
Abstract
Context:
Injury to the anterior cruciate ligament (ACL) causes substantial long-term disabilities for athletes. Exercise methods like plyometrics have been considered ideal due to their neuromuscular and motor control benefits.
Objective:
This systematic review aims to provide practitioners with criteria for starting to perform plyometric training exercise (PTE) after ACL reconstruction (ACLR).
Data Sources:
A review of relevant literature was conducted using PubMed, Cochrane Library, and PEDro.
Study Selection:
Based on a set of criteria, only relevant randomized controlled trials were included in the study from inception to March 18, 2026.
Study Design:
Systematic review of randomized clinical trials.
Level of Evidence:
Level 1.
Data Extraction:
An appropriate form was developed and tested for collecting data from the literature to answer the current question. As part of the risk of bias assessment, an updated version of the Cochrane tool was used, and the GRADE approach was applied.
Results:
Of the studies’ outcomes, 63% raised some concerns about bias. Across 16 studies, 685 participants (70% men, 30% women) were included, with a mean age of 25.23 years. PTE began on average after 13.50 weeks post-ACLR as reported in 14 studies. A number of criteria were considered when starting PTE, including clinical, strength, performance, biomechanics, and patient-reported outcomes.
Conclusion:
Programs of plyometric training have been reported to start on average 13.50 weeks after ACLR. There is still a need to conduct more research to establish the validity of the proposed assessment criteria to start plyometric exercises in a safe manner. This study’s findings may enable PTE to be implemented more practically in ACL rehabilitation programs, which reduces the gap between research and practice.
Anterior cruciate ligament (ACL) tear is a common knee injury during sports participation. 43 Injuries to the ACL occur at a rate of 2.8 to 3.2 per 10,000 hours of exposure to different sports. 50 Young female athletes have shown a higher rate of getting ACL injuries (0.7 injury per season) than young male athletes (0.4 injury per season) during a playing season. 54 The risk of ACL reinjury for young athletes has been estimated to be 15 times after return to sport within 1 year and 6 times within 2 years.19,31
Approximately 25% of athletes who sustained an ACL injury could not participate at their preinjury level in sport, while 65% could not continue participation.7,38 Some athletes with ACL reconstruction (ACLR) have experienced an impairment and symptoms from moderate to severe during walking (31%) and stair-climbing (44%).35,38 According to Noyes et al, 35 walking activities increased joint swelling 5-fold, while recreational sports activities increased swelling 4-fold in athletes who were injured 11 years earlier.
Rehabilitative intervention is one of the most crucial recovery strategies after ACLR. 30 Injured athletes seek to return to sports as soon as possible and reduce reinjury risk. 30 The use of plyometric training is an important element in ACLR rehabilitation, 44 as plyometric exercises can help restore neuromuscular performance during late-stage rehabilitation. 8
There are no suggestions in the literature on how and when athletes with ACLR can progress to plyometric training during functional recovery. 30 However, the return to training after ACLR is a critical milestone in the rehabilitation process. In any case, the progression criteria of the rehabilitation protocol should not consider solely the timeframe after ACLR alone; measurement criteria should also be taken into account. The research question was: “Are there any specific methods or criteria for determining when athletes can resume plyometric training after ACLR?”. This systematic review aims to provide practitioners with suggestions for criteria to return to plyometric training. As a result, plyometric training programs can be implemented more practically, thereby reducing the barriers between research and practice.
Methods
This systematic review was conducted in accordance with the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) 2020 statement, 39 as per the recommendation of the Cochrane Collaboration. Guidelines of Prisma in Exercise, Rehabilitation, Sport medicine and SporTs science (PERSiST) were also considered. 2 This study was registered in the International Prospective Register of Systematic Reviews (PROSPERO Registration No: Study ID, CRD42023432145)
Eligibility Criteria
This systematic review includes studies on rehabilitation after ACLR in an adult population. Only studies published in the English language in peer-reviewed journals were considered. The language restriction was based on previous studies showing that when non-English publications were excluded from evidence syntheses, similar conclusions were reached.34,36 Only randomized controlled trials were included (highest level of evidence) in the study, and the outcome measures contained strength, pain, range of motion, patient-reported outcome measures, swelling, laxity, functional activities, adverse events, and return to activity.
Participants with musculoskeletal injuries (such as ankle or hip injuries) were excluded from the study. In addition, studies involving pediatric interventions after ACLR, as well as those using animals, cadavers, or laboratory-based experimental models, were excluded. A variety of studies were also excluded, including systematic reviews, meta-analyses, nonrandomized trials, observational studies, case reports, medical record analyses, narrative reviews, editorials, and letters. Studies that did not report relevant outcomes or that focused exclusively on concomitant injuries (e.g., meniscal rehabilitation) were also excluded.
Search Strategy
PubMed, Cochrane Library, and PEDro databases were searched to find pertinent literature relevant to the study from inception to March 13, 2026. The search was performed in the database with keywords (search criteria used in each database is available as Supplemental Material in the online version of this article) and Boolean operators were used to identify relevant literature. Medical terms (MeSH) and search manager were used to find studies in a more comprehensive and precise manner.
Study Selection
Potentially eligible articles were selected independently by 2 reviewers. Each reviewer independently screened for eligibility all titles and abstracts (using EndNote X9) of all randomized controlled trials that were identified. For the final selection of studies, 2 reviewers independently reviewed the full texts of all potentially relevant studies. Whenever there was a disagreement between 2 reviewers, a third reviewer was consulted to reach an agreement. In addition, the references from selected studies were read and explored to find more related studies.
Quality Assessment of Studies
An updated version of the Cochrane tool for the assessment of the risk of bias in randomized trials (RoB Version 2.0 [ROB2]) was used for risk of bias assessment. 52 The ROB2 Excel sheet was independently used by 2 reviewers. A signaling question was used to identify 5 domains of bias concerns. The overall signaling questions were then used to determine the overall bias risk (high, low, some concern). A third reviewer was consulted about debates in the initial risk of bias ratings until an agreement was reached.
