
Abstract
Case Presentation
A 61-year-old woman with a history of migraine headaches and focal segmental glomerulosclerosis, chronically immunosuppressed with mycophenolate mofetil, presented to a hospital with 2 weeks of left-sided headache and word finding difficulty. She described her headaches as constant pain similar in location and character to her typical migraines and involving her left face. The day prior to presentation, she developed slowed speech, stuttering, and confusion.
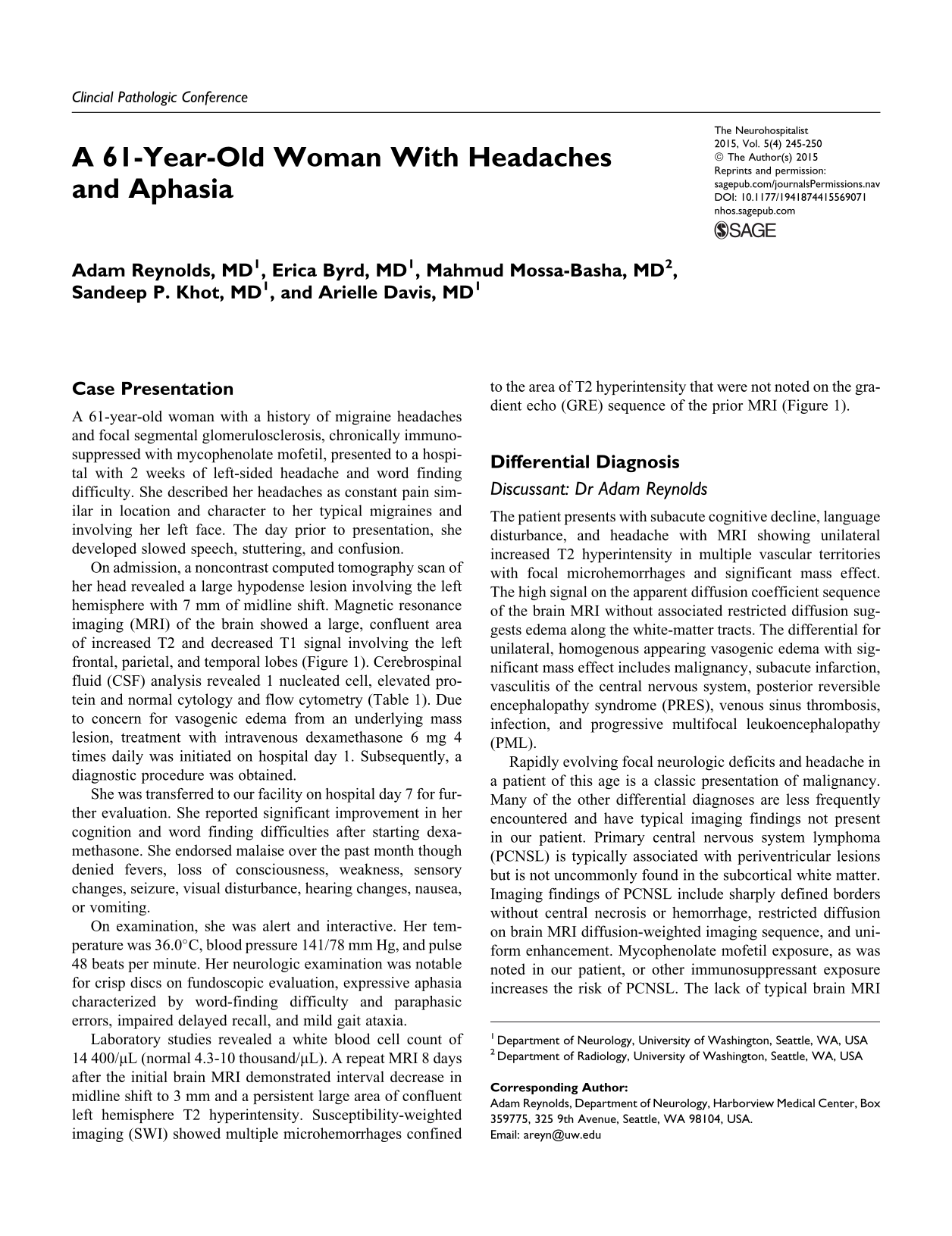
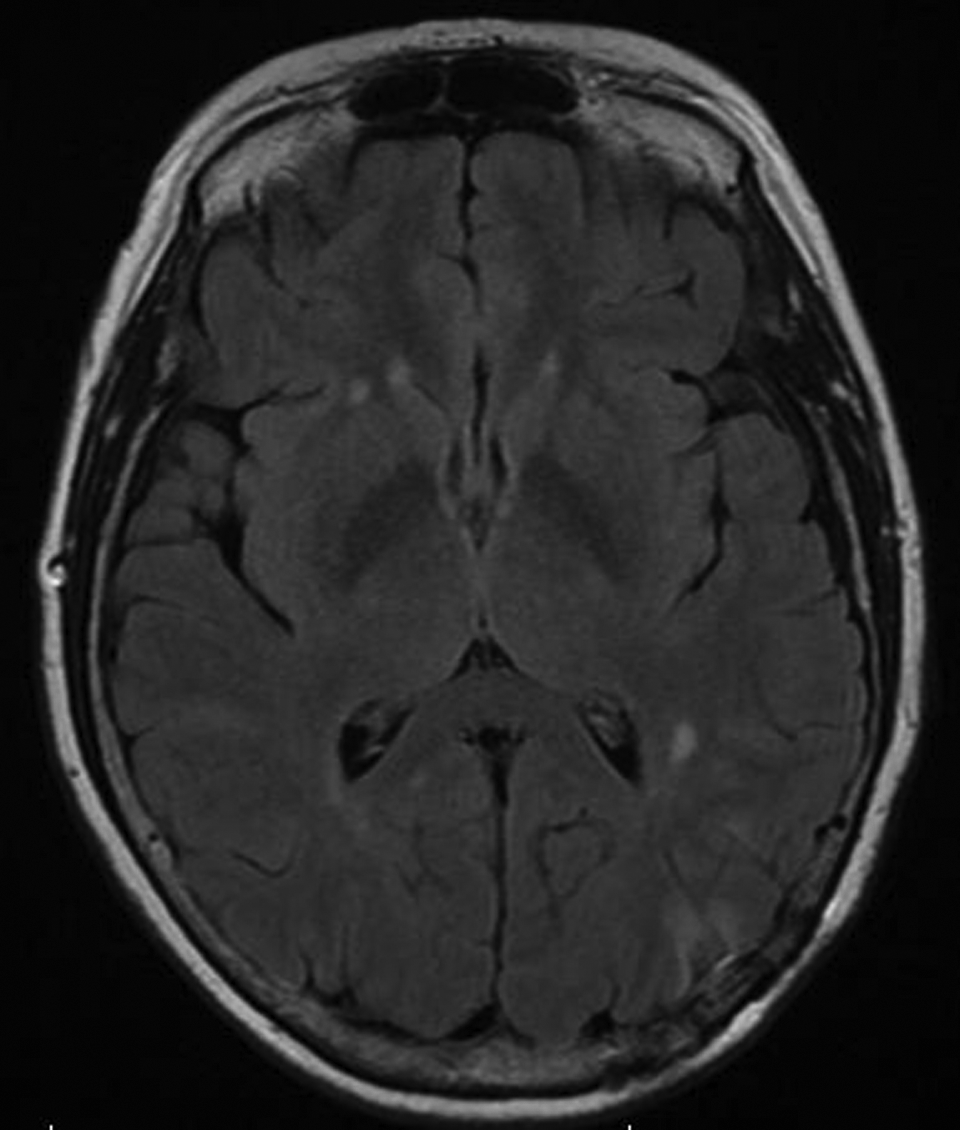
On admission, a noncontrast computed tomography scan of her head revealed a large hypodense lesion involving the left hemisphere with 7 mm of midline shift. Magnetic resonance imaging (MRI) of the brain showed a large, confluent area of increased T2 and decreased T1 signal involving the left frontal, parietal, and temporal lobes (Figure 1). Cerebrospinal fluid (CSF) analysis revealed 1 nucleated cell, elevated protein and normal cytology and flow cytometry (Table 1). Due to concern for vasogenic edema from an underlying mass lesion, treatment with intravenous dexamethasone 6 mg 4 times daily was initiated on hospital day 1. Subsequently, a diagnostic procedure was obtained.
Brain magnetic resonance imaging (MRI) scans. A, Admission brain MRI, fluid-attenuated inversion recovery (FLAIR) sequence demonstrating a large confluent area of hyperintensity involving the frontal, parietal, and temporal lobes. B, Admission gradient echo with no microhemorrhage seen. C, Susceptibility-weighted imaging with arrows indicating microhemorrhages within the area of FLAIR hyperintensity.
