
Abstract
Introduction:
Seizures are a common complication after an ischemic stroke. Electroencephalography can assist with the diagnosis of seizures however, the diagnostic yield of its use when seizure is suspected in the setting of acute ischemic stroke is unknown. We aim to evaluate the yield and cost of EEG in the acute ischemic stroke setting.
Methods:
We conducted a retrospective chart review of patients admitted to a single academic tertiary care center in the United States between September 1, 2015 to November 30, 2019 with a primary diagnosis of acute ischemic stroke and who were monitored on electroencephalography (EEG) for suspected seizures (total number of 70 patients). The primary outcome was how often EEG monitoring changed clinical management defined as starting, stopping, or changing the dose of an anti-epileptic drug. Secondary analysis was estimating the cost of EEG monitoring per change in management.
Results:
We identified 126 patients admitted with acute ischemic stroke who underwent EEG of which 70 met all inclusion and exclusion criteria. EEG monitoring resulted in a change in management in 22 patients (31%). Predictors associated with EEG monitoring resulting in a change in management were admission to the ICU, pre-existing atrial fibrillation, and symptomatic hemorrhagic transformation. Estimated cost of EEG per change in management was $1374.96 USD.
Conclusion:
EEG monitoring resulted in a changed management in nearly one-third of patients admitted with acute ischemic stroke suspected of having seizures.
Keywords
Introduction
Stroke is the most common cause of epilepsy in the older adult. 1 The reported incidence of seizures after ischemic stroke ranges widely depending on the population, length of study, and definition of seizure and stroke applied. Seizures can be an early manifestation of an acute stroke occurring within the first 2 weeks; whereas late seizures are considered to be >14 days. The largest meta-analysis to date estimates a 3% rate of early post-ischemic stroke seizures. 2 The use of continuous EEG monitoring to help aide in the detection and diagnosis of both clinical and subclinical seizures in the inpatient setting has become more widespread over the last few decades. 3 Although seizures are common after stroke, indications for if, and when, to obtain EEG monitoring remain unclear. Indeed, factors associated with greater likelihood of seizure development such as clinical severity, size of infarction, and infarct topography may be useful to consider when considering EEG monitoring for suspected seizures. 4
Congruent with the clinical morbidity of stroke, the financial burden from stroke in the United States is also high. One study estimated the average cost of hospitalization for acute ischemic stroke in the United States to be close to $20,000 USD. 5 The cost of a routine awake EEG (CPT 95816) and a 24-hour continuous EEG (CPT 95951) monitor in the inpatient setting is $370.12 and $329.40, respectively based on the CY 2019 Medicare Physician Fee Schedule and inclusive of professional and technical components. 6 Identifying unnecessary testing and utilization of healthcare resources is paramount in the effort to contain costs. In this study, we examine the diagnostic yield of EEG monitoring during hospitalization for acute ischemic stroke in a real-world setting.
Methods
We performed a retrospective chart review to evaluate the diagnostic yield of EEG in patients hospitalized with an acute ischemic stroke. The study was approved by our local Institutional Review Board (NCR202569) prior to initiation of data collection. Patients admitted to our academic tertiary care center, between September 1, 2015 to November 30, 2019, with a primary diagnosis of acute ischemic stroke (ICD-10 I63) and undergoing EEG monitoring (ICD-10 Procedure 4A10X4Z) were identified in our institution’s administrative database. 7 For context, our hospital has both a Comprehensive Stroke and Level 4 Epilepsy Center designation.
Patients had to be 18 years or older. The time from onset of stroke symptoms to initiation of EEG monitoring had to be >14 days. Patients with a history of epilepsy were excluded. Seizure determination was based on chart documentation of an episode consistent with a clinical seizure and/or electrographic evidence of a seizure on EEG. All EEGs were read by board certified epileptologists.
Baseline and clinical variables collected from chart review included age, sex, history of atrial fibrillation, prior ischemic stroke, initial National Institute of Health Stroke Score (NIHSS), treatment with intravenous recombinant tissue plasminogen activator (IV rt-Pa), symptomatic hemorrhagic conversion, treatment with mechanical thrombectomy, post-procedure Thrombolysis in Cerebral Infarction (TICI) grade, treatment with decompressive hemicraniectomy, hospital location (e.g. stroke unit, ICU) during EEG monitoring, and length of stay.
