
Abstract
Jamestown canyon virus (JCV) is an arbovirus and is an under-recognized cause of mosquito-borne viral encephalitis. In this report we present a patient who presented with focal neurological deficits. Patient was initially evaluated for stroke. However, leptomeningeal enhancement on MRI and CSF studies were concerning for viral encephalitis. Brain biopsy and CSF sample from surgical site was positive for JCV IgM antibodies. Patients presenting with concern for viral encephalitis in endemic areas should undergo antibody testing for JCV to guide appropriate treatment.
Introduction
Arthropod-born illnesses are common in Michigan; these viruses can cause encephalitis, but due to their nonspecific presentation, the diagnosis is challenging. JCV is a rare cause of viral encephalitis and is easily missed as it is not routinely tested for. We present a case of Jamestown Canyon encephalitis that was diagnosed with surgical site CSF testing, and discuss the necessity for testing for it in endemic areas.
Case Report
A 79-year-old male presented to the ER with speech difficulty and left arm cramping lasting for 30 seconds. On evaluation, the patient returned to baseline and was sent home with a plan to follow up with their primary care physician for a transient ischemic attack work up. The patient returned to the ER after 1 day with subjective left arm numbness and weakness. Non-contrast CT head, CTA head and neck were negative. The patient was admitted to the hospital with preliminary diagnosis of stroke for further evaluation. Initial lab work was negative except ESR was 32, CRP 51.1. A brain MRI on day 3 showed T2 hyperintensity signal in right peri-Rolandic area with leptomeningeal enhancement on contrast (Figures 1, 2 and 3).
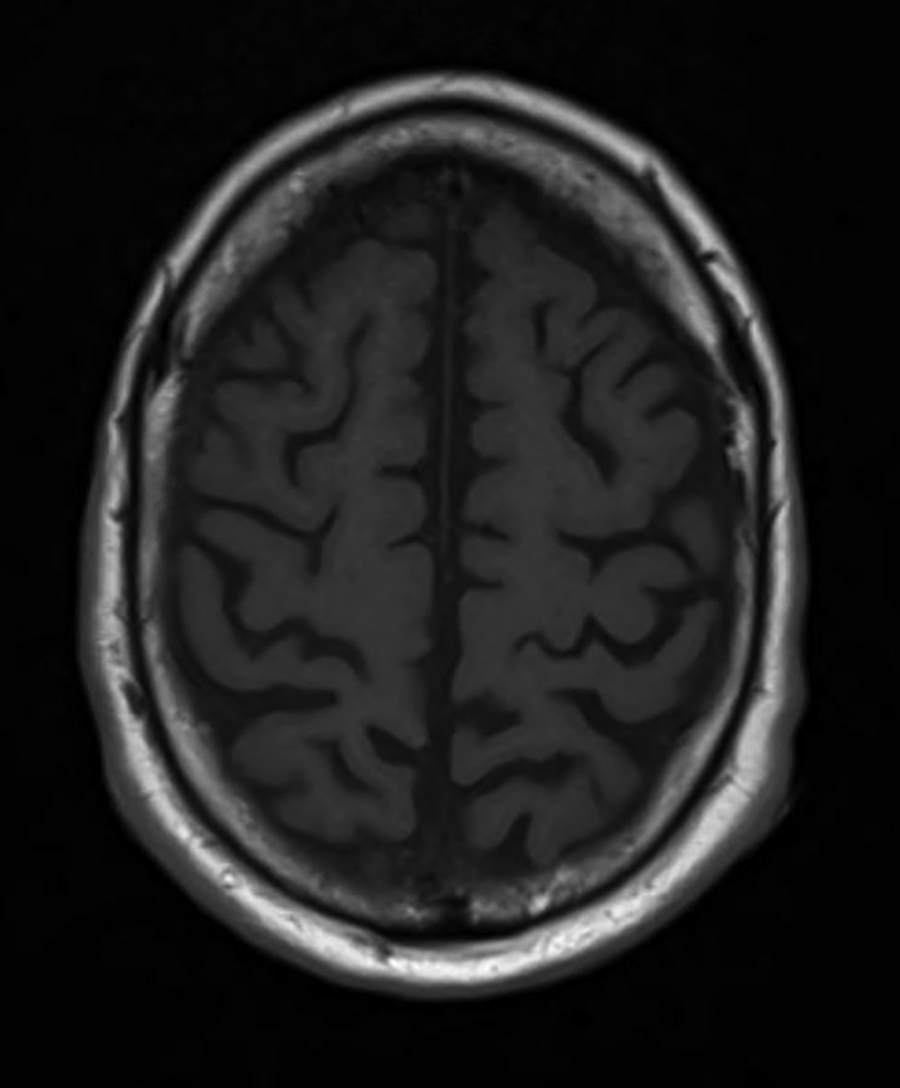
MRI T1 without contrast—normal.