To assess the quality of the body of evidence, the Grading of Recommendations, Assessment, Development and Evaluation (GRADE) approach was used. The first step was to determine and classify all potentially important patient outcomes in accordance with the GRADE guidelines (details in Supplemental Material, available online). A set of criteria for assessing the quality of evidence was also used. The certainty of the evidence for each comparison and outcome was rated as high, moderate, low, or very low based on the risk of bias, inconsistency, indirectness, and imprecision. 47 As part of the publication bias assessment, a funnel plot was to be used for meta-analyses that included ≥10 trials. 24 An online GRADEpro Guideline Development Tool (https://www.gradepro.org/) was used to assess the body of evidence and create summary tables.
Data Extraction and Collection
A specific form, which includes author, study design, population (sample size, sex, and age), groups, type of graft, period of intervention, time for starting plyometric, criteria for return to plyometric training, outcome measure of study and adverse event, was designed to collect data from the literature for answering the current question. During the data extraction and collection phase, 2 reviewers worked independently from each other and consulted a third reviewer when necessary to decide each study’s quality and eligibility. The extraction form was pilot-tested before extracting information from the articles. The information obtained from data extraction was summarized primarily in a table as a qualitative synthesis for this systematic review. In addition, a meta-analysis (quantitative synthesis) was to be conducted when ≥2 studies met the criteria for clinical homogeneity. 13
Data Items
Data were extracted for all predefined outcome measures of interest. No restrictions were imposed on the measurement instrument or scale used in the eligible studies, or on the duration of follow-up, and outcome data were collected at all reported timepoints.
Statistical Analysis
To conduct the meta-analysis, Review Manager (RevMan), developed by the Cochrane Collaboration, was used. In healthcare research, RevMan supports rigorous systematic review preparation and statistical analysis. In addition, it allows structured data input, analysis of findings using fixed-effects and random-effects models, and generation of outputs such as forest plots. Furthermore, the software facilitates the assessment of between-study heterogeneity (e.g., using the I2 statistic) and the evaluation of risk of bias in compliance with established methodologies. The latest version of RevMan Web can be accessed via the official Cochrane website (www.cochrane.org). RevMan Web is a web-based platform that facilitates collaborative workflow, and it provides advantages such as automatic updates, secure data management, and seamless integration with other Cochrane resources. This enhances efficiency, transparency, and reproducibility of the review process.
Results
Study Selection
Based on a database search of relevant literature reviews, 17,860 reports were identified as potentially useful for the study. To remove duplicate reports, EndNote X9 software (n = 1633) was used; thereafter, titles and abstracts of the remaining unique reports (n = 16,227) were screened. A total of 93 full reports were retrieved and assessed for eligibility. Of these, 16 studies were included and reported in the systematic review (Figure 1).
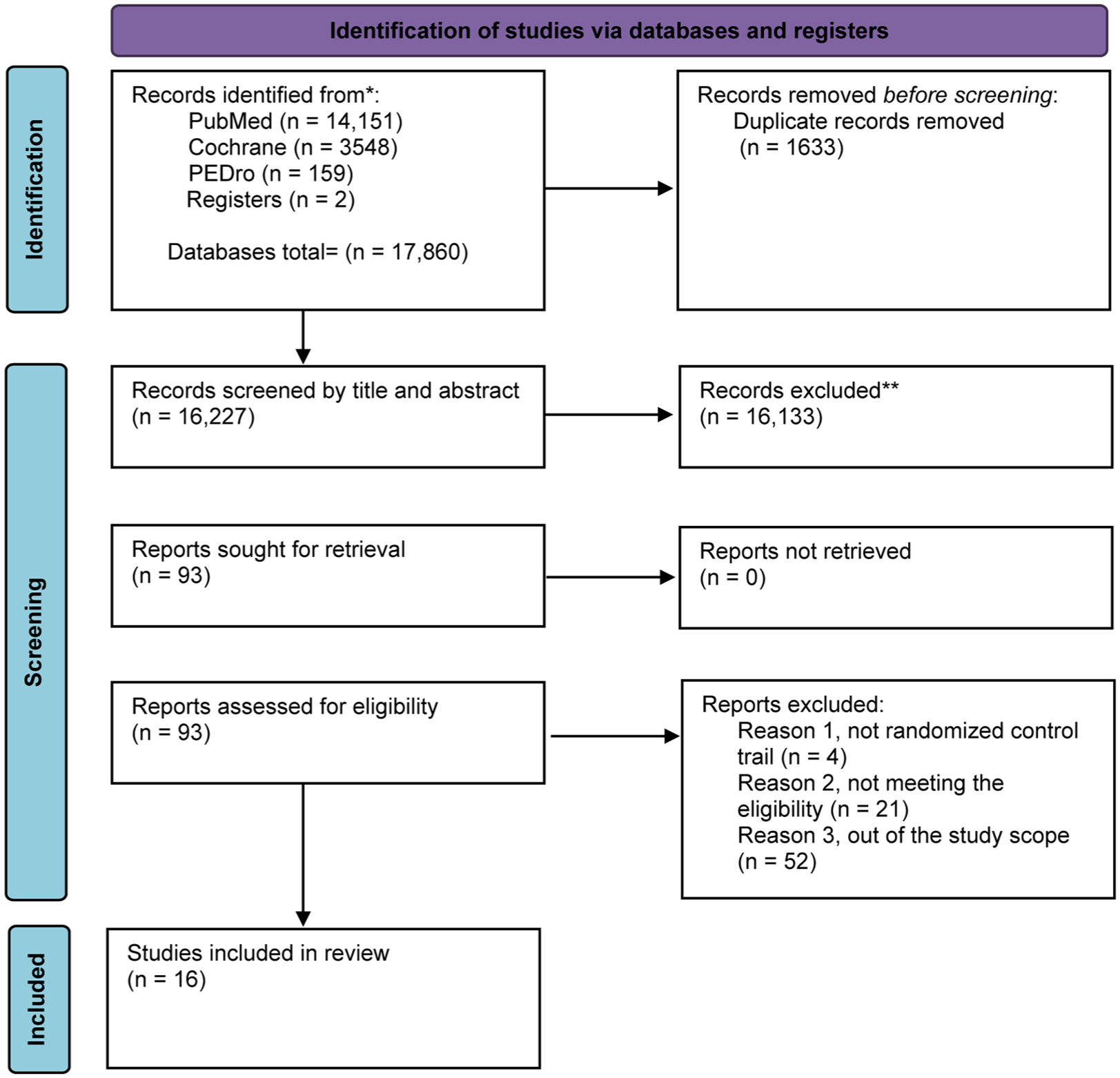
Flowchart for the systematic review.