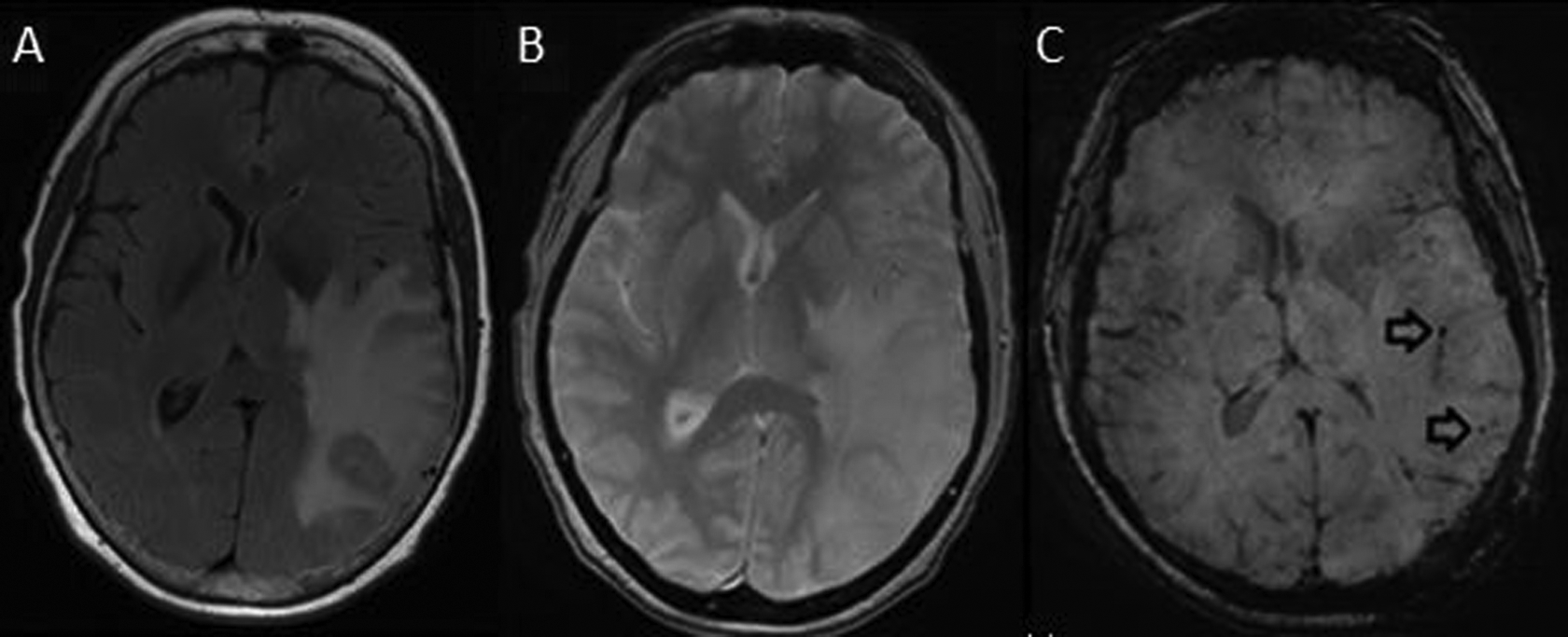
Cerebrospinal Fluid Characteristics of the Patient Compared With Selected Diseases on the Differential Diagnosis.
She was transferred to our facility on hospital day 7 for further evaluation. She reported significant improvement in her cognition and word finding difficulties after starting dexamethasone. She endorsed malaise over the past month though denied fevers, loss of consciousness, weakness, sensory changes, seizure, visual disturbance, hearing changes, nausea, or vomiting.
On examination, she was alert and interactive. Her temperature was 36.0°C, blood pressure 141/78 mm Hg, and pulse 48 beats per minute. Her neurologic examination was notable for crisp discs on fundoscopic evaluation, expressive aphasia characterized by word-finding difficulty and paraphasic errors, impaired delayed recall, and mild gait ataxia.
Laboratory studies revealed a white blood cell count of 14 400/µL (normal 4.3-10 thousand/µL). A repeat MRI 8 days after the initial brain MRI demonstrated interval decrease in midline shift to 3 mm and a persistent large area of confluent left hemisphere T2 hyperintensity. Susceptibility-weighted imaging (SWI) showed multiple microhemorrhages confined to the area of T2 hyperintensity that were not noted on the gradient echo (GRE) sequence of the prior MRI (Figure 1).
Differential Diagnosis
Discussant: Dr Adam Reynolds
The patient presents with subacute cognitive decline, language disturbance, and headache with MRI showing unilateral increased T2 hyperintensity in multiple vascular territories with focal microhemorrhages and significant mass effect. The high signal on the apparent diffusion coefficient sequence of the brain MRI without associated restricted diffusion suggests edema along the white-matter tracts. The differential for unilateral, homogenous appearing vasogenic edema with significant mass effect includes malignancy, subacute infarction, vasculitis of the central nervous system, posterior reversible encephalopathy syndrome (PRES), venous sinus thrombosis, infection, and progressive multifocal leukoencephalopathy (PML).
