
Abstract

Keywords
A 29-year-old right-handed male presented with the complaint of 4 weeks of progressive left neck swelling and burning sensation, and a large mass was palpable over his left neck. The appearance initially was concerning for scrofula, but the patient’s tuberculosis testing was negative. The mass was markedly pulsatile on physical examination over his carotid artery. He underwent computed tomography angiogram and was found to have a large left internal carotid artery (ICA) pseudoaneurysm eroding into the left jugular vein that is seen in figure 1. The patient underwent a cerebral angiogram to delineate his neurovascular anatomy and obtain a left ICA balloon occlusion test for vessel sacrifice. The left ICA balloon occlusion test was well tolerated by the patient, and he underwent vessel sacrifice of the ICA and proximal carotid using numerous platinum coils to shutdown blood flow to the pseudoaneurysm that is seen in figure 2. After the procedure, more history was obtained that the patient had a history of intravenous (IV) drug use and was suspected to be injecting himself with an IV syringe using his right hand to inject his left neck. On postoperative day 1, he complained of severe left neck pain and burning sensation and increased tightness around the left neck mass. This was followed by sudden hypotension with bradycardia and blurred vision in his left eye. Due to concern about impending catastrophic rupture of the left neck pseudoaneurysm, the patient was taken to the operating room for intraoperative angiogram and left carotid artery exploration and hematoma evacuation. Intraoperative angiogram did not show any flow within the pseudoaneurysm, and intraoperative surgical exploration was performed and revealed an erosive abscess-like cavity around the ICA pseudoaneurysm with adjacent destruction of the internal jugular vein causing compression on the vagus nerve in the neck. Open dissection of the ICA pseudoaneurysm showed platinum coils had inflammatory thrombus irritating the nearby vagus nerve (figure 3). Because of this complex finding, the pseudoaneurysm, left ICA, adjacent necrotic internal jugular vein, and vagus nerve were debrided and proximal left common carotid artery ligated for proximal hemostatic control (figure 4).

Cerebral angiogram image revealing large left carotid artery aneurysm.