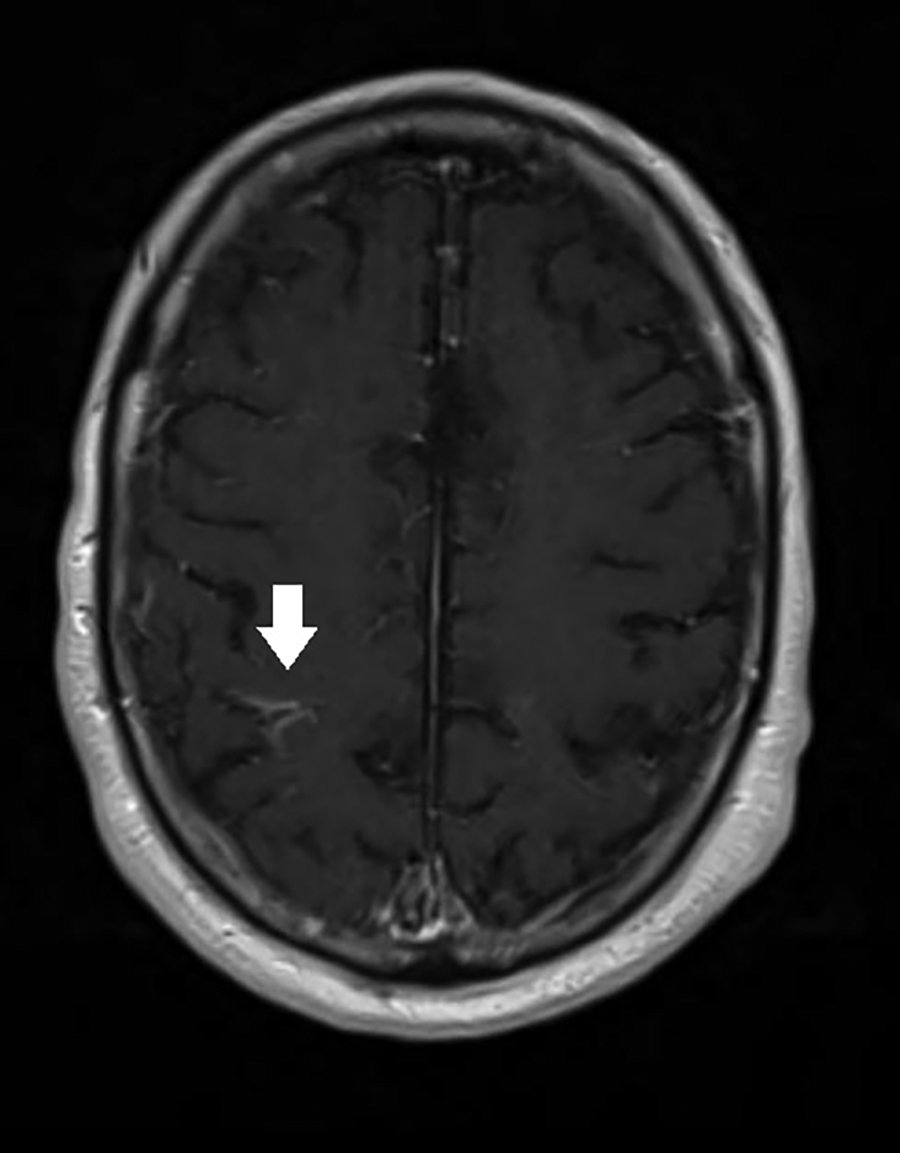
MRI T1 with contrast concerning for right peri-Rolandic leptomeningeal enhancement marked with arrow.
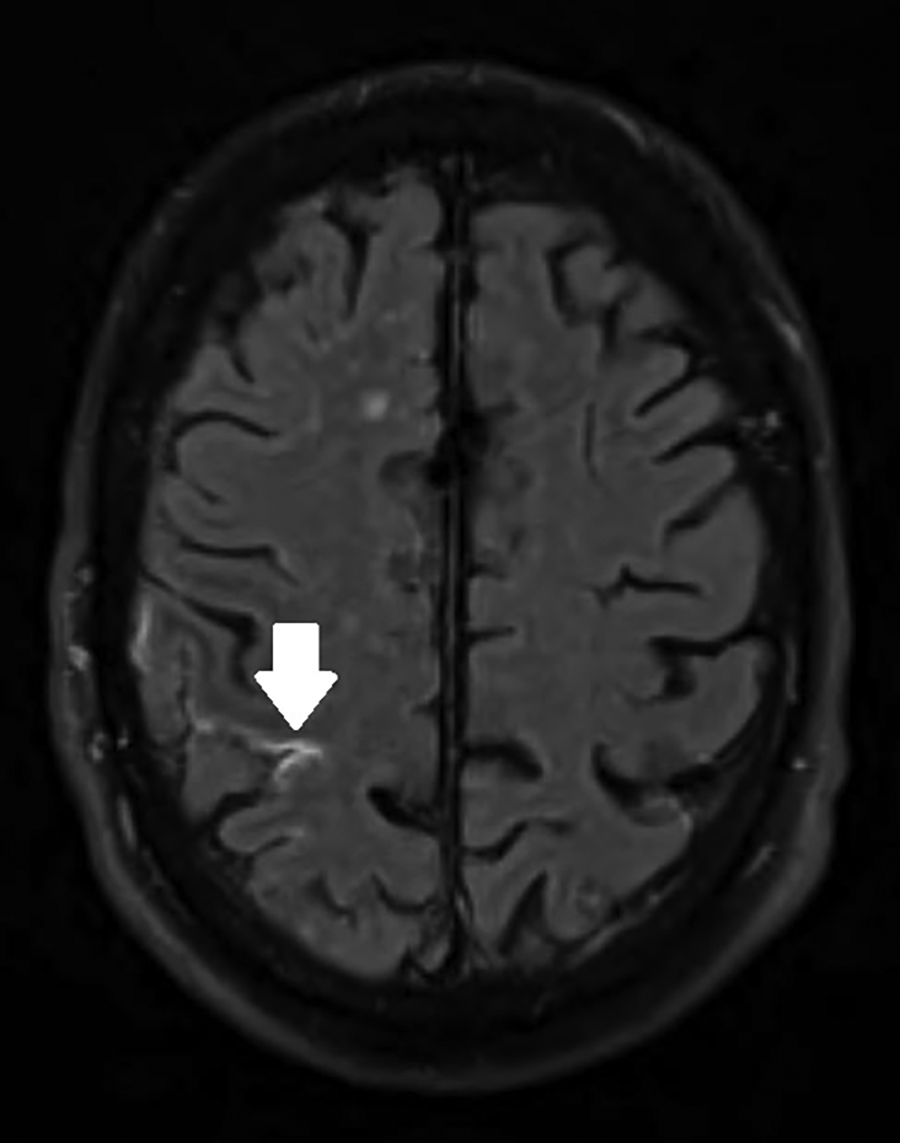
MRI T2 FLAIR concerning for right peri-Rolandic area hyperintensity marked with arrow.