Rapidly evolving focal neurologic deficits and headache in a patient of this age is a classic presentation of malignancy. Many of the other differential diagnoses are less frequently encountered and have typical imaging findings not present in our patient. Primary central nervous system lymphoma (PCNSL) is typically associated with periventricular lesions but is not uncommonly found in the subcortical white matter. Imaging findings of PCNSL include sharply defined borders without central necrosis or hemorrhage, restricted diffusion on brain MRI diffusion-weighted imaging sequence, and uniform enhancement. Mycophenolate mofetil exposure, as was noted in our patient, or other immunosuppressant exposure increases the risk of PCNSL. The lack of typical brain MRI findings, including contrast enhancement or diffusion restriction, and the presence of lobar microhemorrhages are unusual for PCNSL. In addition, the lack of CSF pleocytosis or abnormal cytology or flow cytometry argues against a diagnosis of PCNSL. 4 Finally, repeat brain MRI imaging after a course of corticosteroids would be expected to show dramatic improvement in PCNSL.
Solid malignancy also deserves consideration, though the radiographic features of minimal contrast enhancement, relative homogeneity, and lack of tissue necrosis point to a more indolent process rather than an aggressive tumor. Low-grade malignancies can present acutely when they reach a threshold in size or begin affecting eloquent cortex leading to a more rapid clinical deterioration. Cerebral microhemorrhages confined to the area of T2 hyperintensity raised concern for solid malignancy, as other etiologies of microhemorrhages, including hypertension and CAA, typically produce a more diffuse, bilateral pattern. However, the homogeneity within the centrum semiovale was atypical for solid malignancy—more often there is a heterogeneous appearance due to vasogenic edema contrasting with the underlying mass lesion.
Subacute infarction is a frequent cause of a T2 hyperintense lesion with associated mass effect. However, a subacute infarct should fit a vascular territory and often has contrast enhancement, while this lesion involves multiple vascular territories and has no enhancement. Vasogenic edema was seen on T2-FLAIR in the current case, as compared to the cytotoxic edema pattern expected with ischemia. An infarct would also present with acute symptoms unlike our patient's insidious presentation.
Mass lesions have been reported in cases of primary angiitis of the central nervous system (PACNS), most frequently when PACNS is associated with vascular amyloid deposition, as in cases of CAA-RI. Cerebral amyloid angiopathy-related inflammation, a rare subtype of CAA characterized by immune-mediated perivascular inflammation, can also present with headache, focal neurologic deficits, and unilateral vasogenic edema on imaging. Cerebral amyloid angiopathy has a strong predilection for patients greater than 60 years of age and is only rarely reported in younger cohorts. However, CAA-RI affects a greater proportion of younger patients compared with noninflammatory CAA. 5,6 A meta-analysis of all biopsy proven cases of CAA-RI reported cognitive and behavioral change, headache, and focal neurologic deficits to be the most common clinical manifestations. 2 Contrast enhancement was noted in 63% of cases, and mass effect in 50%. Unlike the more common CAA, CAA-RI often demonstrates unilateral vasogenic edema on brain imaging. Cerebral microhemorrhages are common on hemosiderin-sensitive imaging studies and tend to be lobar and bilateral. Our patient’s age and clinical presentation are both typical of CAA-RI. The imaging further suggests CAA-RI, although the confinement of the microhemorrhages to the area of vasogenic edema is unusual.
The patient’s presentation with headache and marked vasogenic edema with areas of petechial hemorrhage merits consideration of cerebral venous sinus thrombosis (CVT). The age at presentation in our patient is atypical for CVT. The largest cohort study of CVT found that 78% of cases occurred in patients less than 50 years of age. 7 Venous sinus thrombosis can present with infarction and/or vasogenic edema, 8 yet the distribution and extent of our patient’s edema, involving the frontal, parietal, and temporal lobes, would be unusually extensive. Typically, superior sagittal sinus thrombosis results in impaired function of the frontal, parietal, and occipital lobes while transverse sinus and sigmoid sinus thromboses affect the temporal lobe. 9 Isolated cortical vein thrombosis can present similarly to CVT. Vein of Labbe thrombosis involves the temporal lobe, while vein of Trolard thrombosis compromises the parietal lobe. Further, the noncontrast MRI reveals normal flow voids and the postcontrast MRI demonstrates patent sagittal and transverse venous sinuses.
