
Abstract
Neurosarcoidosis is a rare but important cause of stroke as it is treatable. Cases reported thus far have primarily been in young people who are relatively healthy. Here we report the case of a 73-year-old woman presenting with recurrent strokes and high-grade intracranial stenosis caused by probable neurosarcoidosis. This is unique as neurosarcoidosis is not usually considered as an etiology for recurrent strokes in our patient’s age-group. We review and categorize published cases of neurosarcoidosis causing stroke and describe a classification scheme for certainty of diagnosis. Given the implications of this diagnosis for secondary stroke prevention, we recommend that neurosarcoidosis be considered in the differential for patients with few vascular risk factors, recurrent strokes refractory to medical treatment, or possible vasculitis even in the elderly patients.
Introduction
Stroke is a leading cause of death in developed countries. In the majority of cases, the cause is ischemia due to atherosclerosis (associated with risk factors such as diabetes mellitus, hyperlipidemia, smoking, and hypertension) or thromboembolism secondary to atrial fibrillation. In rare instances, ischemic stroke may be caused by a vasculopathic process associated with underlying rheumatologic or inflammatory disease, infection, drug reaction, or malignancy. In many of these atypical cases, the underlying etiology is never identified. However, searching for the underlying etiology of stroke is important for secondary stroke prevention.
Neurosarcoidosis refers to the diverse neurological manifestations of systemic sarcoid, which occurs in 5% to 15% of those with the disease. 1 Importantly, neurosarcoidosis can present without manifestations of systemic sarcoid in 10% to 17% of cases. 2,3 Although cranial nerve palsies represent the most typical neurological finding, neurosarcoidosis can also cause cerebral vasculitis, resulting in headaches, seizures, confusion, and dementia. 2,4 In recent decades, there have been several case reports demonstrating neurosarcoidosis can also cause stroke. 5 -15 There are several possible pathologic mechanisms including direct invasion of medium and small arteries and arterioles by granulomatous inflammation as seen on autopsy, 16 cardiovascular embolism, and large-vessel inflammation. 5 Here, we describe the case of a 73-year-old woman who presented with recurrent strokes of suspected vasculopathic origin. Her workup points to a diagnosis of neurosarcoidosis causing stroke via high-grade intracranial stenosis. We outline our approach to diagnosis, review reports of neurosarcoidosis causing stroke to date, and provide recommendations for physicians dealing with patients having stroke in whom neurosarcoidosis may be an important differential.
Report
A 73-year-old woman of Jewish descent with a medical history of Crohn disease well controlled without medication, and a localized small bowel malignancy that had been resected many years prior, presented for a second opinion after recurrent strokes occurring over a 13-month period, despite being on dual antiplatelet therapy (aspirin 81 mg and clopidogrel 75 mg daily). Her first stroke was characterized by a nonfluent expressive aphasia. Imaging at that time showed a superior division left middle cerebral artery infarct with no evidence of stenosis or atherosclerosis in her bilateral carotid arteries or large intracranial vessels as imaged by magnetic resonance angiogram (MRA) with contrast. Workup for thromboembolic sources with transthoracic echo and telemetry for 9 days was unremarkable. She had a second stroke 4 months later, and magnetic resonance imaging (MRI) at that time was notable for new infarction in the same territory as her previous stroke but patent intracranial vessels. Her third stroke occurred 6 months later (3 months prior to presentation), and at this time, her noncontrast MRA and computed tomography angiogram (CTA) showed occlusion of the left internal carotid artery (ICA) in the cavernous segment (Figure 1A). An angiogram showed high-grade stenosis of the left ICA as well as both superior cerebellar arteries and proximal posterior cerebral arteries in a pattern that was suspicious for vasculitis, without significant atherosclerosis.