Neuroimaging including MRI and/or CT were reviewed and acute infarction location was classified as either cortical or non-cortical involvement. EEG and seizure variables included EEG findings (normal vs abnormal, with abnormal EEG further classified into epileptiform potentials, diffuse slowing, focal slowing and electrographic seizures), seizure type (clinical, electrographic vs both), clinical decision based on EEG findings (AED added, AED discontinued, AED dose change, AED not started), and type of EEG (continuous or routine). EEG was further sub-classified based on billing type (Routine awake and Prolonged EEG). The total number of 24-hour segments monitored on prolonged EEG were noted.
The primary analysis was how often EEG monitoring changed clinical management defined as either stopping, starting, or changing the dose of an anti-epileptic drug. Secondary analysis was evaluating cost per change in management of EEG monitoring during hospitalization of acute ischemic stroke. The professional fees estimate for EEG monitoring were calculated using the CY 2019 Medicare Physician Fee schedule value for a routine awake EEG (CPT 95816) and a prolonged EEG (CPT 95951), $370.12 and $329.40, respectively. 6 The cost per change in management was calculated by “average cost” divided by the yield percentage.
Descriptive statistics were used to analyze patient characteristics. Two-tailed unpaired t tests were used to compare continuous variables, and Mann Whitney U test and χ2 tests were used for non-continuous variables. All statistical analyses were performed using SAS 9.4 version.
Results
A total of 126 patients admitted with acute ischemic stroke who underwent EEG monitoring were identified. After chart review 56 patients (27 with no clinical or imaging evidence of stroke, 26 with an alternate diagnosis, and 4 with prior diagnosis of seizures) were excluded leaving 70 patients for the final analysis (Figure 1).
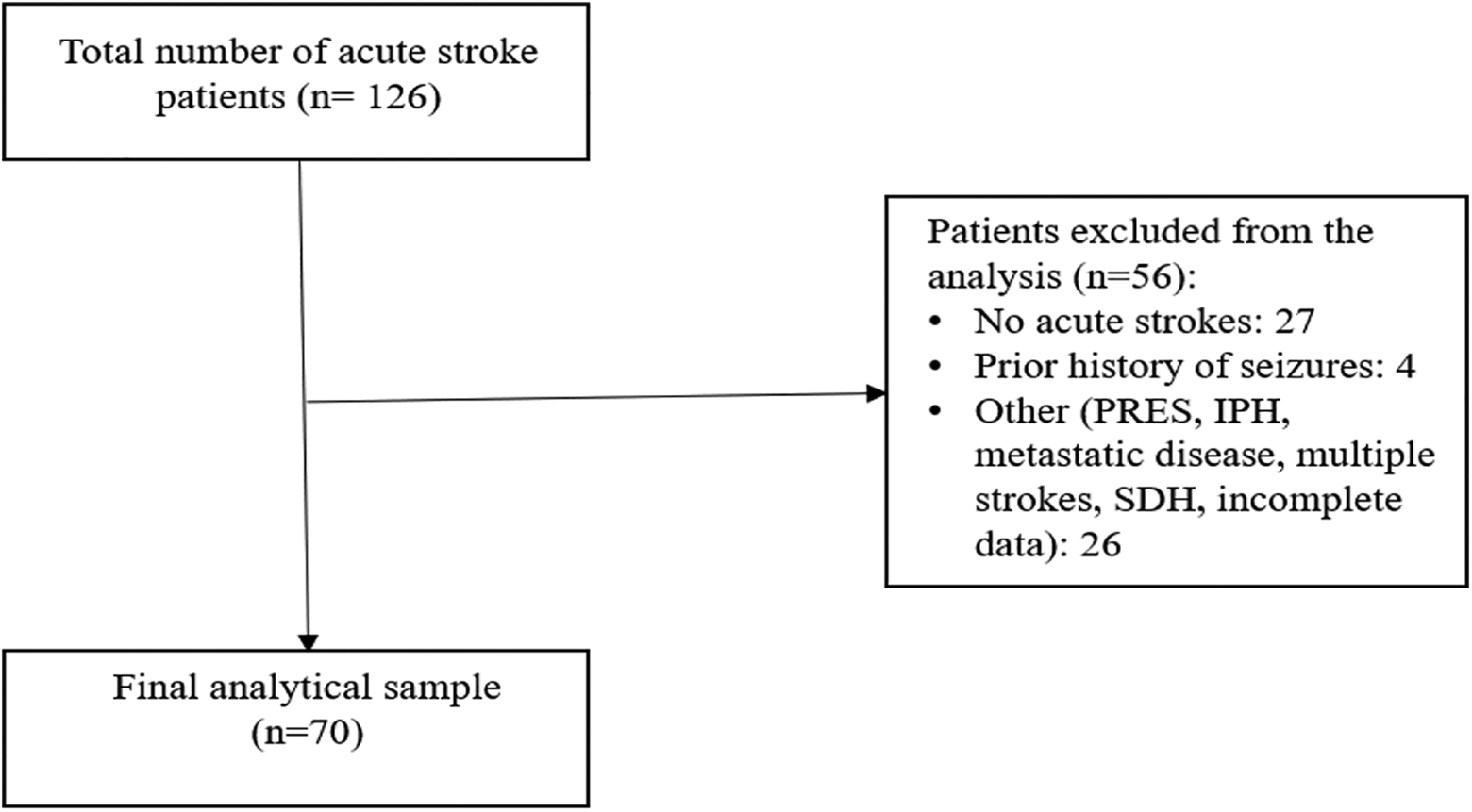
Derivation of the final analytical sample of acute ischemic stroke patients with prolonged EEG monitoring.
