
Abstract
Background:
Spasm control is essential in the management of tetanus. Benzodiazepines are administered as initial treatment of tetanic spasms; however, sedation may be difficult to attain among patients with methamphetamine use disorder. Neuromuscular blocking agents, which act on an entire different mechanism, can be given to induce paralysis.
Methods:
We describe 2 cases of patients with methamphetamine use disorder who were diagnosed with severe tetanus and our experience in the use of rocuronium to control their spasms. We performed a systematic review of the SCOPUS and PubMed databases for case reports and case series describing the use of rocuronium in tetanus patients who also have methamphetamine use disorder. We discussed the clinical features and treatment outcomes.
Results:
A total of 4 cases of patients with substance abuse disorder who had severe tetanus were reported in the literature, including the current cases. The mean age was 28.8 years; all of them male. Trismus, generalized limb and abdominal rigidity were the most common presentation. Three patients underwent emergency tracheostomy. Rocuronium was given as 0.008mg/kg bolus in 1 patient; 2 patients received an intravenous bolus dose of 0.6mg/kg. Infusion dose ranged from 5 to 10 mcg/kg/min. Spasms were controlled within 24-48 hours after giving rocuronium in 3 out of 4 patients. One patient died from complications of dysautonomia and immobility.
Conclusion:
Rocuronium demonstrates a potential role as neuromuscular blocking agent of choice for patients with chronic methamphetamine use disorder and severe tetanus. Management challenges and complications of severe tetanus were also highlighted in this study.
Introduction
Tetanus remains a serious public health concern in developing countries. Seventy-nine percent (79%) of deaths due to tetanus were estimated to occur in south Asia and sub-saharan Africa in 2015. 1 In 2015, the Philippines had 376 deaths with a mortality rate of 0.38 per 100,000 cases of non-neonatal tetanus. 1 The World Health Organization reported 1,057 cases in 2017 and 943 cases in the Philippines despite global strategies for vaccination.2,3 The disease is characterized by muscle rigidity and stimulus-induced spasms beginning in the masseter (trismus being the presenting symptom in more than half of patients), neck, and abdominal muscles. Eventually becoming spontaneous and generalized, the spasms may result in fractures of long bones and vertebrae, and renal failure from rhabdomyolysis. 4 Dysautonomia, characterized by labile blood pressure, tachycardia/arrhythmias and temperature dysregulation, invariably complicates severe cases and it is associated with poorer prognosis. 5
Spasm control is essential in the management of tetanus. Benzodiazepines like diazepam and midazolam are considered first-line drugs because of their anticonvulsant, muscle relaxant, sedative, and anxiolytic properties. 5 In patients with spams unresponsive to benzodiazepines, neuromuscular blocking agents (NMBA) can be given to induce paralysis. 5
Sedation with benzodiazepines (BDZ) is generally difficult to attain among patients with methamphetamine use disorder as these patients may be resistant to BDZ. 6 Managing spasms in tetanus patients who have a history of methamphetamine use may therefore be extremely difficult. Thus, NMBA may represent a useful therapeutic option in this subset of tetanus patients when presenting with refractory spasms. In this article, we describe 2 cases of patients with methamphetamine use disorder who were diagnosed with tetanus and our experience in the use of rocuronium, an NMBA to control their spasms.
Case 1
A 48 year-old male with no known comorbidities presented to the emergency department (ED) complaining of stiffening of the limbs. A week prior, he had a puncture wound on his right foot. At presentation in the ED, his vital signs were stable, although he had trismus and abdominal rigidity. Social history revealed methamphetamine use for the past 10 years. His urine toxicology screen was likewise positive for methamphetamine. Initial treatment for tetanus, including emergency tracheostomy were done.
Due to spontaneous spasms occurring 4 times a day, diazepam 10 mg intravenously every 4 hours was initiated. Diazepam was shifted to continuous infusion of midazolam (0.15 mg/kg/hr) the next day while the patient was under ventilatory support. Spontaneous spasms persisted, occurring approximately every 2 hours. On the third hospital day (HD), the frequency of spasms increased to almost hourly, despite an increase in midazolam infusion to 0.30mg/kg/hr. Laboratory signs of rhabdomyolysis were noted, with myoglobinuria and increased creatinine kinase levels. The managing service therefore decided to start neuromuscular blockade with a rocuronium bolus (0.6mg/kg IV) followed by continuous infusion drip (8mcg/kg/min). Immediate resolution of the spasms was observed. Midazolam was titrated to achieve a Richmond Agitation-Sedation Score of -3 to -4.
