
Abstract

Keywords
A 39-year-old woman with 3 prior episodes of aseptic meningitis without identified pathogen in cerebrospinal fluid (CSF) testing presented with 2 days of headache and neck stiffness. Examination was remarkable only for meningismus. Cerebrospinal fluid revealed lymphocytic pleocytosis (775 cells/µL, 82% lymphocytes, 13% monocytes), elevated total protein (90 mg/dL), normal glucose, negative Gram stain, and the presence of herpes simplex virus 2 (HSV-2) DNA on polymerase chain reaction (PCR) amplification. Cytology revealed large monocytes with varied nuclear morphologies, consistent with Mollaret cells (Figure 1). Treatment with intravenous acyclovir led to rapid clinical improvement.
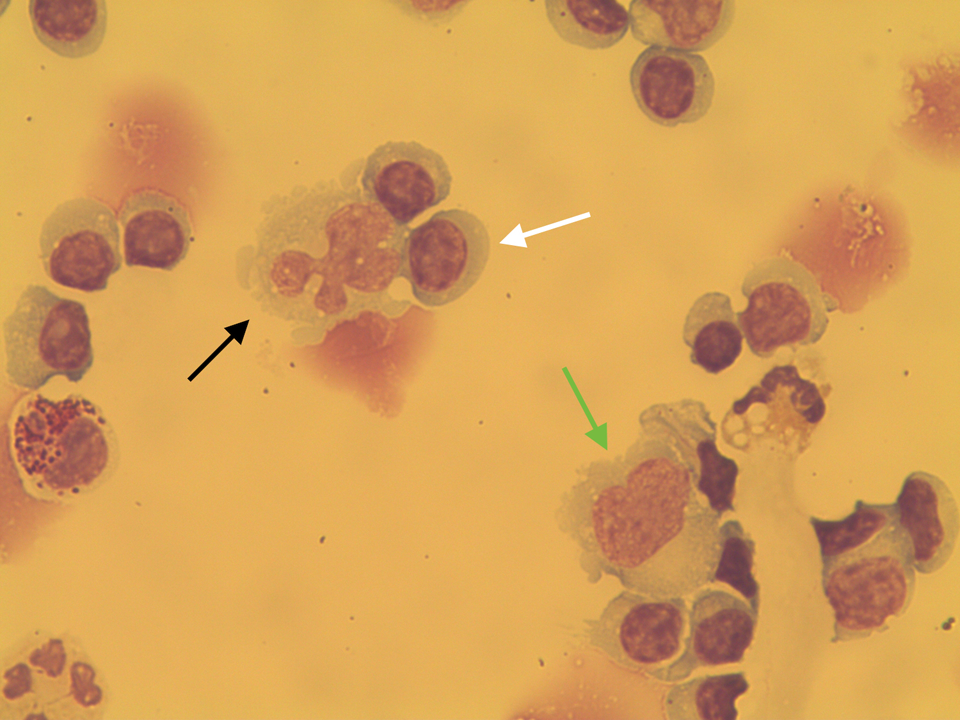
Wright-Giemsa stain of cerebrospinal fluid (CSF) showing a background of lymphocytes (white arrow) with abnormal monocytes typical of Mollaret cells. Mollaret cell with a “clover leaf”–shaped nucleus (black arrow) and “bean”-shaped nucleus with a nuclear cleft (green arrow).
Mollaret cells are activated monocytes with convoluted nuclear lobes and abundant cytoplasm with pseudopods that account for their typical “footprint” or “cloverleaf” shapes. Due to fragility of the nuclear and cytoplasmic membranes in vivo, 1 Mollaret cells are infrequently detected after 24 hours from symptom onset in recurrent benign lymphocytic meningitis attacks. 2 They are encountered in up to 90% of cases of recurrent benign lymphocytic meningitis, or “Mollaret meningitis,” which is strongly linked to HSV-2 reactivation from latent virus in sacral sensory ganglia. 3 However, there are reports of Mollaret cells in meningitis secondary to other herpesviruses (eg, herpes simplex virus 1 (HSV-1), varicella zoster virus (VZV)) and West Nile Virus. 4 In addition to virologic testing, CSF should be reviewed for Mollaret cells when evaluating a case of recurrent aseptic meningitis.
Footnotes
Authors’ Note
Lauren Gluck designed and conceptualized the study, analyzed and interpreted the data, and drafted and revised the manuscript for intellectual content. Matthew Robbins and Benjamin Galen designed and conceptualized the study, analyzed and interpreted the data, and revised the manuscript for intellectual content.
Declaration of Conflicting Interests
The authors declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Matthew Robbins serves on the editorial board for Headache and is a section editor for Current Pain and Headache Reports. He has received book royalties for Headache (Neurology in Practice series) from Wiley.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.