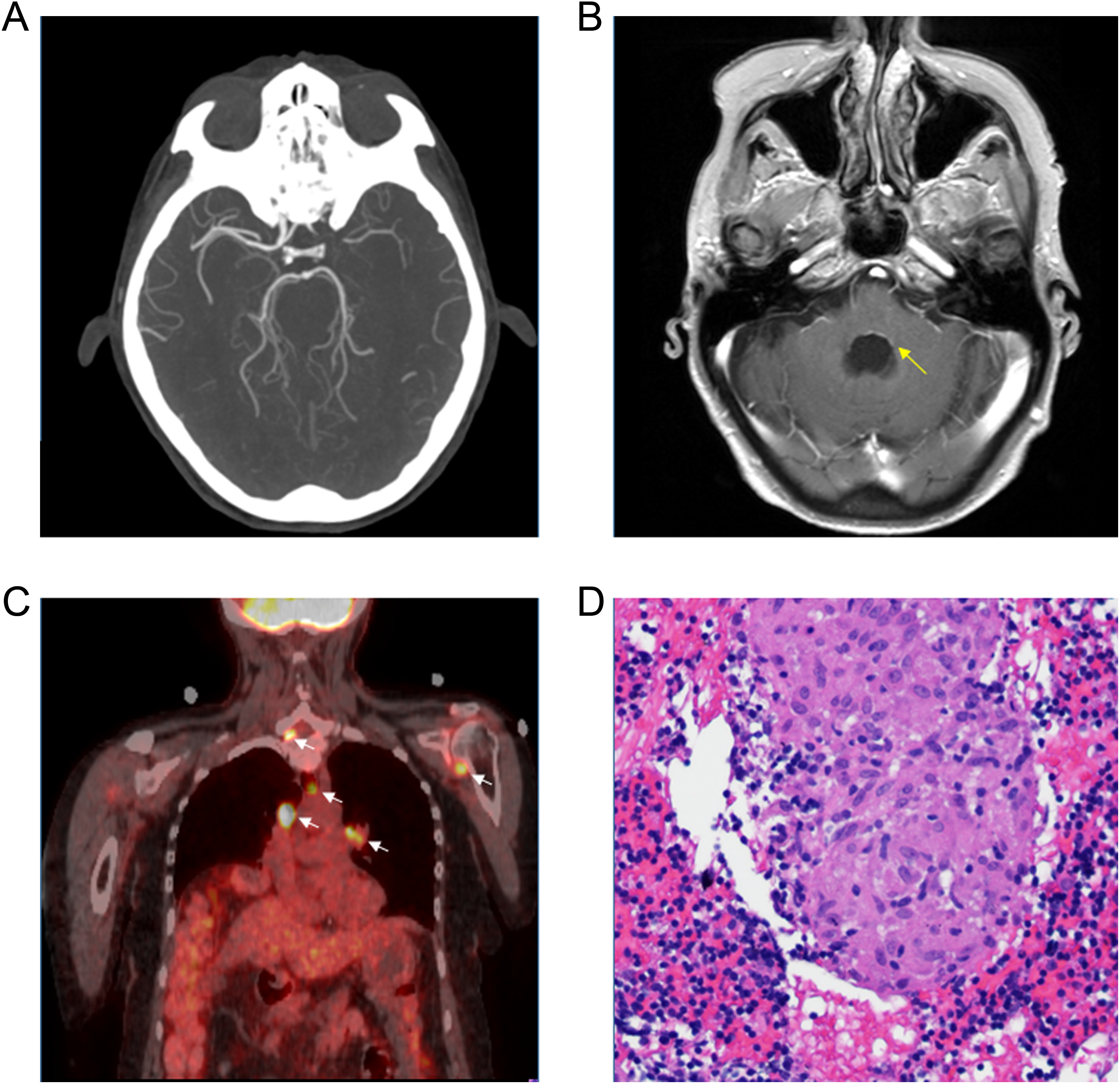
A, Computed tomography (CT) angiogram demonstrating left internal carotid artery occlusion in the distal cavernous segment with retrograde filling. B, Postgadolinium T1 sequence on MRI demonstrating enhancement in the floor of the fourth ventricle (arrow). C, Positron emission tomography demonstrating representative increased fluorodeoxyglucose (FDG) uptake in mediastinal lymph nodes and axillary lymph nodes (arrows). C, Hematoxylin and eosin (H&E) at ×20 magnification of the right supraclavicular lymph node needle biopsy demonstrating noncaseating granuloma (NCG) with histiocytes.
