
Abstract
Background:
Treatment with aspirin plus clopidogrel, dual antiplatelet therapy (DAPT), within 24 hours of high-risk transient ischemic attack (TIA) or minor stroke symptoms to eligible patients is recommended by national guidelines. Whether or not this treatment has been adopted by emergency medicine (EM) physicians is uncertain.
Methods:
We conducted an online survey of EM physicians in the United States. The survey consisted of 13 multiple choice questions regarding physician characteristics, practice settings, and usual approach to TIA and minor stroke treatment. We report participant characteristics and use chi-squared tests to compare between groups.
Results:
We included 162 participants in the final study analysis. 103 participants (64%) were in practice for >5 years and 96 (59%) were at nonacademic centers; all were EM board-certified or board-eligible. Only 9 (6%) participants reported that they would start DAPT for minor stroke and 8 (5%) reported that they would start DAPT after high-risk TIA. Aspirin alone was the selected treatment by 81 (50%) participants for minor stroke patients who presented within 24 hours of symptom onset and were not candidates for thrombolysis. For minor stroke, 69 (43%) participants indicated that they would defer medical management to consultants or another team. Similarly, 75 (46%) of participants chose aspirin alone to treat high-risk TIA; 74 (46%) reported they would defer medical management after TIA to consultants or another team.
Conclusion:
In a survey of EM physicians, we found that the reported rate of DAPT treatment for eligible patients with high-risk TIA and minor stroke was low.
Introduction
Patients with minor acute ischemic stroke and transient ischemic attack (TIA) are at increased short-term risk of stroke.1,2 Two randomized control trials have demonstrated that short-term treatment of high-risk TIA (ABCD2 score ≥4) and minor ischemic stroke (NIHSS ≤ 3) patients with aspirin plus clopidogrel, dual antiplatelet therapy (DAPT), within 24 hours of symptom onset reduces the relative risk of subsequent stroke by nearly 30% as compared to aspirin monotherapy.3-5 Treatment of high-risk TIA and minor stroke patients within 24 hours of symptom onset with aspirin plus clopidogrel for 21 days was first mentioned in American Heart Association/American Stroke Association (AHA/ASA) guidelines in 2014 and is now a strongly recommended treatment.6-8 Similarly, administering aspirin plus clopidogrel to high-risk TIA and minor stroke patients within 24 hours of symptom onset has a strong recommendation from The BMJ and a number of international best-practice guidelines.9-11
Unfortunately, delays in translating evidence-based practices into routine clinical care are often substantial and represent a significant public health problem in many areas of medicine.12,13 The rapid pace of practice-changing evidence in emergency medicine (EM) poses unique challenges to the implementation and dissemination of best practices.14,15 How EM physicians currently evaluate and treat high-risk TIA and minor stroke patients given the aforementioned recent evidence and guideline recommendations in support of DAPT is unknown. Understanding front-line physicians’ treatment patterns for TIA and minor stroke patients is an essential first step to assess the need for additional implementation research in TIA/minor stroke management. 16 We therefore sought to evaluate how EM physicians in practice across the United States (US) treat TIA/minor stroke. We hypothesized that physicians working at academic centers and having been in practice for less than 6 years would be more likely to treat eligible TIA/minor stroke patients with DAPT than other physicians.
Methods
Design
We designed an anonymous online survey targeted toward EM physicians. The survey questions were developed iteratively by vascular neurologists (ALL & NTC), a neurology trainee (ARL), as well as 2 EM physicians (BWF & NLK). Prior to final survey publication, additional feedback was supplied by a content expert with extensive experience in mixed-methods research (SP). The final survey instrument consisted of 13 multiple-choice questions regarding participant characteristics, practice settings, and approach to TIA/minor stroke evaluation and treatment (Supplemental Materials). We focused on antiplatelet treatment preferences as well as the use of the ABCD2 score in clinical practice. We intentionally kept the length of our survey short to encourage study enrollment and survey completion by busy clinicians.
All study data were collected and managed using the Research Electronic Data Capture (REDCap) electronic data capture tools hosted at Albert Einstein College of Medicine. REDCap is a secure, web-based software platform designed to support data capture for research studies, which allows for full audit trails for tracking data manipulation and export procedures.17,18 Study data was analyzed only after the survey was closed for participation. De-identified data may be shared upon reasonable request to the corresponding author.