EEG was negative for seizures, however showed lateralized rhythmic delta activity (LRDA) in the right frontal region with focal paroxysmal fast activity in the right temporal region (Figures 4 and 5). Patient later revealed history of 1-week of night sweats, weight loss, and lethargy. The patient recently stayed near a lake in the lower peninsula region of Michigan. At that time, differential diagnoses included infection, demyelinating disease, and malignancy, for which a spinal tap was ordered. Blood workup was sent to rule out autoimmune, vitamin deficiency, and sarcoidosis.
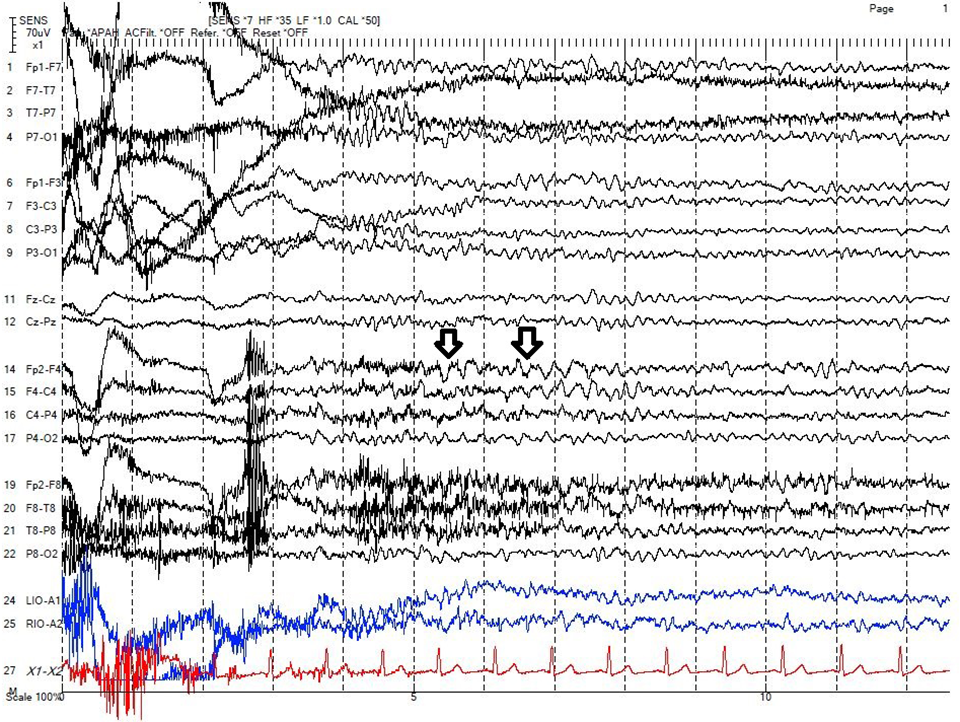
This EEG tracing shows a typical 4-5 second run of 3.5 Hz lateralized rhythmic delta activity (LRDA) over the right frontal region (F4), which is superimposed over an encephalopathic background, marked with multiple arrows.
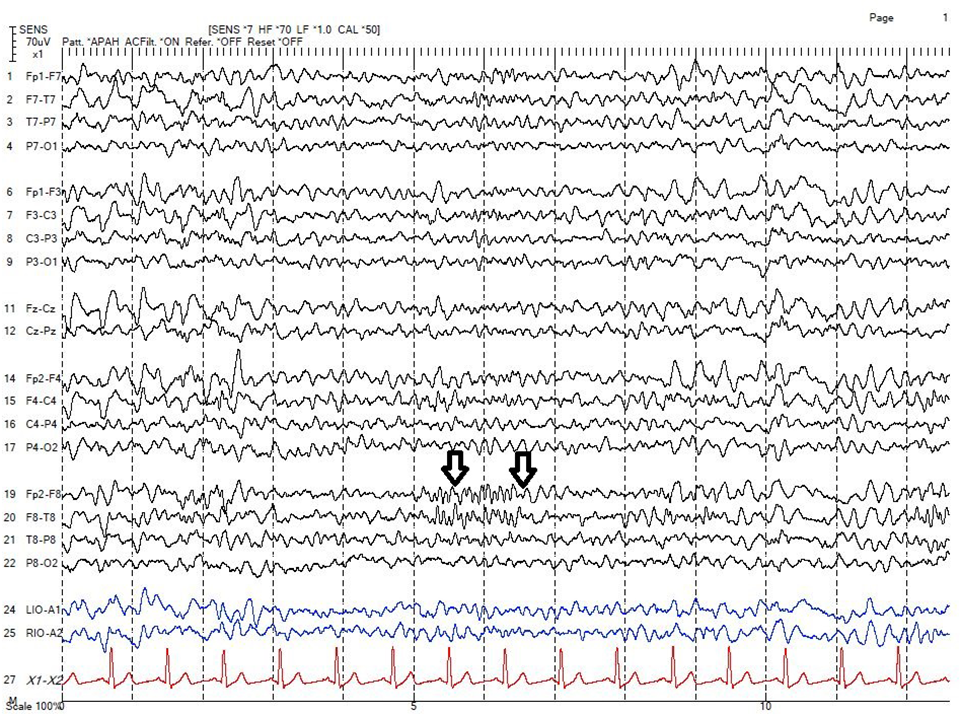
This EEG tracing shows a typical 1-2 second burst of right anterior temporal (F8) paroxysmal fast activity (PFA), which is superimposed over an encephalopathic background marked with multiple arrows.