Demographic, clinical, and hospitalization characteristics of ischemic stroke patients are summarized in (Table 1).
Demographics, Clinical Characteristics, Stroke Treatment, and Imaging Findings (n = 70).
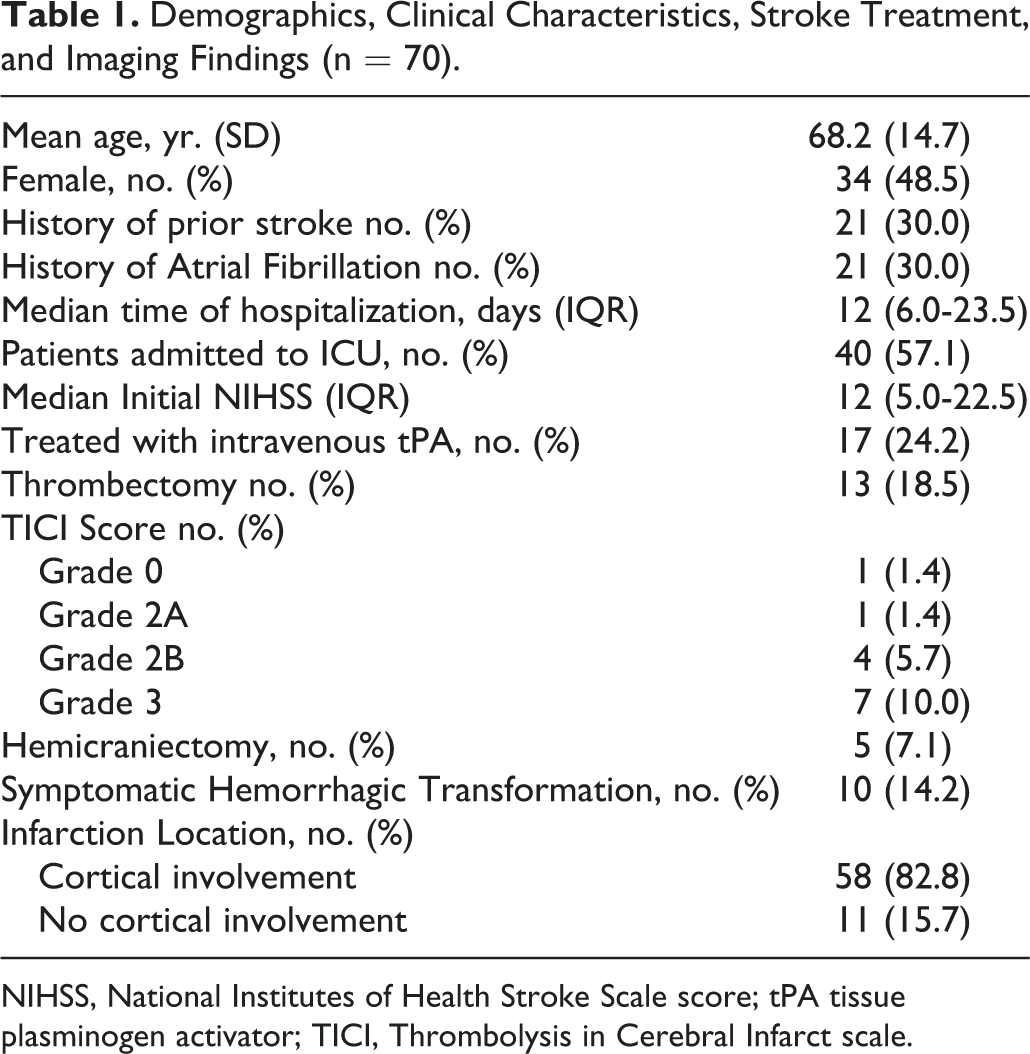
NIHSS, National Institutes of Health Stroke Scale score; tPA tissue plasminogen activator; TICI, Thrombolysis in Cerebral Infarct scale.
