
Abstract
Anterior cruciate ligament (ACL) injuries represent one of the most devastating diagnoses in sports -degrading abilities, shortening careers, and jeopardizing financial potential.5,10,12 Despite proliferating prevention strategies, injury rates in professional sport continue to rise, with annual increases of ~6% reported in elite football. 12
ACL mechanisms were classified historically as direct contact, involving an impact to the knee, and noncontact (NC), not involving impact to the knee. This binary approach failed to distinguish, define, and capture incidental player-to-player interactions not involving the knee (bumps, pushes, pulls, hand-offs, mid-air collisions) that nonetheless disrupted control at the knee. Such contacts often appear insignificant and are classified commonly as NC injuries. They are often subtle, unanticipated by the player, and frequently overlooked in monitoring contexts. Yet, although seemingly trivial, these consequential contacts can immediately and catastrophically destabilize postural control and instantly derail planned movement strategies.
Although Marshall 7 addressed this ambiguity by categorizing these indirect contact (IC) events as a distinct injury mechanism, many studies and surveillance systems still ignore and/or conflate IC and NC injuries.
Despite this lack of attention, current evidence illustrates that IC mechanisms:
(1) drive a substantial proportion of ACL injuries (25% to 33% of all cases) in competitive field sports 10 ;
(2) clearly differ from the mechanisms underpinning direct contact and NC injuries7,9,10; and
(3) are unlikely to be reduced via implementation of conventional prevention programs that fail to address the unique mechanical and neurocognitive challenges triggering IC events.5,9
This editorial emphasizes the need for customized prevention and rehabilitation programs specifically addressing the unique challenges associated with IC ACL mechanisms.
The IC ACL Injury Cascade
Safe and efficient human movement relies on continuous anticipatory postural adjustments that prepare contractile and structural tissues for upcoming movement challenges. These pre-emptive activations, informed by previous experience and contextual awareness, regulate joint positioning and coordinate the muscular co-contractions required to stabilize the knee in advance of predicted neuromechanical perturbations.3,5 However, incidents triggering IC events are frequently unexpected and inherently unpredictable.
Video analyses reveal ACL injuries most frequently occur during moderate-to-high-speed scenarios and while decelerating, changing direction, pivoting, or landing.3,8,10 NC scenarios typically involve stabilization failures, driven by compromised coordination. IC injury mechanisms, however, are driven by unexpected movement volatility - unforeseen bumps and incidental nudges. These unanticipated perturbations can lead to a rapidly propagating cascade of local destabilizations that outpace the neuromuscular system’s capacity to restabilize. When overwhelmed, planned movement sequences are instantly derailed, and the coordinated interplay between the trunk, pelvis, and limbs collapses.
When destabilization spreads, the trunk may laterally flex or rotate, shifting the center of mass away from the planted foot. This shift increases rotational and valgus stress at the knee. If the knee is relatively straight during this chaotic collapse, the likelihood of ACL rupture rises sharply. 9
This injury cascade unfolds rapidly (~30-50 ms), 8 too quickly for involuntary reflexes (~30-80 ms),4,8 and/or voluntary activations (>170 ms) to intervene and buffer unanticipated perturbations, 4 restoring stability. Cumulative forces rapidly converge on a poorly positioned ACL. When the ligament’s tensile strength (~1800 Newtons) is exceeded, rupture occurs. 1
This situation is intensified by elevated neurocognitive load, stemming from the complex and dynamic demands of decision-making and information processing. 11 When neurocognitive resources are consumed by other attention-demanding tasks, central nervous system responsiveness to external perturbation diminishes, further compromising the ability to quickly restore coordinated control.3,5,10,11 Attentional overload, when coupled with unexpected perturbations, subsequently escalates ACL vulnerabilities (Figure 1).
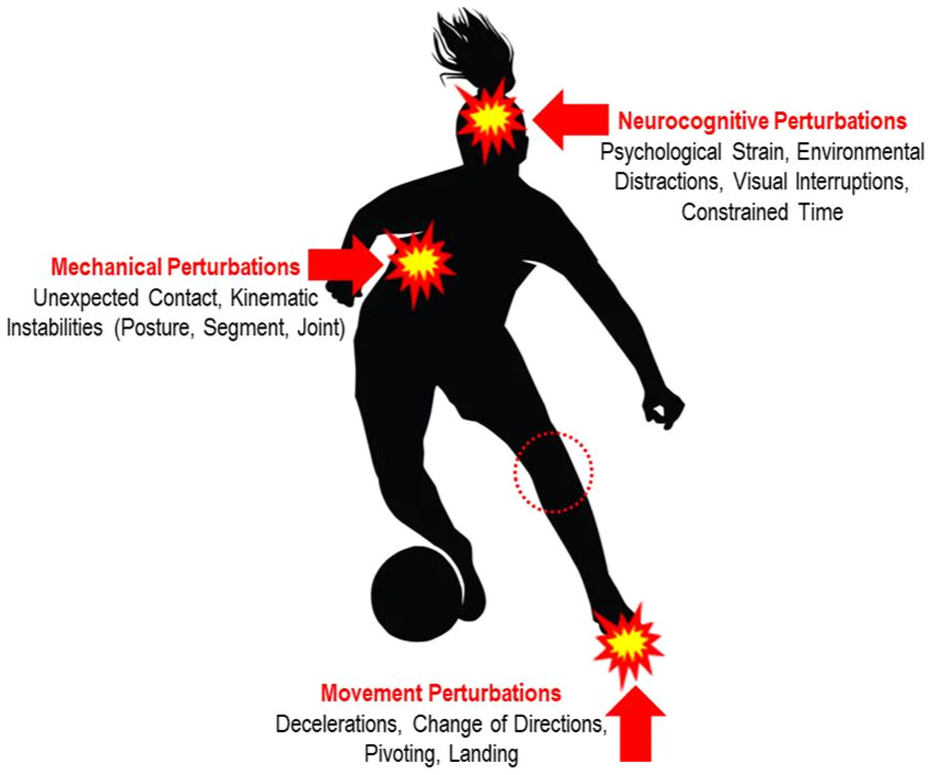
Indirect contact injury mechanisms.
