
Abstract
Neuromelioidosis is a severe tropical infection with high morbidity and mortality. Isolated myelitis is an extremely rare manifestation of melioidosis which may evade diagnosis. We report a 69-year-old diabetic male patient who presented with acute flaccid paraplegia and longitudinally extensive myelitis and no systemic symptoms. MRI of spinal cord showed lower dorsal cord and conus T2 hyperintensity and microabscesses with dural enhancement. The diagnosis was clinched with blood culture growing Burkholderia pseudomallei. He rapidly developed colitis, septicemia and multiorgan dysfunction and succumbed to the illness in spite of antibiotics and aggressive supportive care. The case highlights that melioidosis should be considered as a differential diagnosis of infectious myelitis, especially in the tropics. Presence of a neutrophilic blood and cerebrospinal fluid picture and microabscesses in spinal cord are important diagnostic clues. The outcome is dismal unless the diagnosis is considered early in the disease course and managed expeditiously with sensitive antibiotics.
Introduction
Infectious myelopathies account for a sizeable proportion of non-traumatic myelopathies requiring inpatient rehabilitation in developing countries. 1 A wide variety of pathogens can precipitate spinal cord disease, producing distinct clinical syndromes including acute flaccid paralysis, acute transverse myelitis, cord compression, myeloradiculitis, and chronic spastic paralysis. Among these, acute suppurative myelitis leading to intramedullary abscess formation is rare and devastating. Staphylococcus aureus, Escherichia coli, and Brucella melitensis are the most common pathogens isolated from culture of spinal cord aspirate in such cases. 2
Melioidosis is an emerging bacterial infection endemic to the tropics including regions of Northern Australia and Southeast Asia and is caused by the gram-negative bacillus Burkholderia pseudomallei. Clinical manifestations of melioidosis can range from an acute fulminant septicemic illness to chronic deep-seated abscesses. 3 Neuro-melioidosis is associated with substantial morbidity and mortality and typically presents with cranial and meningeal manifestations. 4 Spinal disease is extremely rare and hence, melioidosis is often overlooked as a differential diagnosis of myelitis. We present a patient with a rapidly progressive myelitis with intramedullary abscess due to melioidosis with unique radiological features. We review the spinal presentations of melioidosis and discuss the clinical and investigatory parameters which should raise concern for this diagnosis.
Case Report
A 69-year-old man from Kerala, South India, presented with symptoms of ascending numbness and weakness of both lower limbs which progressed to complete paraplegia with urinary retention and constipation in 2 days. He did not have radicular or spinal pain, history of trauma, fever, or other systemic symptoms. He had poorly controlled diabetes mellitus of 14 years duration. He supervised farming in rice fields, but reported no contact with animals. He had no antecedent trauma or skin injury. He was evaluated elsewhere at the onset of symptoms. Routine hematology evaluation had shown neutrophilic leukocytosis with normal erythrocyte sedimentation rate (ESR) and normal biochemical parameters. Magnetic resonance imaging (MRI) of the spine done 3 days into the illness had shown a long segment holo-cord hyperintense signal in T2-weighted images from T8 to conus level. Non-contrast computerized tomography (NCCT) brain and contrast-enhanced CT thorax and abdomen were normal. Cerebrospinal fluid (CSF) examination done there, 5 days into the illness, showed 1400 white cells per mm3 with lymphocytic predominance (61% lymphocytes and 39% neutrophils), elevated protein (156 mg/dl) and hypoglycorrhachia (48mg/dl with a corresponding plasma sugar of 175mg/dl). CSF tuberculosis polymerase chain reaction (TB-PCR) was negative, adenosine deaminase (ADA) level was 46.5 U/L (elevated) and culture did not show any growth. CSF meningoencephalitis panel (qualitative PCR testing for Cryptococcus neoformans/gattii, cytomegalovirus, enterovirus, Escherichia coli-K1, Haemophilus influenzae, Herpes simplex 1 and 2, Human herpesvirus 6, Human parechovirus, Listeria monocytogenes, Neisseria meningitidis, Streptococcus agalactiae, Streptococcus pneumoniae, and Varicella zoster) was negative. He was given intravenous steroids with a presumptive diagnosis of acute spinal cord demyelination. As his symptoms were unabated, he was referred to this center for further evaluation.
