
Abstract
Background:
The emergence of neurologic symptoms after carotid revascularization is not uncommon and typically caused by perioperative ischemic stroke or hyperperfusion. Postoperative vasculopathy, including reversible cerebral vasoconstriction syndrome (RCVS) is a rare complication of carotid intervention and may be an under-identified cause of neurologic deficit after revascularization. We report a case of reversible postoperative vasculopathy following carotid revascularization as well as its management.
Case Presentation:
A 74 year old right-handed woman presented to the emergency department with sudden onset left arm weakness and episodic shaking while hypotensive. Computed tomography angiography revealed total occlusion of her right internal carotid artery. Transcranial Doppler monitoring demonstrated active embolic events in her right middle cerebral artery raising concern for continued stump embolization. She underwent carotid revascularization with carotid endarterectomy, mechanical thrombectomy, and carotid angioplasty and initially did well postoperatively. On postoperative day 5, she developed a fixed right gaze and left hemiparesis. Computed tomography revealed new right frontal lobe and basal ganglia infarcts, and angiography showed new right internal carotid, middle cerebral, and anterior cerebral artery vasoconstriction consistent with postoperative vasculopathy. Despite treatment with pressure augmentation and vasodilator therapy, her symptoms persisted resulting in left hemiplegia at discharge.
Discussion:
This case highlights postoperative vasculopathy (including RCVS) as a rare potential complication after carotid revascularization that should be considered in a patient with persistent acute neurologic symptoms. Information regarding incidence and predisposing risk factors is limited. Multiple diagnostic and therapeutic modalities may be necessary in the recognition and treatment of postoperative vasculopathy.
Keywords
Introduction
Multiple trials have shown the efficacy of carotid endarterectomy (CEA) and carotid stenting for patients with moderate to severe carotid stenosis in order to decrease the risk of future stroke. 1,2 However, once the carotid artery is completely occluded intervention is rarely performed as the risk of complications is felt to outweigh the benefits, but revascularization may still be considered in specific cases. The emergence of new neurological symptoms is not uncommon after carotid artery surgery, and is frequently caused by perioperative ischemic stroke or cerebral hyperperfusion. Reversible Cerebral Vasoconstriction Syndrome (RCVS) is a rarely reported postoperative complication of carotid revascularization and may be an under-recognized cause of post-procedural neurologic deficits. We report a case of reversible cerebral vasculopathy following carotid endarterectomy and stenting for an occluded carotid artery as well as its management.
Case Description
A 74 year old right handed woman presented to the emergency department with the chief complaint of sudden onset left arm weakness and episodic shaking. Her medical history included polymyalgia rheumatica for which she was on chronic prednisone therapy complicated by adrenal insufficiency. Initial computerized tomography (CT) scan of the brain was unremarkable. CT angiography of the head and neck showed complete occlusion of the right internal carotid artery (ICA) at its origin. Digital subtraction angiography (DSA) confirmed the right ICA occlusion with right anterior circulation supplied by retrograde filling from both the external carotid artery (via the ophthalmic artery) and the vertebrobasilar system (via the right posterior communicating artery) (Figure 1A). Magnetic resonance imaging (MRI) showed a punctate right frontal lobe infarct. Transcranial Doppler (TCD) demonstrated frequent high intensity transient signals in the right middle cerebral artery suggestive of stump emboli. The decision was made to revascularize the patient’s internal carotid artery despite its total occlusion given the high risk of ischemic stroke with active embolism and her symptomatic episodes of weakness during periods of hypotension concerning for ongoing cerebral hypoperfusion. Carotid endarterectomy was initially performed by the neurosurgical team with no antegrade flow despite plaque removal. Next, local angiography and mechanical thrombectomy of the proximal ICA were performed by the endovascular team via direct carotid shuttle, resulting in patent flow (thrombolysis in cerebral infarction [TICI] grade 2C) but with evidence of a distal luminal irregularity. Finally, 2 stents were deployed via femoral access resulting in resolution of this luminal irregularity and angiographic evidence of restoration of flow to the right internal carotid artery (Figure 1B) and patent right anterior and middle cerebral arteries (2A). The total duration of endarterectomy and endovascular procedure was 4 hours. She initially did well after the procedure with a stable neurologic examination with no evidence of a new ischemic event including midline gaze, no visual field deficit, no neglect, and normal left sided strength.
