
Abstract
Objectives:
Posterior reversible encephalopathy syndrome (PRES) is a clinicoradiological syndrome characterized by headache, altered mental status, seizures, or loss of vision. In this study, we report the largest series of PRES coming from Saudi Arabia and explore the etiology, clinical presentation, and outcome. We also report new imaging findings associated with this condition.
Methods:
We performed a retrospective study of all cases of PRES admitted to King Abdulaziz Medical City, Jeddah, Saudi Arabia, between the years 2005 and 2015. A neurologist reviewed all charts and analyzed the clinical presentations, etiological factors, and outcomes, and a neuroradiologist reviewed the imaging studies. Only patients with clinical and imaging features consistent with PRES were included in the study.
Results:
We collected 31 patients who had clinical and radiological features consistent with PRES. Females were more affected than males (18 females and 13 males), and patients’ age ranged from 6 to 95 years, with a mean of 38.3 years. Patients were treated by removing the precipitating causes and treating the underlying conditions. Resolution of neurologic signs occurred within 2 to 3 weeks in all patients.
Conclusion:
In our opinion, PRES itself is usually a benign condition with complete recovery if the condition is recognized early and managed appropriately. Although clinical signs are nonspecific, the constellation of symptoms including headache, visual problems, seizures, and altered level of consciousness should suggest the possibility of PRES, especially in high-risk group. Abnormalities on magnetic resonance imaging are often characteristic and may be the first clue to the diagnosis.
Introduction
Posterior reversible encephalopathy syndrome (PRES) is a clinicoradiological syndrome characterized by visual disturbances, headache, altered mental status, seizures, and occasional focal neurological signs. 1 In 1996, Hinchey et al 1 used this term for the first time and suggested that PRES represented a localized manifestation of hypertensive encephalopathy. The causes of this condition are diverse, but common precipitants include acute elevation of blood pressure, immunosuppressive drugs, and renal failure. The characteristic findings on imaging are subcortical edema without infarction in a relatively symmetrical pattern. These changes predominantly involve the parietal and occipital lobes, corona radiata, pons, and cerebellum. 2,3 These striking imaging findings resolve on follow-up studies after appropriate therapy. 4 In this study, we report the largest series of PRES coming from Saudi Arabia. Then we explore the etiology, clinical presentation, and outcome. The aim of this study is to shed light on this syndrome and its pathophysiology and to demonstrate its benign nature if treated appropriately. We also report new imaging findings associated with this condition.
Patients and Methods
This study is a retrospective review of patients presented to King Abdulaziz Medical City (KAMC), Jeddah, Saudi Arabia, and diagnosed with PRES during a 10-year period from January 2005 to September 2015. The KAMC–Jeddah is a teaching and tertiary care center for all medical and surgical specialties. In the western region of Saudi Arabia, it is a major referral center for the management of patients with cancer and is also involved in the management of patients with renal disorders including renal failure. This study was approved by the institutional review board of King Abdullah International Medical Research Center and since this is an observational study, the consent was waived per the institutional policy. A neurologist reviewed all charts after identification of patients using the International Classification of Diseases, Tenth Revision code and analyzed the clinical presentations, etiological factors, and outcomes, and a neuroradiologist reviewed the imaging studies. Only patients with clinical and imaging features consistent with PRES were included in the study. Total number of patients was 31 (13 males and 18 females). All charts were reviewed systematically, including history and neurological examination, at the time of presentation. In addition, information regarding concurrent medical illnesses, medications, and the results of electroencephalogram recordings (if done) were analyzed. Laboratory investigations including complete blood count, urea, creatinine, electrolytes, and liver function test were also reviewed. In patients on immunosuppressive therapy, drug levels prior to, during, and after episode of PRES were reviewed and compared. The cerebrospinal fluid was also reviewed if a lumbar puncture was performed. All neuroimaging studies including computed tomography (CT) and/or magnetic resonance imaging (MRI) were reviewed by a neuroradiologist. Results were analyzed including the distribution of lesions, predominant lobe involvement, presence of restricted diffusion, and contrast enhancement. The degree of resolution of abnormalities was assessed in patients who had a follow-up study.
