
Abstract
Embolization in new territories (ENT) is a known complication of mechanical thrombectomy with incidence dependent upon a variety of procedural factors. We present 2 cases of anterior circulation to posterior circulation ENT. These cases were managed with manual aspiration thrombectomy with excellent radiographic and clinical outcome. We present the available literature involving ENT along with our experience in management.
Keywords
Introduction
One challenge of mechanical thrombectomy is to avoid emboli in previously unaffected territories, or embolization in new territories (ENT). ENT can result in an infarct in new territory (INT). These can be classified based on size and whether the catheter was manipulated across the territory ostium. 1 The frequency of INT is estimated to be 1-8.6 percent. 2 Most INT (35%) have been shown to be small (<2 mm) and not related to catheter manipulation across the new infarct territory ostium. 3 Large INT (>20 mm) has been shown to be relatively rare with a rate of 5%. 3 The rate of ENT is dependent on a variety of factors including choice of endovascular device, 4 incorporation of balloon guided catheters,5,6 and method of procedural sedation. 7 Trans-circulation ENT is a rare entity and optimal management is unknown. We present 2 cases of trans-circulation ENT to the posterior cerebral artery (PCA) territory through the posterior communicating artery (PComm), along with our experience in addressing this complication.
Case Summary
Patient 1
A patient in their nineties with a past medical history of hypertension and pulmonary embolus not on anticoagulation presented with right sided weakness and aphasia. They were last seen well 6 hours prior to evaluation and received a National Institutes of Health Stroke Scale (NIHSS) of 11. CT of the brain demonstrated a left frontal hypodensity with an Alberta Stroke Program Early CT Score (ASPECTS) of 7. CT angiogram of the head and neck showed a left internal carotid artery (ICA) terminus and a left middle cerebral artery, M2 segment occlusion. The patient subsequently underwent cerebral angiography with recanalization of the left ICA/MCA achieved after 2 passes of manual aspiration thrombectomy with TICI 2b reperfusion. (Figure 1) The procedure was complicated by a left posterior cerebral artery (PCA) ENT visualized on a post-thrombectomy angiography. This new occlusion