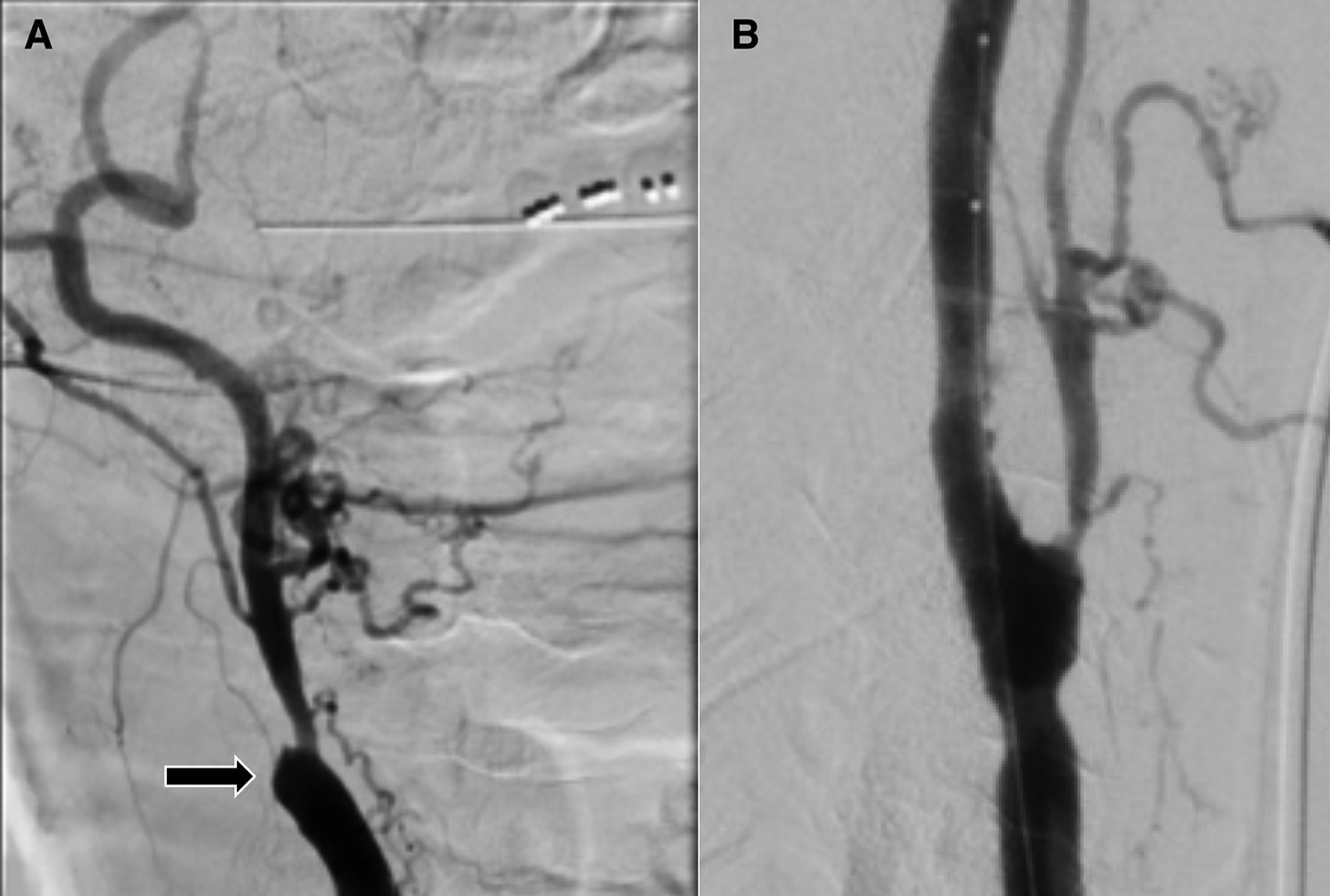
A, Digital subtraction angiography of the right common carotid artery showing complete occlusion of the internal carotid artery (black arrow). B: Digital subtraction angiography of the right common carotid artery immediately after revascularization with carotid endarterectomy, mechanical thrombectomy, and angioplasty with stent deployment.
