
Abstract
Approximately 200 000 patients per year will require mechanical ventilation secondary to neurological injury or disease. The associated mortality, morbidity, and costs are significant. The neurological patient presents a unique set of challenges to airway management, mechanical ventilation, and defining extubation readiness. Neurological injury and disease can directly or indirectly involve the process involved with respiration or airway control. This article will review the basics of airway management and mechanical ventilation in the neurological patient. The current state of the literature evaluating extubation criteria in the neurological patient will also be reviewed.
Introduction
It has been estimated that about 200 000 patients per year will require mechanical ventilation secondary to neurological injury. The mortality for this population varies with the particular illness but ranges between 20% and 50%. The associated cost of caring for these patients is significant and has been estimated to be greater than $25 billion annually. Thus, decreasing time on the ventilator for these patients will have significant medical and economic implications. 1 , 2
Airway and pulmonary management of the patient with neurological disease contains an array of challenges, whose composition varies with the pathology at hand. The managing physician should be familiar with the patient's neurological and cerebrovascular pathophysiology and the implications for management of their airway and respiratory status.
Extubation of the neurological patient also demands particular consideration of airway patency as well as respiratory mechanics. This article will examine factors specific to the neurological patient relevant to initiation and removal of mechanical ventilation with reference to the current literature.
Neurological Implications of Ventilatory Impairment
Increases in P
Airway Management
Assessment of the airway is the starting point of most algorithms involved in the airway management including patients with neurologic disease. This assessment includes an examination of the oropharynx, teeth, and tongue. Trauma is often self-evident, with immediate tissue injury and hemorrhage as well as delayed swelling of tongue, lips, and pharyngeal soft tissue.
Patency of the airway is also dependent on the neuromuscular tone. This will be adversely affected with significant obtundation. Under these circumstances the effect of gravity on the tongue in the supine position will produce posterior occlusion of the pharynx, augmented by the negative pressure of inspiration and its effect on a hypotonic pharyngeal wall. This combination can produce effects ranging from sonorous breathing to complete occlusion. Nasal flaring, tracheal “tug,” and intercostal indrawing are all objective signs of increased effort and threatened obstruction.