At the time of our evaluation, the patient denied any recent weight loss, fever, chills, rashes, cough, or headaches. General examination was unremarkable aside from an enlarged right supraclavicular lymph node. Neurological evaluation revealed a dense, nonfluent aphasia with intact naming of high-frequency objects and normal comprehension but difficulty naming low-frequency objects and impaired repetition. The remainder of the neurological examination, including cranial nerves, strength, reflexes, sensation, coordination, and gait, was intact with the exception of mild pronator drift in the right arm. Brain MRI was notable for both her recent and distant infarcts and leptomeningeal enhancement most prominent in the floor of the fourth ventricle (Figure 1B). In light of these findings, and the unusual history of recurrent strokes affecting the same vascular territory, a lumbar puncture with flow cytometry was performed. It showed white blood cell count (WBC 39), red blood cell count (RBC) 2, protein 180, and glucose 28. She had positive oligoclonal bands indicating intrathecal synthesis of immunoglobulin IgG. Other cerebrospinal fluid (CSF) studies including herpes simplex virus polymerase chain reaction (PCR), varicella-zoster virus PCR, cytomegalovirus PCR, Epstein–Barr virus PCR, toxoplasmosis IgG and IgM, syphilis (VDRL), lyme PCR, tuberculosis (mycobacterial cultures), angiotensin-converting enzyme (ACE), and cytopathology were normal. Serum studies including erythrocyte sedimentation rate, C-reactive protein, antinuclear antibody, antineutrophil cytoplasmic antibody, serum protein electrophoresis, β-
Given the patient’s age and presence of lymphadenopathy, there was concern the etiology might be due to an occult malignancy. A whole-body positron emission tomography (PET) scan demonstrated multiple enlarged lymph nodes, particularly in the hilar and mediastinal regions, raising concerns for lymphoma, metastatic cancer, or sarcoidosis (Figure 1C). A biopsy of her enlarged supraclavicular lymph node showed histiocytes and granulomas (Figure 1D) but no abnormal cells. A second biopsy obtained from a mediastinal node showed noncaseating granulomas, which are diagnostic for sarcoid. Based on the histological finding of noncaseating granuloma, CSF evidence of inflammation, an MRA suggestive of vasculopathy rather than atherosclerosis, and an MRI showing leptomeningeal enhancement, we diagnosed the patient with probable neurosarcoidosis. She was offered a biopsy but declined, opting for empiric therapy with a high-dose steroid pulse followed by a slow taper instead. Unfortunately, the patient did not experience significant improvement with steroids. Follow-up has been complicated by the patient’s difficulty tolerating treatment and our inability to ascertain whether the stenosis improved due to motion artifact on MRA and insufficient renal function to permit a computed tomography scan with contrast.
Discussion
Neurosarcoidosis is a rare but important cause of stroke that is difficult to diagnose, as it requires a high index of clinical suspicion. To date, there have been only a handful of cases of neurosarcoidosis causing stroke described in the literature, despite the frequent vascular and perivascular involvement observed in the cerebral manifestation of this disease described in autopsy series. 16,17 The most typical presentation is strokes due to small or medium-sized arteries, although large cerebral arteries can be involved as well. 6,10,13 Table 1 summarizes published cases where sufficient information was given to make a diagnosis of both stroke and likely neurosarcoidosis. In the absence of universal criteria for diagnosing neurosarcoidosis, we have classified these cases as definite or probable according to the extent to which they meet criteria for neurosarcoidosis proposed by Zajicek et al. 18 Based on these criteria, a patient with a clinical presentation consistent with neurosarcoidosis in whom alternative diagnoses have been excluded has “definite neurosarcoidosis” with a positive nervous system biopsy. If tissue is not available, a diagnosis of “probable neurosarcoidosis” can be made with laboratory data supporting central nervous system (CNS) inflammation (elevated CSF protein, elevated CSF leukocytes, or positive oligoclonal bands) and/or MRI findings consistent with neurosarcoidosis. 18 Using this classification, our patient has probable neurosarcoidosis.
Literature Review of Cases of Neurosarcoidosis Causing Stroke.
