
Abstract
The artery of Davidoff and Schechter (ADS) is the only meningeal branch of the posterior cerebral artery (PCA), supplying the medial tentorial margin and posterior portions of the falx. Given its small size, it is rarely identified on angiographic studies, unless enlarged in pathologies such as dural arteriovenous fistulas (DAVFs) or vascularized masses. This artery was first described by Wollschlaeger and Wollschlaeger in 1965, and to date, only a few reports have described its significance. The objective of this study is to report our experience with the ADS in dural fistulas from 2 tertiary medical centers and to emphasize the importance of recognizing this artery during angiographic examination of vascular tentorial and posterior fossa lesions. To our knowledge, this report demonstrates the largest angiographic case series published to date, recognizing a total of 7 patients with ADS arising secondary to a posterior fossa or tentorial DAVF and one of the largest reported series of DAVFs supplied by the ADS treated by endovascular and surgical techniques. Our cases validate the importance of prompt identification of the ADS for the diagnosis as well as endovascular treatment of vascular malformations in the posterior fossa and tentorial region.
Introduction
The Artery of Davidoff and Schechter (ADS) is the only dural branch of the posterior cerebral artery (PCA), giving vascular supply to the medial tentorium and posterior falx. 1 Wollschlaeger and Wollschlaeger originally described the artery in 1965 in 9 out of 10 cadavers, noting a fairly consistent origin from the ambient segment (P2) of the PCA and named it after their mentors.2-4 The artery has an average diameter of 0.8 mm, mean length of 12 mm, maintains an intradural origin, courses posteriorly through the ambient cistern between the superior cerebellar artery and the fourth cranial nerve, and terminates along the medial undersurface of the tentorium where it supplies the falcotentorial junction.1,5 Visualization and enlargement of the ADS portends underlying pathology, including dural arteriovenous fistulas (DAVF).4,6 Currently, DAVFs supplied by the ADS are only reported in case reports and the largest angiographic case series includes less than a dozen patients.4,7-10 Our aim is to present a case series of ADS supplied DAVFs in order to provide information on the spectrum of clinical presentation, cross-sectional and angiographic diagnosis, management strategies and functional outcomes.
Methods
Our study was approved by the Institutional Review Board and the requirement for informed consent was waived due to the retrospective nature of the study. Angiography reports were electronically searched via a database analytical tool (Montage TM, Nuance Communications) using “artery of Davidoff and Schechter” and “Davidoff and Schechter” as keywords between 2016 and 2020. Reports were verified for accuracy by fellowship trained neurointerventionalists, and generated by faculty with group average of a decade experience. All patients who had this artery identified during their diagnostic or interventional angiographic studies were enrolled. Clinical evaluation of the 5 patients who underwent treatment of the ADS supplied DAVF consisted of a mean follow up time of 31.6 months (range 20-52 months).
Results
Seven independent cases were identified for review. The laterality, arterial feeder, primary venous drainage, clinical symptoms, Borden and Cognard classifications, management strategies, angiographic and functional outcomes are presented in Table 1. The artery had a right, left and bilateral distribution in 4, 2, and 1 patient, respectively. The mean age at presentation was 61.9 years (95% CI 50.6-73.1), the median was 64.0 years and 57% male. There were a variety of presenting symptoms, including thunderclap headache, worst headache of life (WHOL), pulsatile tinnitus, poor appetite, lethargy, generalized fatigue, worsening drowsiness and confusion. The ruptured DAVF cases were associated with gross or xanthochromia/microscopic subarachnoid hemorrhage (SAH) with corresponding imaging findings.
All Patients’ Presenting, Treatment and Follow-Up Data.