Study Characteristics
Detailed descriptions of the 16 included studies are provided in the Supplemental Material, available online.3,5,9,10,16 -18,25 -29,44,45,48,51 The total sample size was 685 participants, of which 70% were men and 30% were women. Participant mean age was 25.23 (±4.34) years. The grafts used for the majority of the operative interventions (80%) for the participants were hamstring tendon autograft (HS; 45.40%) and bone-patellar tendon-bone (BPTB; 34.60%). In the remaining participants, different types of grafts were used, including allografts and autografts (15.04%), tibialis anterior tendon allografts (4.67%), and cadaveric grafts (0.29%). However, in 13 studies, functional training exercises incorporating plyometrics were compared with conventional rehabilitation programs.5,10,16,18,25 -29,44,45,48,51 One study compared the plyometric training exercises (PTE) with a combination of plyometric and a perturbation program. 3 The effect of low-intensity versus high-intensity PTE was compared in 1 study. 9 Finally, 1 study compared the effect of PTE under normal bodyweight with PTE augmented with bodyweight support. 17
Risk of Bias and Certainty in Studies
The majority of study outcomes (63.5%) were evaluated with some concerns, while the remaining outcomes had either a low (17.3%) or high (19.2%) risk of bias for overall assessment (Figure 2). Detailed risk of bias assessments is provided for all outcome measures (in Supplemental Material, available online). In total, 10 outcome measures from 5 studies 5,25,29,45,48 were judged to have high risks associated with deviations from the intended intervention domain. This was related to 5 different measurement domains as follows: patient-reported outcome measures in 1 study assessed high risk, 5 functional performance measures in 3 studies,5,25,29 strength outcome measures in 2 studies,29,48 knee laxity measurement in 2 studies,5,48 pain outcome measures in 1 study, 45 and proprioception outcome measures in 1 study. 29 The main reasons for judging “high risk” were that appropriate analysis was not performed (intention-to-treat),5,25,29,45,48 no detailed information was provided regarding blinding or randomization process,5,29,45,48 and pain measurements were different from those intended. 45
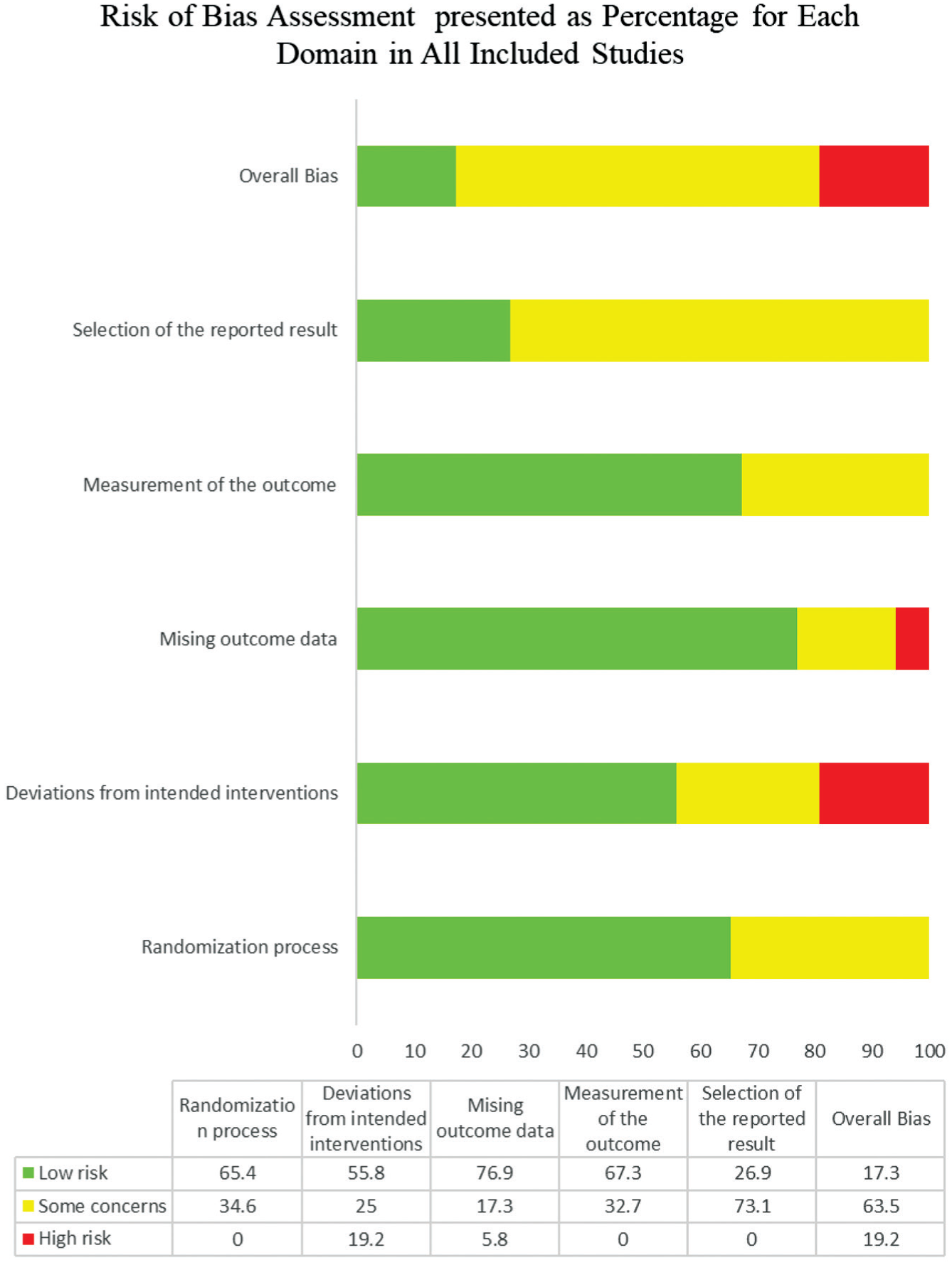
Risk of Bias Assessment Using the Cochrane RoB2 Tool. RoB2, risk of bias in randomized trials Version 2.0.