Lumbar Puncture on day 4 revealed lymphocytosis, with elevated proteins and normal glucose (Table 1). Viral and bacterial cultures, HSV, Lyme, Syphilis, Eastern Equine, Western Equine, La Crosse, St. Louis’ virus was negative for IgG and IgM antibodies. Medical cytology, paraneoplastic panel and protein electrophoresis, autoimmune panel were also negative.
CSF Results on Day 4 and Day 11.
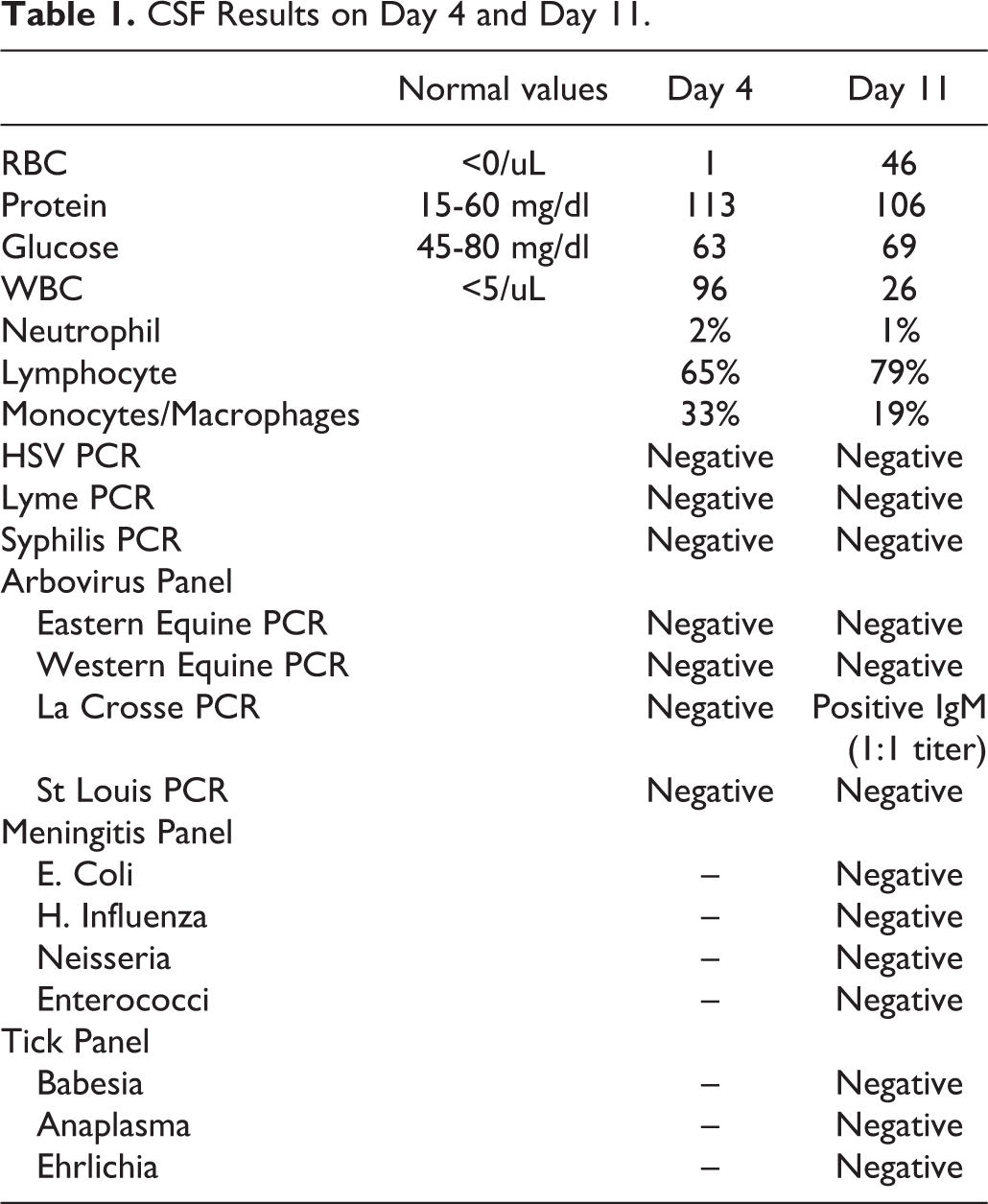
The patient continued to have waxing and waning left arm weakness with aphasia. MRI on day 10 revealed diffuse left cerebral hyperintensity with leptomeningeal enhancement (Figures 6, 7, and 8 respectively). Neurosurgery was consulted and a left frontal brain biopsy was performed. CSF lab work on day 11 showed lymphocytosis with elevated proteins as mentioned in Table 1. Meningitis panel PCR, including Neisseria, listeria, enterococci, HSV, H. Influenza, and E. Coli, was negative. Tick panel, including Lyme, Babesia, Anaplasma, and Ehrlichia, was negative. Repeat Arbovirus panel demonstrated 1:1 titer positive testing for the La Crosse virus IgM antibody. Brain biopsy revealed a reactive lymphocytic infiltration in the leptomeninges. The parenchyma showed microglial activation and microglial nodules without definitive neuronophagia. These features were most consistent with a viral meningoencephalitis (Figures 9 and 10). CSF sample from the biopsy site tested positive for Jamestown Canyon Virus IgM antibodies and Plaque Reduction Neutralization (PRNT) titer was >1:64. The patient was started on 3 days of high dose steroids due to concern for autoimmune encephalitis as CDC confirmation testing was awaited. The diagnosis was confirmed by the Center for Disease Control (CDC) via plaque reduction neutralization testing. The patient was discharged on day 14 after patient’s symptoms improved significantly.