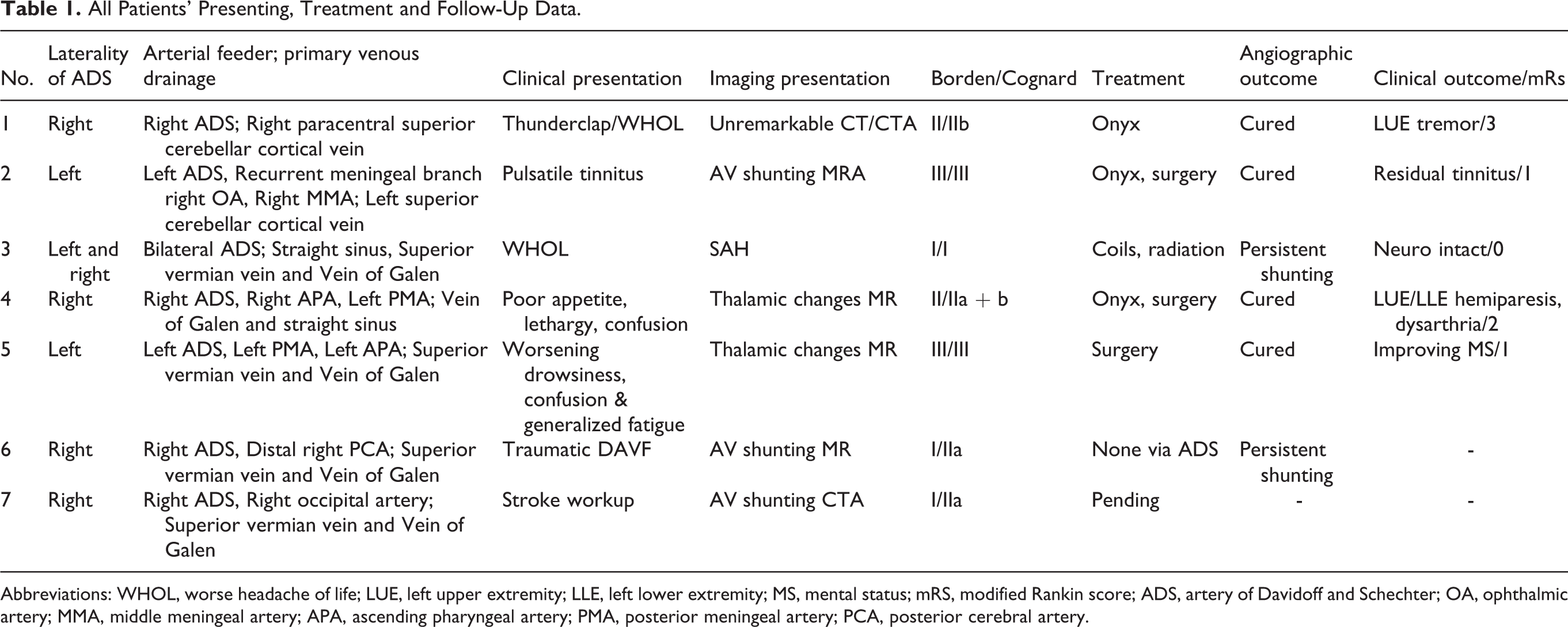
Abbreviations: WHOL, worse headache of life; LUE, left upper extremity; LLE, left lower extremity; MS, mental status; mRS, modified Rankin score; ADS, artery of Davidoff and Schechter; OA, ophthalmic artery; MMA, middle meningeal artery; APA, ascending pharyngeal artery; PMA, posterior meningeal artery; PCA, posterior cerebral artery.
In our case series, 5 patients underwent treatment for their ADS supplied DAVFs. One patient had adjuvant radiotherapy after coil embolization of a venous varix; 2 patients underwent trans-arterial neoadjuvant liquid embolization using Onyx 18 (ev3, Irvine, California) prior to surgical resection; and 1 patient underwent trans-arterial liquid embolization alone using Onyx 18. Case 6 is undergoing progressive endovascular treatments of a traumatic DAVF via embolization of external carotid artery feeders, however the ADS feeders supplying the tentorial fistula have not been embolized; as such, follow-up clinical evaluation was not included for this patient. One patient underwent only surgical intervention. The remaining patient in our case series (case 7) has elected conservative management.