Population
We sought to enroll EM physicians in a variety of practice settings across the US. The survey was circulated exclusively in 2 closed online social media groups for EM physicians (“Emergency Physician Forum” and “EM Docs”). Permission was granted from each groups’ founder/moderator prior to posting the study invitation which included a brief introduction to the survey followed by a hyperlink. The survey hyperlink was accessible from November 2020 until February 2021. Selecting to participate in the study by clicking on the survey hyperlink implied study consent. Once the survey was accessed, participants were asked to complete the survey only one time and assured anonymity (Supplemental Materials). Study participants were not incentivized or compensated. The email address of the primary investigator (ALL) was provided to anyone who began the online survey for questions or comments. The Albert Einstein School of Medicine and Montefiore Medical Center institutional review board approved this study.
Statistical Analysis
We used standard descriptive statistics to characterize study participants, their practice contexts, and additional responses to survey questions. We used chi-squared tests to evaluate whether years of experience or practicing at an academic center was associated with treating either minor stroke or high-risk TIA patients with DAPT. The threshold for statistical significance was set as <0.05 and all tests of comparison were 2-sided. Analyses were performed using Stata/IC, version 16.
Results
A total of 170 EM physicians accessed the online survey. We excluded 7 individuals who reported practicing outside of the US and 1 person who did not complete the entire survey. Thus, 162 participants were included in the final study analysis. One hundred and three participants (64%) reported being in practice for more than 5 years, 129 (80%) were board certified in EM and the remainder of participants, 33 (20%), were board-eligible in EM. Sixty-two (38%) participants were in practice at academic centers and 96 (59%) at non-academic centers. Participants reported practicing across all major US regions with the largest proportion, 62 (38%), in the Northeast (Table 1).