Results
Table 1 provides the number of patients, male to female ratio, and patients’ age. Patients’ age ranged from 6 to 95 years, with a mean of 38.3 (median 35). Seizures were the presenting feature in 17 patients, 1 was partial and the rest were generalized tonic–clonic seizures. One patient presented with status epilepticus due to eclampsia. Other presenting features included acute confusional state (10), headache (10), visual symptoms (9), sensory symptoms (1), and vomiting (6). No patients had focal sensory or motor deficits. There were 2 patients who were admitted to intensive care, whereas the rest of the patients were managed either in emergency department or in medical ward.
Clinical Data of Patients in Our Study With Posterior Reversible Encephalopathy Syndrome.a
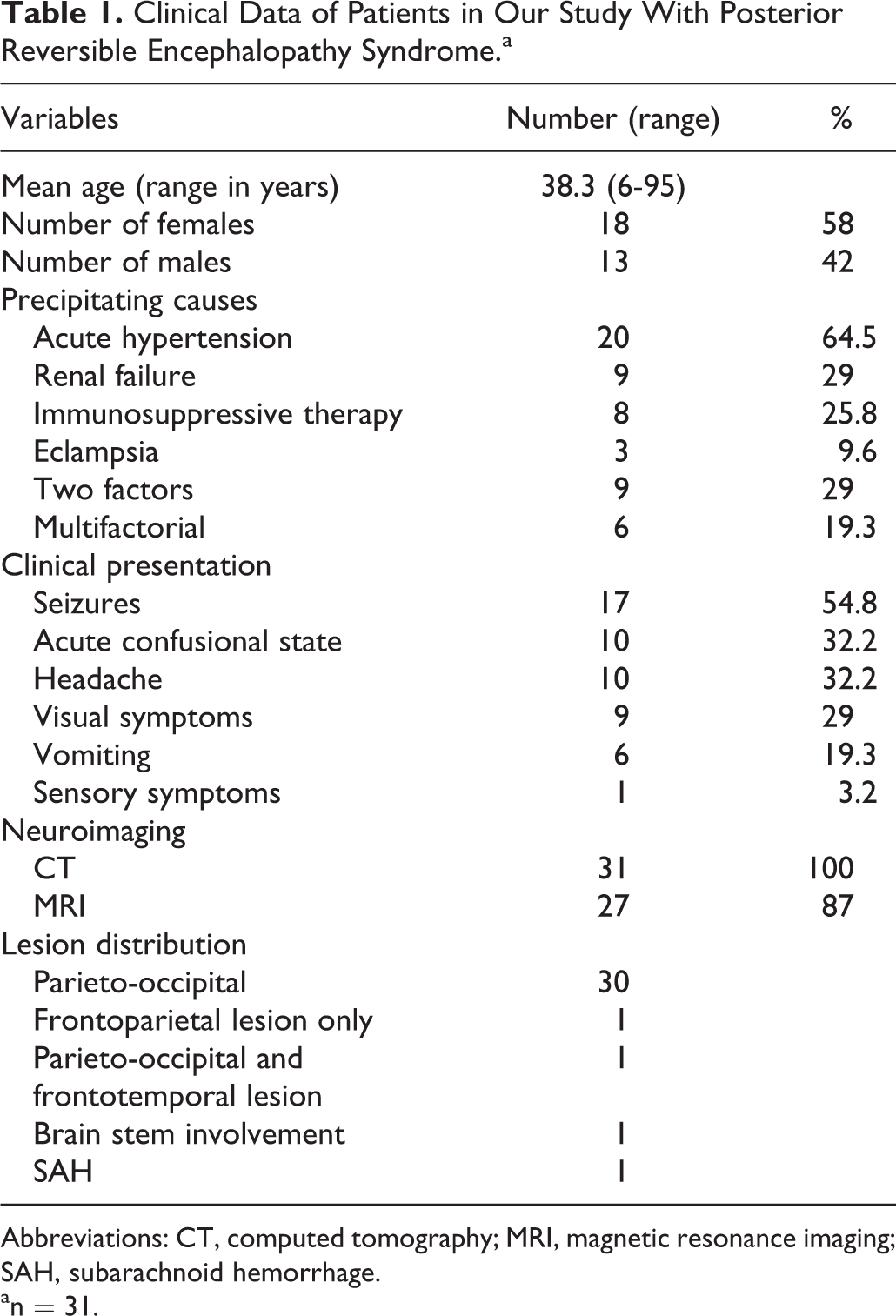
Abbreviations: CT, computed tomography; MRI, magnetic resonance imaging; SAH, subarachnoid hemorrhage.
an = 31.
