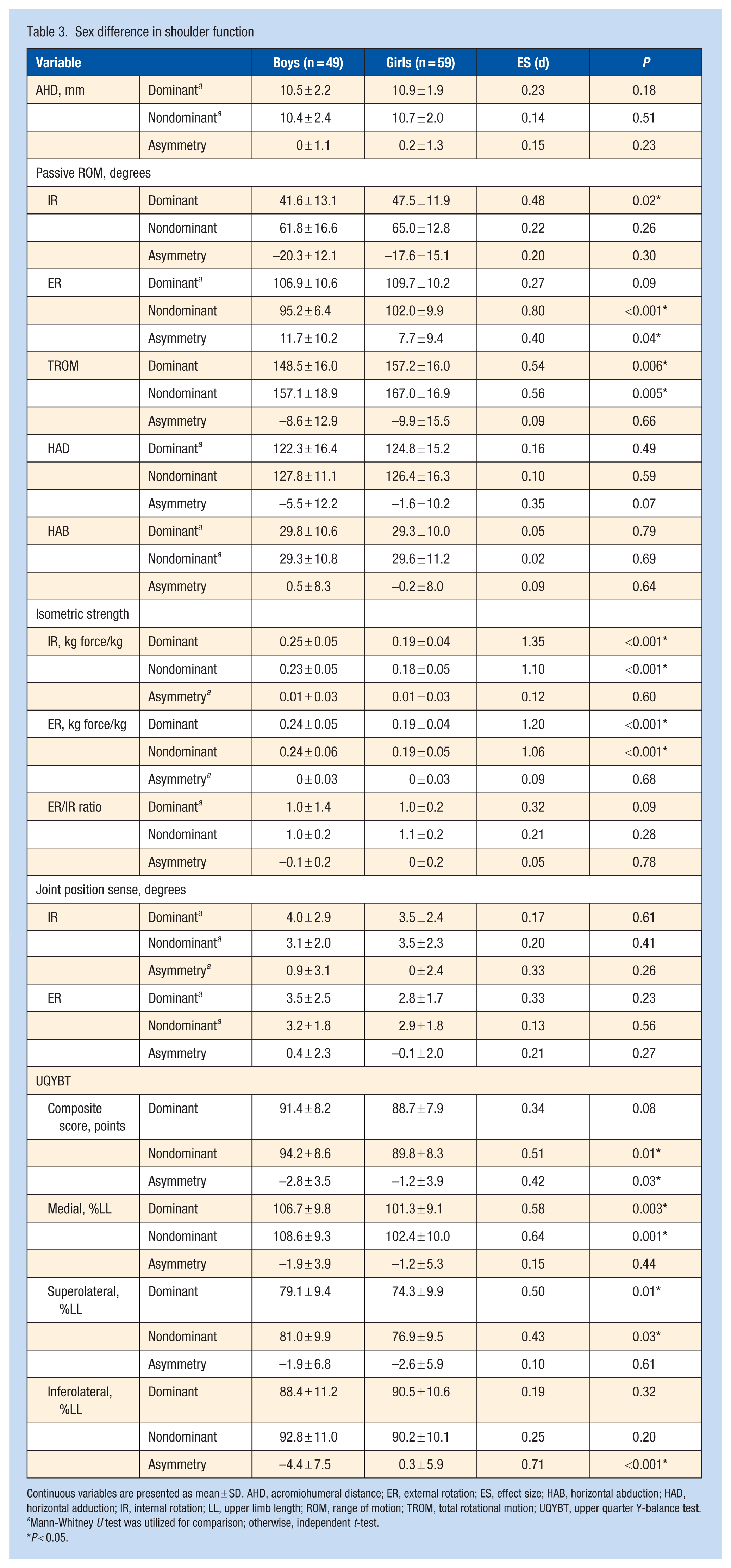
Continuous variables are presented as mean ± SD. AHD, acromiohumeral distance; ER, external rotation; ES, effect size; HAB, horizontal abduction; HAD, horizontal adduction; IR, internal rotation; LL, upper limb length; ROM, range of motion; TROM, total rotational motion; UQYBT, upper quarter Y-balance test.
Mann-Whitney U test was utilized for comparison; otherwise, independent t-test.
P < 0.05.