Interventions in these patients include a simple jaw thrust (lifting the mandible upward, thereby pulling the base of the tongue away from the posterior pharynx), placement of an oro- or nasopharyngeal or supraglottic airway, endotracheal intubation, or tracheostomy.
Jaw lift often occurs just with the placement of a well-fitting cervical collar but is often of only transient benefit. Nonetheless, it may buy time for the relief of other contributing factors (oversedation, agitation, etc). Pharyngeal airways are often successful in relieving snoring and other partial obstructions. Their risks include trauma to teeth, gums, nasal turbinates, tongue, and palate as well as the sinusitis associated with prolonged nasal use. Supraglottic airways can also be viewed as an extension of the pharyngeal airway, with some ability to ventilate, but in essence both these and the pharyngeal airways are inferior to the tracheal cannulation in overall effectiveness of the ventilation and carry a higher risk of aspiration. Endotracheal intubation and tracheostomy are equally effective in the maintenance of the airways and there are no significant differences in the outcome, although there is management benefits associated with tracheostomy.3,4
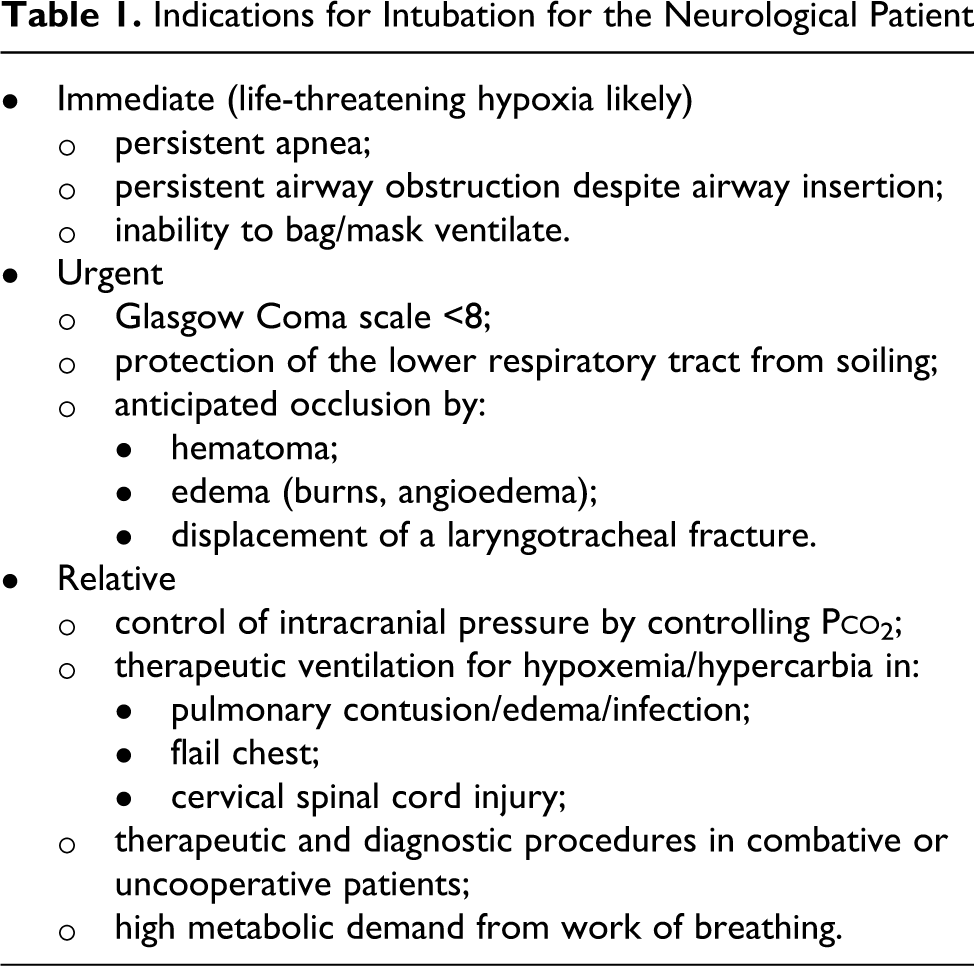
Indications for intubation for the neurological patient are listed in Table 1, chief among which is coma. The national trauma data bank reported an increase in aspiration pneumonia and worse outcomes in patients who were not immediately intubated. 5 Similarly, the concept of early intubation is well supported in the subsequent studies.6,7
Indications for Intubation for the Neurological Patient
There is a risk of cervical spine injury during instrumentation of the airway in patients with trauma. Therefore, it is necessary to take appropriate precautions to avoid neck movement and consequent cord damage. Over 14% of all the major trauma cases have a potentially unstable spine. Up to 5% of the patients with moderate or severe head injury have an unstable cervical spine and half of those have sustained actual cord injury. 7
Direct laryngoscopy has advantages of familiarity and speed and also has several disadvantages. Direct laryngoscopy requires an additional operator to provide in-line manual stabilization (ILMS) which together with the placement of a cervical collar may impair the available view and reduce the chances of successful endotracheal cannulation. Even with ILMS, significant cervical spine movement can occur.
Videolaryngoscopy reduces but does not remove cervical spine movement. It requires the use of and familiarity with specialized equipment. Although a good view of the glottis can be rendered, the tracheal tube cannot always be guided through the cords, and this can delay intubation unless a tube guide is incorporated. 8 Nevertheless, these devices are now relatively affordable and commonplace in most hospitals and emergency medical services facilities.