On postoperative day (POD) 5, she developed acute onset of left sided hemiplegia with right gaze deviation. CT of the brain demonstrated new right frontal and basal ganglia infarction (Figure 2B and D). CT angiography showed patency of the extracranial right internal carotid artery with new right intracranial ICA stenosis. She underwent repeat DSA on POD 7 which demonstrated multifocal ipsilateral vasoconstriction (Figure 2C). Review of the patient’s medications did not reveal any vasoactive medications or antidepressants as potential triggers. She continued to have fluctuating neurological symptoms correlating with periods of hypotension. Her refractory hypotension was felt to be secondary to a combination of adrenal insufficiency (the diagnosis of which was confirmed during her hospitalization based on a low basal cortisol with inadequate response to cosyntropin) and exaggerated baroreceptor reflex after revascularization. Her hypotension was managed with intravenous phenylephrine and milrinone infusions. Oral midodrine, fludrocortisone, and pyridostigmine were also required to treat hypotension. Daily TCD monitoring showed increased right sided velocities consistent with worsening vasoconstriction. She underwent repeat DSA on post-operative day 17 and 21 which showed continued diffuse multifocal right internal carotid territory vasoconstriction that improved with intra-arterial verapamil. Despite blood pressure augmentation and intra-arterial therapy initially improving her symptoms, her left sided weakness progressed and she was hemiplegic at the time of discharge. Follow up at 2 months and 1 year after admission showed interval improvement in her weakness with normalization of her intracranial mean flow velocities on TCD, and she was able to achieve independent ambulation with a walker.
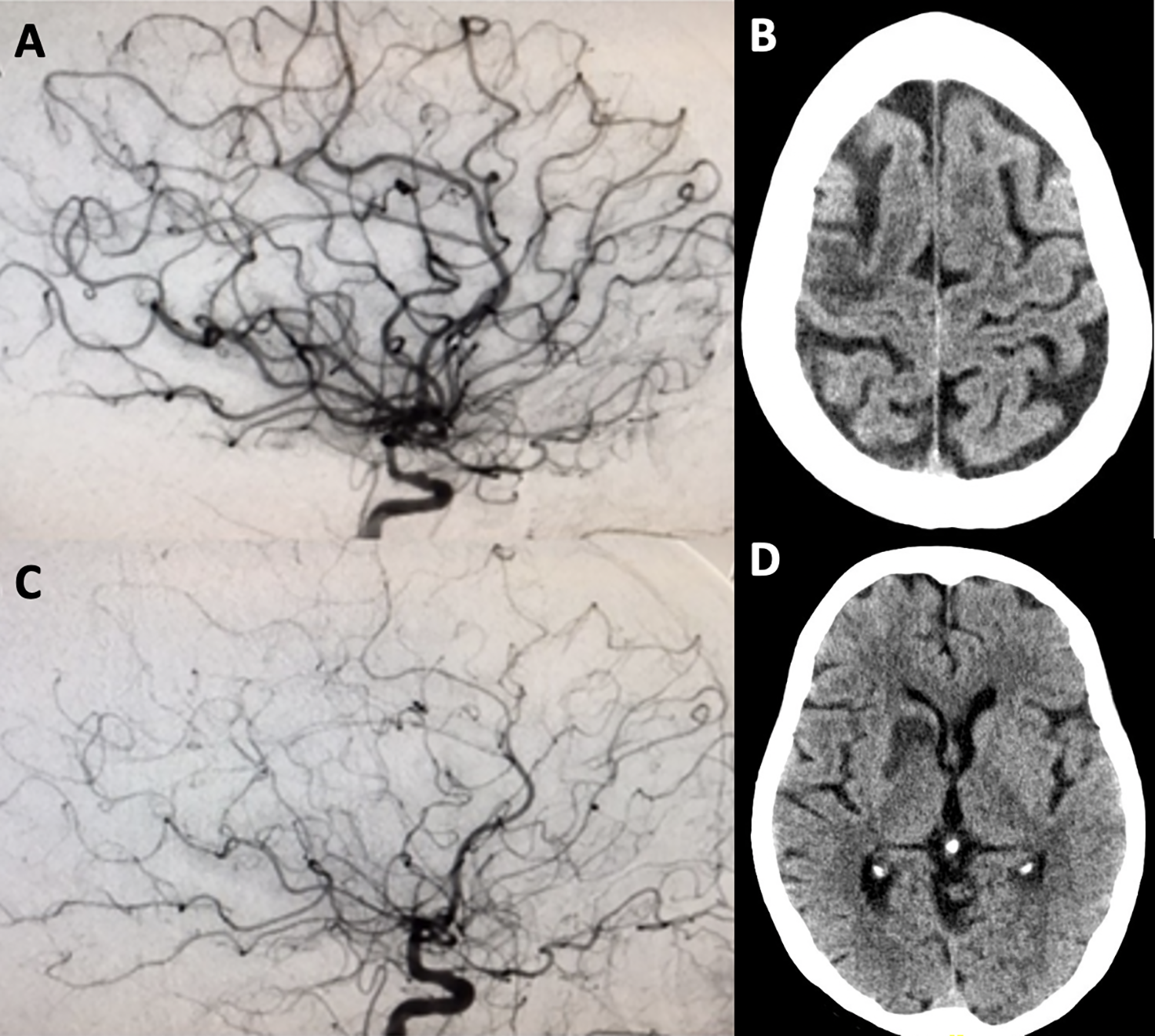