Cerebral angiogram image revealing coiling of left carotid artery.
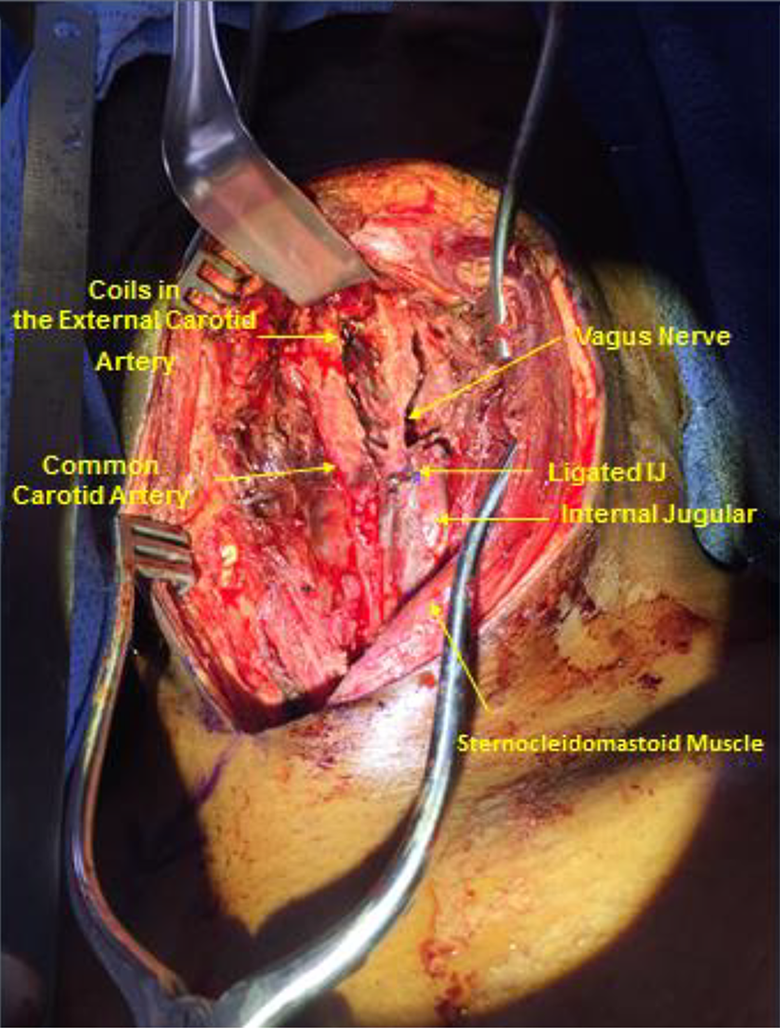
Intraoperative figures delineating carotid anatomy with labeling with relation to carotid sinus and vaso-vagal physiology prior to vascular surgical intervention.
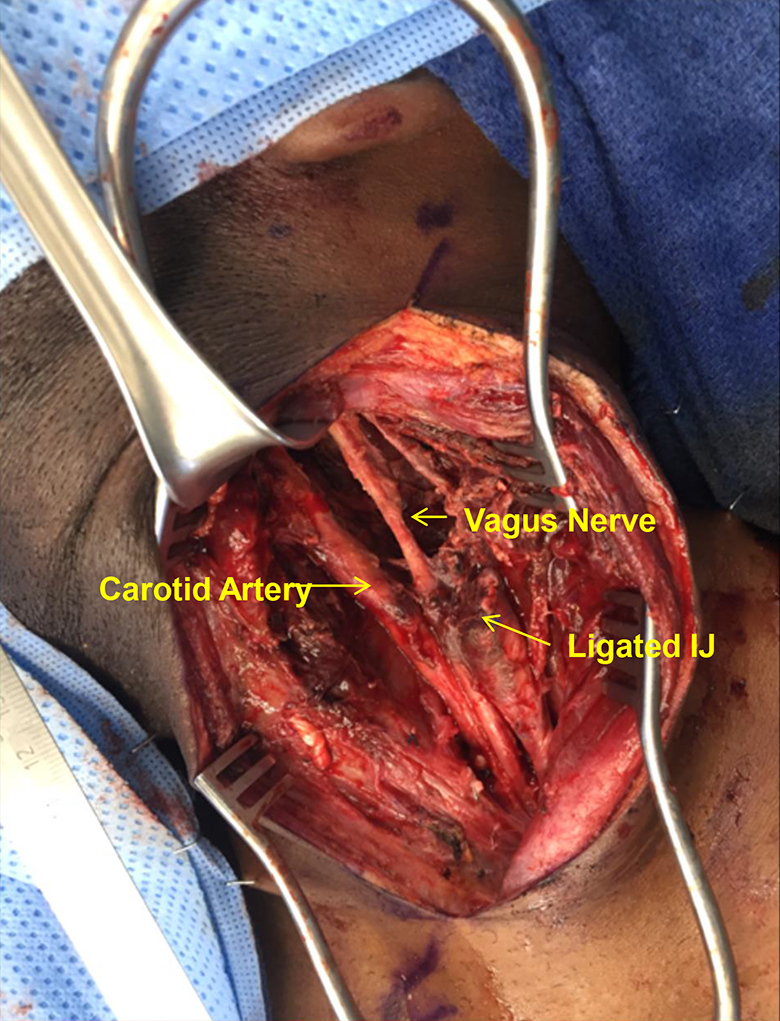
Intraoperative figures delineating carotid anatomy with labeling with relation to carotid sinus and vaso-vagal physiology post debridement.
The term “vasovagal” syncope was originally described by Sir Thomas Lewis in 1932 in the British Medical Journal 1 as the combination of both vasomotor (dilation causing a drop in blood pressure) and vagal nerve influences causing bradycardia causing unresponsiveness due to insufficient cerebral blood flow to the brain. It is critical for neurohospitalists to recognize vasovagal physiology to have a balanced differential diagnosis approach including central nervous system or localized lesions of the carotid sinus or vagus nerve. In this case, the pain and pressure and inflammation from the platinum coils triggered a vasovagal episode leading to acute hypotension and bradycardia. Recognition of vasovagal physiology is key to differentiate mimic conditions associated with syncope including potentially life-threatening such as pulmonary embolism, carotid/vertebral dissection, aortic aneurysm, subclavian steal, and hemorrhagic or ischemic stroke. 2 A systematic approach including a focused history and physical examination is fundamental to the proper diagnosis and management.
Footnotes
Authors’ Note
All authors contributed to the conception, design, image acquisition, and writing of the manuscript. They all had final approval of the submitted manuscript.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.