In addition, 3 outcome measures were deemed to have high risks associated with missing outcome data. There was 1 study with high risk that examined functional performance measures, strength outcomes, and proprioception outcomes. 29 This judgment was made due to missing outcome data, which was less than the accepted level of 95%, which could be the result of participants’ health conditions.
All certainty assessment results were detailed in the summary of findings tables (details in Supplemental Material, available online). The majority of study outcomes included in this systematic review showed very-low to low certainty results for the critical outcome. In contrast, the important outcome was very-low to moderate.
Specific Criteria to Start PTE
This report included 10 studies (63%) using specific criteria to determine when patients should begin plyometric exercises after an ACLR (Table 1),3,9,17,18,25,29,44,45,48,51 whereas in 6 studies (38%),5,10,16,26 -28 the plyometric exercise program was carried out based on a timeframe for the healing process. In 6 studies (60%) muscle strength measurements were used as a criterion for starting PTE.3,9,18,25,48,51 Table 1 illustrates the different types of specific criteria domains for starting PTE, as well as the number and percentage of studies and outcome measures for each criterion.
Specific criteria to start PTE after ACLR
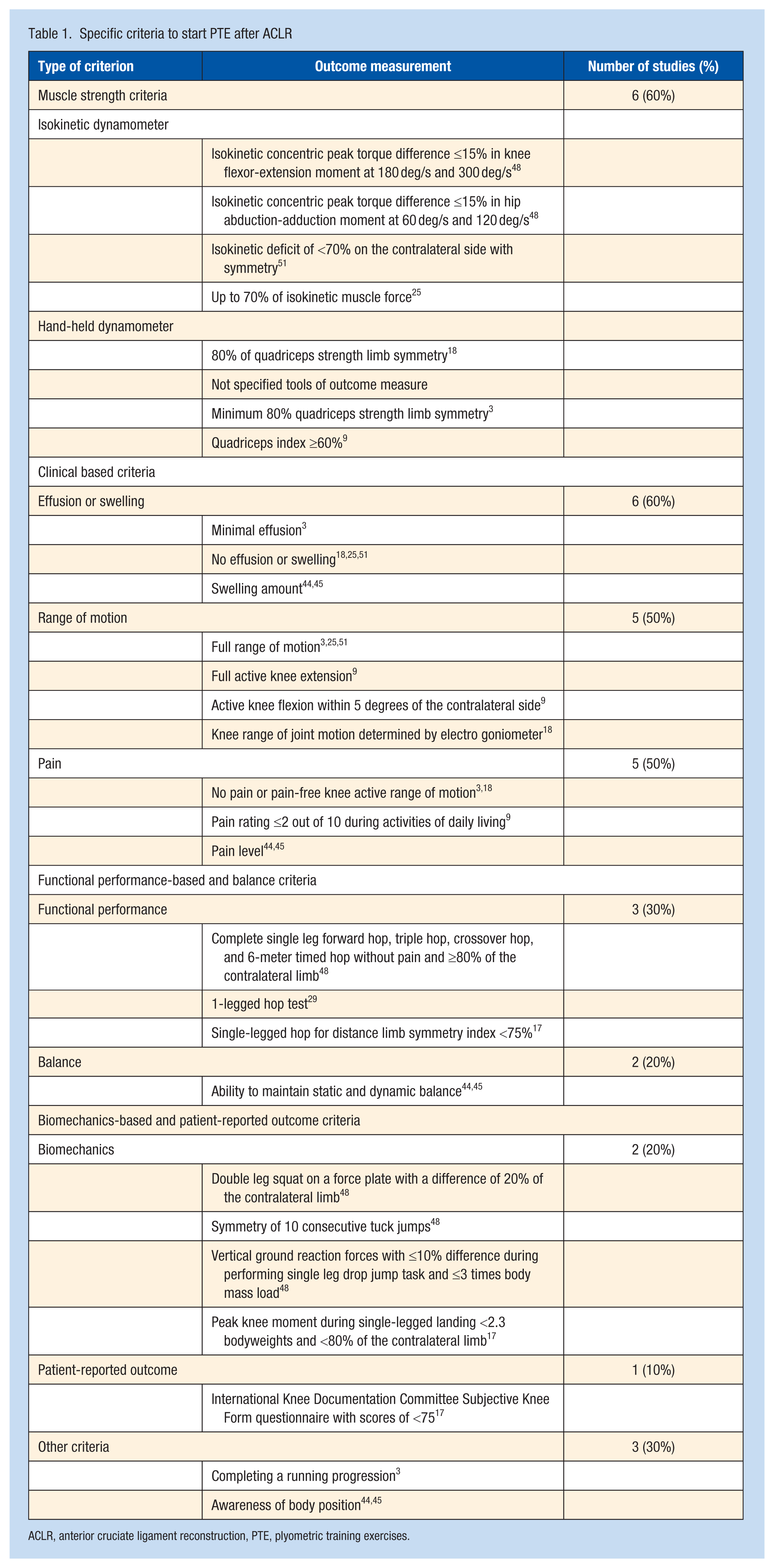
ACLR, anterior cruciate ligament reconstruction, PTE, plyometric training exercises.