A, Digital subtraction angiography internal carotid artery injection immediately after carotid revascularization showing normal antegrade flow. B, Computed tomography obtained after onset of left hemiplegia demonstrating right frontal ischemic stroke. C, Digital subtraction angiography internal carotid artery injection on postoperative day 7 showing multifocal vasoconstriction in the anterior and middle cerebral arteries. D, Computed tomography obtained after onset of left hemiplegia demonstrating right basal ganglia ischemic stroke.
Discussion
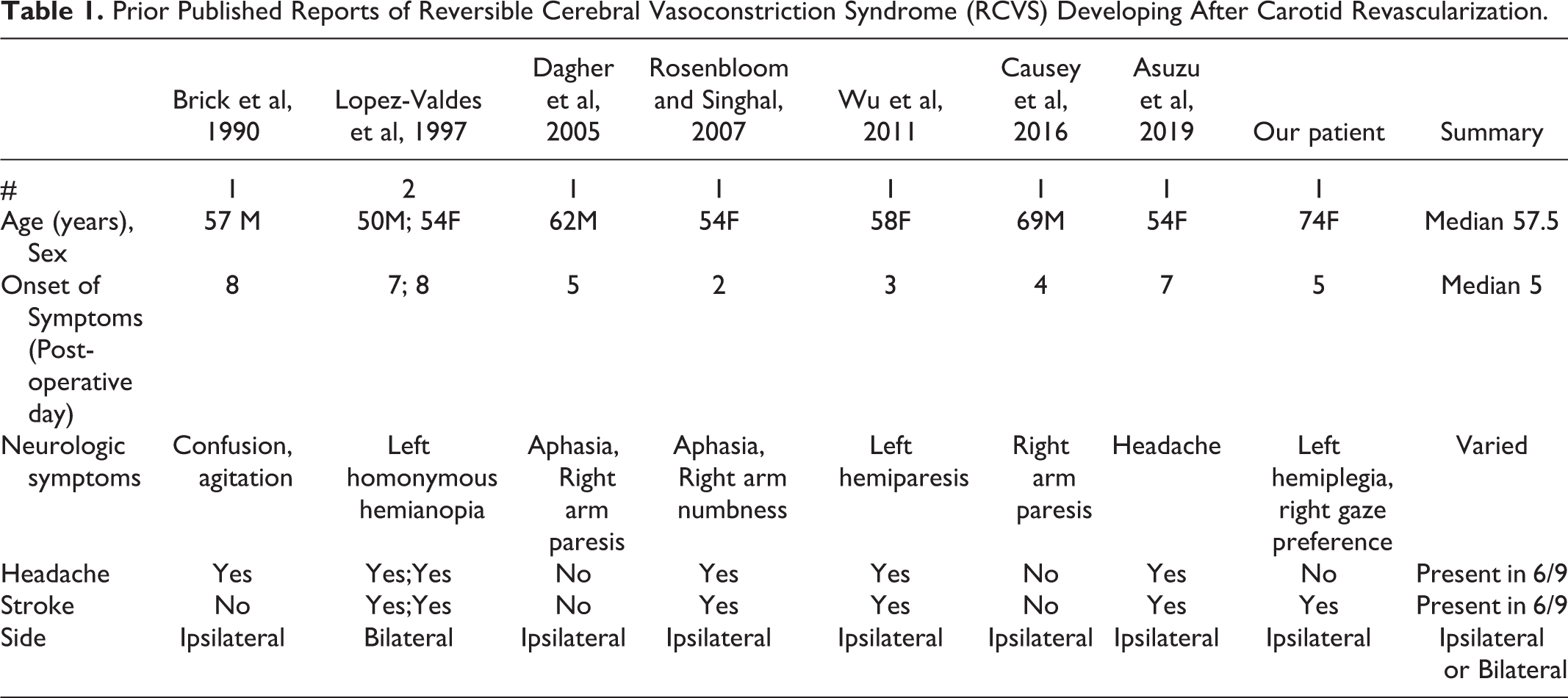
Our case highlights the uncommon complication of reversible cerebral vasculopathy after carotid revascularization, as well as the importance of managing systemic diseases (such as this patient’s adrenal insufficiency) in order to better manage acute neurologic disease. Additionally, multiple imaging modalities may be necessary to diagnose and longitudinally follow this vasculopathy, including transcranial Doppler and cerebral angiography. Previously reported cases of reversible vasculopathy after carotid endarterectomy were diagnosed with RCVS, and characteristics of these cases have been summarized in Table 1. 3 -9 Headache, typically present in RCVS, was the most common presenting symptom but was notably absent in our patient and 2 other previous cases making the diagnosis of RCVS less certain, and classic triggers for RCVS such as vasoconstrictive agents may be absent. Reported cases of post-procedural RCVS have all been either ipsilateral to the revascularized artery or bilateral, and subsequent cerebral infarction in the affected territory is common. The vasculopathy seen in this patient and the previously reported cases of RCVS likely exist along the same spectrum of disease of a procedure-induced reversible vasoconstriction with unclear pathophysiology. Severe stenosis prior to the procedure may lead to chronic cerebral hypoperfusion and disruption of cerebral autoregulation. After the procedure, the relative “hyperperfusion” state may induce accentuated vasoconstriction in affected individuals. This could explain the severity of our patient’s symptoms given her previously completely occluded carotid artery, and provides further