Attempts to discontinue the rocuronium were started on the fifth HD and continued daily to look for spasm recurrence. On the sixth HD, the patient developed dysautonomia which was managed with the use of carvedilol given through a nasogastric tube. Rocuronium was successfully discontinued on the 14th HD. Midazolam infusion was terminated and oral diazepam was re-initiated, with a slow progressive taper. The patient underwent intensive physical therapy and he was finally discharged to home after 18 days of hospitalization. Decannulation was done after 1 month. He was independent in performing activities of daily living 3 months after hospital discharge.
Case 2
A 31 year-old male presented to the ED with generalized muscle rigidity. One week prior to admission, the patient sustained a puncture injury on his left fourth finger. At presentation in the ED, his vital signs were stable, although he had abdominal rigidity and stiff limbs. He used methamphetamine for the past 14 years. Urine toxicology screen was positive for methamphetamine. Emergency tracheostomy was done.
Diazepam was initiated for his generalized spasms and rapidly escalated to a dose of 20 mg intravenously every 2 hours, with limited response. While under mechanical ventilatory support, rocuronium was initiated with an intravenous bolus (0.6mg/kg IV) followed by continuous infusion (5-10 mcg/kg/min) titrated to effect. While on rocuronium, midazolam was started (0.15mg/kg/hr). Unfortunately, on the third HD, he developed severe dysautonomia characterized by hemodynamic instability and he suffered an asystolic cardiac arrest. Return of spontaneous circulation (ROSC) was achieved after 6 minutes of cardio-pulmonary resuscitation. Rocuronium was discontinued to allow better neurological assessment, but unfortunately his spasms recurred. Initial cranial computed tomography scan showed diffuse cerebral edema. Electroencephalogram, performed while on sedation, showed diffuse slowing pattern but no epileptiform discharges. Attempts to discontinue the rocuronium were continued daily, but unsuccessfully. On the 15th HD, during a trial of rocuronium discontinuation, he was noticed to have myoclonic movements. These were attributed to post-hypoxic myoclonus. Later on the same day, he had another episode of asystolic cardiac arrest with achievement of ROSC after 10 minutes. Family opted for change in goals of care and to focus on comfort measures. The patient expired on the 18th HD.
Methods
Because of the rarity of this condition, the authors decided to perform an extensive literature search to comprehensively discuss different cases describing the utility of rocuronium as an NMBA in severe tetanus patients with substance abuse disorder. Guided by the Preferred Reporting Items for Systematic Reviews and Meta-analyses statement, 7 we performed a systematic search of the PubMed and SCOPUS databases on April 5, 2020 using the keyword and MeSH terms “tetanus” and “rocuronium”. The reference list of the assessed articles also were searched for relevant studies.
All case reports and case series on patients with tetanus and substance abuse disorder, wherein rocuronium was used as a neuromuscular blocking were collected and analyzed. We included all English language studies published from the databases’ inception until the time of search.
The following data were collected: demographic information (age, sex, country of origin), clinical features (presenting symptoms), medical intervention (dose of rocuronium, sedatives given) and treatment outcome. Results were summarized using descriptive statistics. Written consent was obtained from the patient and patients’ family for the cases presented.
Results
A total of 216 articles were identified through the database search. After duplicates were removed, 8 articles were screened. Of these, 6 articles were excluded because it discussed rocuronium on non-human subjects, were incomplete and had abstracts only, or described rocuronium in the pre-operative setting. The full text of 2 articles was assessed. Two articles were included in the qualitative analysis (Figure 1).