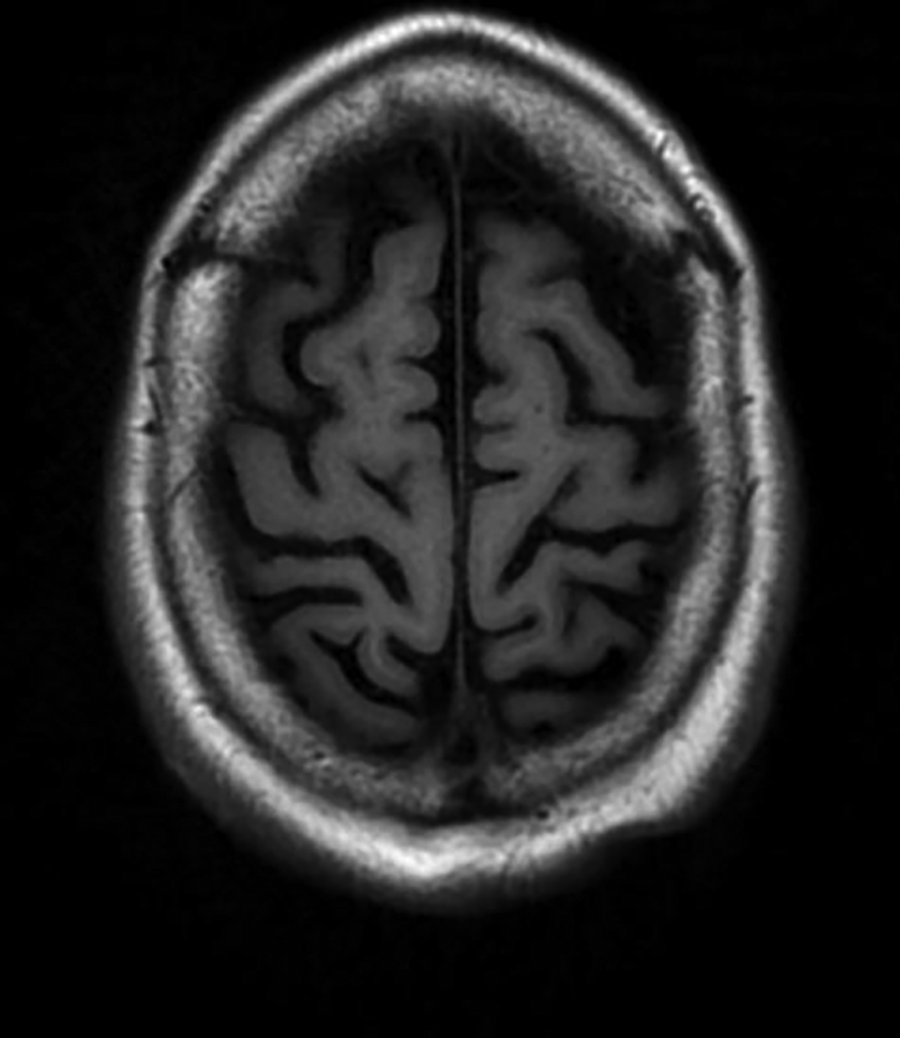
MRI brain without contrast—normal.