In our study, the causes of PRES were acute hypertension in 20 (64.5%) cases, renal failure in 9 (29%) cases, and immunosuppressive therapy in 8 (25.8%) cases. Other causes included eclampsia in 3 (9.6%) cases and pulse steroid therapy in 1 (3.2%) case. All 3 patients with eclampsia have recovered rapidly after control of their blood pressure with magnesium sulfate infusion and delivery. One patient had intrauterine fetal death and 2 patients had normal baby after performing a cesarean section. Chronic hypertension was noticed in 22 (70.9%) patients. Two precipitating factors causing this syndrome were observed in 9 (29%) cases. More than 3 precipitating factors were observed in 6 (19.3%) cases. The immunosuppressive agents causing PRES (8 cases) were cyclosporine, FK506 and Methotrexate. Reasons for using these chemotherapeutic agents were renal transplant (4 patients), hematological malignancies (3 patients), and choriocarcinoma (1 patient). Serum levels of immunosuppressive drugs were within the therapeutic value in all patients. One patient abused cocaine with secondary hypertensive encephalopathy, with no past history of any medical illness. From our series, 1 patient with autoimmune hemolytic anemia developed PRES following the initiation of pulse steroid therapy but had complete resolution of PRES symptoms after the steroids were stopped.
In our study, all our patients had CT and only 27 patients had MRI. Characteristic CT abnormalities of PRES include areas of hypodensity in the white matter predominantly posteriorly in the occipital and parietal lobes, however, other regions such as the frontal lobes, basal ganglia, and posterior fossa structures have been visualized. On MRI, these changes correlate with high signal intensity on T2-weighted images. Diffusion-weighted imaging (DWI) and apparent diffusion coefficient (ADC) maps did not show restricted diffusion (except in 1 patient) that is thought to reflect vasogenic edema (Figure 1). In 1 patient with eclampsia, subarachnoid hemorrhage (SAH) was seen in addition to the previously mentioned changes of PRES (Figure 2). Although PRES is known to predominantly affect the white matter, cortical involvement has been reported in a significant number of cases. Occipital and parietal white matter edema was seen in all patients in our series. Additional involvement of temporal lobes, frontal lobes, and basal ganglia was seen in 5 patients. Unfortunately, DWI and ADC maps were done only in 16 patients. Follow-up clinic visits with MRI was done in all of our patients with complete resolution of white matter edema noticed within 4 weeks of the onset of the problem. The mean follow-up interval was 16 months.
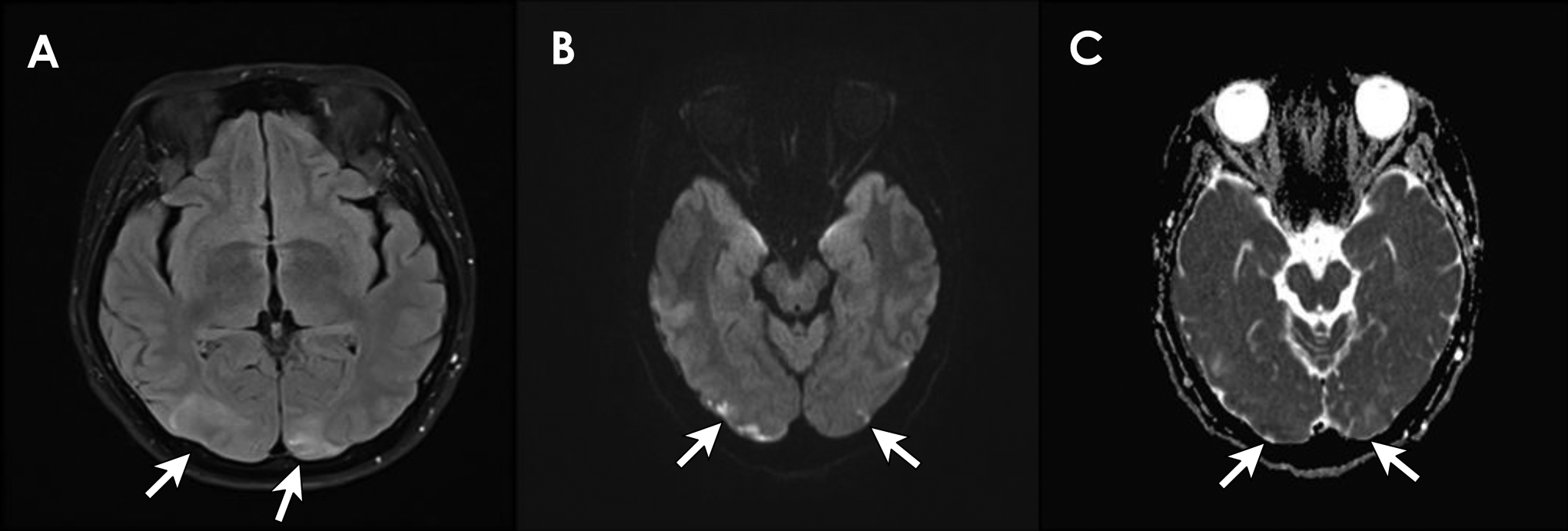
Magnetic resonance imaging (MRI) brain of a 45-year-old woman with acute hypertension and seizures. Fluid-Attenuated Inversion Recovery (FLAIR) image (A) is showing the typical occipital changes in posterior reversible encephalopathy syndrome (PRES). B1000 image (B) is showing occipital cortical–restricted diffusion and apparent diffusion coefficient (ADC) confirms this (C).