Participants and Practice Characteristics (N = 162).
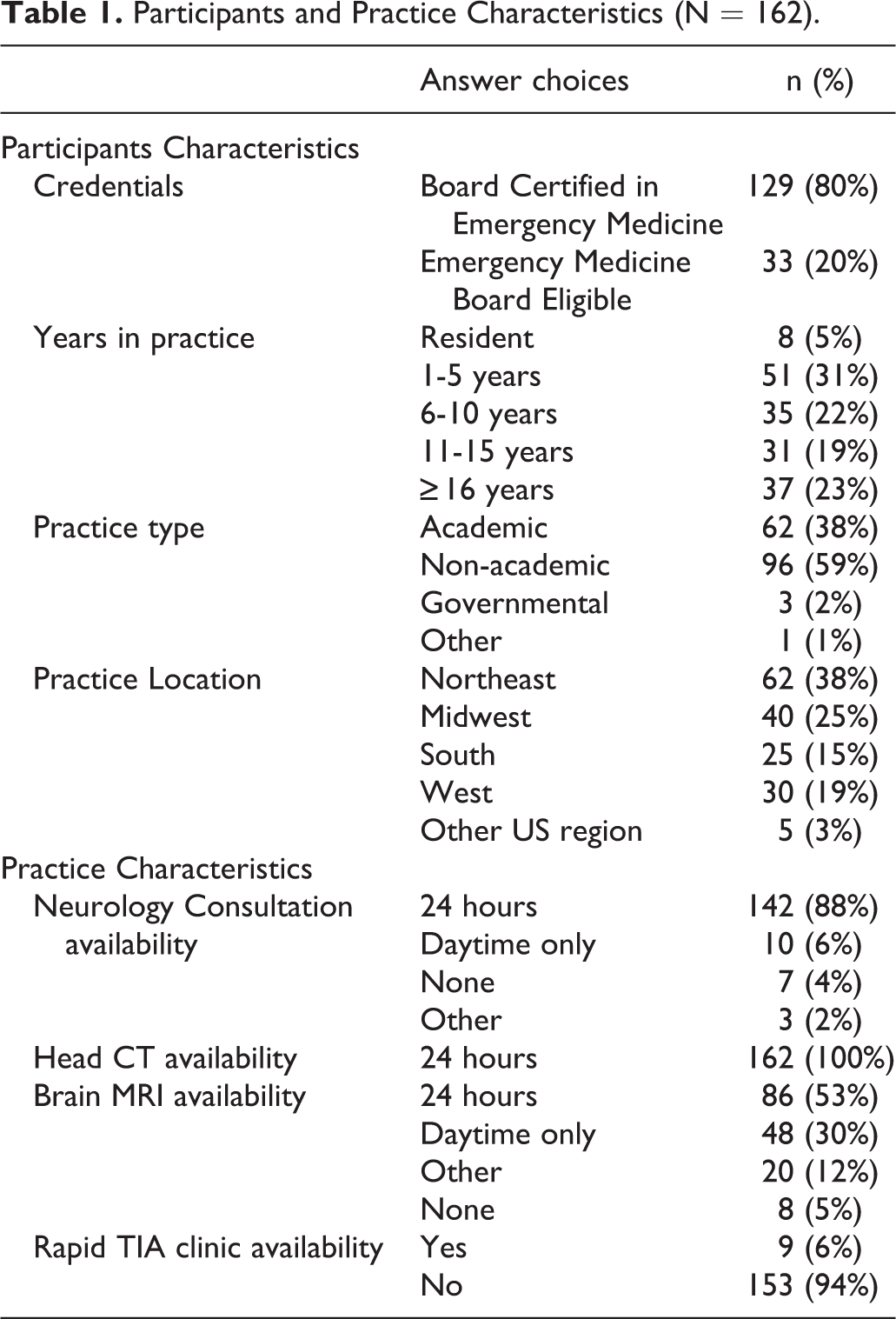
All participants reported full-time access to head CT, 142 (88%) of participants reported full-time access to neurology consultation, and 86 (53%) reported full-time access to brain MRI. Only 9 (6%) participants indicated that they have rapid-access TIA clinics (Table 1).
One-hundred and ten (68%) participants reported not using any clinical prediction rules for TIA. The ABCD2 score was only used by 56 (35%) participants in clinical practice and only 29 (18%) reported using the ABCD2 score to inform medication choices for TIA patients (Table 2).
Evaluation and Treatment of TIA and Minor Stroke (N = 162).
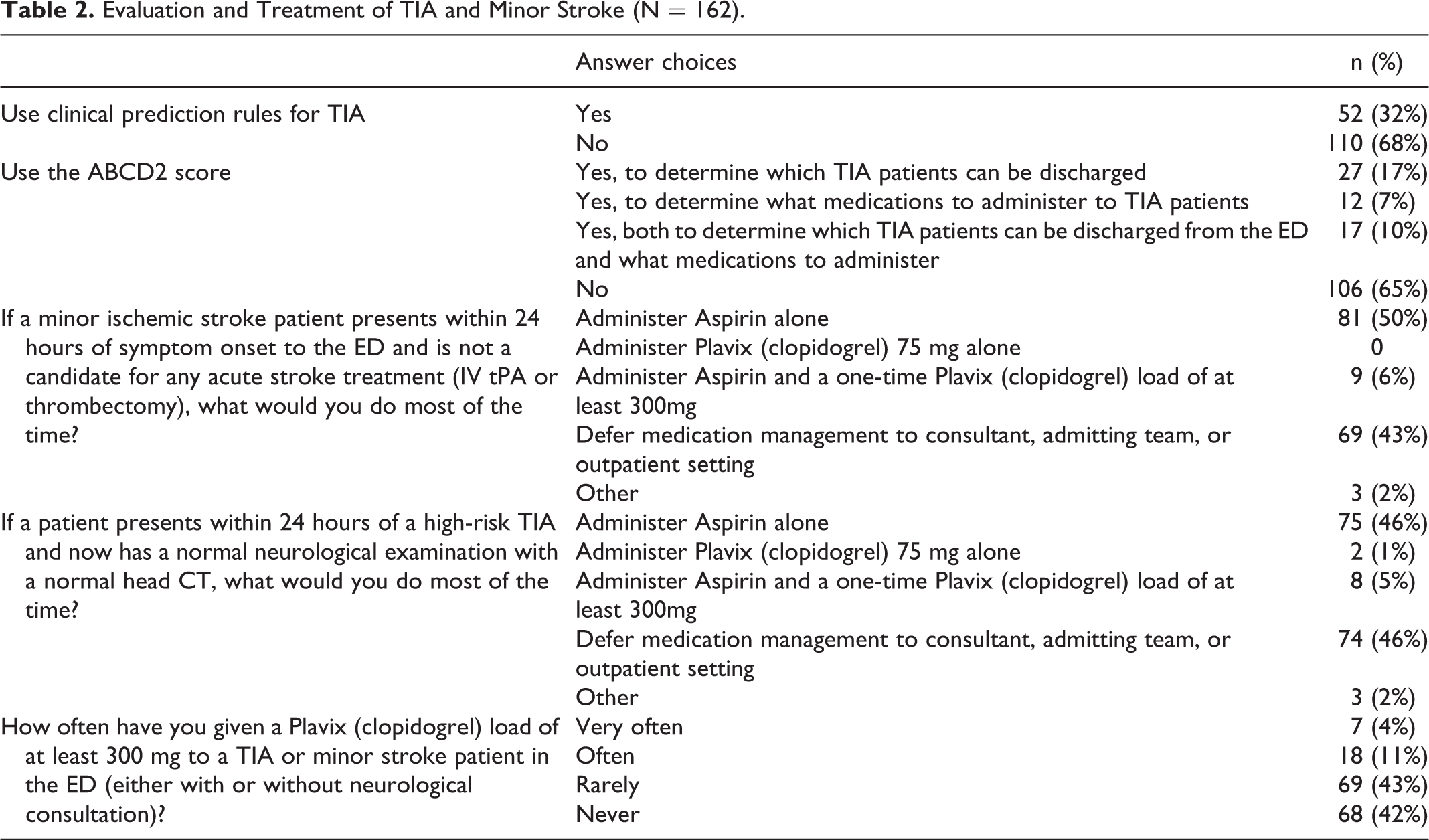
Many participants reported treating minor stroke and high-risk TIA patients who were eligible for DAPT with aspirin alone. Eighty-one (50%) reported treating minor stroke with aspirin and 75 (46%) reported treating high-risk TIA with aspirin only. Nine (6%) participants reported using aspirin plus clopidogrel, DAPT, to treat minor stroke patients and only 8 (5%) indicated that they would use DAPT for a high-risk TIA patient. Only 4 (2%) participants reported that they would treat both a minor stroke patient and a high-risk TIA patient with DAPT. Rather than select any antiplatelet agent(s) for treatment, 69 (43%) participants said they would defer medication management for minor stroke patients to a consultant, the admitting team, or the outpatient setting. Seventy-four (46%) participants reported that they would defer medication treatment decision making for high-risk TIA patients to another team. Treating high-risk TIA or minor stroke patients with a clopidogrel load of at least 300 mg was noted to have been done rarely by 69 (43%) and never by 68 (42%) participants (Table 2).
