
Abstract
We report a case of a woman with a history of systemic lupus erythematosus who developed persistent ataxia and was diagnosis with lupus cerebellitis. Magnetic resonance imaging of the brain showed T2/FLAIR signal hyperintensity within the cerebellar vermis without mass effect. The patient’s condition improved with pulse IV methylprednisolone. This case highlights unique imaging findings within the cerebellum, our diagnostic and treatment regimen, and compares this case to previous literature on similar cases.
Introduction
Systemic lupus erythematosus (SLE) is a well-known systemic autoimmune disease that affects many organ systems through autoantibodies and immune complex formations. SLE may attack the neurologic system, with the prevalence of neuropsychiatric SLE (NPSLE) ranging from 6-12% in the first year of diagnosis and 19-38% overall. 1 Multiple classification criteria for NPSLE exist, and the diagnosis is made based on neurologic manifestations, cerebrospinal fluid (CSF) studies, neuroimaging, and the exclusion of alternate diagnoses including infection, metabolic derangement, and medication adverse effects. While both the peripheral and central nervous systems (CNS) can be affected, CNS involvement makes up the majority of NPSLE manifestations. 2 NPSLE commonly presents with headaches, mood disorders, cognitive dysfunction, acute altered mental status (AMS), psychosis, or stroke. 1 Cerebellar syndromes have been infrequently documented and are less common than cerebral manifestations.3,4 In this report, we describe the case of a 35-year-old female in an active lupus flair who developed AMS and cerebellar ataxia with a corresponding cerebellar lesion concerning for acute lupus cerebellitis.
Case Report
The patient was a 35-year-old woman with a history of SLE on chronic prednisone 10 mg and hydroxychloroquine 400 mg with recurrent truncal ulcerations thought to be attributable to lupus profundus who was initially admitted with a 2-week history of fevers. On admission, she was bicytopenic (hemoglobin 7.6, platelets 73) and had an acute kidney injury (creatinine 1.17 from a baseline of 0.8, normal 0.58-0.96 mg/dL). Given her fevers, an infectious workup was initiated which was unremarkable, with the exception of staphylococcus lugdenensis cultured from a lumbar skin ulcer; this received appropriate antibiotic therapy. The patient was given 2 units of platelets and 3 units of packed red blood cells for her bicytopenia. Hydroxychloroquine was stopped since it was thought to be contributing to her decreased cell counts.
She was transferred to our facility due to gastrointestinal bleed caused by duodenal arteriovenous malformation and hemorrhagic esophagitis. Upon arrival, there was initially a concern for a seizure due to encephalopathy and tremulous movements. Computed tomography of the brain at that time was unremarkable and electroencephalography following the event did not show any epileptiform changes. Her physical examination was notable for discoid lesions, areas of hyperpigmentation, and alopecia on her face and scalp, which according to her family, had been worsening over the past several weeks prior to hospitalization. Her neurologic exam was notable for disorientation and marked vocal, truncal, and limb ataxia with dysmetria. The patient was unable to sit up in bed unassisted or feed herself secondary to her truncal and limb ataxia. Labs at this time were significant for elevated dsDNA antibody (751, normal <30 IU/mL), ANA (1:640, normal <1:80 nucleolar), C reactive protein (4.6, normal <0.9 mg/dL), WSR (68, normal 0-20 mm/Hr), and low complement (C3 76, normal 86-166 mg/dL). Magnetic resonance imaging of the brain was obtained and demonstrated areas of T2/FLAIR signal hyperintensity involving the uvula and ventral pyramids of the cerebellar vermis as well as along the inferior margins of the left cerebellar tonsil and inferior margins of the bilateral cerebellar hemispheres (Figure 1A and B). These regions demonstrated asymmetric linear enhancement along the inferior margins of the cerebellum (Figure 1C and D). There was no significant mass effect or restricted diffusion. MRA showed no apparent intracranial proximal arterial occlusion, abnormalities, or evidence of vasculitis. Additionally, MRI of the spine also showed questionable enhancement of the cauda equina nerve roots.