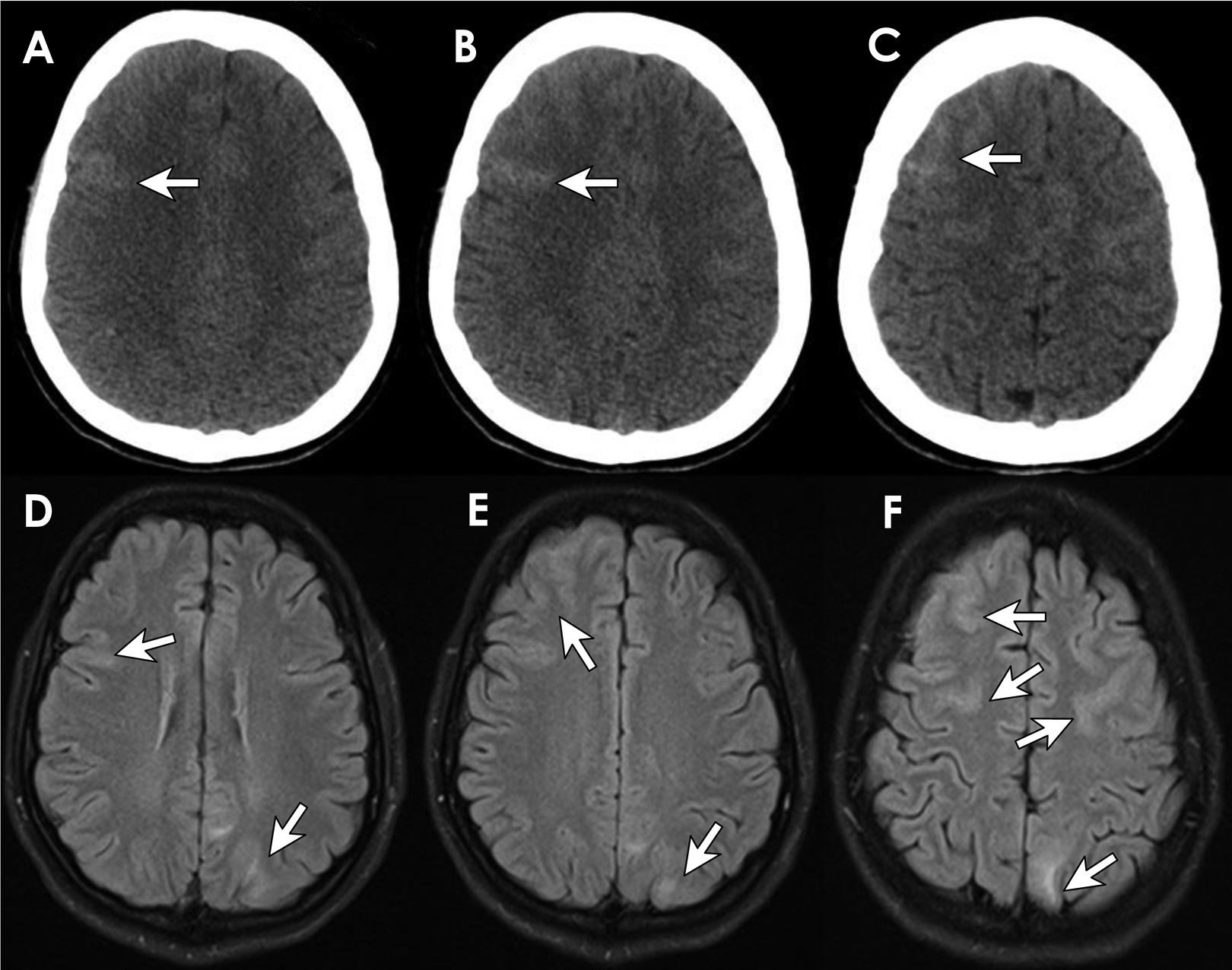
Multiaxial computed tomography (CT) scan images of the brain without intravenous (IV) contrast. A-C show evidence of subarachnoid hemorrhage seen in the right anterior frontal region reaching up to the vertex with suspicious subarachnoid hemorrhage on the left anterior frontal areas also seen. Magnetic resonance imaging (MRI) of the brain (D-F) is showing areas of vasogenic edema seen involving the left parietal lobe with no associated restricted diffusion and bilateral frontal linear high signal intensity seen within the sulci of the frontal lobe in the FLAIR sequences in keeping with bilateral subarachnoid hemorrhage.