At presentation here, he was alert, afebrile and had normal vital signs. Both lower limbs were hypotonic and areflexic with complete loss of power. Beevor’s sign was positive and plantar reflexes were equivocal bilaterally. He had a horizontal sensory level at the level of umbilicus. Rest of the neurological examination was normal. There was no spinal tenderness, deformity, or bruit and no meningeal signs. Systemic examination was unremarkable. He was started on anti-tubercular therapy (ATT) with rifampicin 400 mg/day, isonizaid 300 mg/day, pyrazinamide 1600 mg/day and ethambutol 1100 mg/day on admission after reviewing the imaging and CSF reports and while awaiting further investigations.
Routine laboratory tests revealed significant peripheral blood neutrophilic leucocytosis with a total leukocyte count of 17800 cells/mm3 (93% polymorphs), an ESR of 13 mm in the first hour and elevated C-reactive protein (20 mg/L). Serum electrolytes, and liver and renal function tests were normal at admission.
MRI of the spine repeated after 17 days of symptom onset showed increase in the extent of T2-weighted hyperintense signal changes in cord, extending from T7 to conus level with cord swelling. Contrast administration revealed multiple intramedullary rim-enhancing lesions in the conus region extending along the cauda nerve roots, suggestive of microabscesses with thickening and enhancement of the adjacent dura (Figure 1). No abnormal signal changes or enhancement of vertebral bodies were noted. MRI brain showed no obvious enhancing lesions or leptomeningeal enhancement. A repeat CSF analysis showed 730 white cells per mm3 with neutrophilic predominance (85% neutrophils and 15% lymphocytes), elevated protein (106 mg/dl) and hypoglycorrhachia (70mg/dl with a corresponding plasma sugar of 242 mg/dl). Etiological workup including CSF gene Xpert MTB (Mycobacterium tuberculosis), and brucella and toxoplasma antibodies were negative. Re-evaluation for focus of systemic infection with NCCT thorax and abdomen showed diffuse wall thickening, submucous edema and surrounding fat stranding involving distal ileum, ascending colon, transverse colon and descending colon, suggestive of pan-colitis and minimal ascites. An infectious bacterial myelitis was strongly suggested by the investigations and blood and CSF cultures were sent. The patient was started on ceftriaxone 4g/day and metronidazole 1500 mg/day on the third day of admission and meropenem 1g/day on the fifth day. Four days after the admission, he developed drowsiness, hypotension and oliguric renal failure. Diagnosis was clinched with blood culture after 48 hours which showed Burkholderia pseudomallei (Figure 2) sensitive to ceftazidime, meropenem, trimethoprim/sulfamethoxazole (TMP/SMX) and ciprofloxacin.