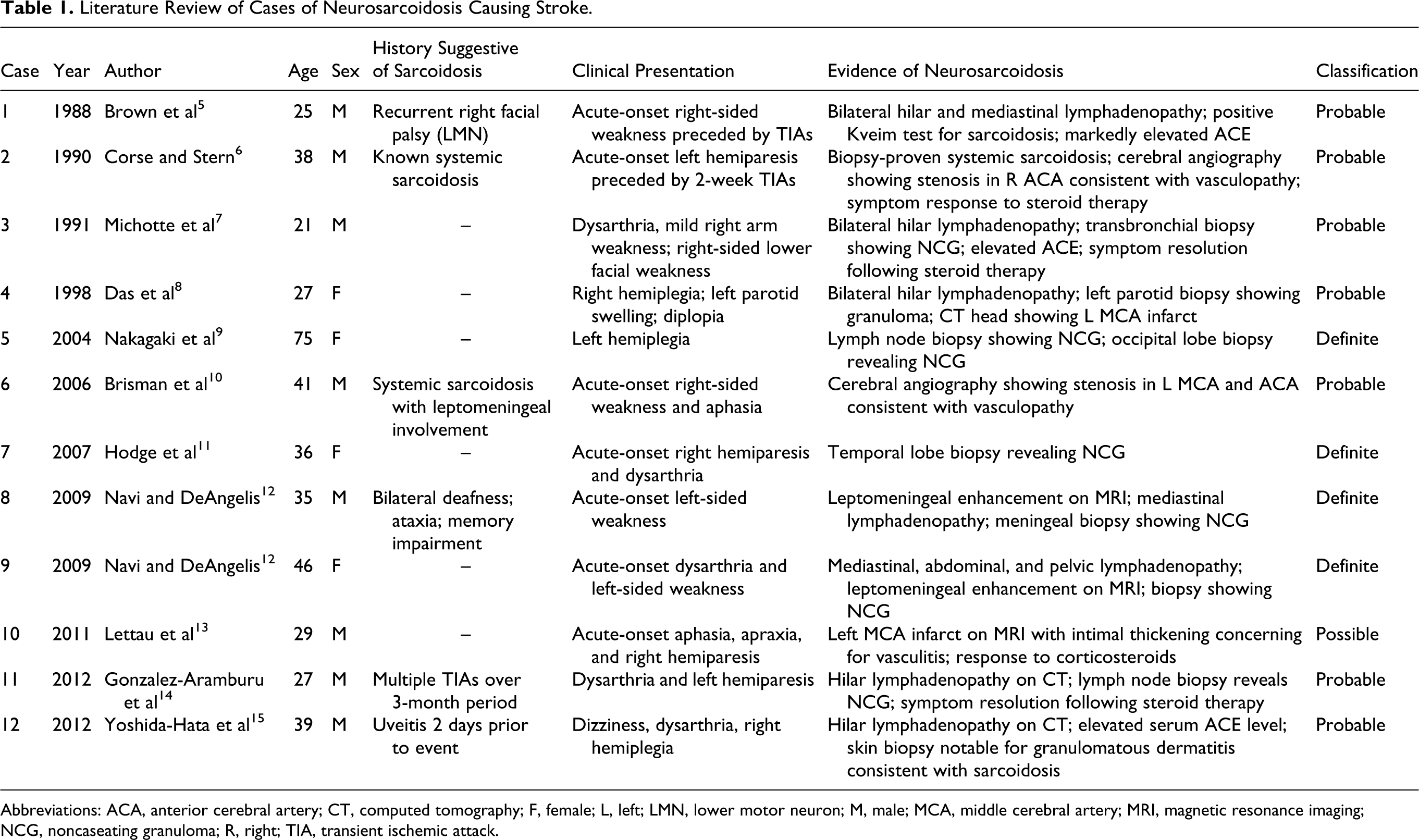
Abbreviations: ACA, anterior cerebral artery; CT, computed tomography; F, female; L, left; LMN, lower motor neuron; M, male; MCA, middle cerebral artery; MRI, magnetic resonance imaging; NCG, noncaseating granuloma; R, right; TIA, transient ischemic attack.
The majority of strokes due to neurosarcoidosis in the literature have occurred in young people. This is very different from our patient who presented at age 73. Although this could indicate that neurosarcoidosis causes strokes more commonly in the young, it is also possible that this represents sampling bias. Older individuals often have many other risk factors for stroke, and a detailed workup including lumbar puncture such as this patient had is frequently not performed in the evaluation of stroke.
We recommend a diagnostic screen for any patient in whom one suspects neurosarcoidosis, which includes MRI with gadolinium, MRA, or CTA to evaluate cerebral vasculature, lumbar puncture to evaluate CSF inflammation, and consideration of a PET scan to evaluate for other etiologies such as lymphoma. Positive nervous system histology is the gold standard for the diagnosis of neurosarcoidosis and should ideally include the area that is affected. However, given the invasive nature of biopsy, access issues, and possible side effects when the CNS is involved, we advise the use of criteria proposed by Zajicek et al 18 for the classification of probable and possible neurosarcoidosis based on alternative findings when biopsy is not possible.
In summary, neurosarcoidosis is a chameleonic disorder, seemingly able to mimic almost any neurological presentation. It presents a diagnostic challenge to the clinician, not least due to the difficulties of obtaining the tissue biopsy necessary for a definitive diagnosis. Given the treatment of neurosarcoidosis is with immunosuppression rather than antiplatelet therapy as would typically be pursued for secondary stroke prevention, it should be considered on the differential in patients who have few vascular risk factors, a history of recurrent strokes refractory to medical therapy, presentation concerning for vasculitis, or atypical intracranial stenosis on cerebral angiography, regardless of patient age.
Footnotes
Authors’ Note
The patient described in this report consented to the report, and a waiver was granted from the Johns Hopkins IRB Committee per policy 102.3.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.