evidence against intervention on total carotid artery occlusions. Given its infrequent prevalence, there is no proven medical management for postoperative vasculopathy. Treatments used for RCVS have been tried including calcium channel blockers like nimodipine and verapamil, and intra-arterial calcium channel blockers may also be of transient benefit in refractory cases. 10 Once other therapies have been maximized, intravenous milrinone has shown promising results in managing aneurysmal subarachnoid hemorrhage related vasospasm and may have utility in treating the vasoconstriction seen in this population 11 -13 ; however in our case it was ineffective.
Prior Published Reports of Reversible Cerebral Vasoconstriction Syndrome (RCVS) Developing After Carotid Revascularization.
Conclusion
This case highlights postoperative vasculopathy as a rare cerebrovascular complication in patients who underwent carotid revascularization procedure. Along with the more common perioperative stroke and hyperperfusion syndrome, postoperative vasculopathy including RCVS should be considered in patients with fluctuating neurological symptoms in the perioperative period. In patients presenting with post-procedural vasculopathy, hypotension might worsen the neurological prognosis due to hypoperfusion and necessitates close monitoring in the neurocritical care unit. Pharmacological management with calcium channel blockers may be limited in these patients due to hypotension and the use of blood pressure augmentation may be helpful in stabilizing neurologic symptoms.
Supplemental Material
Supplemental Material, CARE_Checklist_RCVS - Ipsilateral Reversible Cerebral Vasculopathy Secondary to Carotid Artery Revascularization: A Case Report
Supplemental Material, CARE_Checklist_RCVS for Ipsilateral Reversible Cerebral Vasculopathy Secondary to Carotid Artery Revascularization: A Case Report by Aaron Shoskes, Naresh Mullaguri, Meghan Purohit, Pravin George and Christopher Ryan Newey in The Neurohospitalist
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.