Fiberoptic intubation is the most reliable method of avoiding further distraction injury to the cord but requires significantly more investment in both training and equipment. Fiberoptic airway evaluation may be limited under circumstances of aspiration, swelling, or hemorrhage of the airway. 8
Careful attention should be given to identifiable predictors of difficult mask ventilation as well as those associated with difficulty in intubation. Simple consideration of the acronym OBESE (explained as O = Obese with body mass index > 26 kg/m2; B = Bearded; E = Elderly—older than 55 years; S = Snorer; and E = Edentulous) can alert the user to the possibility of difficult mask ventilation. This acronym has a sensitivity of 72% and specificity of 73%. 9
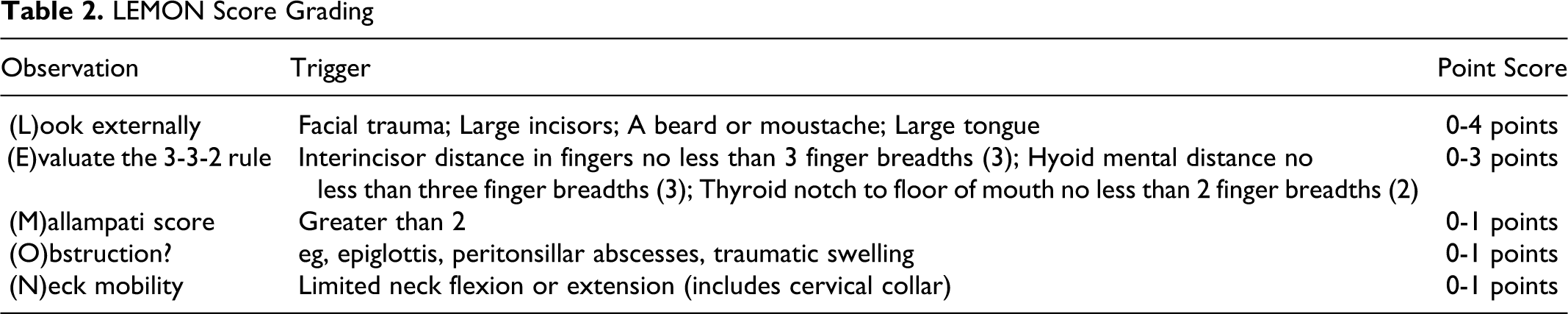
Similarly, the LEMON score (Table 2) has been developed to aid objective assessment of the possible difficult intubation. Although it does use the established Mallampati score, this is often not useable in emergent circumstances and a modified version has been proposed that drops the Mallampati element. 10 Awake intubation (whether endotracheal or via tracheotomy) is rarely employed within the intensive care unit (ICU), requires specialist expertise, and is outside the scope of this review.
LEMON Score Grading
Concerns for intracranial hypertension will affect both the method and the medications used during the endotracheal intubation. Agents commonly employed are listed in Table 3.