The clinical evaluation of the 5 patients who underwent treatment of the ADS supplied DAVF consisted of a mean follow-up time of 31.6 months (range 20-52 months) without recurrent presentations with the exception of patient 3 who showed persistent filling of a venous varix on 28 months follow-up MRA. Although there were no immediate intraprocedural complications, 2 patients experienced delayed brainstem/midbrain infarcts due to reflux of embolization agent into the posterior cerebral artery. This resulted in left upper extremity tremor/hemiparesis in patient 1 and left upper and lower extremity hemiparesis in patient 4 with associated dysarthria. The neurological deficits persisted on follow-up evaluations. Patient 5 developed immediate temporary cranial VI neuropathy attributed to postoperative symptomatic tension pneumocephalus and new right-hand numbness which subsequently resolved. The remaining 3 patients demonstrated angiographic cure of the fistula without immediate or delayed complications.
The 7 Cases Are Detailed Below
Case 1
Patient presented with thunderclap headache and WHOL. Head CT/CTA were negative; lumbar puncture demonstrated xanthochromia. Digital subtraction angiography (DSA) showed arteriovenous shunting from the right ADS with early venous drainage into dural and cortical veins consistent with DAVF. Single session Onyx embolization of the DAVF was performed after microselection of the ADS, resulting in angiographic cure of the fistula. mRS 3 at 52 months.
Case 2
Patient presented with right-sided pulsatile tinnitus and hearing loss. MRI demonstrated prominent cortical veins in the posterior fossa. DSA showed multiple AVFs, including a posterior fossa DAVF supplied by the left ADS, a recurrent meningeal branch arising from the right ophthalmic artery into a cortical vein, and suspected much lesser contribution from right middle meningeal artery (Figure 1). Onyx embolization was performed after microselection of the ADS with decreased AV shunting (Figure 2); followed by suboccipital craniectomy and microsurgical obliteration of the DAVF. Patient had angiographic resolution of the fistula, but there was residual tinnitus. mRS 1 at 29 months.
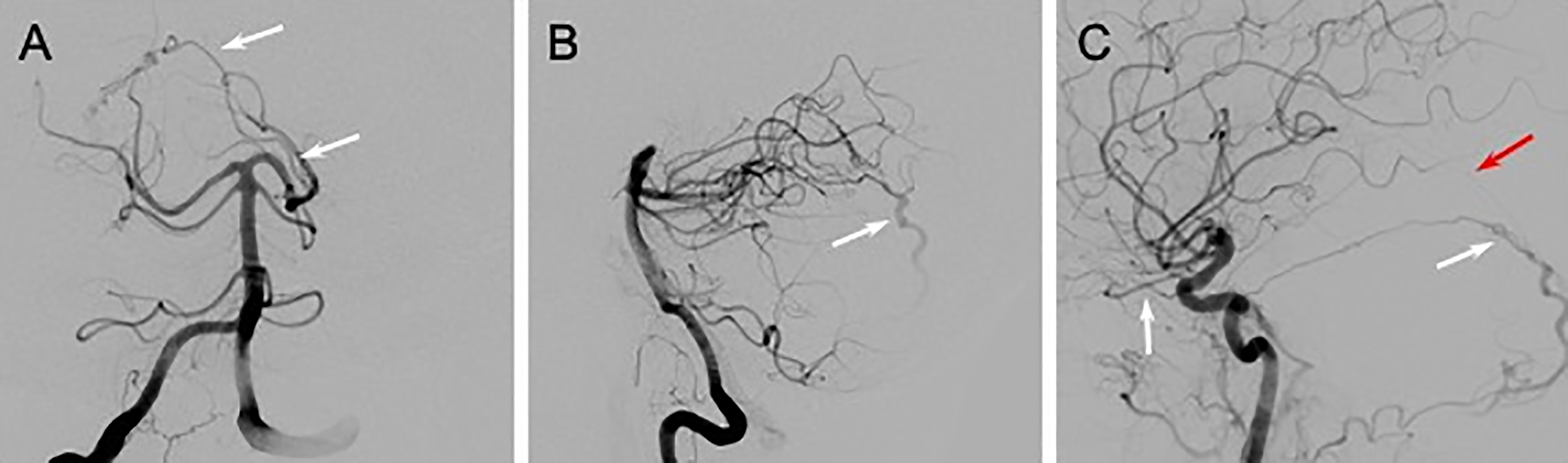
Cerebral DSA of posterior fossa dural AVF (patient 2). Frontal and lateral views of the right vertebral artery shows supply to the fistula from an enlarged ADS arising from the left PCA (arrows in A) and early venous drainage (arrow in B). Lateral view of the right internal carotid artery with reflux into the right external carotid artery shows additional supply to the posterior DAVF from a recurrent meningeal branch arising directly from the right ophthalmic artery (white arrows in C) and a much smaller contribution from the right middle meningeal artery (red arrow in C).