Posterior reversible encephalopathy syndrome represents another interesting, albeit unlikely consideration in the differential. The patient’s clinical presentation lacks many of the typical features of PRES, including the tetrad of visual changes, seizure, headache, and encephalopathy. Mycophenolate mofetil has been implicated in PRES 10 but is an unusual offending agent, with chemotherapeutic agents, and calcineurin inhibitors such as tacrolimus being more common. The unilateral distribution of edema and frontal lobe involvement are atypical for PRES, but both have been described. One large series found unilateral PRES in 2.6% of cases. 11 Mass effect is also uncharacteristic, however, cases of PRES mimicking glioma with mass effect have been reported. 12 Hemorrhage complicates about 15% of PRES cases with petechial hemorrhages being the most common. 13 One possible distinction on brain MRI between PRES and CAA-RI is the tendency of CAA-RI edema to be hypointense on T1 sequences (Figure 1), while lesions in PRES are typically isointense on T1, but such radiographic differences do not reliably differentiate the two. 5
In a patient on chronic immunosuppression presenting with headache and mental status changes, infectious etiologies should also be considered. The lack of meningismus or fever, meningeal enhancement on MRI, and pleocytosis on CSF analysis effectively eliminates meningitis. Encephalitis is unlikely as it tends to present with fever, seizures, and focal neurologic deficits in addition to confusion, behavioral changes, and decreased level of consciousness. Cerebritis may have a more subtle clinical presentation than encephalitis, and CSF cell count and protein may be normal. Systemic markers of infection such as leukocytosis also lack sensitivity for both cerebritis and brain abscess. 14 The progression from cerebritis to brain abscess follows discrete radiologic and pathologic stages. Early cerebritis is characterized on brain MRI by ill-defined contrast enhancement and poorly demarcated T2 hyperintensity. With time, focal cerebritis may progress to an encapsulated abscess with restricted diffusion centrally and associated vasogenic edema on brain MRI. 15 Early cerebritis represents the most compelling infectious possibility in our case given the imaging studies, CSF profile, and clinical presentation of our patient, although the imaging findings, including the lack of contrast enhancement, would be atypical.
One final infectious consideration is PML. Progressive multifocal leukoencephalopathy, an infection of the JC virus, typically manifests with seizures and focal neurologic deficits in the setting of immunosuppression. Case reports have implicated mycophenolate mofetil as a risk factor for PML. 16 Progressive multifocal leukoencephalopathy typically exhibits multiple T2 hyperintense lesions within the periventricular white matter on brain MRI, which are hypointense on T1 and lack contrast enhancement or mass effect. Intraparenchymal hemorrhages (IPHs) are not typical of PML but have been reported. 17 Our patient’s solitary lesion, extensive mass effect, and clinical improvement with corticosteroids would be incongruous with PML.
Diagnostic Results
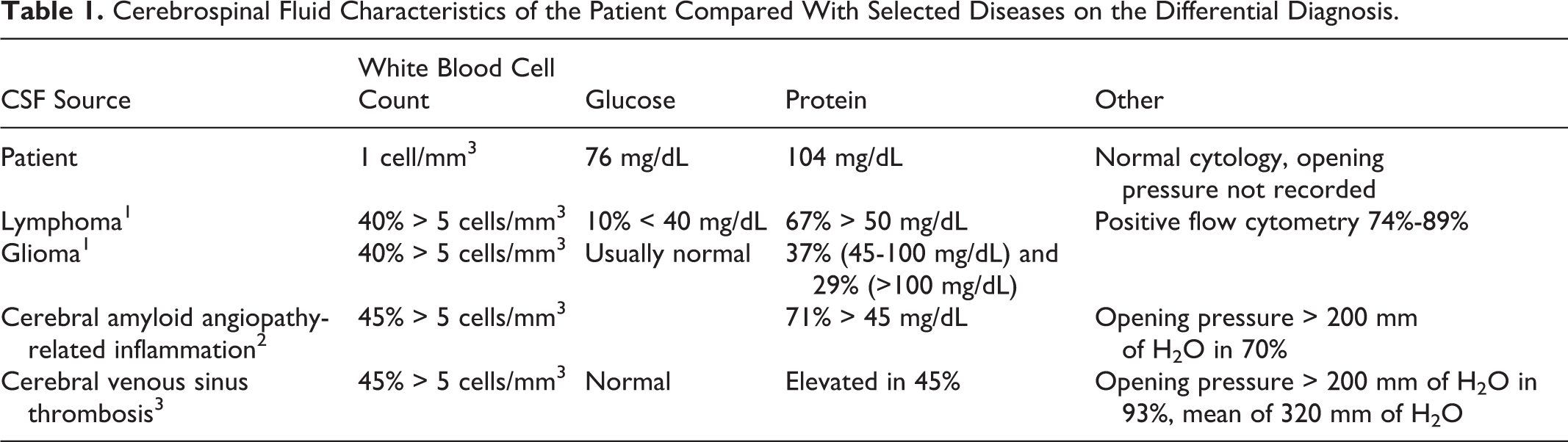
Three days after her initial admission, the patient underwent a brain biopsy at the outside hospital. Brain biopsy revealed CAA-RI (Figure 2).