Commonly Used Induction Agents With Typical Doses
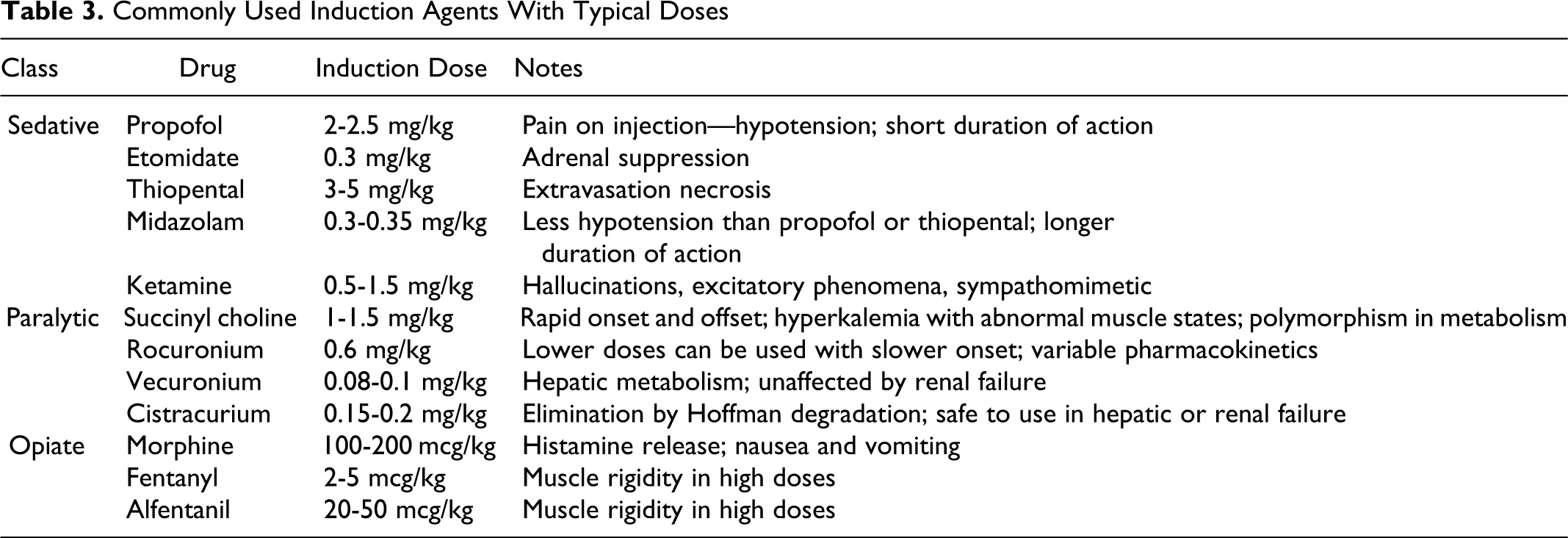
Medications used for endotracheal intubation include sedative agents, opiates, and paralytics. However, these agents can obstruct the close neurological monitoring often required in these cases. A balanced approach uses all 3 classes, with variation in the contributing ratios to meet individual patient needs and optimize neurological assessments. This approach also serves to minimize individual side effects, with opiates and paralytics both reducing the amounts of sedation required for procedural control. Care should be taken with the reduction of cardiac output seen with the removal of sympathetic activity in virtually all sedative drugs. Ketamine and etomidate have the least cardiovascular depressive effects, but ketamine’s sympathomimetic action has been associated with increases in ICP. The significance of these findings however has been questioned. 11 Opiates may contribute to hypotension on induction but serve to reduce hypertension associated with laryngoscopy, and any cough reflexes persisting beyond induced paralysis. Paralytics do not inhibit the hypertensive response but are valuable in facilitating instrumentation and intubation. Succinylcholine is frequently cited as being contraindicated in the neurological patient to avoid intracranial hypertension. Good quality evidence for this is wanting, and the benefits afforded by its rapid effect and swift control of the airway vastly outweigh any transient clinically insignificant effects on ICP. Its use can be associated with hyperkalemia in the immobilized patient, but this is rarely pertinent in the first 72 hours of hospital admission, except in the cases of existing burns, muscle disease, or paralysis. It is generally avoided in ICU patients who have been immobilized for more than 48 hours.
Once the neurological patient has been successfully intubated, they should be transported to an ICU (preferably a neuro-ICU).
Ventilatory Management of the Neurological Patient
After control has been gained of the airway, the neurological patient also has specific requirements of mechanical ventilation. The importance of hypoxia and hypercarbia has been previously outlined. However, the associated hypocarbia secondary to hyperventilation may also adversely initiate decreases in the CBF.
There are some positioning challenges especially in patients with unstable spines (who may need to be nursed flat in traction) but as a rule the head of the bed should be raised to at least 30° as soon as possible to minimize the risk of ventilator-associated pneumonia. Meticulous mouth care needs to be undertaken.