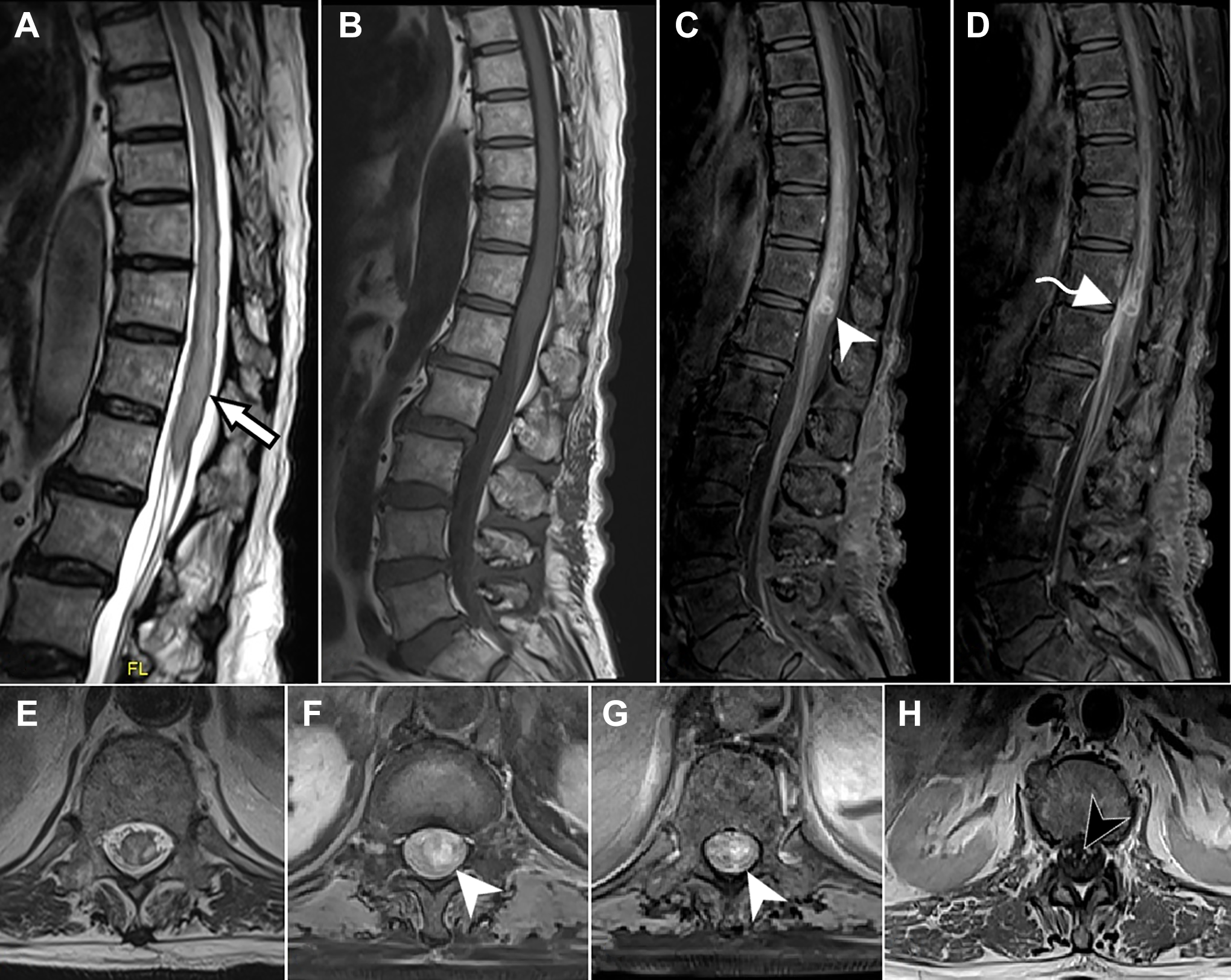
MRI of spinal cord. Sagittal T2, T1 (A, B), and axial T2-weighted (E) images show long segment lower thoracic cord and conus hyperintense signal changes from T7 level with swelling of the cord at T9 to T12 level and wavy undulations of posterior pial surface (white arrow). Post-contrast sagittal (C, D) and axial (F, G, H) images show multiple intramedullary conglomerate rim-enhancing lesions (white arrowhead) at the conus extending along the cauda nerve roots (black arrowhead). Adjacent thickening and enhancement of the dura at the level of conus (curved arrow in D) are noted.

Burkholderia pseudomallei in blood culture. Growth of Burkholderia pseudomallei on 5% sheep blood agar showing greyish-white glistening non-hemolytic colonies (A) and MacConkey agar showing wrinkled non-lactose fermenting colonies (B) at 48 hours of aerobic incubation. Gram staining of colonies from blood agar showing the characteristic bipolar stained (Safety Pin Appearance [Black arrows]) gram negative bacilli (C). [Magnification ×1000].
The patient further developed septic shock and multiple organ dysfunction syndrome (MODS) with rapid deterioration, requiring ventilatory and inotropic support. He succumbed to refractory septic shock after 1 week of admission with us, despite aggressive supportive care.