Brain biopsy of left temporoparietal region (images and interpretation courtesy of Dr Desiree Marshall and Dr Dirk Keene). A, Hematoxylin and eosin (H&E) stain, 200× magnification, shows a meningeal vessel with amyloid (arrow head) and surrounding inflammatory cells (arrows). B, Congo red stain, 400× magnification, highlights amyloid in the vessel wall (arrows). C, Amyloid β immunohistochemistry (IHC), 400× magnification, shows amyloid β in the vessel wall (arrow) and adjacent amyloid plaque in brain parenchyma (arrow head).
Cerebral Amyloid Angiopathy-Related Inflammation
Discussant: Dr Erica Byrd
CAA is a disease isolated to the brain in which amyloid infiltrates the small- and medium-sized arteries, arterioles, and less often veins of the leptomeninges and superficial cortex. CAA can be either sporadic or hereditary but the single most identifiable risk factor is aging. 18
Patients with CAA can present with IPH, cognitive dysfunction, or episodic spells with focal neurologic deficits that often resemble transient ischemic attacks (TIAs). CAA-associated IPHs are classically lobar and over time, may accumulate, becoming bilateral or multilobar. 18 Intraparenchymal hemorrhage due to CAA, typically occurring in patients in their eighth decade or older, accounts for an estimated 10% to 34% of spontaneous IPH. 2 The pathophysiology of IPH in CAA is not clearly understood, with various mechanisms proposed for amyloid β (Aβ) accumulation. More recently, suggested mechanisms have included production of Aβ by smooth muscle cells and/or pericytes of vessel walls and impaired perivascular drainage from the neuropil. 19 Dementia in CAA has been described as rapidly progressive, in contrast to Alzheimer dementia, with severe vascular amyloid, large and small lobar hemorrhages, small cortical infarctions, and neuritic plaques. 20 Transient, stereotyped neurologic symptoms concerning for TIA may also occur in CAA, termed “amyloid spells.” The underlying mechanism of such spells is unclear, although focal seizures caused by IPH are a presumed etiology. 20 Although amyloid spells often respond to antiepileptic medication, the recurrence of IPH and decline of cognitive function in CAA have no proven treatments.