Mean age was 68 years with 34 females (48.5%). Median hospital stay was 12 days with the majority (57%) of admissions to the critical care unit. Median initial NIHSS was 12 (IQR 5-22.5), 17 patients (24%) were treated with IV rt-Pa, and 13 (18.5%) underwent mechanical thrombectomy. Cortical involvement was noted in 58 (83%) patients and 10 patients (14%) had symptomatic hemorrhagic transformation.
Continuous video EEG was used more frequently for monitoring compared to routine video EEG with 32.8% patients monitored for 26 hours or longer. An abnormality on EEG was detected in 66 (94%) patients with focal slowing (44.3%) being the most common finding. Seven patients (10%) were found to have non-convulsive seizures (NCS), 3 (4%) had clinical seizures and 1 (1.4%) had both NCS and clinical seizures. EEG results changed management in 22 patients (31%) with change in dosage of AED being most common (10 patients) followed by discontinuation of AED (7 patients) (Table 2).
Seizure Type, Electroencephalogram Findings, and Seizure Management (n = 70).
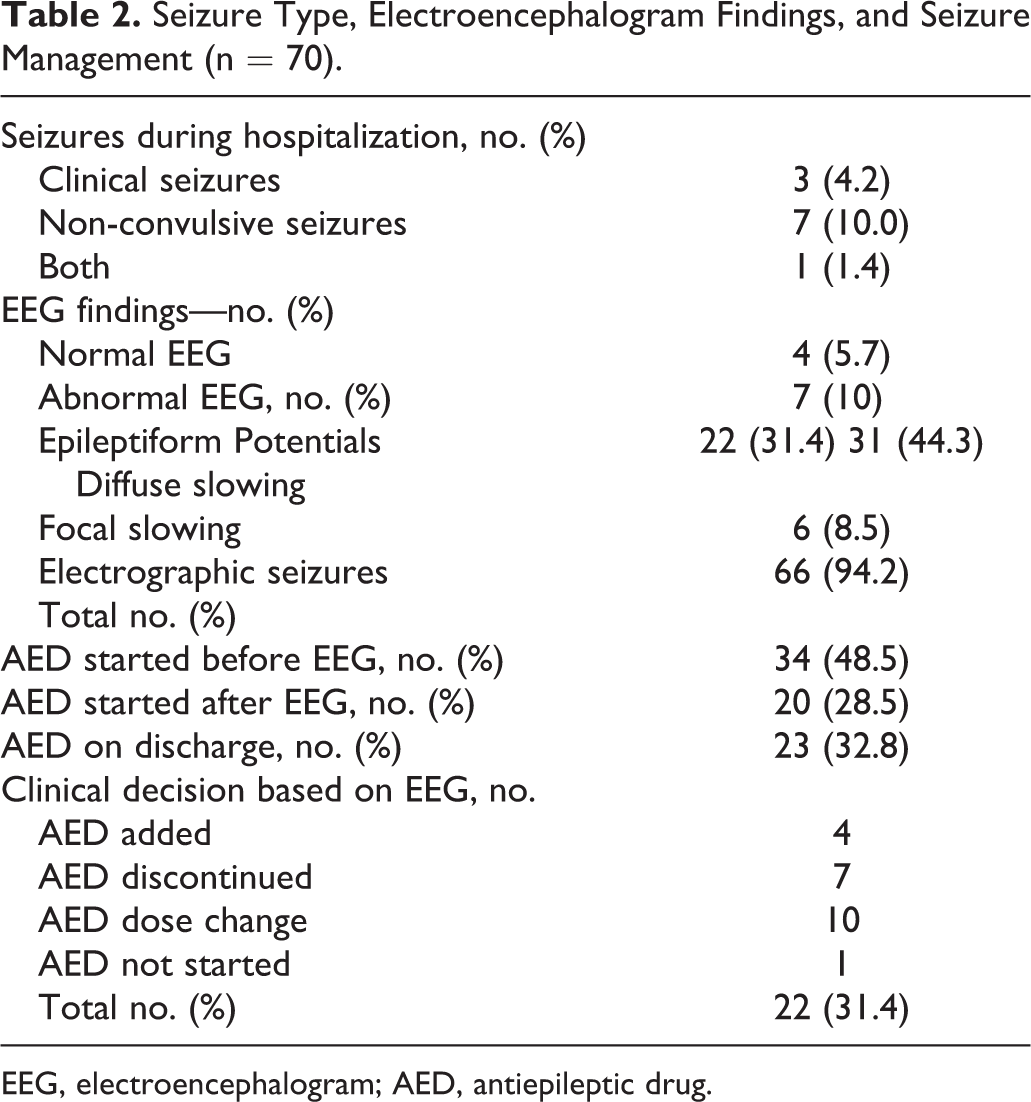
EEG, electroencephalogram; AED, antiepileptic drug.