Strength-Based Criteria
Strength was assessed by isokinetic dynamometry in 3 studies,25,48,51 hand-held dynamometry in 1 study, 18 and 2 other studies did not report using tools to collect the outcome data of the strength criteria.3,9 One study reported using isokinetic concentric peak torque difference ≤15% for knee flexor-extension moment at 180 deg/s and 300 deg/s and hip abduction-adduction moment at 60 deg/s and 120 deg/s. 48 One study reported using the isokinetic outcome measure with a criterion of a deficit <70% for symmetry with the contralateral side. 51 One study adopted an isokinetic outcome measure, using a threshold of ≤70% isokinetic muscle force. 25 One study reported using a hand-held dynamometer with a criterion of 80% quadriceps strength limb symmetry to clear patients for starting plyometrics training exercises. 18 Two studies reported using quadriceps strength limb symmetry index of 80% (determined by dividing the maximum torque of an involved limb by the maximum torque of an uninvolved limb × 100%) and ≥60% (the calculation by utilizing a normalized peak knee extensor torque [peak knee extensor torque/body mass in kg] and the quadriceps index (peak knee extensor torque on the surgical side/peak knee extensor torque on the nonsurgical side × 100)).3,9
Clinical-Based Criteria
Three studies reported using a criterion of no effusion or swelling to begin PTE.18,25,51 Arundale et al 3 reported minimal effusion as a criterion, and 2 studies reported using a swelling amount measure for starting PTE.44,45 A criterion of complete knee range of motion was used to initiate PTE in 3 studies.3,25,51 Chmielewski et al 9 reported full active knee extension and active knee flexion within 5 degrees of the nonsurgical side as a criterion to clear the patients. Ghaderi et al 18 reported only the knee range of joint motion via an electrogoniometer without a specific range limit. There were 2 studies that used the criterion of no pain or pain-free active range of motion in the knee to start plyometric training.3,18 In the study by Chmielewski et al, 9 a pain rating of ≤2 out of 10 during daily activities was used as a criterion. Two studies used pain level to indicate when to begin plyometric training without mentioning a specific level limit.44,45
Functional Performance-Based and Balance Criteria