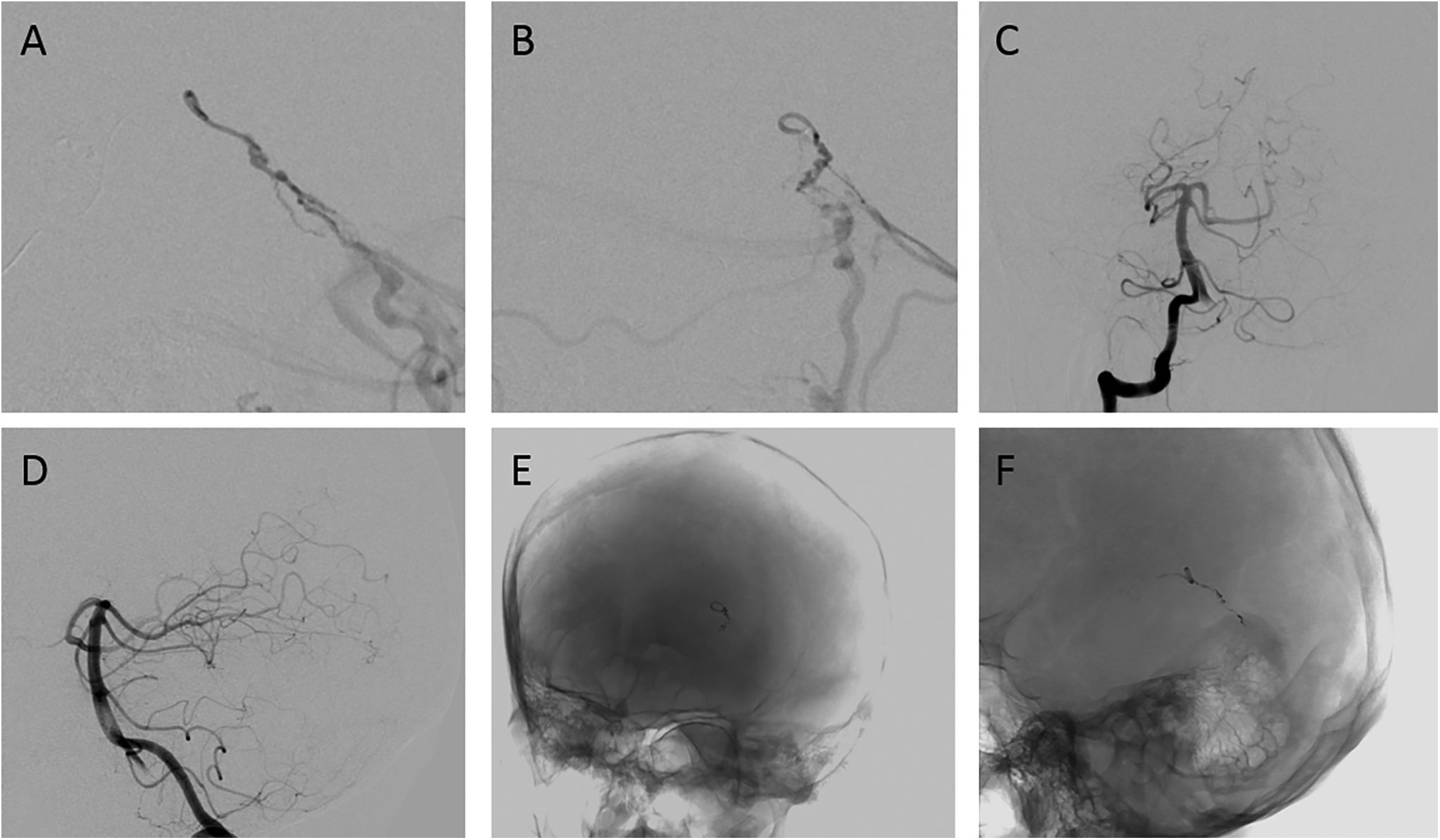
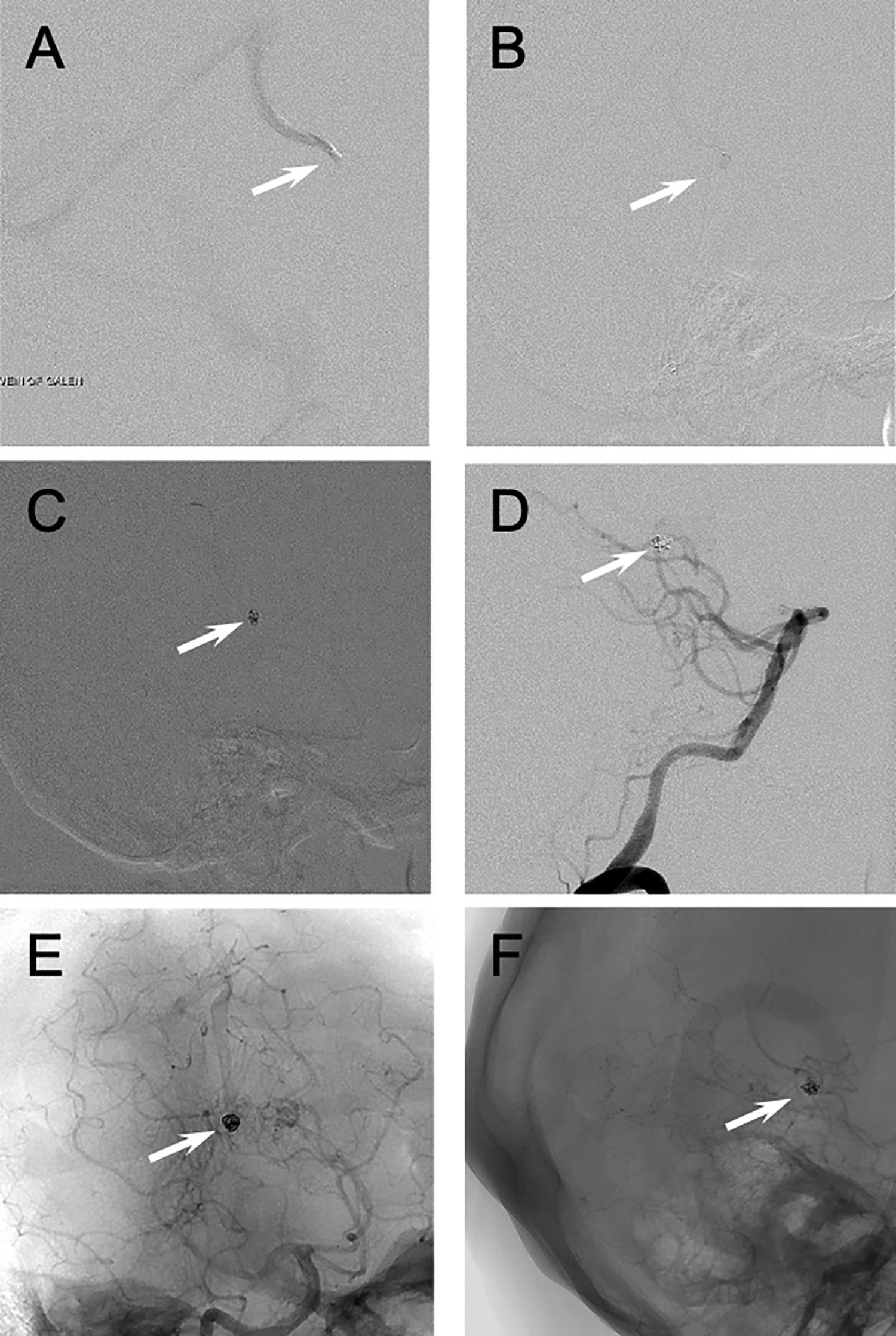
Cerebral DSA and endovascular treatment of posterior fossa dural AVF (patient 2). Frontal and lateral microcatheter injections via the left ADS confirm fistulous communication (A and B). Complete obliteration of arterial supply to the posterior fossa DAVF via the left ADS is demonstrated by post embolization control injections through the right vertebral artery (C and D). Frontal and lateral nonsubtracted views show the Onyx cast following the transarterial embolization (E and F).
Case 3
Patient presented with WHOL and lethargy. CT demonstrated SAH with intraventricular extent. DSA demonstrated a DAVF supplied by bilateral ADS branches and a venous varix which was interpreted as the source of SAH (Figure 