Relationship Between Shoulder Function and Attack Form
Logistic regression analysis (Table 4) showed a significant overall model fit (model χ2 = 10.11; P = 0.006; Nagelkerke R2 = 0.13; correct classification 74.1%). In this exploratory, unadjusted model, greater IR strength asymmetry was associated with higher odds of using a bow‑and‑arrow or circular swing (OR, 1.18; 95% CI, 1.01-1.40; P = 0.04), whereas greater inferolateral reach asymmetry in the UQYBT was associated with lower odds of this swing pattern (OR, 0.92; 95% CI, 0.86-0.98; P = 0.01). Because most male players used a bow‑and‑arrow or circular swing and most female players used a straight‑arm swing, attack form and sex were highly collinear; including sex in the logistic model produced quasi‑complete separation and unstable estimates, so we report only this unadjusted exploratory model. To further address this issue, an additional exploratory subgroup analysis was performed in the female cohort only, in whom attack-form distribution was more balanced (31 bow-and-arrow vs 28 straight-arm). No significant between-group differences were observed in IR ROM asymmetry (P = 0.70), TROM asymmetry (P = 0.77), IR strength asymmetry (P = 0.07), or UQYBT inferolateral reach asymmetry (P = 0.51), although IR strength asymmetry tended to be greater in the bow-and-arrow group.
Association between shoulder function asymmetry and attack form: logistic regression
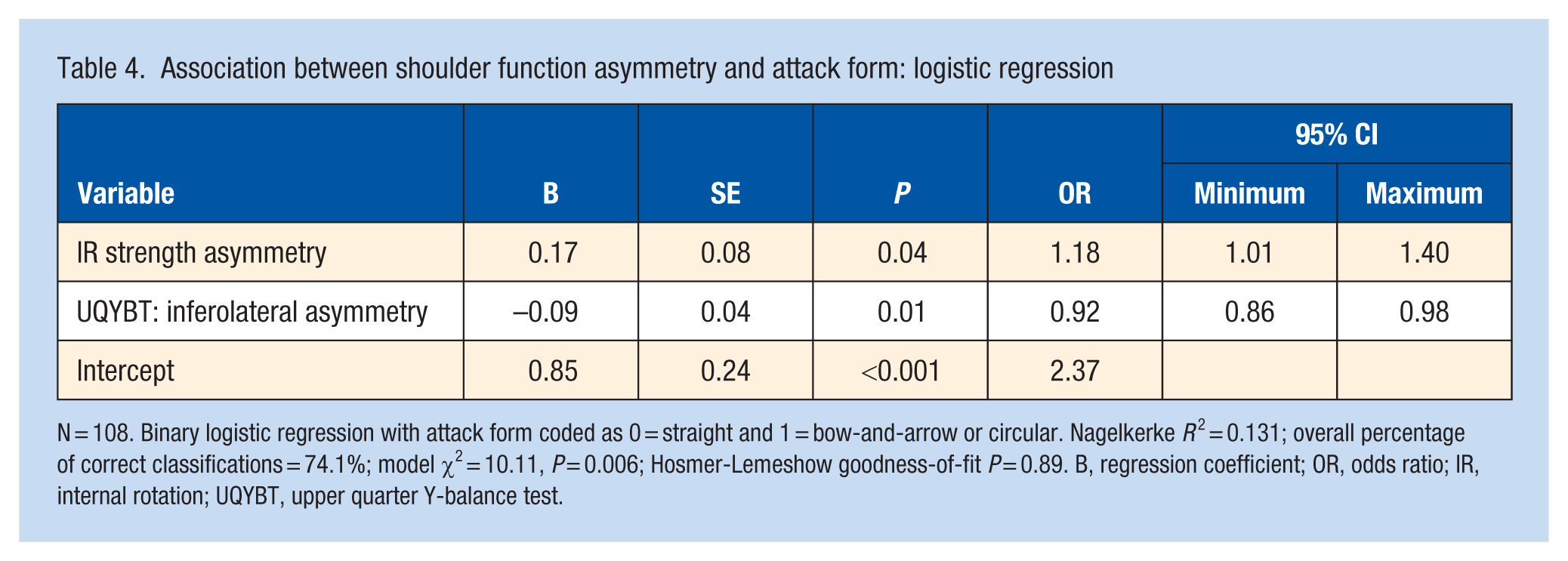
N = 108. Binary logistic regression with attack form coded as 0 = straight and 1 = bow-and-arrow or circular. Nagelkerke R 2 = 0.131; overall percentage of correct classifications = 74.1%; model χ2 = 10.11, P = 0.006; Hosmer-Lemeshow goodness-of-fit P = 0.89. B, regression coefficient; OR, odds ratio; IR, internal rotation; UQYBT, upper quarter Y-balance test.
Exploratory analyses were also performed to examine whether current dominant‑shoulder pain was associated with shoulder asymmetry. Players with and without pain did not differ significantly in IR ROM asymmetry, TROM asymmetry, IR strength asymmetry, or UQYBT inferolateral reach asymmetry (all P > 0.10; data not shown).