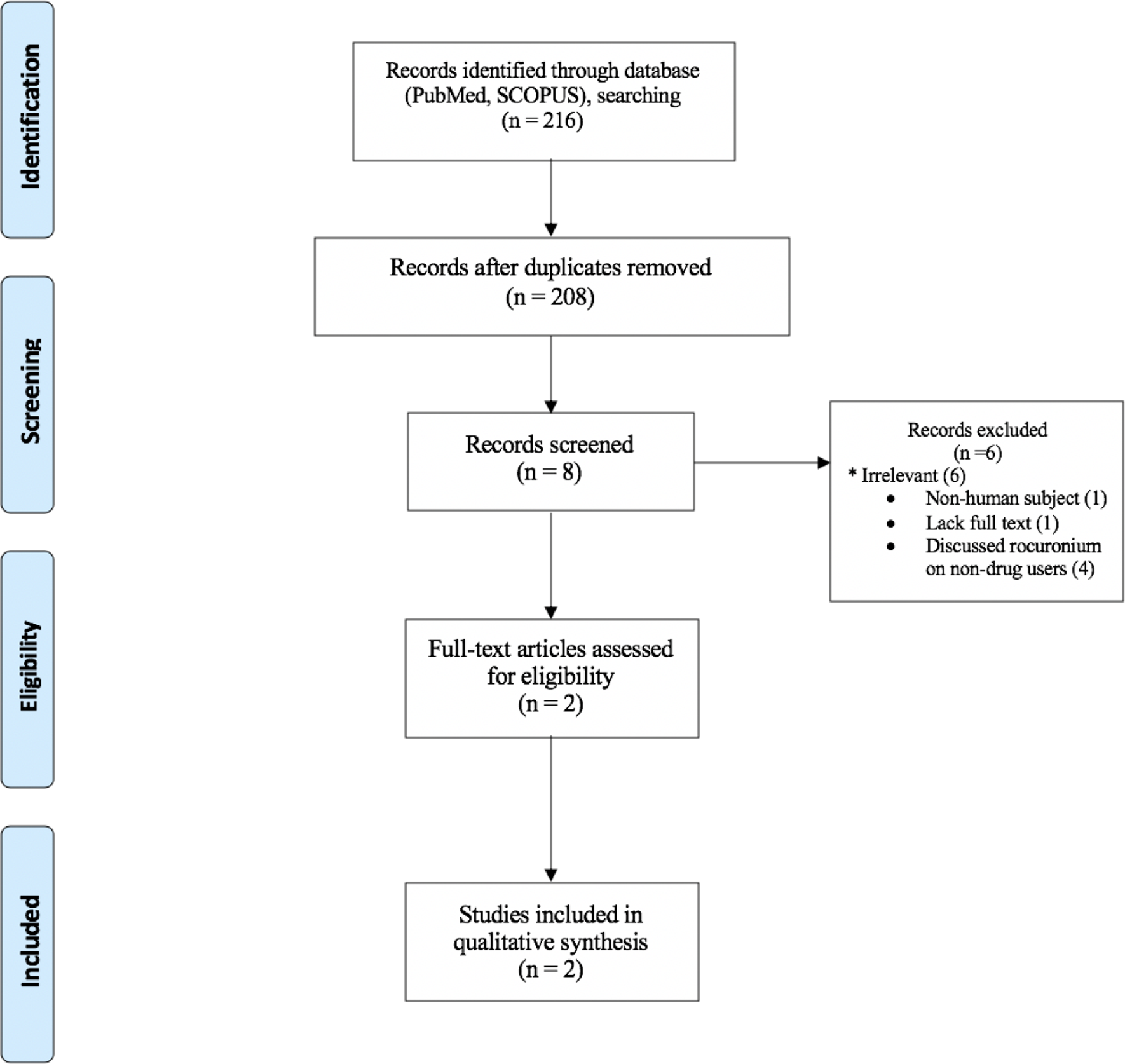
Preferred reporting items for systematic reviews and meta- analyses flow diagram of the systematic review.