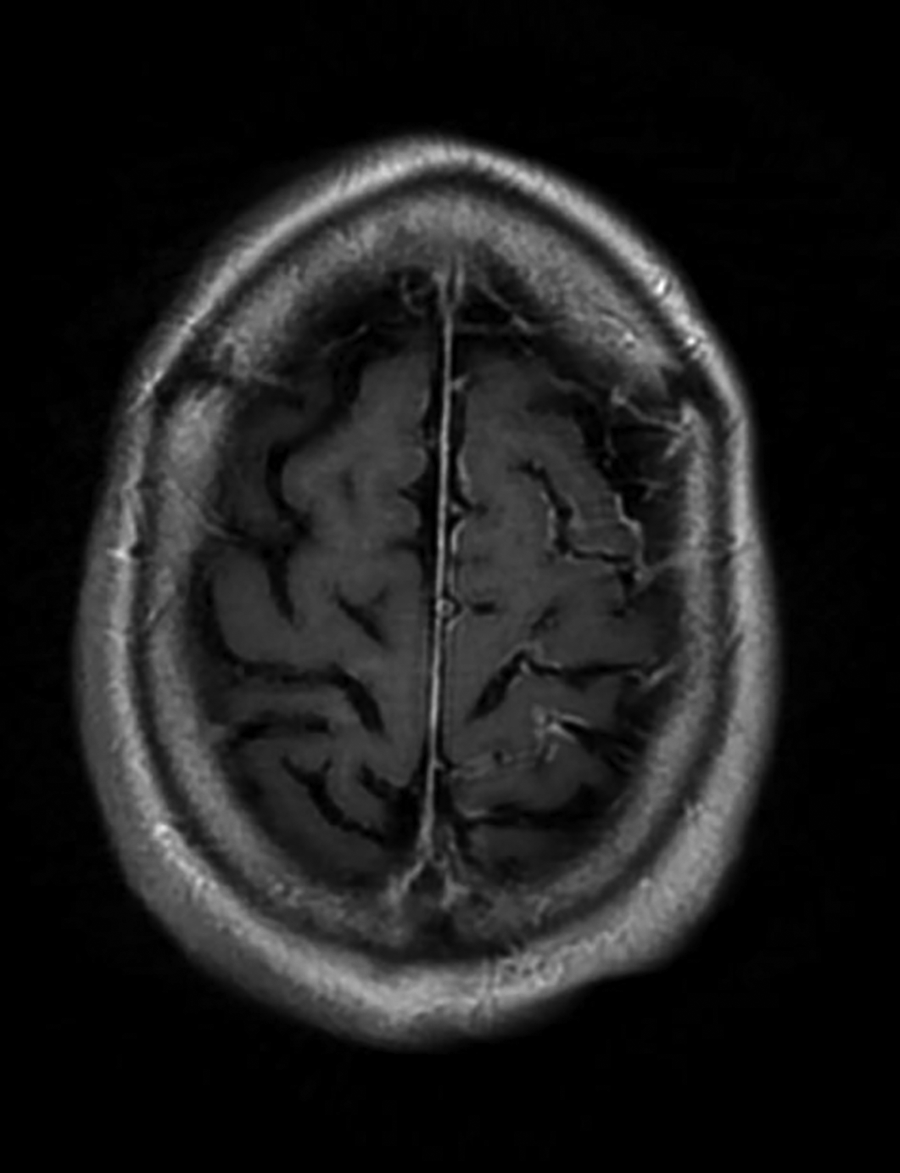
MRI brain with contrast concerning for diffuse leptomeningeal enhancement on left.
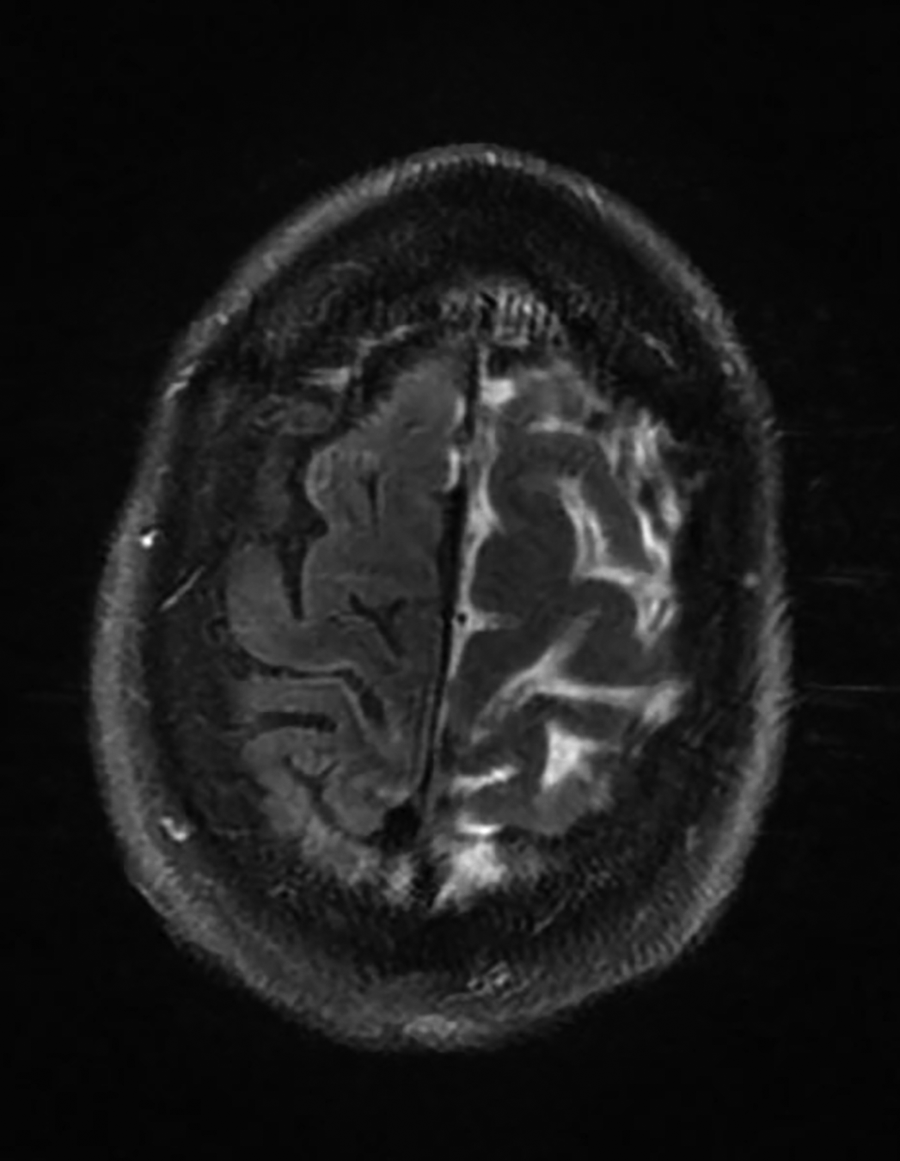
MRI brain T2 FLAIR concerning for diffuse left cerebral hyperintensity.