Together, these insights:
(1) underscore the need for mechanism-specific strategies in preparing for unpredictable disruptions;
(2) highlight why conventional prevention training modalities (comprised of preplanned, predictable movement challenges) fail to adequately replicate in-game IC scenarios; and
(3) reinforce the necessity of integrating biomechanical robustness and neurocognitive responsiveness into proactive prevention and rehabilitation strategies.
Closing the Gap: IC ACL Injury Prevention and Rehabilitation
Conventional ACL prevention paradigms target performance capacities during preplanned, predictable movement tasks. 5 These training designs do not address the unanticipated, rapid-onset cascade of events typical of IC ACL injuries.
Such injury prevention programs (e.g., FIFA 11+, PEP) successfully reduce ACL injuries by conditioning players to better manage anticipated movement challenges. 6 Yet no investigation and validated initiatives safely, gradually, and progressively expose players to the unpredictable, externally triggered perturbations characterizing many IC injuries.
Although emerging prevention approaches increasingly incorporate decision-making, visual distraction, and movement variability, these strategies target primarily neurocognitive and/or self-initiated movement perturbations. 11 Practitioners rarely expose athletes to unexpected external mechanical disturbances applied to the trunk or a noninjured limb, the defining feature of many ICs. 9 As a result, critical failure results as these mechanisms remain undertrained.
Although the prevalence of IC ACL injuries is increasingly acknowledged, there are no validated prevention protocols specifically targeting IC injury mechanisms. Accordingly, despite decades of preventive program implementation, the incidence of IC ACL injuries remains unchanged.
Notably, the persistent sex imbalance, evident within the ACL-injury research, exacerbates these shortcomings. Female athletes sustain ACL injuries at rates 2 to 8 times higher than male athletes, yet less than half of study participants are female. 2 This mismatch limits our understanding of IC injury mechanisms, constrains the generalizability of findings, and perpetuates existing sex inequalities.
To address this mismatch between existing preventive paradigms and IC ACL injury mechanisms, 3 priorities emerge:
Standardize IC classification - promote robust surveillance by integrating enhanced technologies enabling accurate detection, categorization, and reporting of IC events; thereby supporting reliable epidemiology, cross-sport comparisons, and mechanism-specific research.
Develop and research IC-specific prevention and rehabilitation programs - design protocols that systematically and gradually expose athletes to unpredictable, externally triggered challenges, potentially through neuromuscular training and technology-enabled simulation; thereby more authentically replicating IC-imposed challenges.
Address non-movement risk factors - incorporate neurological and psychophysiological monitoring into screening protocols, prevention, and rehabilitation strategies to develop personalized, multidimensional, and sex-specific strategies for IC injury risk reduction.
Key Takeaways
The unpredictable, rapid-onset cascade driving many IC ACL injuries reveals a key limitation of traditional prevention methods. The challenges presented by IC mechanisms are substantial, and complete prevention is unlikely. Nevertheless, a better mechanistic understanding and more intelligent deployment of emerging technologies, along with creative training designs, may foster interventions capable of reducing injury rates and protecting athletes’ livelihoods. While such approaches may enhance neuromuscular robustness across multiple injury mechanisms, this editorial does not propose reactive or game-based training as novel. Instead, it highlights that IC injuries possess a distinct perturbation profile that has yet to be isolated or systematically incorporated into existing prevention paradigms.
IC injuries are not simply reactive injuries but rather injuries due to disrupted control, in which externally imposed forces abruptly override feedforward neuromuscular regulation. Effective translation of these insights into practical contexts demands integrated collaboration among medical and performance staff, coaches, biomechanists, and neuroscientists. This team-based approach is essential to fulfill the scientific community’s commitment to enhancing player welfare. The glaring sex imbalance within ACL research undermines the development of effective and equitable prevention strategies. Closing this disparity should be an urgent priority.
Meaningful progress hinges on our collective willingness to reimagine injury prevention designs, leverage emerging technologies, and innovate beyond traditional methodologies to address the unpredictable, rapidly unfolding nature of IC mechanisms.