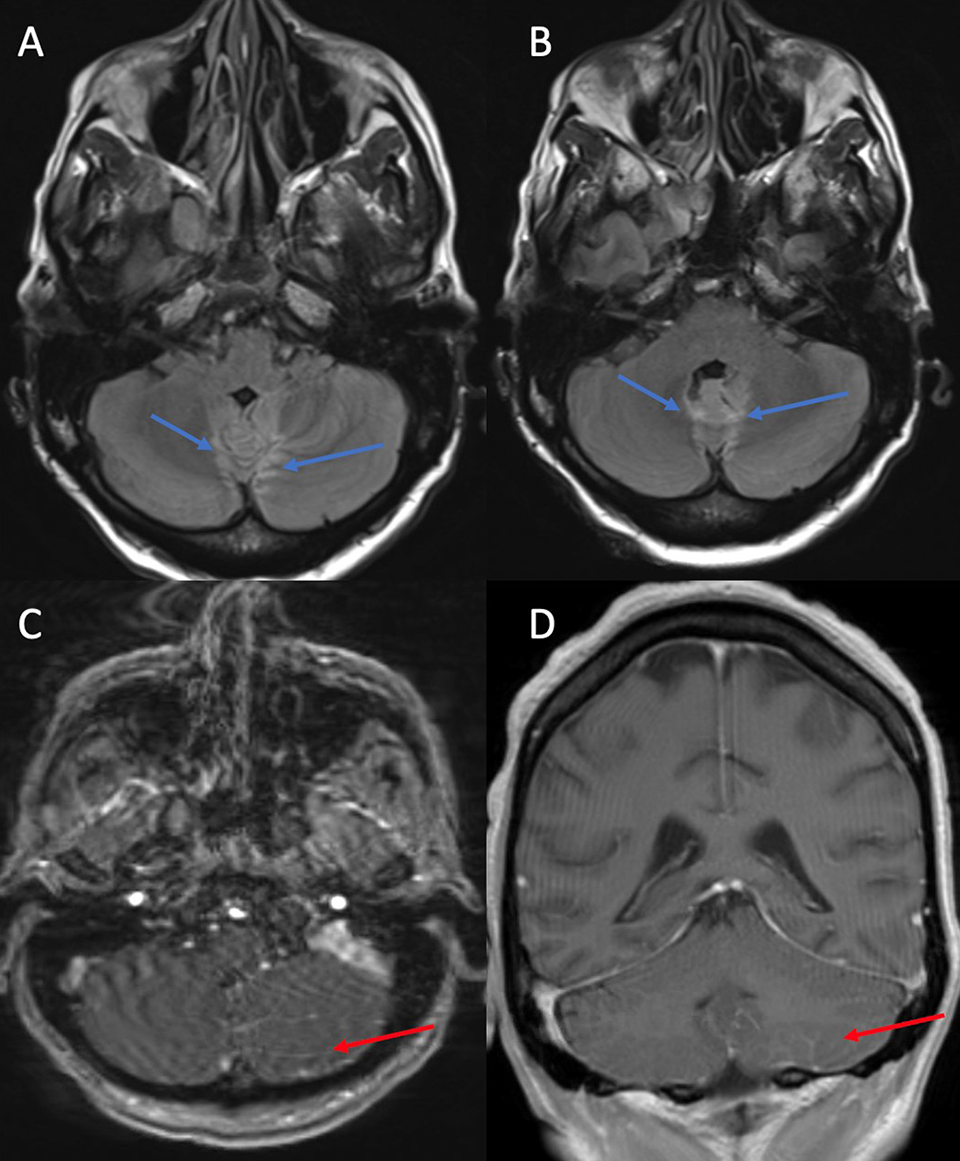
A and B, Magnetic resonance imaging FLAIR sequences of the brain demonstrating bilateral cerebellar uvula and vermis hyperintensities (arrows). C and D, Magnetic resonance imaging Post contrast T1 sequences of the brain demonstrating areas of linear enhancement along the inferior margins of the cerebellum, left (arrows) more so than right.
A lumbar puncture could not be done due to her overlying infected skin ulcers; however, a cervical puncture was performed. Her CSF showed a lymphocytic pleocytosis (white blood cell count 19, normal 0-4 cells/uL), elevated protein 120 mg/dL (normal 15-45 mg/dL), and normal glucose 48 mg/dL (normal 40-70 mg/dL). IgG synthesis index was increased at 1.77 (normal 0-0.61). Multiple CSF studies to evaluate for infection were negative, including culture and gram stain, herpes simplex virus (HSV) 1/2, enterovirus, mycoplasma, varicella zoster virus, West Nile virus, listeria, JC virus, and cytomegalovirus (CMV). A paraneoplastic encephalitis panel, which included Hu, Yo, CV2, Ri, Ma2, and GAD65 antibodies among others, was negative. CSF cytology was also negative for malignant cells. Additional serum infectious workup was negative for HIV, syphilis, rocky mountain spotted fever, typhus, ehrlichiosis, histoplasma, hepatitis, CMV, Lyme disease, and HSV. Given her history of SLE, evidence of active SLE flare, and inflammatory CSF profile without evidence of infection or other auto-immune pathology, lupus cerebellitis was thought to be the most likely cause of her cerebellar lesions. She was started on IV methylprednisolone 1000 mg daily for 3 days followed by an oral prednisone taper. She received further immunosuppression with monthly doses of IV cyclophosphamide 500 mg. Prior to completion of pulse steroids, the patient saw improvements in her mentation and ataxia. The patient was able to work with physical and occupational therapy, demonstrating continued improvement and her family stated that she appeared back to her baseline at the time of discharge. She was continued on maintenance therapy with oral prednisone and monthly cyclophosphamide following discharge.