Discussion
This case illustrates an extremely rare and severe manifestation of melioidosis. Melioidosis of central nervous system (CNS) is infrequent, reported only in 1.5 to 5 percent of melioidosis.5,6 Encephalomyelitis, brain abscess, meningitis, extra-axial collections, and cranial neuropathies 5 have been reported commonly in them, while isolated myelitis as the initial presentation is exceedingly rare, accounting for only 1% of CNS melioidosis. 6 Table 1 summarizes the spinal cord presentations of melioidosis reported in literature. Our case presented with isolated myelopathy with microabscesses in the lower spinal cord, which has not been reported previously. The rarity of this presentation contributed to the delay in instituting specific antibiotic therapy.
Spinal Cord Presentations of Melioidosis.
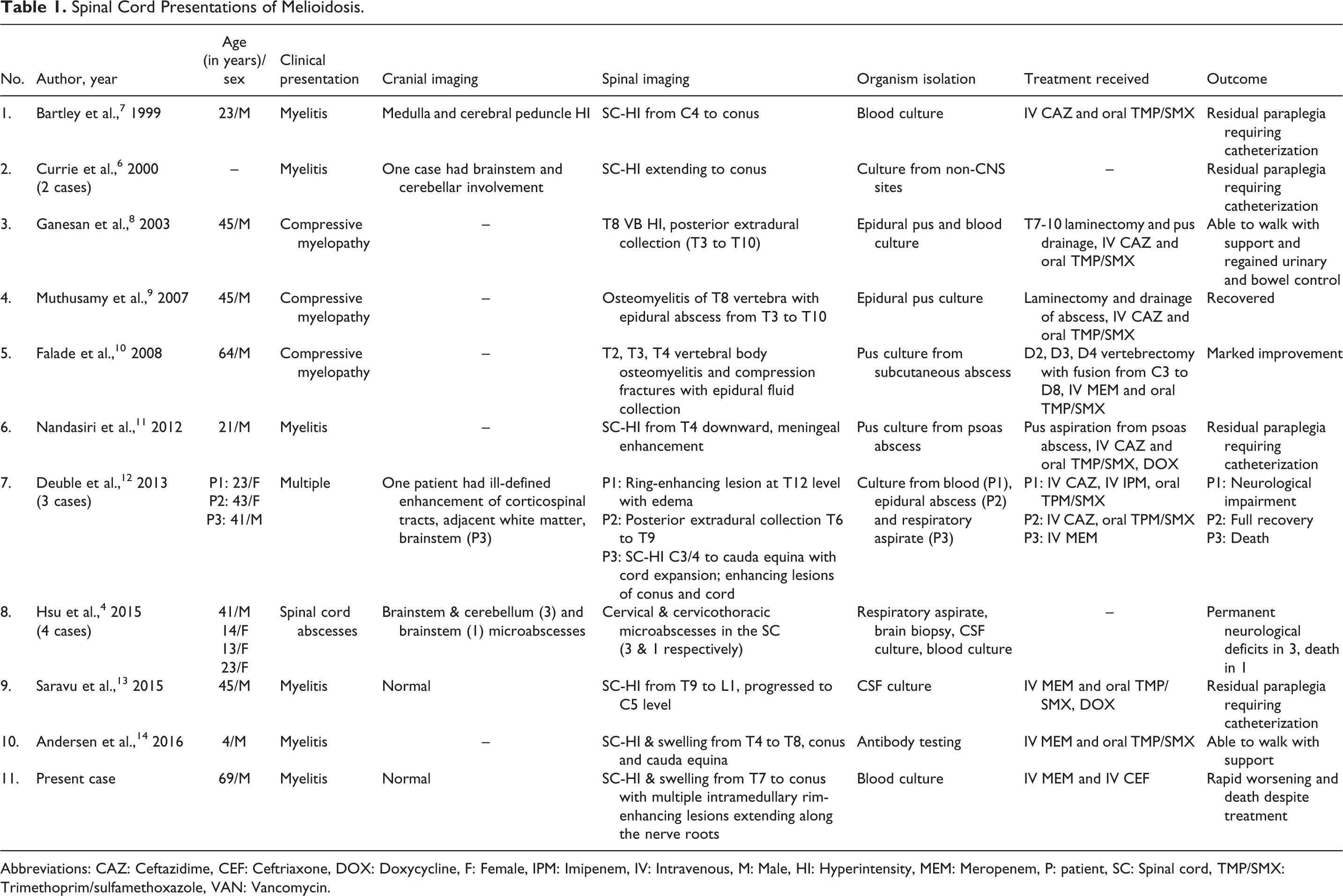
Abbreviations: CAZ: Ceftazidime, CEF: Ceftriaxone, DOX: Doxycycline, F: Female, IPM: Imipenem, IV: Intravenous, M: Male, HI: Hyperintensity, MEM: Meropenem, P: patient, SC: Spinal cord, TMP/SMX: Trimethoprim/sulfamethoxazole, VAN: Vancomycin.