In contrast, CAA-RI is a less common but treatable variant of CAA. The syndrome has been given various labels, emphasizing the relationship between amyloid and vasculitis, including primary angiitis of the central nervous system (PACNS) associated with CAA and Aβ-related angiitis. 2,6 CAA-RI likely is the result of inflammation in blood vessel walls due to improper clearance and accumulation of Aβ. 2 The incidence is equal in men and women. The mean age of onset of CAA-RI is in the seventh decade, distinguishing CAA-RI from PACNS, onset in the fifth decade, and from CAA, onset in the eighth decade. 5,6
Clinical Presentation and Diagnosis
Patients with CAA-RI typically present with acute to subacute cognitive and behavioral changes, headache, focal neurological signs, and seizures. 21 Diagnostic criteria (Table 2) include both clinical and MRI findings. Our patient met all of the clinical and radiographic criteria of CAA-RI—the insidious onset of headache and mental status change in the setting of an abnormal brain MRI showing asymmetric and confluent hyperintensity with multiple subcortical microhemorrhages. As demonstrated in our case, SWI has been shown to have greater sensitivity to detect cerebral microhemorrhages compared with the routine MRI GRE sequence. 22 Thin-section SWI imaging in patients with CAA reveals approximately 3 times as many cerebral microhemorrhages compared to conventional GRE imaging. 23 The cerebral microhemorrhages in CAA-RI are typically located separate from white matter lesions, 5 whereas the cerebral microhemorrhages in our patient’s brain MRI were localized to the area of hyperintensity. The patchy or confluent areas of T2 hyperintense signal in CAA-RI are usually asymmetric and postulated to result from an inflammatory response to cerebral amyloid leading to vascular endothelial dysfunction and fluid leakage into the surrounding tissue. 24 The asymmetric MRI appearance may be mistaken for a malignancy, such as in our patient, or infection. A definite diagnosis of CAA-RI (Table 2) would include clinical criteria in addition to pathologic verification of vascular inflammation and amyloid deposition within cortical and leptomeningeal vessels. 2
Proposed Diagnostic Criteria for CAA-RI. 4
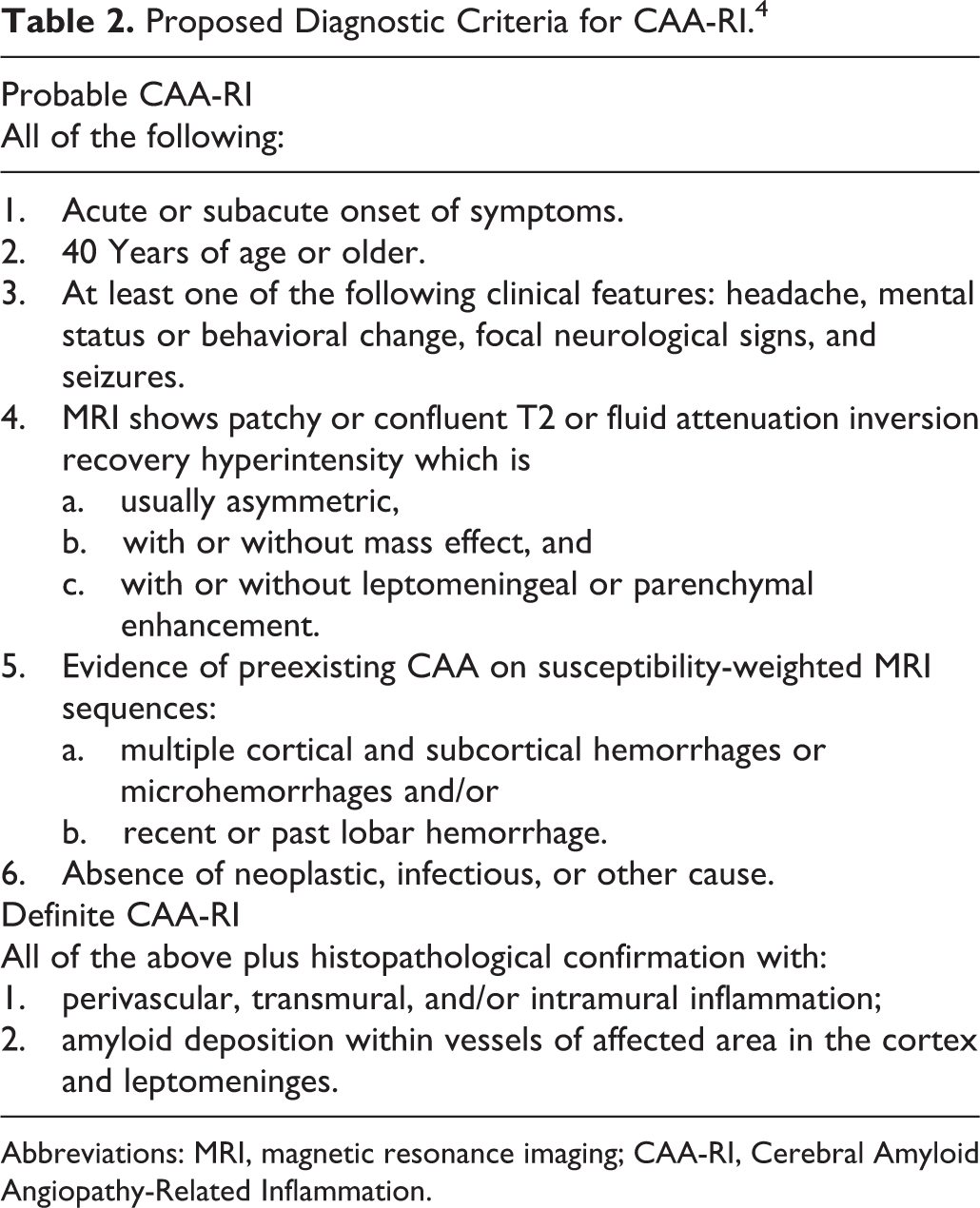
Abbreviations: MRI, magnetic resonance imaging; CAA-RI, Cerebral Amyloid Angiopathy-Related Inflammation.