Lumbar puncture was done in 1 patient who had changes of PRES and SAH on CT. It showed normal values with no evidence of xanthochromia. This patient had also both CT angiography and 4-vessel cerebral angiography to rule out the possibility of aneurysmal bleeding or arteriovenous malformation. These tests were also unremarkable.
Patients were managed by removing the precipitating causes and treating the underlying conditions. These include antihypertensive agents, decreased doses or withdrawal of the offending immunosuppressant drugs, treating eclampsia, or hemodialysis. Resolution of neurologic signs occurred within 2 to 3 weeks in all patients with no mortality or morbidity related to PRES.
Discussion
Posterior reversible encephalopathy syndrome is a clinical and radiological syndrome first coined by Hinchey et al 1 in 1996. She described 15 patients with clinical and radiological findings of PRES, and all her patients recovered completely. In fact, this syndrome was described prior to Hinchey report by Fisher et al in 1985 in patients with hypertensive encephalopathy. 5 A number of different terminologies have been used to describe this syndrome such as posterior leukoencephalopathy syndrome, reversible posterior cerebral edema syndrome, reversible posterior leukoencephalopathy syndrome, and reversible leukoencephalopathy syndrome. There is still disagreement over the appropriate terminology of this condition for various reasons including that the lesions are not always posterior, the changes may involve cerebral cortex and are not always confined to the white matter. The condition is not always reversible but is not a true leukoencephalopathy.
Posterior reversible encephalopathy syndrome is caused by diverse precipitants that include acute elevation in blood pressure, renal failure, and treatment with immunosuppressive drugs. Our study yielded similar results, with acute hypertension, renal failure, immunosuppressive therapy, and eclampsia being the main causes of PRES. 1,6 Some patients had more than 1 contributory factor especially in patients with renal disease and posttransplant patients. This implies that this disorder may be multifactorial in etiology and pathogenesis.