The common modes of acquisition of melioidosis include inhalation, ingestion, or direct inoculation of the contaminated source. 3 The various hypothesized modes of spread of the pathogen to CNS include hematogenous spread after percutaneous inoculation, direct brainstem invasion through the nasal passage and cranial nerves, and percutaneous inoculation over the scalp and subsequent direct extension to the skull and brain. 5 Spinal cord may be involved due to direct microbial invasion from contiguous sites or compression from the surrounding abscesses. Intramedullary microabscesses in upper spinal cord in previous reports has been attributed to contiguous spread from the brainstem. 4 A case with acute flaccid paraplegia and psoas abscess with pus culture growing Burkholderia pseudomallei was reported previously where the cord involvement was hypothesized to be secondary to ischemia. 11 The exact pathogenesis of lower cord involvement in our case is unclear. However, the presence of microabscesses implies direct infection of the cord. In view of the forthcoming history of visit to rice fields, percutaneous inoculation with hematogenous dissemination would be the probable mode of systemic spread. He had uncontrolled diabetes mellitus which is a risk factor for severe disease; the others being chronic renal and lung disease, alcohol abuse, and immunosuppression. 5
Infectious etiology must be considered in the differentials in any patient presenting with myelitis. Peripheral neutrophilic leucocytosis, neutrophilic pleocytosis in CSF, severe constitutional symptoms, and sepsis strongly suggest acute suppurative myelitis. Inflammatory features can be masked in elderly patients, especially with diabetes or immunocompromised state, leading to erroneous diagnosis and management. Blood and CSF neutrophilic leucocytosis and CSF hypoglycorrhachia were indicative of infection in our patient whereas lack of local symptoms and constitutional features were deceptive. Tuberculous myelitis is a strong consideration in an endemic region like India, although lymphocytic predominance in CSF is the rule. A marked elevation of CSF ADA as noted in this patient was shown to be useful in differentiating tuberculous from bacterial meningitis, though a direct comparison with neuromelioidosis was not done. 15
Coexistent pneumonia, genitourinary infection, extraaxial collections, and skull osteomyelitis should prompt evaluation for melioidosis. 3 Tracking of infection along white matter tracts, particularly, corticospinal tract and corpus callosum, and along the trigeminal nerve are defining features of cranial involvement in melioidosis. 4 A high index of suspicion for melioidosis should be maintained in the presence of rim-enhancing microabscesses, diffusion restriction and meningeal enhancement. 4 Early institution of antibiotics is required, especially in high risk patients when inflammatory features may be masked. Mortality reaches up to 50%, which can be reduced with early diagnosis and treatment. 3
Melioidosis is endemic in tropics with an average annual global incidence exceeding 160,000 cases. 16 Signs and symptoms can be non-specific and diagnosis can be missed when index of suspicion is low. Isolated myelitis should be recognized as a possible presentation of melioidosis although cranial and combined presentations are more common. While tuberculosis remains the commonest cause of infectious myelitis in India, 1 atypical clinical, CSF, and imaging features should prompt rapid evaluation and treatment for other infectious causes. Melioidosis which gained notoriety as the ‘Vietnamese time bomb’ after the Vietnam war, is indeed a ticking time bomb and should be identified promptly to prevent dissemination and mortality.
Footnotes
Authors’ Note
Signed Patient Consent Form: Informed consent for publication was obtained from patient’s relatives.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.