Discussion
This patient developed acute cerebellar ataxia during her hospital course with findings of cerebellitis on brain MRI. Given the inflammatory nature of her CSF studies, a clinical picture consistent with an active SLE flair, and absence of another etiology, this ataxia was attributed to NPSLE. Isolated cerebellar manifestations of SLE are a rare occurrence. 3 Ahmed et al conducted a literature review in 2017 of cases of NPSLE related cerebellar ataxia. Their search yielded 15 previously reported cases with slightly varying presentations. 4 Cerebellar imaging findings varied greatly during initial presentations and included normal findings, ischemic lesions, T2/FLAIR hyperintensities with vasogenic edema, and atrophy. Some SLE patients presenting with ataxia were found to have deep white matter lesions of the brain and brainstem. In many of these cases, the cerebellar findings on imaging were asymmetric.4-9 Since the review by Ahmed et al, there have been several additional cases reported that continued to have variable imaging findings. Casciato et al reported a case of subacute cerebellar ataxia that showed marked atrophy of the left cerebellar hemisphere and vermis while a case reported by Sy et al showed unremarkable MRI findings.10,11 In our case, MRI showed linear areas of enhancement along the inferior margins of the cerebellum most pronounced on the left with corresponding areas of T2/FLAIR signal hyperintensity involving the uvula and ventral pyramids of the cerebellar vermis without evidence of mass effect. Interestingly there was also enhancement of the cauda equinae nerve roots. To the best of our knowledge, this array of neuroimaging findings has not been previously reported. The inconsistencies in imaging findings in NPSLE related cerebellar ataxia suggests that there may be multiple mechanisms inflicting damage. Previously proposed mechanisms included vascular changes, hypercoagulable states, and autoantibody mediated break down of the blood brain barrier and subsequent CNS inflammation. Of the many different autoantibodies potentially present in SLE, anti-dsDNA has been identified as a likely culprit as it can cross react with NMDA receptors in the brain. 12
In addition to her cerebellar ataxia, this patient also presented with disorientation compared to her baseline. In previously reported cases of lupus associated cerebellar ataxia, mental function was generally preserved.7,10,13 Those cases that did report a change in mental status generally had associated imaging findings. Krief et al. reported a case of unilateral cerebellitis that presented with acute mental status change; image findings in this case showed cerebellar edema with mass effect and cerebellar herniation. 6 Watanabe et al. similarly described a slight alteration in mental status that was associated with imaging findings that showed cerebellar edema. 14 However, Sy et al. reported symptoms include headache, visual hallucinations, and disorientation while having unremarkable MRI findings. 11 In our case, MRI did not provide any definitive cause for our patient’s disorientation. Changes in mood, cognitive dysfunction, and psychosis have all been observed previously in NPSLE. 1 Given this patients extensive workup for other causes of her symptoms, NPSLE remains the most likely cause of her change in mental status despite a lack of explanatory imaging findings.
High doses of steroids followed by a steroid taper with additional immunosuppressive agents like cyclophosphamide or azathioprine were common treatments among previous cases.4-9 This patient showed marked improvement at discharge following a three-day course of pulse methylprednisolone followed by a steroid taper and monthly cyclophosphamide infusions. Most reported cases report marked clinical improvement at follow up. MRIs done at follow up have also shown inconsistent results, with several cases showing cerebellar atrophy or persistent lesions while others show complete resolution.4-9 Another case had recurrence of ataxia at a later date with a reappearance of his previous lesion on MRI. 5 This suggests some degree of persistent damage or susceptibility to repeat attack even in the case of previous resolution. Follow up studies to look at the long term structural changes of the cerebellum after SLE cerebellitis are warranted.
Conclusion
Cerebellar ataxia is a rare manifestation of NPSLE. Corresponding imaging findings on MRI are variable and show inconsistent involvement of the cerebellum, suggesting a combination of inflammatory mechanisms. Extra-cerebellar lesions occur frequently and may include deep white matter, brainstem, or even spinal nerve roots. Prompt treatment with pulse methylprednisolone or high dose prednisone can markedly improve the patient’s symptoms and may potentially reverse lesions found on imaging.
Footnotes
Authors’ Note
Verbal informed consent for publication of this clinical case and images were obtained from the patient.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.