Ghaderi et al 18 reported using a single-leg forward hop, triple hop, crossover hop, and 6-meter timed hop at an equivalent distance and/or rate of ≥80% of the contralateral side. Elias et al 17 also reported using a single-legged hop for a distance limb symmetry index <75% to indicate when to begin. Kaya et al 29 reported using a single-legged hop test to determine the functional level of patients without providing a specific capacity limit or cutoff as a criterion. In 2 studies,44,45 it was reported that a patient’s ability to keep a static and dynamic balance was used as a criterion to determine when it was time to begin plyometric training without providing a specific cutoff point.
Biomechanics-Based and Patient-Reported Outcome Criteria
Setuain et al 48 reported using multiple criteria to clear patients for training, including load distribution symmetry ≤20%, qualitative tuck jump symmetry, vertical ground reaction force difference ≤10% during a 50-cm single-leg drop jump while maintaining a load of ≤3 times body mass. Elias et al 17 reported using a peak knee moment while performing a single-legged landing with <2.3 bodyweights and <80% of the nonsurgical side. However, only 1 study reported using the International Knee Documentation Committee Subjective Knee Form questionnaire with scores of <75 as a criterion for introducing plyometrics training exercises. 17
Time to Start PTE
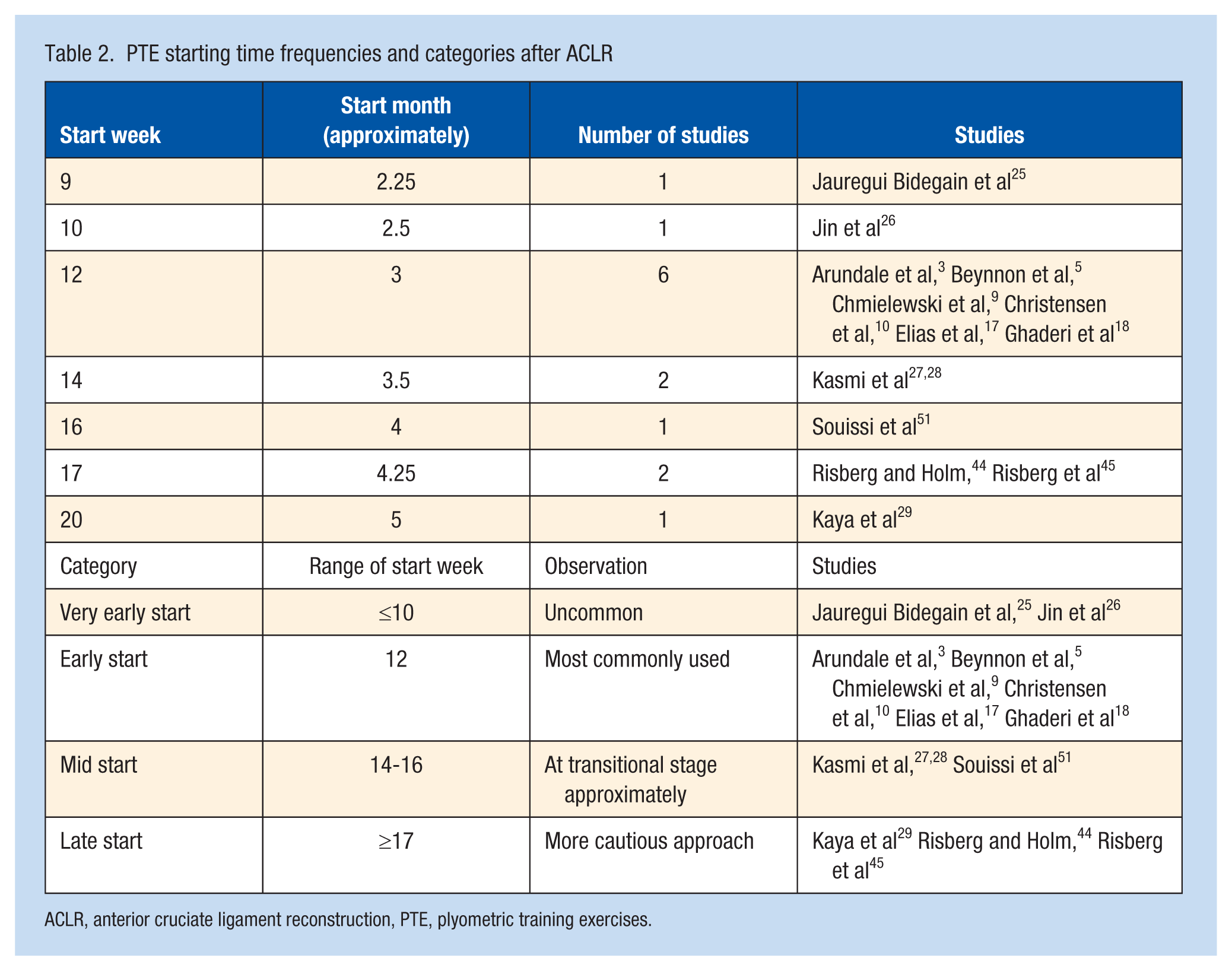
A total of 14 studies reported plyometric training starting times with a mean of 13.50 weeks and a standard deviation of 3.03 (mean ± SD = 3.38 ± 0.76 months) (Figure 3).3,5,9,10,16 -18,26 -29,44,45,51 In 2 studies,25,48 no information was reported about when to begin PTE. Table 2 demonstrates the frequencies and categorized distribution of weeks at which plyometric training was initiated after ACLR. However, in 8 studies that used specific criteria to clear patients, PTE were started after a mean of 14.75 weeks and a standard deviation of 3.15 (mean ± SD = 3.69 ± 0.79 months).3,9,17,18,29,44,45,51 In 6 studies that used a timeframe,5,10,16,26 -28 PTE were started after a mean of 11.83 weeks and a standard deviation of 2.04 (mean ± SD = 2.96 ± 0.51 months).
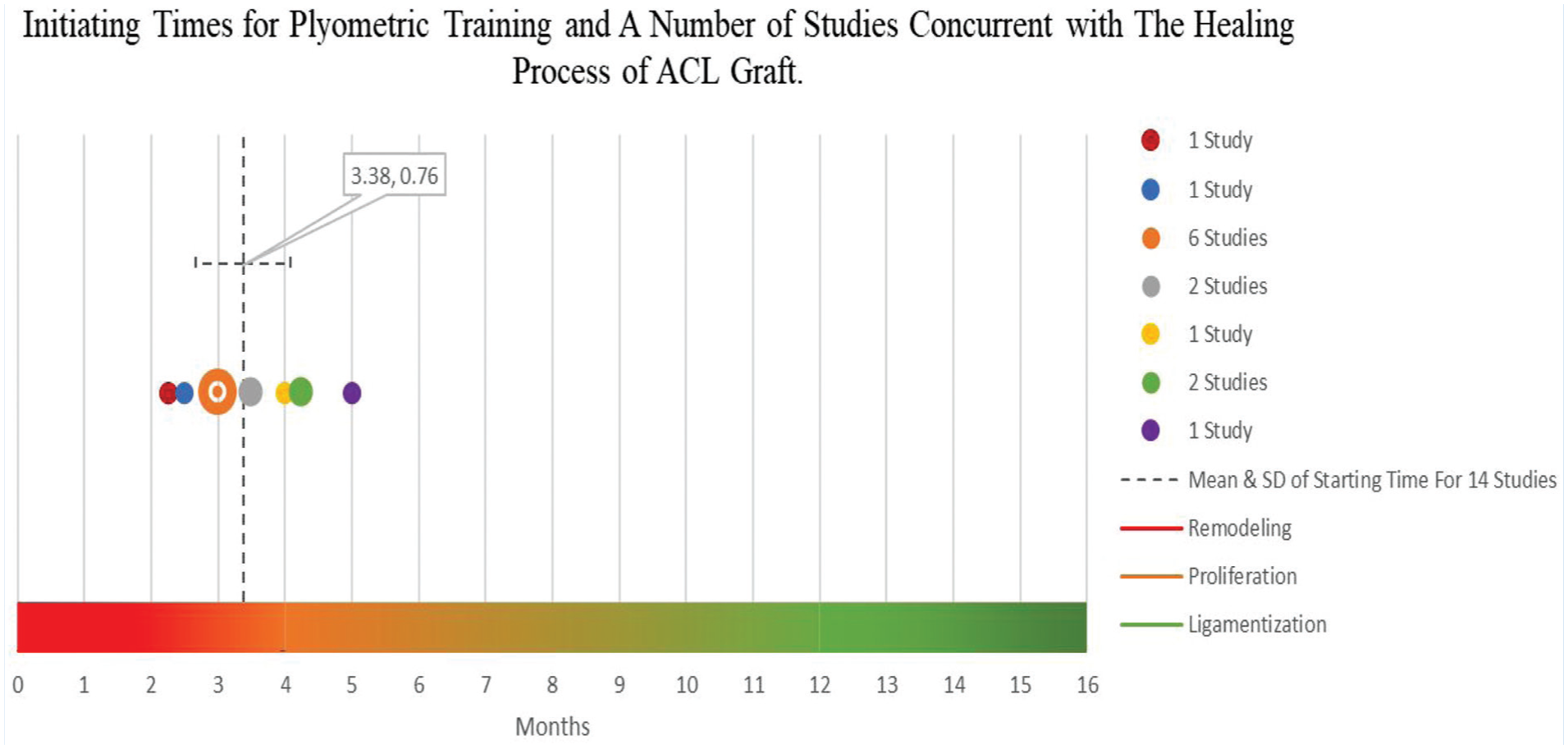
Illustration of starting time of PTE after ACLR. ACL, anterior cruciate ligament; ACLR, ACL reconstruction; PTE, plyometric training exercises.