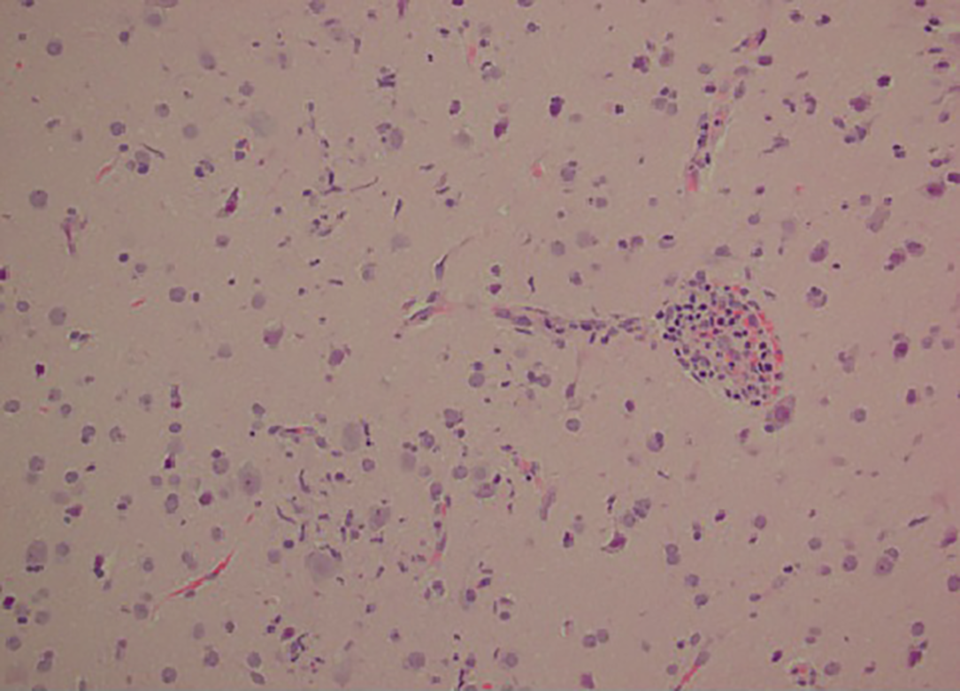
CNS cortex with a small vessel showing lymphocytic inflammation with infiltration of lymphocytes into the parenchyma. There is a microglial nodule adjacent to this vessel. No definitive neuronophagia was identified.
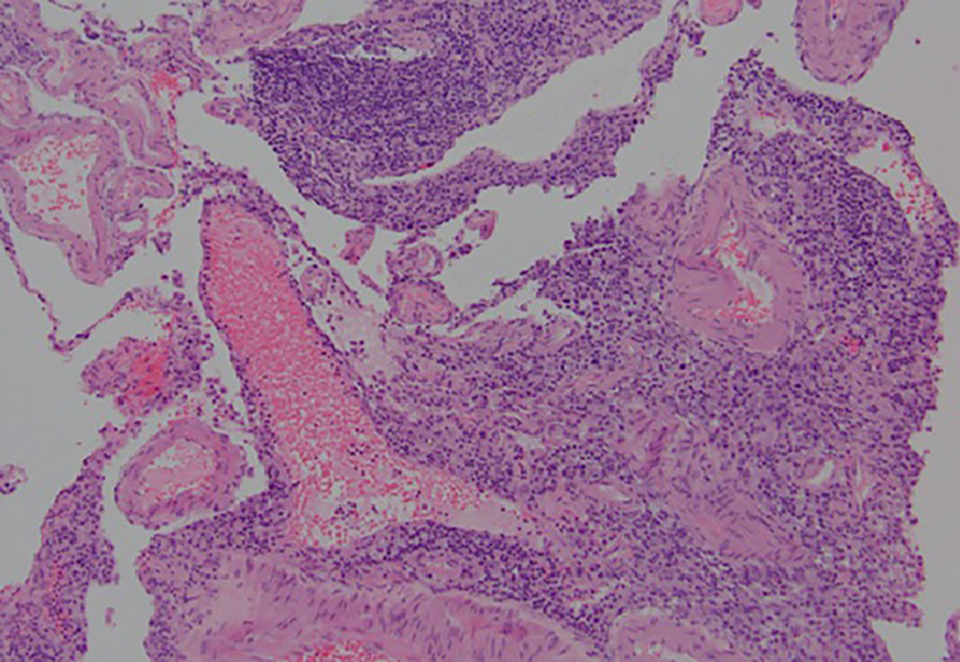
Diffuse lymphohistiocytic inflammatory infiltrate within the leptomeninges. These features are non-specific but are consistent with a viral pathogen.
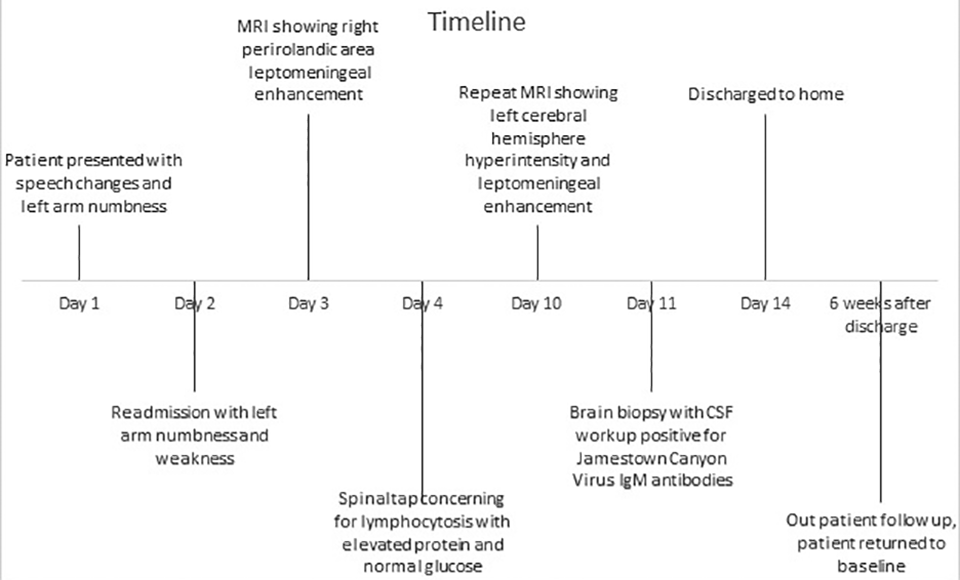
Timeline.