Supporting laboratory data in CAA-RI may include CSF pleocytosis and elevated CSF protein, but these tests are not specific (Table 1). 6 Currently, there is no single noninvasive diagnostic test for the diagnosis of CAA-RI, although the use of CSF anti-Aβ autoantibodies as potential marker for CAA-RI is currently being investigated. 25 The experimental CSF testing in our patient for the anti-Aβ autoantibodies revealed a markedly elevated level (F. Piazza, personal communication, November 8, 2013). Additionally, the apolipoprotein E ∊4/∊4 genotype has been noted to have a “striking overrepresentation” in patients with CAA-RI, raising the possibility that E4 isoform may have a specific proinflammatory response to CAA. 21
Treatment
The treatment for CAA-RI is immunosuppression, typically with high-dose intravenous steroids. 2,5,21 One treatment protocol is a 5-day course of methylprednisolone (500 mg-1 g/d) followed by a rapid oral steroid taper (S. Greenberg, personal communication, September 10, 2013). Clinical improvement is variable but commonly correlates with radiographic improvement. 2,5 Reimaging and clinical reassessment in 3 to 4 weeks after initiating steroids are recommended. If there is no clinical and/or radiographic improvement, other etiologies should be investigated and brain biopsy should be considered, particularly before considering immunotherapies with significant side effects. Other immunosuppressive agents that have been studied for refractory CAA-RI include cyclophosphamide, methotrexate, or mycophenolate mofetil, although evidence for these agents is limited and the optimal duration of treatment is unclear. 2
Case Follow-Up
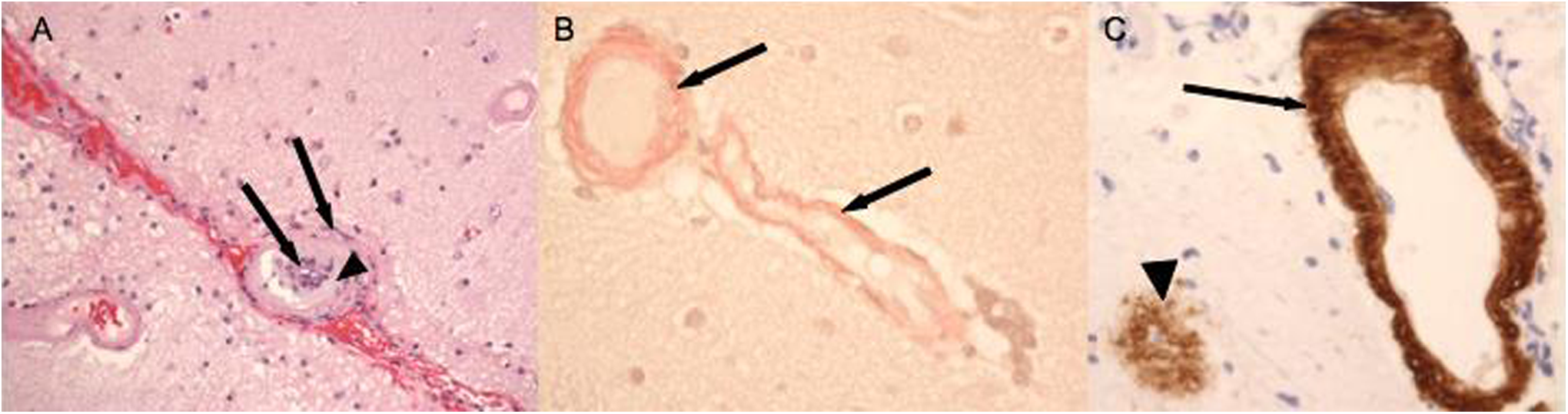
Our patient was tapered off steroids within 2 weeks of hospital discharge and required no further treatment other than her chronic immunosuppression with mycophenolate mofetil. After 6 months, she was near her baseline with only mild acalculia and memory difficulty. Brain MRI at this time showed complete resolution of the confluent area of T2 hyperintensity (Figure 3).
Brain magnetic resonance imaging (MRI) FLAIR sequence at 6-month follow-up. Note the near complete resolution of the hyperintense lesion.
Our case underscores the importance of considering CAA-RI in the differential for asymmetric white matter lesions that may otherwise have the imaging characteristics of a tumor. Prior to biopsy, our patient met clinical and imaging criteria for probable CAA-RI and empiric treatment with steroids would have been reasonable. Such an approach may have avoided the need for a brain biopsy, although fully excluding neoplastic, infectious, or other causes would have been challenging.
Footnotes
Acknowledgments
We wish to thank the patient, who provided her consent for this article. We wish to recognize Drs Desiree Marshall and Dirk Keene who provided the brain biopsy images and assistance with pathology interpretation and Fabrizio Piazza, PhD, and the iCAβ International Network for performing anti-Aβ autoantibody testing.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Keywords
cerebral amyloid angiopathy, cerebral amyloid angiopathy-related inflammation, amyloid-β-related angiitis