PTE starting time frequencies and categories after ACLR
ACLR, anterior cruciate ligament reconstruction, PTE, plyometric training exercises.
Length of PTE Intervention
Training interventions varied between studies from 4 weeks to 12 weeks in terms of the duration of plyometrics training. One study implemented PTE for 4 weeks, 29 1 study for 5 weeks, 3 2 studies for 6 weeks,27,28 3 studies for 7 weeks,5,44,45 3 studies for 8 weeks,17,18,51 2 studies for 12 weeks,9,10 and 4 studies did not report the length of training.16,25,26,48 The most common duration range was 7 weeks to 8 weeks for the PTE after ACLR.
Adverse Events Associated With PTE Intervention
Only 2 studies reported that patients were not adversely affected by PTE when performed as part of their training program.3,28 The other studies did not provide information as to whether or not there were adverse events that occurred during the training period for the patients with ACLR.5,9,10,16 -18,25 -27,29,44,45,48,51
Statistical Syntheses Results
None of the included studies investigated the criteria for starting plyometrics training exercises and none provided data related to the included criteria. Therefore, conducting a meta-analysis to explore the efficacy of the criteria based on returning to plyometrics training exercises after ACLR was impossible. Thus, since there were not 10 trials to include in a funnel plot, publication bias was not assessed and sensitivity analysis was also not possible. The effectiveness of the plyometrics training exercise was not investigated because it was outside the scope of this systematic review.
Discussion
This systematic review was aimed at providing rehabilitation practitioners with evidence-based suggestions for criteria for returning to PTE. Of 16 studies, 10 (63%) used specific criteria to determine when patients should begin plyometric exercises after an ACLR procedure. The criteria used most frequently by studies to start PTE after ACLR were strength measurements (60%), effusion (60%), range of motion (50%), and pain level (50%). In addition, patients were permitted to perform PTE after ACLR based on assessing the functional performance, balance, biomechanics, patient-reported outcomes, and other undefined criteria (which included running progressions and awareness of body position). Across 14 studies, PTE began, on average, after 13.50 weeks (ranging from 9 weeks to 20 weeks); 7 weeks to 8 weeks was the most common reported duration for plyometric training. The majority of this systematic review’s findings were based on very low certainty of evidence, as judged by GRADE criteria, and almost all outcomes were subject to bias. There was considerable heterogeneity among the included studies concerning study criteria, type of graft, enrolment time, intervention duration, as well as measurement methods, and time intervals between outcomes. Furthermore, no data existed about the included criteria for starting PTE. Implementing meta-analyses in this study was therefore not possible.
The criteria-based assessment may not be used as the sole criterion for determining whether or not a patient can return to demanding activities after ACLR. 23 The systematic review demonstrated that 8 studies used specific criteria, while 6 used a timeframe to initiate PTE after ACLR, with respective means of 14.75 weeks and 11.83 weeks. In all studies that used the specific criteria or timeframe approaches, the biological healing process was appreciated as a basis for starting PTE. Despite the lack of a comprehensive understanding of the ligamentization process after ACLR, 11 human biopsy studies indicate that remodeling of the graft may continue even ≥1 year after ACLR. 53
Overall, patients may expect that it will take between 12 weeks and 16 weeks before they begin returning to more challenging activities, starting an advanced rehabilitation intervention that includes sports-specific skills after ACLR. 6 Among the included studies, the twelfth week (3 months) was the most common time to start PTE. In addition, this systematic review demonstrated that 13.50 weeks was the average starting time for PTE across 14 studies. Nevertheless, determining the optimal load that can be applied during the healing process, especially from the twelfth to thirteenth week of rehabilitation, remains challenging. 4
Lower limb strength must be sufficiently recovered to facilitate the transition to more challenging functional activities during the advanced stage of rehabilitation. In light of this, before starting plyometrics training, the systematic review suggested that the patient should first restore knee extension strength to within 60% to 85% of that of the contralateral limb. This threshold determination should be based on assessment tools (i.e., isokinetic or hand-held dynamometry) and take into account whether the limb symmetry index or normalized peak torque is used as the criterion. Thus, using a specific criterion that quantifies the capability of the lower limbs to produce and accept load with ground reaction forces of 2 to 6 times body mass,12,15 resulting from implementing PTE, would be essential. This may provide a better understanding of when patients with ACLR may be ready for these challenging exercises.
As a result of pain and swelling, arthrogenic muscle inhibition (AMI) may be present.21,40 The inability to recover knee extensor strength is believed to be attributed to AMI, which persists after injury or ACLR and continuously limits the improvement of knee extensor muscle volume and strength. 41 There is a tendency for AMI to limit the ability of patients to achieve the required neuromuscular activation and necessarily intensity levels for facilitating response to strength training. 49 According to the studies we review and present for discussion, patients should also meet specific clinical criteria before beginning PTE after ACLR. These clinical criteria include no effusion or swelling, full range of motion of the knee (e.g., full active knee extension and active knee flexion within 5 degrees of the nonsurgical side), and no pain or no more than 2 out of 10 pain rating score during daily activities.