On outpatient evaluation, the patient had complete resolution of his symptoms and was back to baseline (Figure 11).
Discussion
Jamestown Canyon Virus is an RNA arbovirus from the California serogroup. 1 This virus was first isolated from Culiseta Inomata mosquitoes in Jamestown, Colorado in 1961. 2 It is a vector born disease, and mosquitos, like Aedes, Culex, and Coquillettidia, serve as its primary vectors. 3 In the 1960s, JCV related human infections were first described in forest workers in Wisconsin as a nonspecific minor illness. 2 The CDC reports 181 cases between 2009-2018; mainly in Wisconsin and Minnesota. Out of these, 121 had neurological symptoms. 4 Only 4 of these cases are from Michigan; 2 in 2018, 1 in 2019, and this being the 4th. 5 Most cases were reported between April and September; a period of active disease transmission via mosquito bites. 1
In Michigan, the white-tailed deer, Odocoileus Virginianus, has been studied as a primary host for JCV. 6 Infections related to JCV have been under-recognized and under-diagnosed in Michigan, as an older study suggested high neutralizing antibodies for JCV in the Michigan population. 6 A close relationship was noted in the distribution of tested individuals and the white-tailed deer population in the Lower Peninsula of Michigan. 6 Our patient also visited a lakeside in the lower peninsula with high populations of white-tailed deer.
Most cases of JCV are asymptomatic, however in documented cases, a wide range of symptoms have been noted, ranging from a mild febrile illness to severe encephalitis. 1 Historically, JCV cases have male predominance and most patients were immunocompetent. 3 Typical presentation includes headache, altered mental status, fever and occasional seizures. 7 Sweats and chills are less commonly reported. 8 A recent case from Manitoba, Canada reported recurrent unilateral headaches with speech difficulties, mimicking a migraine with aura. 9 Our patient presented with numbness and tingling of one side, waxing and waning speech difficulty, a viral prodrome of lethargy and night sweats.
Lymphocytosis is also seen on spinal tap. A recent case series showed elevated white cell count with lymphocyte predominance in 4 out 7 cases. 8 Patients with viral encephalitis are at risk of acute seizures. 10 Data regarding JCV encephalitis causing seizures is scarce. A recent case report from Quebec, Canada was the first to document new onset refractory status epilepticus (NORSE) with JCV encephalitis. 7 One possible explanation for waxing and waning symptoms in our patient could be explained by seizures, however no active seizures were noted on scalp EEG.
MRI imaging performed for suspected common viral encephalitis can have specific patterns of image-related changes, especially if seen with CSF pleocytosis. 11 In cases of JCV encephalitis, leptomeningeal enhancement (LME) can be seen, however some cases can have normal MRI. 1 In our patient, leptomeningeal enhancement was observed. Interestingly this was initially noted on the right hemisphere and later imaging showed LME which was limited to the left hemisphere.
A recent JCV encephalitis case report showed a similar pattern, where the initial MRI was unremarkable, however repeat MRI after few days showed significant bilateral LME. 9 These changes are atypical and, in our patient, this occurred with a rapid resolution of changes in one hemisphere. These changes can be due to the neuro-invasive nature of the virus and disruption of the blood-leptomeningeal barrier. Positive sampling for JCV titers from biopsy showed a viral meningoencephalitis pattern, supporting our hypothesis. However, data regarding MRI changes in JCV encephalitis is limited which makes it difficult to correlate these changes with confidence.
JCV encephalitis is diagnosed on serology with confirmatory testing through viral neutralizing antibodies based on viral serology. Cross-reactivity with La Crosse antibodies has been noted with cases of JCV. 12 Commercial testing is limited without help from local health departments and the CDC.
Currently, treatment for JCV is limited to supportive care but recent case reports have shown some efficacy with Ribavirin. One patient with JCV encephalitis with NORSE was given ribavirin which improved seizure activity. 7 An immunocompromised transplant patient diagnosed with JCV encephalitis, was placed on Ribavirin for 6 weeks resulting in significant improvement in memory and cognition. 3 Following general mosquito-based prevention can decrease the incidence of this disease. 4
Conclusion
Jamestown Canyon virus has been associated with encephalitis, and it is difficult to diagnose, as patients may present with nonspecific symptoms. However, we recommend testing patients for JCV if they present with signs and symptoms of encephalitis, and a spinal tap concerning lymphocytosis in endemic areas (Wisconsin, Minnesota, and lower peninsula of Michigan). This disease is rare, but early diagnosis can prevent additional testing for noninfectious etiology.
Footnotes
Authors’ Note
Prior to submission, verbal consent was taken from the patient and his family. According to Spectrum Health IRB, “A case report that does not meet the definition of research and is not subject to IRB oversight.” For this reason, our case report did not receive IRB review at our institution.
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.