In our study, females were more affected than males, which is consistent with most published studies. A higher incidence of PRES in women may result from differences in vascular reactivity to various hormones. 1,7
The pathophysiology of PRES has been studied extensively and continued to be debated. Two opposed mechanisms have been suggested—the earliest theory suggested that overreaction of brain autoregulation results in cerebral vasospasm and reversible ischemia to the brain, especially in the vascular border zone territories. 8 –10 This hypothesis is based on angiographic finding of arteriolar vasoconstriction, vessel thrombosis, and infarction especially in patients with eclampsia. Pathological reports in PRES have shown little or no evidence of infarction, instead revealing only interstitial edema and petechial microhemorrhages. An alternative view suggests that sudden systemic blood pressure elevation exceeds the autoregulatory capabilities of brain vasculature. This failure of autoregulation leads to brain hyperperfusion, with resultant breakdown of blood–brain barrier, allowing extravasations of fluid, macromolecules, and even red blood cells into the brain parenchyma. 6,11,12 This theory is also supported by other studies, with DWI and ADC maps suggesting that PRES represents vasogenic rather than cytotoxic edema. 13 The tendency for the involvement of posterior rather than anterior circulation can be explained by topographic variation in the cerebrovascular sympathetic innervation. 1,14 The density of sympathetic innervation is maximal in the anterior cerebral circulation (supplied by branches from the superior cervical ganglion along the carotid arteries). It decreases posteriorly, and the innervation density is the lowest in the basilar artery and its branches. As a result, sympathetic-mediated vasoconstriction may be more effective in protecting small perforating arterioles in the anterior circulation during hyperperfusion secondary to sudden increases in blood pressure. This is exaggerated by fluid-retaining conditions such as eclampsia, acute glomerulonephritis, or treatment with immunosuppressants such as cyclosporine, tacrolimus, and interferon α. Patients with chronic elevation of blood pressure develop adaptive vascular mechanisms and need higher blood pressure to overcome this cerebral autoregulation. In patients with normal or only mildly elevated blood pressure, disruption of the blood–brain barrier is believed to result from endothelial toxic effects of underlying conditions such as sepsis and chemotherapeutic drugs. Certain drugs such as cyclosporine are more associated with PRES than other drugs, likely due to its ability to cause elevation of blood pressure and fluid retention. Cyclosporine also has a direct toxic effect on vascular endothelium, resulting in release of endothelin, prostacyclin, and thromboxane A2. 15 Cyclosporine has high lipophilic property and about 80% of total cyclosporine in plasma binds to high- and low-density lipoproteins. As a result, low plasma cholesterol levels can result in increased incidence of cyclosporine-induced neurotoxicity because of an increase in unbound cyclosporine in plasma. Other factors that potentiate the neurotoxic effects of cyclosporine include hypomagnesemia, aluminum overload, and high-dose steroids. 11,13 Once it crosses the blood–brain barrier, cyclosporine binds to lipid-rich neuronal tissue and exerts a direct toxic effect on neurons and results in edema.
The possibility that seizures could be a potential cause of PRES, rather than a symptom of the condition, has been suggested previously. 7,16 Seizures themselves may contribute to an abrupt rise in blood pressure and may increase vascular permeability by increasing serum CO2 and lactate levels. In our series, none of our 12 patients who presented with seizures or status epilepticus developed epilepsy, and antiepileptic drugs were discontinued 6 months after the illness, with full recovery. This is consistent with the more widely accepted view that seizures are a symptom of the disease process rather than the initiating event.
Other reported causes of PRES include systemic lupus erythematosus, polyarteritis nodosa, endocrine disorders including pheochromocytoma and primary hyperaldosteronism, porphyria, thermal injury, scorpion envenomation, thrombotic thrombocytopenic purpura, hemolytic uremic syndrome, hypercalcemia, and blood transfusion. 17 None of these medical conditions were seen in our series.
Posterior reversible encephalopathy syndrome has also been reported to be caused by few other drugs such as immunotherapy with interleukin, 18 antiretroviral therapy in HIV-infected patients, 19 erythropoitin, 20 granulocyte-stimulating factor, 21 intravenous immunoglobulins, 22 and over-the-counter stimulants 23 such as phenylpropanolamine, ephedrine, and pseudoephedrine.
Conclusion
In our opinion, PRES itself is usually a benign condition with complete recovery if the condition is recognized early and managed appropriately. The recognition of this disorder is important to avoid incorrect diagnosis and mismanagement and also to stop the ongoing etiological process. Although clinical signs are nonspecific, the constellation of symptoms including headache, visual problems, seizures, and altered level of consciousness should suggest the possibility of PRES especially in high-risk group. Abnormalities on MRI images are often characteristic and may be the first clue to the diagnosis. The important differential diagnoses are multiple bilateral cerebral infarcts, viral encephalitis, opportunistic infection including tuberculous, fungal, and viral agents especially in patients on immunosuppressive drugs, demyelination, and vasculitis. An interesting finding in 1 of our patients was SAH secondary to eclampsia that is an extremely rare finding in the literature. In most cases, PRES can be managed easily by control of blood pressure and seizures as well as by reduction or temporary discontinuation of any culpable immunosuppressive drugs. While waiting for confirmation of the diagnosis and the results of various serological tests and cultures, empirical therapy with antiviral, antifungal, and antituberculous drugs has the potential to aggravate renal impairment in postrenal transplant patients presenting with PRES. Similarly, unnecessary discontinuation or dose reduction of immunosuppressive drugs may aggravate graft versus host disease in posttransplant patients. These management difficulties highlight the importance of prompt and accurate diagnosis of PRES.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.