Many factors influence knee movement, including biomechanical factors, which may impact the quality of movement. 14 A person is more likely to sustain an injury when landing with knee valgus since increased ground reaction forces are experienced. 22 In varied combinations of tibial movement, the ACL was strained 4.6 times more than normal during landing when abduction and anterior tibial translation were combined. 42 However, the systematic review showed that using a double leg squat with 90º knee flexion on a force plate with symmetry of ≤20% difference of the contralateral, as well as vertical ground reaction forces difference of ≤10% while performing a 50-cm single leg drop jump task and ≤3 times body mass load to assess the movement quality to allow patients to start the training. Furthermore, visual and audible qualitative analysis symmetry could be assessed while performing 10 consecutive tuck jumps as a criterion to initiate the advanced rehabilitation.
Different aspects should be considered when deciding whether to return to high-demanding activities after ACLR. For example, functional skills, movement quality, balance, and psychological state should be assessed to determine whether a patient is prepared to confront the forces in a way that minimizes reinjury risk. 33 Functional tests, such as a hop or jump test, are used commonly to measure knee stability and lower extremity strength during explosive movements. 1 Practitioners could consider a wide range of performance-based criteria, including functional tests (single-leg forward hop, triple hop, crossover hop, and 6-meter timed hop) at an equivalent distance and/or rate of ≥80% of the contralateral side and the ability to maintain static and dynamic balance, as a criteria to determine readiness for initiating plyometric training. In addition, the International Knee Documentation Committee Subjective Knee Form with scores of 75 could be used as a criterion for introducing plyometrics training exercises.
Among 16 studies, 14 did not provide information on whether plyometric training adversely affected participants. Only 2 studies reported explicitly that plyometric training did not cause adverse effects, which may not provide enough evidence to conclude that such exercises are safe to implement. This advanced rehabilitation for returning to sports activity may not be safe for patients who do not achieve a certain level of adequate knee functional performance and strength. 32 Therefore, the transition to advanced rehabilitation should be based on objective measures that specify the knee functional demand and neuromuscular control to improve successful return to PTE and satisfactory long-term results. 46
Clinical Implications
Advanced rehabilitation exercises involving plyometrics exercise improved knee function and impairments as well as boosted psychological wellbeing. The time to start plyometrics exercise has no consensus timeframe. Studies reviewed demonstrate that patients with ACLR have been initiated on a plyometric training program at an average of 13+ weeks. A criteria-based assessment with a concomitant timeframe after ACLR might be a reasonable approach for practitioners. The criteria as a precursor to initiate PTE include no effusion, full active knee extension with active knee flexion within 5 degrees of the nonsurgical side, no pain or ≤2 out of 10 pain rating during daily activities, and the International Knee Documentation Committee Subjective Knee Form questionnaire with scores of 75 can be a prerequisite for introducing plyometric training. Before starting plyometrics training exercises, a battery of tests may also be considered, such as strength-based criteria, performance-based criteria (functional and balance), and biomechanics-based criteria.
Nevertheless, each patient with ACLR should be assessed individually before returning to plyometric exercise for safety purposes. Some measurements may be more pertinent for certain patients with ACLR, depending on their sport performance profile. Researchers and practitioners should consider the patient’s individual sport when designing research and treatment plans.
Study Limitations and Future Research
This systematic review study has limitations that need to be acknowledged. Only randomized control trials were included; other study designs were not included, which may provide different valuable information. The study design restrictions were implemented to minimize bias and promote evidence certainty. Different types of grafts that have been used for the ACLR in the included studies may influence the time to start PTE. The presence of concurrent injuries, such as meniscal injuries with ACL injury, is likely to have additional healing concerns that could prolong the return to PTE. 20 In the case of revision ACLR, more substantial chondral damage can adversely affect functional outcomes and activity levels. 55
Consequently, the time of returning to PTE may need to be changed based on the healing process requirement. A patient’s psychological condition can influence their ability to return to sport after ACLR, 37 but no study included here used psychological outcome measures as a criterion to initiate plyometric training. However, the systematic review search for relevant literature was completed on March 13, 2026, which may not reflect newly developed studies thereafter. More research is required to validate the proposed assessment criteria for starting plyometric training safely with an appropriate equilibrium between loading and graft healing after ACLR. It is also important to investigate whether psychological status affects the readiness of patients to handle the load associated with advanced rehabilitation. In addition, future research may consider different study designs to extend insight regarding the time of starting plyometric, parameter (load, specificity, and frequency), and safety to optimize the related load of exercise post-ACLR.
Conclusion
Patients with ACLR in the studies reviewed initiated PTE based on assessing the pain level, range of motion, functional performance, balance, biomechanics, and patient-reported outcomes. PTE began on average after 13.50 weeks, ranging from 9 weeks to 20 weeks, and were implemented in advanced rehabilitation with a common duration range of 7 weeks to 8 weeks post-ACLR. The systematic review findings were based on a low level of certainty of evidence, and almost all of the study outcomes demonstrated some concern of bias. A conclusion that such exercises are safe cannot be drawn from the available evidence. It is still necessary to conduct more research to validate the proposed assessment criteria for starting plyometric exercise safely.
Supplemental Material
sj-docx-1-sph-10.1177_19417381261457612 – Supplemental material for When to Start Plyometric Training After Anterior Cruciate Ligament Reconstruction? A Systematic Review of Randomized Clinical Trials
Supplemental material, sj-docx-1-sph-10.1177_19417381261457612 for When to Start Plyometric Training After Anterior Cruciate Ligament Reconstruction? A Systematic Review of Randomized Clinical Trials by Majed Alabbad, Shibili Nuhmani and Qassim Muaidi in Sports Health
Footnotes
The authors report no potential conflicts of interest in the development and publication of this article.
Ethics Statement
Ethical approval was not sought for the present study.
Consent to Participate
Not applicable for this systematic review.
Consent for Publication
Not applicable for this systematic review.
Data Availability Statement
The authors have included all data generated or analyzed throughout this study in this article and its supplementary information files.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.