There is no data to support one mode of ventilation over another, provided there is adherence to reasonable targets of oxygenation and CO2 clearance. On the other hand, the need for actual ventilation may vary with pathology since many patients with stroke or traumatic brain injury may be able to regulate their own breathing once an airway has been provided. In this condition, pressure support modes may facilitate this approach.
Ventilatory requirements can be gauged by arterial blood gases and the chest x-ray. The P
Noninvasive positive pressure applied via a close fitting facemask can be used to maintain airway patency as in continuous positive airway pressure for sleep apnea, whereas the application of a time-cycled positive pressure can actually ventilate the patient (noninvasive positive pressure ventilation) and may gain time to permit another acute intervention to have effect (eg, reversal of narcotization). However, it has not been shown to alter the need for longer term ventilation in the respiratory failure. It does not protect against aspiration and presents challenges in feeding. In circumstances of decompressive craniectomy, a prohibition on the elastic head straps precludes its use altogether. Cervical spine injury may have varying effects on the phrenic nerve function (C3, C4, and C5). Injuries above C3 will lead to complete denervation of the diaphragm as well as the chest and abdominal wall musculature. These patients can only utilize their accessory muscles for respiration and need emergent intubation. As the level of injury descends below C3, phrenic nerve function will be retained to a greater degree with proportional preservation of diaphragmatic activity. However, any injury above the first thoracic vertebral segment will induce a loss of intercostal and abdominal wall muscle function. The consequent respiratory pattern sees the abdomen protrude with diaphragmatic contraction during inspiration. However, without intercostal and abdominal muscles, the chest wall will involute during inspiration, resulting in minimal air movement. Such patients are best managed lying supine. In this position, the abdominal contents can push up the diaphragm placing it in a mechanically advantaged position for contraction, with an increase in tidal volume. A pragmatic clinical alternative is the use of an abdominal binder, which replaces the muscle tone of the abdominal wall, forcing the viscera inward and the diaphragm upward, even in upright and semirecumbent positions.
Many patients with lower cervical neck injuries will need to be intubated in the acute phase of injury, when cord edema is at its worst. Either resolution of that swelling or surgical decompression of the cord, most will be successfully extubated. Air movement improves as the chest wall develops spasticity and chest level involution decreases with inspiration. 13 This may facilitate later extubation.
Neuromuscular diseases (primarily myasthenia gravis and Guillain-Barré– syndrome) also present with a specific set of challenges. The need for intubation should be based on the pulmonary function tests and not the typical criteria used to access the medically ill patient. The progression of weakness starts with a subtle decrease in oxygenation and in some cases a subtle increase in respiratory rate. Hypercapnea may be initially compensated but is a late sign for the deteriorating patient. Many patients with ascending paralysis cannot increase their respiratory rate or use their accessory muscles. These patients can look deceivingly well until complete respiratory collapse. In general, a vital capacity of <10 to 15 cc/kg or a negative inspiratory force of <20 should prompt elective intubation. 14 As mentioned previously, noninvasive ventilation may permit pharmacologic intervention in myasthenic patients and avoid intubation in some cases but has largely proved useless in patients with Guillian-Barré syndrome with longer term needs.15,16
There is a controversy on the need for sedation to facilitate mechanical ventilation for all ICU patients and may have significant implications for the neurological patient, where frequent neurological assessments are necessary.