Discussion
This study examined shoulder function asymmetry, sex differences, and their relationship to attack form in high school volleyball players. Both sexes demonstrated marked IR and ER ROM asymmetries. Boys showed lower shoulder mobility and higher strength than girls, and players using a bow-and-arrow swing exhibited greater IR strength asymmetry and reduced inferolateral reach asymmetry.
Shoulder ROM Asymmetry
Both male and female players showed clear differences between the dominant and nondominant shoulders, consistent with reports from other overhead sports.3,4,14,17,21 Reduced IR ROM and increased ER ROM on the dominant side reflect adaptations to repetitive overhead actions, aligning with previous work identifying IR deficits and ER gains as common adaptations in overhead athletes.12,17 TROM was also reduced significantly on the dominant side in both sexes. These patterns likely represent sport-specific adaptations to the repetitive demands of volleyball, although extreme values may still be problematic.
The magnitude of the adaptations observed in this cohort (dominant IR deficits of approximately 18° to 20° and TROM reductions of about 9°) falls within the range reported in collegiate and professional volleyball players and other overhead athletes.3,4,14,17,21,31 Previous studies in older volleyball cohorts have described similar dominant-side IR loss and ER gain with modest TROM asymmetry,15,21 suggesting that these sport-specific changes are already established by late adolescence. Our findings therefore extend the existing literature by indicating that “adult-type” glenohumeral rotation profiles are present in competitive high school players, rather than emerging only at the university or professional level.
Sex Differences in Mobility and Strength
Male players demonstrated lower IR ROM on the dominant side, lower ER ROM on the nondominant side, and reduced TROM bilaterally, indicating less flexibility compared with female players. This may relate to differences in muscle mass and training load.21,23 Previous research indicates that men often present with relative hypomobility, whereas women may be more susceptible to joint hypermobility, including at the shoulder. 21 These sex-specific patterns suggest that male athletes may benefit from flexibility programs, whereas female athletes may require greater emphasis on stabilization and strengthening to manage excessive ROM and maintain joint integrity during overhead actions. Importantly, these mobility patterns mirror those reported in university and professional volleyball players,21,31 indicating that the combination of relatively restricted rotation in men and greater laxity in women is already evident by the high school level. Thus, sex-tailored flexibility and stability strategies commonly recommended for older athletes may need to be implemented earlier in the developmental pathway.
For isometric strength, male players exhibited significantly greater IR and ER strength on both sides, likely reflecting larger muscle mass and higher absolute loading.14,23 However, no sex differences were observed in strength asymmetry or the ER/IR ratio, indicating balanced rotational strength across sexes. This pattern of higher absolute rotational strength but comparable ER/IR ratios is consistent with findings in collegiate and elite volleyball players, 14 suggesting that relative rotational balance is maintained across the performance spectrum, even though absolute strength scales with sex and body size. Although IR deficits are considered normal adaptations to repetitive overhead activity and not necessarily injury-related in volleyball, 6 an ER/IR ratio <1.0 has been associated with long-term injury risk. 9 In this study, the dominant-side ratio was 0.99 in boys and 1.04 in girls, suggesting that some athletes may fall within a potentially vulnerable range and warrant ongoing monitoring.
UQYBT Performance
Male players achieved longer reach distances than female players in the medial and superolateral directions on both sides but also demonstrated greater asymmetry, with shorter inferolateral reach on the dominant side. This pattern may result from limited IR ROM, which restricts the shoulder flexion required for inferolateral reach, leading to performance in this direction that is comparable with female players despite superior performance in the other directions. These results suggest that male and female athletes adapt shoulder function differently to meet sport demands and that direction-specific UQYBT performance may provide more nuanced information than composite scores alone when designing tailored training and injury-prevention programs.
Attack Form and Shoulder Function
Our findings suggest that attack form may be associated with shoulder function asymmetry; however, these results should be interpreted cautiously. In the full cohort, an exploratory logistic regression model showed that players using a bow-and-arrow or circular swing had greater IR strength asymmetry and smaller inferolateral reach asymmetry. Because attack form and sex were highly overlapping in the full cohort, however, it was difficult to distinguish the effect of attack form from sex-related characteristics. To further address this issue, we performed an additional exploratory subgroup analysis in the female cohort, in whom attack-form distribution was more balanced. No significant between-group differences were observed in IR ROM asymmetry, TROM asymmetry, IR strength asymmetry, or UQYBT inferolateral reach asymmetry, although IR strength asymmetry tended to be greater in the bow-and-arrow group. These findings do not provide clear support for an independent effect of attack form in the female cohort, although the tendency toward greater IR strength asymmetry in bow-and-arrow hitters was directionally consistent with the full-cohort model. Accordingly, the present findings regarding attack form should be considered exploratory and hypothesis-generating. Previous work has linked reduced ER/IR ratios to long-term injury risk in overhead athletes, and to subacromial space narrowing.14,27,30
Monitoring IR strength asymmetry, ER/IR ratios, and direction-specific UQYBT performance may help characterize shoulder function in players with different attack forms. In the present study, the findings do not clearly support routine efforts to increase dominant-side IR strength or ROM in bow-and-arrow hitters solely to match a presumed technique profile. Rather, clinicians may consider monitoring athletes with extreme or symptomatic asymmetries and addressing these findings with individualized programs that emphasize IR/ER balance, scapular control, and kinetic-chain coordination.