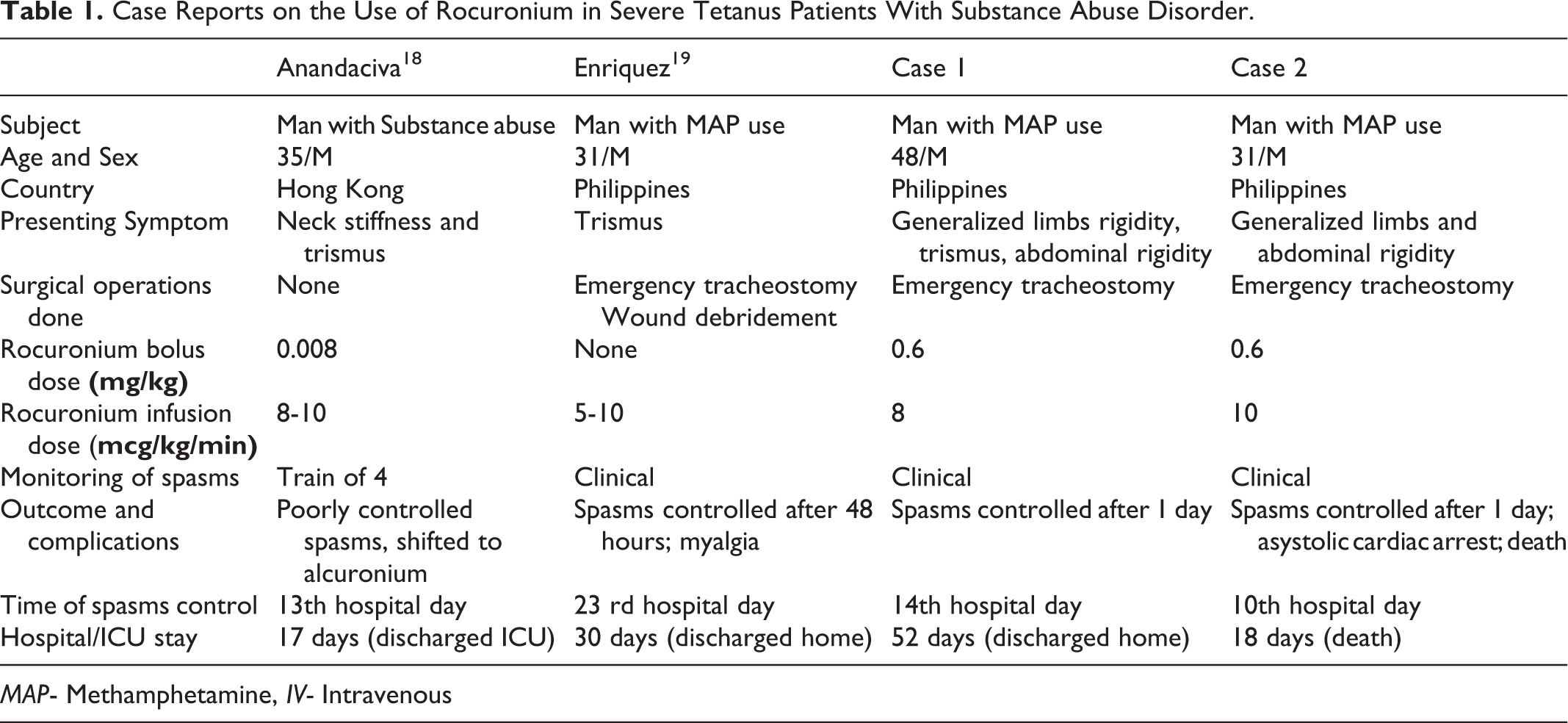
Including the current cases, there were a total of 4 cases in the current reported literature which used rocuronium in the control of muscle spasms of severe tetanus patients who had substance abuse disorder. The mean age was 28.8 years (range 31-48; standard deviation: 8.1), all of them male. The most common clinical presentation was trismus followed by generalized limb and abdominal rigidity. Three out of the 4 patients underwent emergency tracheostomy. Rocuronium was given as 0.008mg/kg bolus in 1 patient; 2 patients received an intravenous bolus dose of 0.6mg/kg. Infusion dose ranged from 5 to 10 mcg/kg/min. Spasms were monitored using train of 4 in 1 case. Spasms were controlled within 24-48 hours after giving rocuronium in 3 out of 4 patients. One of the 4 patients in the systematic review died from complications of dysautonomia and immobility (Table 1).
Case Reports on the Use of Rocuronium in Severe Tetanus Patients With Substance Abuse Disorder.
Discussion
Tetanic spasms are due to release inhibition of the neurotransmitters glycine and GABA caused by the toxins tetanospasmin and tetanolysin produced by Clostridium tetani. In particular, tetanospasmin (also called tetanus toxin), after reaching the spinal cord and brainstem via the motor neurons, is secreted and enters inhibitory interneurons, causing their inactivation. The net effect is a widespread disinhibition of anterior horn cells and autonomic neurons resulting in generalized contraction of agonist and antagonist muscles and dysautonomia. Clinically, patients present with rigidity, painful muscle spasms, and autonomic instability. 5
NMBA act directly on the muscle motor endplates by competing for the acetylcholine binding site. Drug-induced paralysis with NMBA prevents uncontrollable and painful spasms that cause rhabdomyolysis and can inflict kidney damage. 8 International guidelines mentioned the utility of pancuronium, vecuronium, pipecuronium, and rocuronium however, their detailed use and dosages in this specific population is not discussed in detail.5,9 In our hospital, we were also limited by the availability of only 2 NMBAs: atracurium and rocuronium.