Among the 13 (8%) participants who indicated that they would treat either an eligible high-risk TIA patient or an eligible minor stroke patient with DAPT, DAPT treatment rates were not significantly different between physicians practicing in academic centers as compared to those at any other center (46% vs. 54%; p = 0.54). Similarly, DAPT treatment rates were not significantly different between physicians who completed medical school in the past 5 years as compared to participants in practice for at least 6 years (46% vs. 54%; p = 0.17). No emails were received by the study’s primary investigator from any survey participants.
Discussion
In an online survey of 162 EM physicians practicing in the US, we found that few physicians reported using aspirin plus clopidogrel, DAPT, to treat high-risk TIA and minor stroke patients within 24 hours of symptom onset. Only 4 (2%) participants indicated they would treat both a high-risk TIA as well as a minor stroke patient with DAPT; nearly half favored treatment with aspirin monotherapy. Our results suggest a significant opportunity to improve evidence-based treatment of high-risk TIA and minor stroke patients who present to the emergency department.
Given that the incidence of TIA is at least 200,000 events per year and nearly one half of all ischemic stroke patients initially present with minor symptoms,19-21 implementation and dissemination of up-to-date treatment paradigms among these patients is essential for reducing stroke risk. While EM physicians likely play a particularly important role in assuring timely administration of DAPT for TIA/minor stroke since ischemic stroke risk is highest shortly following index event, 22 our results emphasize that physicians from other services and specialties are also frequently involved in TIA and minor stroke management. Full-time access to neurological consultation was reported by most survey participants, some of which may have been via teleneurology. 23 Furthermore, nearly half of the survey respondents indicated they would defer medical management of TIA/minor stroke to consultants or admitting teams, suggesting that additional targets for guideline dissemination exist outside of the emergency department.