Limitations
This study has several limitations. First, its cross-sectional design precludes causal inference between shoulder asymmetry, sex differences, attack form, and injury risk. Longitudinal studies are needed to determine whether these adaptations contribute to shoulder injuries or performance changes. Second, participants were high school volleyball players from a single prefecture, mainly top-performing teams, which may limit generalizability to other regions, levels, or recreational athletes. Third, although multiple shoulder function parameters were assessed, other biomechanical factors such as scapular kinematics, thoracic spine mobility, and kinetic-chain contributions were not evaluated. Fourth, attack forms were classified from video of practice sessions, and individual variations in swing mechanics and competition-specific adaptations could not be fully captured. Fifth, current dominant-shoulder pain was recorded only as a yes/no variable, and exploratory comparisons between players with and without pain were underpowered; pain severity, duration, validated shoulder-specific outcome scores, and detailed injury history were not collected, so the absence of clear differences in asymmetry by pain status should not be interpreted as evidence that these adaptations are benign. Sixth, the logistic regression relating attack form to shoulder asymmetry was exploratory and unadjusted for sex; in this sample, attack form and sex were highly collinear, and sex-adjusted models showed quasi-complete separation and unstable estimates. Although we also performed an exploratory female-only subgroup analysis to reduce confounding by sex, that analysis did not provide clear support for an independent effect of attack form and was limited by the modest subgroup sample size. Finally, we performed numerous between-side and between-sex comparisons without formal correction for multiple testing, so some statistically significant findings may represent type I error and should be viewed as hypothesis-generating rather than confirmatory. Despite these limitations, the present findings advance understanding of shoulder function in high school volleyball players and may inform training strategies tailored to sex, attack form, and functional asymmetry.
Conclusion
High school volleyball players demonstrated marked shoulder functional asymmetries, sex differences, and associations between attack form and IR strength and dynamic stability. The magnitude and pattern of IR, ER, and TROM adaptations were broadly similar to those reported in collegiate and professional volleyball players, suggesting that characteristic overhead-shoulder profiles are largely established by the high school years. Although such adaptations may contribute to mechanisms underlying shoulder problems, their direct link to injury risk remains uncertain and requires confirmation through longitudinal studies. Routine monitoring of rotation ROM, strength balance, and dynamic stability may help clinicians and coaches design sex- and attack form-specific conditioning programs that optimize performance while minimizing undue stress on the shoulder.
Supplemental Material
sj-docx-1-sph-10.1177_19417381261457121 – Supplemental material for Functional Shoulder Adaptations and Attack Form in High School Volleyball Players: Sex Differences in Range of Motion, Strength, and Dynamic Stability
Supplemental material, sj-docx-1-sph-10.1177_19417381261457121 for Functional Shoulder Adaptations and Attack Form in High School Volleyball Players: Sex Differences in Range of Motion, Strength, and Dynamic Stability by Yasuaki Mizoguchi, Kenta Suzuki, Seita Hasegawa, Naoki Shimada, Toby Hall and Kiyokazu Akasaka in Sports Health
Footnotes
Acknowledgements
The authors would like to thank the coaches and players of the high school volleyball clubs in Saitama, Japan, for their valuable cooperation.
The authors report no potential conflicts of interest in the development and publication of this article.
Ethics and Consent Declarations
All procedures performed in studies involving human participants were in accordance with the ethical standards of the institutional review board of the Saitama Medical University (Approval No. DAI 2022-019, 20/1/2024) and with the 1964 Helsinki Declaration and its later amendments or comparable ethical standards. Informed consent was obtained from all participants and their legal guardians after detailed explanations were provided to high school principals, coaches, players, and parents. Written consent included agreement to participate in the study and for data publication.
Clinical Trial Registration
This study has been registered as a clinical trial with the Universal Medical Information Network (UMIN) under the registration number UMIN000049517.
Data Availability Statement
The datasets generated and/or analyzed during the current study are available from the corresponding author on reasonable request.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.