3). Venous varix was successfully treated with transvenous microcoil embolization but there was unresolved arteriovenous shunting (Figure 4). Trans-arterial embolization of the bilateral ADS feeders was not performed as they also supplied the thalami. Patient therefore underwent adjuvant Cyberknife stereotactic radiotherapy (3,300 cGy 3 fractions of 1,100 cGy per fraction for 2 sessions). mRS 0 at 36 months.
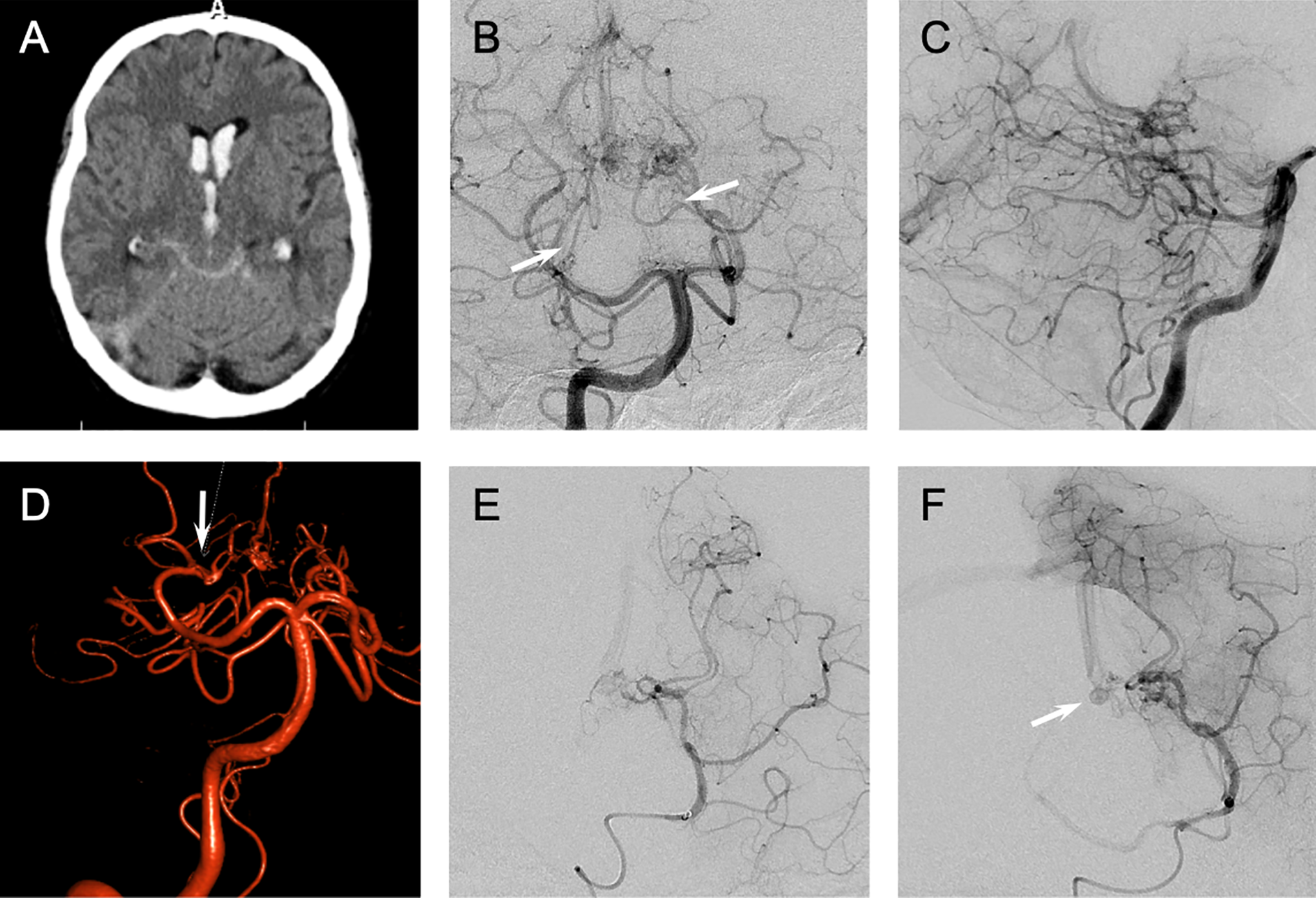
Non contrast head CT and cerebral DSA of posterior fossa dural AVF (patient 3). Non contrast head CT on presentation shows subarachnoid hemorrhage with blood in the quadrigeminal cistern and moderate intraventricular extension (A). Frontal and lateral views of the right vertebral artery show enlarged bilateral ADS supplying the fistula (arrows in B). 