Rocuronium use is described mostly in literature in reference to the peri-operative period. Its drug effect is characterized by rapid onset and intermediate duration of action; 10 compared to pancuronium and vecuronium, rocuronium has a more rapid onset 11 and is comparable to succinylcholine. 12 Rocuronium has demonstrated a safer cardiovascular profile than pancuronium, which also acts as an inhibitor of catecholamine reuptake. No identifiable cardiovascular or untoward side effects associated with bolus injections of rocuronium in doses up to 3 times the effective dose have been described. 13 In a study specifically designed to detect changes in hemodynamic variables, rocuronium boluses were not associated with identifiable hemodynamic changes and also limited histamine- releasing effect was demonstrated. 14 Human and animal studies show that the route of plasma clearance is predominantly hepatic uptake, with gastrointestinal and renal elimination. Therefore, patients with renal and hepatic impairment may demonstrate prolonged paralytic effect.
In our literature review, only 2 case reports described the use of rocuronium as a NMBA in patients affected by tetanus. Interestingly, one case study demonstrated poor control of the spasms with rocuronium at 0.008mg/kg IV bolus followed by another 0.9mg/kg IV bolus and 8-10 mcg/kg/min drip, eventually leading the physicians to switch to alcuronium. 15 Spasms were monitored through train of 4 in this study. The authors did not elaborate why spasms were not controlled in this patient.
Patients with a substance abuse disorder, particularly with chronic methamphetamine use, tend to be less responsive to sedative agents, including BDZ. 16 An animal study demonstrated the effect of methamphetamine on downregulation of the GABA receptors at the level of the nucleus accumbens. 17 Several studies have also shown that increasing GABAergic tone by activation of GABA_A or GABA_B receptors, or by inhibition of GABA metabolism and reuptake, abates the effects of drugs such as amphetamine. 18
Moreover, patients with chronic methamphetamine use paradoxically seem to be at higher risk of cardiovascular adverse events. 19 Chronic methamphetamine use is associated with the depletion of catecholamine storages of peripheral nerve terminals, therefore contributing to a blunted physiologic sympathetic response during hypotension and shock. 20 This mechanism can also worsen the effects of dysautonomia in severe tetanus. Patients with methamphetamine use disorder are also at higher risk for cardiovascular complications; 20 In some studies, rocuronium is said to have a better cardiovascular profile and may represent a safer alternative to pancuronium which is studied to worsen autonomic instability. 11 However, it should be noted that in our series, one of the patients succumbed to cardiac asystole although this could be attributed to the severity of tetanus or cardiovascular compromise from chronic methamphetamine use.
Case 2 highlights the challenges in monitoring the sensorium of patients with tetanus requiring neuromuscular blocking. When using NMBA, it is extremely important to have in place a protocol allowing to determine the earliest time when the NMBA can be discontinued.
The authors acknowledge that the difficulty of performing a randomized control trial that can ascertain the best dose and route of which rocuronium should be given in this special population. Nonetheless, we suggest further rigorous methods that employ a prospective collection of data to substantiate our findings. The use of train of 4 test to monitor the spasms is also recommended in future studies to investigate rocuronium’s role in this population more objectively. Mechanisms of neuromuscular blockade and novel biochemical processes behind dysautonomia among these patients are likewise an interesting area of research.
Conclusion
We report 2 cases of patients with severe generalized tetanus and chronic methamphetamine use disorder who received rocuronium. Rocuronium demonstrates a potential role as neuromuscular blocking agent of choice for these patients. Management challenges and complications of severe tetanus were also highlighted.
Footnotes
Author Contribution
Dr. Sarmiento was involved in the direct patient care, acquisition of data, analysis and interpretation, and writing of the initial and final draft of the manuscript for intellectual content.
Drs. Enriquez, Jalipa, Piamonte, and Diestro were involved in the study conception, acquisition of data, analysis and interpretation, critical revision of the manuscript for intellectual content, and study supervision.
Drs. Jamora, Dioquino, and Goffi were involved in the study conception, acquisition of data, analysis and interpretation, critical revision of the manuscript for intellectual content, and study supervision.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Disclosure
The authors disclose no commercial or financial relationships, as well as potential conflicts of interest in the conduct of this research.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
Written informed consent was obtained from the patient and relatives for submission of these case reports.