There are also increasing concerns on the effect of delirium on outcome and the contribution of sedative drugs to that delirium. There are suggestions that dexmedetomidine—an α-2 agonist—may be superior in this regard. 17
Some sedation choices are listed in Table 4. A recent review of the brain injury could find no evidence of any benefit of one sedative agent over another. 18
Sedative Agents Cerebral Hemodynamic and Adverse Effects
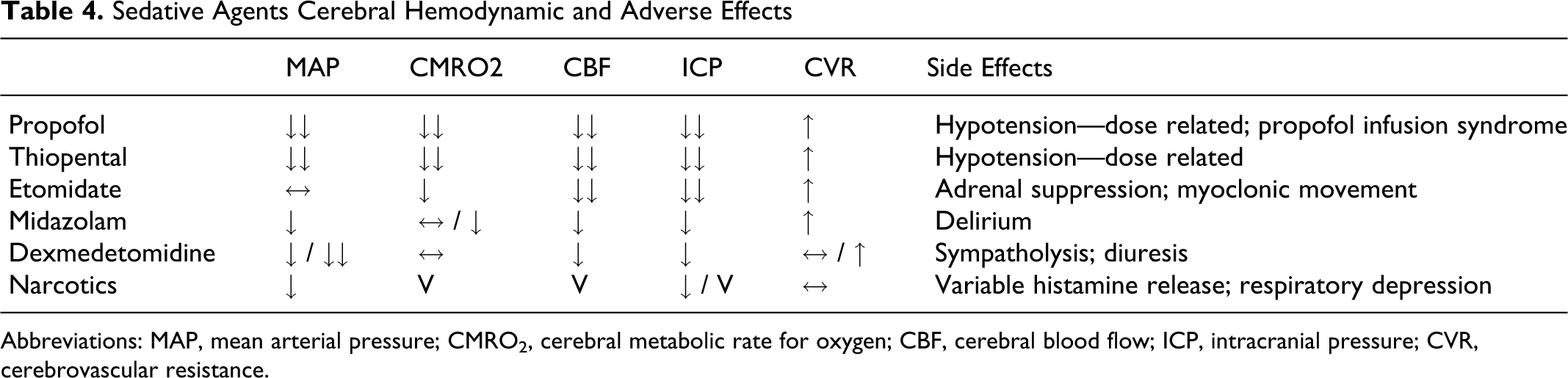
Abbreviations: MAP, mean arterial pressure; CMRO2, cerebral metabolic rate for oxygen; CBF, cerebral blood flow; ICP, intracranial pressure; CVR, cerebrovascular resistance.
There is no sedation assessment tool that has been credibly validated in neurological injury. This includes the Ramsay score, Richmond Agitation Sedation scale (RASS), and the Sedation-Agitation scale (SAS) as well as devices such as the Bispectral Index (BIS) and entropy monitoring. The BIS monitor has been proposed in this role but was developed for general anesthesia, calibrated in circumstances of muscle relaxation, and cannot be recommended for routine use in the ICU. 19 The distinction between coma and sedation confounds assessment in clinical scales, while monitoring devices possess significant interindividual variability even before considering the effect of brain injury. 20 What is certain is that a daily program of automatic interruption and reinstitution at a lower level is superior to physician judgment in dosing and thereby facilitates shorter durations of ventilation and ICU stay. 21 Neuromuscular patients will be successfully weaned from mechanical ventilation when their primary disease process has improved. In the case of myasthenia gravis, the offending antibodies must be removed and regeneration of the acetylcholine receptors must occur. A similar process must also occur in Guillian-Barré syndrome. Attempting to wean the patient from the mechanical ventilation prior to the disease running its course will be unsuccessful.
Extubation Criteria for the Neurological/Neurosurgical Patient
Developing specific extubation criteria for the neurological patient has proved to be somewhat problematic. Successful extubation requires both resolution of underlying pulmonary processes and the ability to maintain airway patency. Many studies have examined the criteria required for extubation success in the nonneurological patient. Most have focused on the patients’ respiratory muscle strength and their ability to maintain oxygenation with decreasing ventilatory support. Spontaneous breathing trials (SBTs) from 30 minutes to 2 hours have been proposed to assess both of these functions,22–24 with no increase in the accuracy beyond the shorter period. The rapid shallow breathing index (RSBI) has a low accuracy but is more useful when used in an algorithm that looks at changes in the RSBI over the course of an SBT. 25 Minute volume recovery time after these trials has most recently been proposed as a simplified method to predict extubation success. 26 Specific guidelines have been developed for weaning and discontinuation of ventilatory support. 27
The neurological patient is likely to have a higher incidence of problems with airway patency. Cervical neck surgery is often performed in the prone position and its combination with large amounts of fluids produces significant facial and laryngeal edema. Stridor and reintubations are common post extubation and in many circumstances occur in patients with difficult airways. Requiring a cuff leak prior to extubation is controversial. The most recent meta-analysis did not demonstrate any advantage in its use. One approach is to consider a trial of extubation with the ICU team in readiness to replace the tube should 28 it be required.