Patients who had a change in clinical management based on EEG were more often admitted to critical care (72.7% vs 39.5%; p = 0.01), more likely had pre-existing atrial fibrillation (50% vs 16.6%; p = 0.003) and more often underwent symptomatic hemorrhagic transformation (31.8% vs 4.1%; p = 0.001) compared to those who did not have a change in management. Patients who had a change in clinical management based on EEG also had a trend toward higher initial NIHSS (15 vs 10), tPA treatment (31.8% vs 14.5%), and cortical involvement of infarction (95.4% vs 83.3%) compared to Group B without attaining statistical significance (Table 3).
Comparison of Patients With and Without a Change in Clinical Management Based on Electroencephalogram.
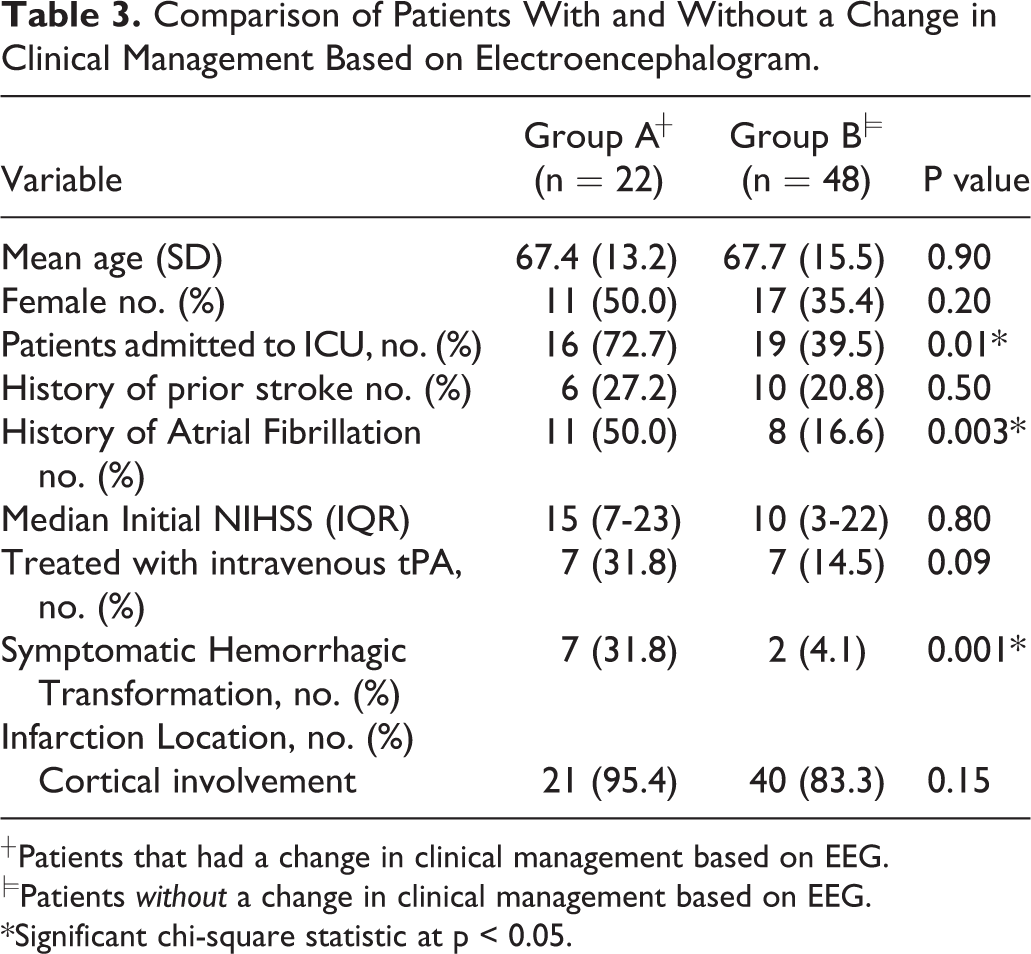
*Significant chi-square statistic at p < 0.05.