3D rotational digital subtraction angiography shows supply to the fistula via the right ADS (arrow in D). Frontal and lateral microcatheter injection via left PCA confirms the fistulous communication (E and F). A small venous varix is best seen on the lateral view (arrow in F).
Cerebral DSA and endovascular treatment of posterior fossa dural AVF (patient 3). Lateral transvenous views show the venous varix at the level of the vein of galen (arrows in A and B). Lateral view of transvenous coil embolization (C) and lateral view of right vertebral artery run (D) show coil mass in the venous varix at the level of the vein of galen (arrows in C and D, respectively). Frontal and lateral nonsubtracted views show the coil mass following the transvenous embolization (arrows in E and F).
Case 4
Patient presented with 2 weeks of lethargy, poor appetite and confusion. Brain MRI demonstrated T2 prolongation in the left greater than right thalami with enhancement and central areas of restricted diffusion, concerning for venous congestion secondary to arteriovenous shunting. DSA demonstrated a tentorial DAVF supplied by the right ADS, ascending pharyngeal (APA) and left posterior meningeal arteries (PMA) with drainage into the straight sinus. The right ADS was successfully embolized with Onyx, resulting in decreased filling of the DAVF. 18 days later, 150-250 µm contour polyvinyl alcohol particle embolization of right APA feeders was performed. Left PMA feeders were treated surgically. There was complete angiographic obliteration of the DAVF. mRS 2 at 22 months.