The use of corticosteroids to reduce laryngeal edema has recently come into favor. Older studies showing no benefit to steroid use in reducing postextubation stridor involved only single doses. Newer studies employing several doses initiated prior to extubation have reported improvements in postextubation stridor. Current data suggest that methylprednisolone (20-40 mg every 4-6 hours) should be considered 12 to 24 hours before a planned extubation in a patient at high risk for postextubation stridor. 29
Neurological/neurosurgical patients with lesions involving the posterior fossa may have similar issues in maintaining airway patency. Lesions in this area may have a direct impact on the ability to maintain or support the airway reflexes and musculature. Prediction of which patients can specifically maintain airway patency is difficult and poorly studied.
Another issue that is oftentimes encountered is whether nonawake patients can be extubated. Traditionally, patients with a Glasgow Coma scale (GCS) ≤ 8 have remained intubated based on the assumption that patients in coma are unable to maintain airway patency.
Support for this assumption was provided by Namen et al who reported in a multivariate analysis that a GCS ≥ 8 was associated with an extubation success rate of 75% versus a 33% success rate for a GCS < 8. They reported that the odds of successful extubation increased by 39% for each incremental improvement in the GCS. 30
Coplin et al however reported that patients that had extubation delayed based on a GCS ≤ 8 had a greater number of ventilator-associated pneumonias, higher costs, and worse outcomes compared to a group that was immediately extubated. This study incorporated an airway care score evaluating the patients’ ability to detect and control secretions. The most consistent airway parameters associated with extubation success were the presence of a spontaneous cough and a required suctioning frequency of >2 hours. 31 Other authors have reported similar results with the presence of a strong cough and minimal secretions. 32
Manno et al performed a pilot trial randomizing patients that met a set of extubation criteria to either immediate extubation or delayed extubation (until their GCS improved to >8). From their results, they were able to generate a power analysis suggesting that approximately 100 patients would be needed in each group for a noninferiority trial. Subgroup analysis could be performed to evaluate superiority in a number of secondary measures including reintubation rates and ventilator-associated pneumonia. 33
There is little data on when patients with neuromuscular disease can be safely extubated. One study evaluating the predictors of extubation failure included prolonged intubation, atelectasis, lower pH, and forced vital capacities but were generally nonspecific. 34 For extubation it seems reasonable to incorporate the same pulmonary function tests used for intubation. Physical examination of the proximal muscle strength and treatment of secondary infections should also enter into the consideration for extubation. Extubation to noninvasive ventilation in the neuromuscular patient has not proven helpful. 35
Tracheostomy does offer advantages in removing the association of extubation and ventilation. Trials of ventilatory function can be accomplished simply by a change in the mode without concern for the later airway obstruction. The advantages of rapid effective airway suctioning without return to the ventilator cannot be overlooked. There are benefits in the duration of ventilation and ICU stay with decreased sedation and antibiotic use. There is however no evidence of longer term outcome differences, including mortality.
Conclusions
The neurological/neurosurgical population presents with a unique set of circumstances and problems for airway management, mechanical ventilation, and establishing extubation criteria. Primary neurological injury or disease can directly affect the ability to initiate respiration or control airway secretions or musculature. Neuromuscular disease can affect the respiratory muscle strength.
Typical methods to assess extubation success may not be applicable to patients with neurological disease. Establishing which parameters can safely predict extubation success needs to be a focus of future research.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.