Our finding that 65% of study participants reported not using the ABCD2 score is internally consistent with our finding that few participants reported using DAPT since the ABCD2 score is a key component of determining DAPT eligibility among TIA patients.3-5 A previous state-wide provider survey of mostly EM physicians demonstrated infrequent use of the ABCD2 score in management of TIA; only 11% of surveyed providers reported using the score most or all of the time. 24 A majority (56%) of their study participants selected “don’t know” to the question regarding strength of evidence for the ABCD2 score, leading the authors to hypothesize that reluctance to use the ABCD2 score might relate to lack of clinicians’ knowledge about the rule’s validity. 24 While consistent with our study’s findings, this prior work was published before the first AHA/ASA guidelines strongly recommending DAPT for TIA/minor stroke. 7 Understanding the reasons most EM physicians in our current study reported infrequent use of the ABCD2 score to determine DAPT eligibility requires further investigation, but may similarly relate to concerns about the rule’s validity. 25 We did not find that our study participants were using alternative clinical decision rules to inform TIA care; clinical decision support for EM providers to improve TIA/minor stroke evaluation and treatment has great potential to improve patient care.26,27
Importantly, this current study was not designed to identify determinants of appropriate DAPT use in the emergency setting. A prior mixed-methods study within the Veterans Health Administration (VHA) identified some key barriers for acute TIA care including access to timely brain imaging, working with a constantly rotating pool of house staff, resource constraints related to personnel and services provided, poor care coordination across services, and limited staff and patient education. 28 Timely administration of evidence-based antiplatelet treatment to TIA and minor stroke patients was not directly addressed in the VHA study, but we suspect that improving staff education and updating facility protocols to incorporate DAPT use may play an important role in assuring high-quality care in the emergency setting.
In our pre-specified analysis, we did not identify differences according to physician or practice features associated with DAPT treatment. Understanding features associated with early adoption of evidence-based practices among EM physicians, in addition to barriers and facilitators of DAPT treatment, are important targets for future research efforts. Empirical data regarding TIA/minor stroke patient treatment within 24 hours of symptom onset are also needed. To date, we are only aware of one abstract using data from Get with the Guidelines-Stroke which found that, while the proportion of patients prescribed DAPT has increased over time, only 31% of minor stroke patients were discharged on DAPT in 2019. 29 Taken together with our results, these findings suggest that real-world treatment gaps exist for high-risk TIA and minor stroke patients, but more data are needed.
Our study has several limitations. First, we do not know the true number of physicians who saw our study invitation and, therefore, cannot calculate a survey response rate. Second, our study population is a convenience sample, although we did have good representation from multiple US regions and a well-balanced mix of non-academic and academic physicians to enhance the generalizability of our findings. Third, we did not include neurologists or other providers who may be involved in acute TIA and minor stroke evaluation and treatment in the emergency setting. We also failed to explicitly clarify in our study whether neurological consultation was available in person or via teleneurology and whether or not either is routinely requested for minor stroke/TIA patients who arrive outside the time window for thrombolysis. Finally, our survey questions were brief and did not include any true case vignettes. As in all survey studies, it is uncertain whether or not our participants’ survey answers precisely correspond to their real-world clinical decision making.
Conclusion
In a survey of EM physicians, we found that the use of DAPT to treat eligible TIA and minor stroke patients was rarely reported. Our findings highlight the need to identify determinants of DAPT treatment in the emergency setting as well as to develop strategies to improve the uptake of this treatment to reduce stroke risk.
Supplemental Material
Supplemental Material, sj-pdf-1-nho-10.1177_19418744211022190 - Treating High-Risk TIA and Minor Stroke Patients With Dual Antiplatelet Therapy: A National Survey of Emergency Medicine Physicians
Supplemental Material, sj-pdf-1-nho-10.1177_19418744211022190 for Treating High-Risk TIA and Minor Stroke Patients With Dual Antiplatelet Therapy: A National Survey of Emergency Medicine Physicians by Ava L. Liberman, Andrea R. Lendaris, Natalie T. Cheng, Nicole L. Kaban, Sara K. Rostanski, Charles Esenwa, Benjamin R. Kummer, Daniel L. Labovitz, Shyam Prabhakaran and Benjamin W. Friedman in The Neurohospitalist
Footnotes
Acknowledgments
Dr. Liberman is supported by NINDS research grant K23NS10764. Dr. Prabhakaran reports funding from AHRQ grant R18HS025359 and grant R18HS027264.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Dr. Liberman is supported by NINDS research grant K23NS10764. Dr. Prabhakaran reports funding from AHRQ grant R18HS025359 and grant R18HS027264.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.