Case 5
Patient was transferred from an outside institution for work up of bithalamic lesions that were previously biopsied but unrevealing for originally suspected lymphoma. MRI demonstrated left greater than right thalamic increased FLAIR signal abnormality. MRA demonstrated abnormal venous flow along the left tentorium. DSA demonstrated a tentorial DAVF supplied by the left ADS, and feeders from the left PMA and the left APA. Due to concern for reflux of Onyx into the midbrain after microselection of the ADS, endovascular embolization was not performed. Patient underwent successful surgical clipping of the tentorial DAVF with intraoperative angiogram confirming complete DAVF obliteration. mRS 1 at 20 months.
Case 6
Patient presented with hemorrhage on CT from a complex posttraumatic DAVF involving the posterior portion of the superior sagittal sinus. A tentorial DAVF was also identified with arterial supply from a right ADS feeder as well as pial arterial supply from distal right PCA and drainage into a midline venous pocket.
Case 7
Patient presented with episodes of syncope and transient dysarthria. CTA demonstrated prominent vasculature in the posterior fossa. DSA demonstrated multiple DAVFs including a posterior fossa DAVF with arterial supply from the right ADS and the right occipital artery. Patient was discharged home in stable condition and elected conservative treatment at baseline.
Discussion
In this retrospective case series, we provide clinical presentation, non-angiographic imaging findings, angiographic classification, treatment strategies and functional outcomes of ADS supplied DAVFs. The clinical presentation of our patients included headaches, nausea, tinnitus, confusion and hearing loss which is consistent with prior reports.7,8,10 The diagnosis of an ADS supplied DAVF can be challenging not only due to these non-specific clinical symptoms at presentation but also due to its variable imaging appearance. Radiological imaging presentation can range from SAH to central venous congestion manifested as increased signal abnormality of the thalami, seen in 2 of our patients. Prior reports have identified venous congestion without thalamic MRI signal.4,10,11
The angioarchitecture identified in our cases was associated with predominately unilateral ADS feeders with the exception of 1 case. These findings are concordant with prior cadaveric study of the ADS that identified only unilateral presence of the vessel in most microdissections. 1 The majority of our cases were also associated with a higher-grade Borden and Cognard type DAVF which overall explains the higher risk of SAH. 12
In our case series, angiographic resolution of the DAVF was associated with a permanent cure on follow-up evaluation in 4 cases, while subtotal occlusion resulted in clinical improvement in 1 case. These findings are consistent with prior tentorial DAVF case series. 7 Overall, our functional outcomes and complication spectrum are more in line with work from Byrne and Garcia 7 and risks are possibly higher than previously reported 8 even in the hands of experienced neurointerventionalists. Our case series may also reflect a more heterogeneous group of patients, which could explain higher risks. Non-targeted embolization using Onyx 18 via anastomosis between the ADS and PCA is possible and resulted in brainstem infarcts in 2 cases, but overall functional outcomes showed improvement without any mortality. Onyx leaves little room for reflux into the adjacent PCA, but the alternative of nBCA liquid embolic agent also suffers from this limitation, and is less used in other cases series.7-9 A transvenous approach has been described to seal the fistula site using a reverse pressure cooker effect to the Vein of Galen, 8 but this technique is less commonly used and risks injury to the venous outflow and potential hemorrhage.
The diagnosis of an ADS supplied DAVF can be challenging due to its nonspecific associated clinical symptoms and variable radiological presentation. Knowledge of this angiographic anatomy is fundamental for neurointerventionalists-especially given repercussions of embolization while selecting meningeal feeders from an eloquent PCA. Our experience adds to the small but growing body of literature of this rare pathology.
Table 1. Laterality, arterial feeder, primary venous drainage, clinical symptoms, Borden and Cognard classifications, management strategies, angiographic and functional outcomes for each patient.
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.