A total of 31 routine EEGs and 57 24-hour segments of prolonged EEG were obtained. The sum of the total cost of EEG studies was $30, 249.52 and a calculated cost per change in management of $1374.96.
Discussion
In this study, we evaluated the diagnostic utility of EEG in suspected seizure in individuals admitted with an acute ischemic stroke at an academic Level 4 Epilepsy and Comprehensive Stroke Center. We observed a change in management as a result of the EEG findings in 31% of cases.
The patients that EEG changed management were more likely to be admitted to the ICU, have pre-existing atrial fibrillation, and have a higher rate of symptomatic hemorrhagic transformation. Furthermore, there was a non-statistically significant trend toward higher initial NIHSS, remote history of stroke, and cortical involvement of infarct in this group in patients that EEG changed management. Interpreting these observations, EEG seems to have the greatest diagnostic yield in more severe ischemic strokes and medically complicated cases of acute ischemic stroke. Indeed, our findings align with previous studies. For example, stroke severity has been observed as a predictor for development of post-stroke seizures. 8 Additionally, atrial fibrillation, larger infarct volume, and cortical involvement have been shown to be predictors of developing subsequent late seizures and epilepsy. 4
Nearly all patients had an abnormal finding on EEG and, as expected, focal slowing followed by diffuse slowing were the most common findings observed. Perhaps most important when deciding to initiate an AED, we observed electrographic seizures in 8.5% and epileptiform potentials in 10%. In contrast, we observed a normal EEG in 5.7% of patients which is perhaps most important when stopping an AED. We observed clinical and/or subclinical seizures in 15.6% of patients. The rate of early post-stroke seizures we observed in our population was slightly higher compared to a prior study conducted at a large academic center study examining a general inpatient population (excluding ICU patients), undergoing EEG, 7.4%. 9
In an era of increasing emphasis on healthcare cost containment, the expense of EEG monitoring in the setting of acute ischemic stroke is not trivial. In our study, we estimated an overall cost of $1374.96 per change in management. Relative to the average estimated cost of $20,000 USD per stroke hospitalization, 5 as well as the potential morbidity in missing a seizure, the cost per change in management arguably appears favorable. Furthermore, the utilization of EEG in the setting of acute stroke when seizure is suspected, may lead to a reduction in individual and overall healthcare costs by potentially reducing adverse side effects and complications related to unnecessary anti-epileptic drugs in patients without seizures and by reducing subsequent work-up needed to clarify the diagnosis.
A major limitation of the study is its retrospective design, and variations in individual practice and threshold for obtaining an EEG, likely results in sampling bias limiting the generalizability of our findings. At least 1 previous prospective study examining consecutive patients hospitalized with anterior circulation ischemic strokes monitored with serial EEG’s found a 17.9% occurrence of epileptiform activity. 10 It is conceivable EEG testing may have been underutilized at our center, resulting in a falsely elevated diagnostic yield, since only patients suspected of seizures were monitored. Nevertheless, our study likely better estimates diagnostic yield of EEG in a real-world setting.
Additionally, reliance on administrative data to identify patient with acute ischemic stroke and undergoing EEG monitoring may have resulted in incomplete sampling from coding bias. Nevertheless, stroke ICD9/10 codes seem to be relatively reliable with sensitivity and specificity greater than 80%. 11
Lastly, accurately measuring actual expenses related to EEG monitoring is difficult and using Medicare reimbursement values may underestimate costs depending on payer mix. Additionally, recent changes in 2020 for Medicare reimbursement and coding for EEG may result in inaccurate cost estimates; however, most likely the cost per change in management would be lower given the overall reduction in reimbursement from the recent changes in Medicare. Future studies using larger, multicenter cohorts are needed to improve the generalizability of our observations. Additionally, studies designed to assess the impact of EEG monitoring in acute stroke when seizure is suspected on hospital length of stay, functional and clinical outcomes, mortality, and readmission rates would be useful.
Conclusion
We observed a change in management in nearly one-third of patients admitted with acute ischemic stroke suspected of having seizures undergoing EEG monitoring. The cost to change in management is relatively low.
Footnotes
Authors’ Note
Mohanad AlGaeed: Literature review, manuscript writing, concept analysis.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.