was addressed via the vertebral and basilar artery with TICI 3 recanalization achieved through manual aspiration thrombectomy. MRI Brain following the procedure showed a left temporal infarction in the posterior left MCA territory as well as punctate infarction in the right MCA territory. (Figure 2) Upon discharge, the patient’s NIHSS was 8 with improved right sided weakness and mild expressive aphasia.
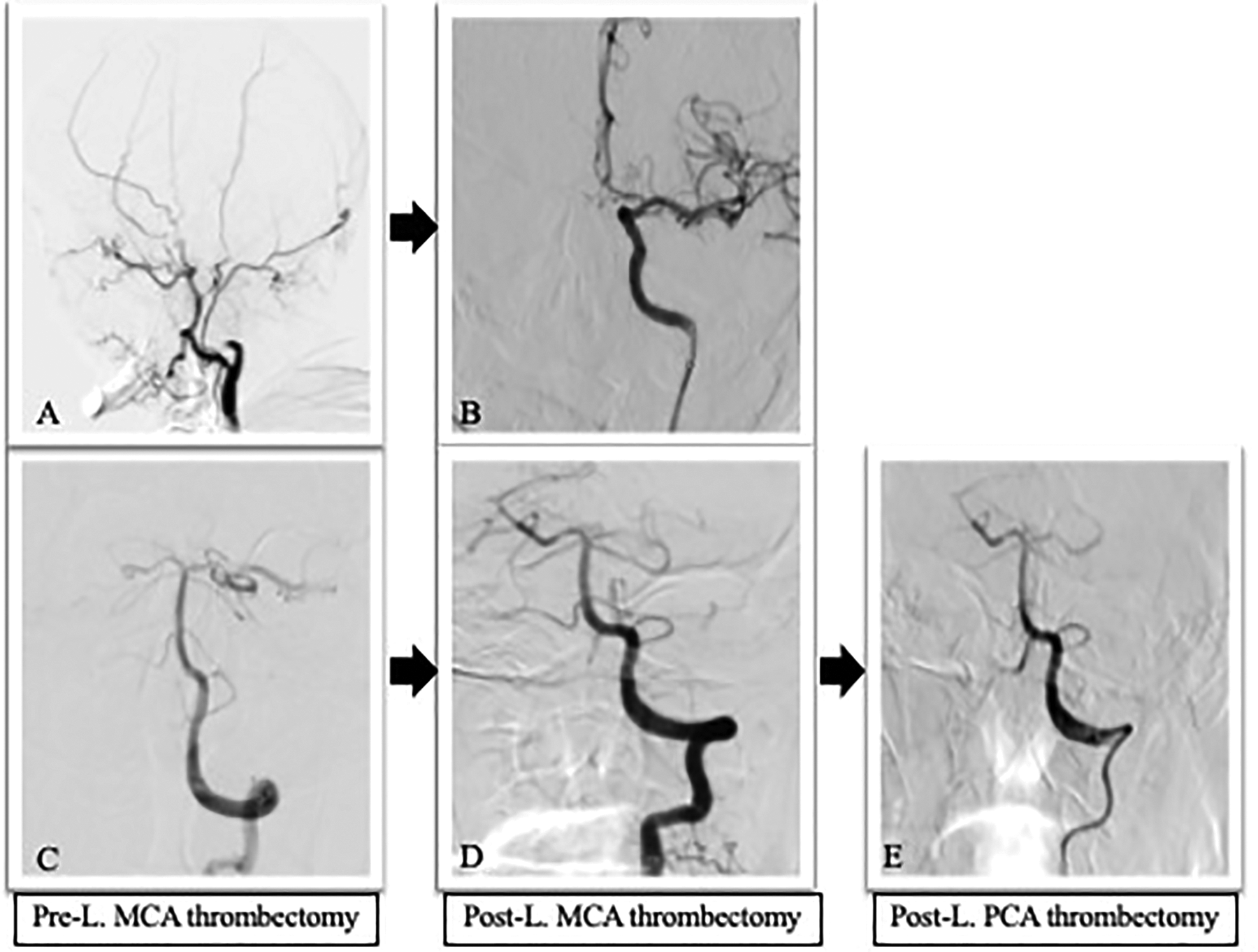
A. Left common carotid sagittal plane demonstrating left common carotid occlusion pre-thrombectomy. B. Left Internal Carotid AP view demonstrating TICI2B reperfusion of the left MCA. C. Left vertebral artery AP view showing patent left PCA pre-thrombectomy. D. Left vertebral artery AP view showing left PCA occlusion post- left MCA thrombectomy. E. Left vertebral artery AP view showing TICI3 reperfusion of the left PCA following left PCA thrombectomy.
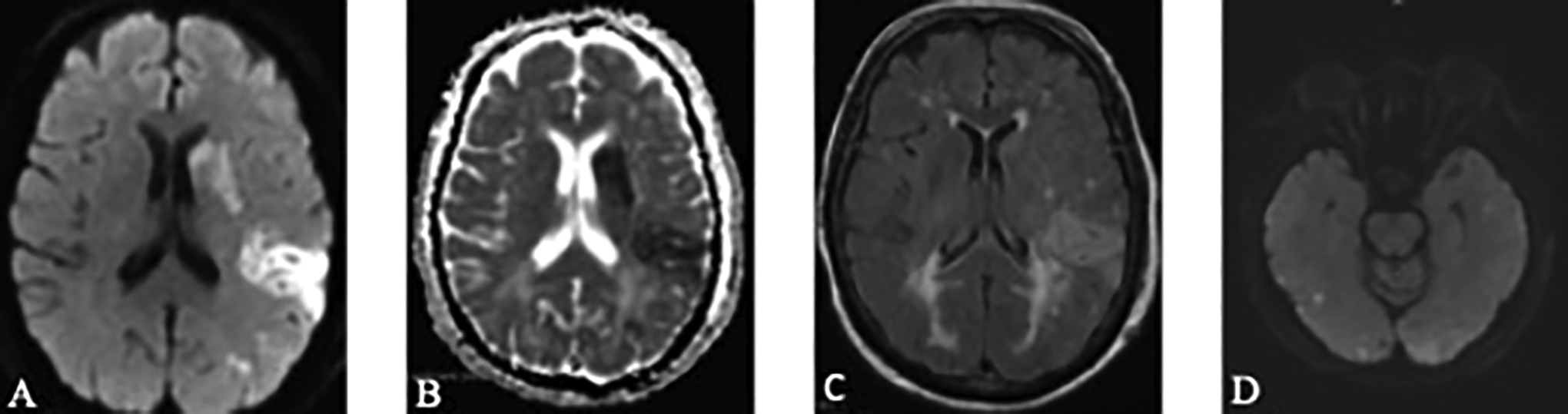
A. Diffusion weighted imaging showing left temporal infarction post-thrombectomy. B. apparent diffusion coefficient post-thrombectomy. C. T2 FLAIR post-thrombectomy. D. Diffusion weighted imaging post-thrombectomy showing infarction in the left posterior MCA territory as well as punctate infarction in the right temporal lobe, right MCA territory.
Patient 2
A patient in their sixties with a past medical history of hyperlipidemia presented with left sided weakness and neglect. They were last seen well 7 hours prior to evaluation and received an NIHSS of 7. CT brain showed an ASPECTS of 7 with a right frontal hypodensity. CT angiogram of the head and neck was performed which showed a right ICA occlusion and a right middle cerebral artery (M1 segment) occlusion with a patent fetal right PCA. Cerebral angiography confirmed a right ICA occlusion. (Figure 3) The right M1 occlusion was selected and manual aspiration thrombectomy was performed with TICI 2b recanalization. Following aspiration, angiography revealed a new right PCA occlusion. The right PCA occlusion was addressed with a trans-circulation approach via the right PComm and TICI 2b recanalization was achieved with the Solitaire device. MRI Brain following the procedure showed a right temporal and right occipital lobe infarction in the right MCA and right fetal PCA territory respectively. (Figure 4) Upon discharge, the patient’s NIHSS was 2 for left sided homonymous hemianopsia.
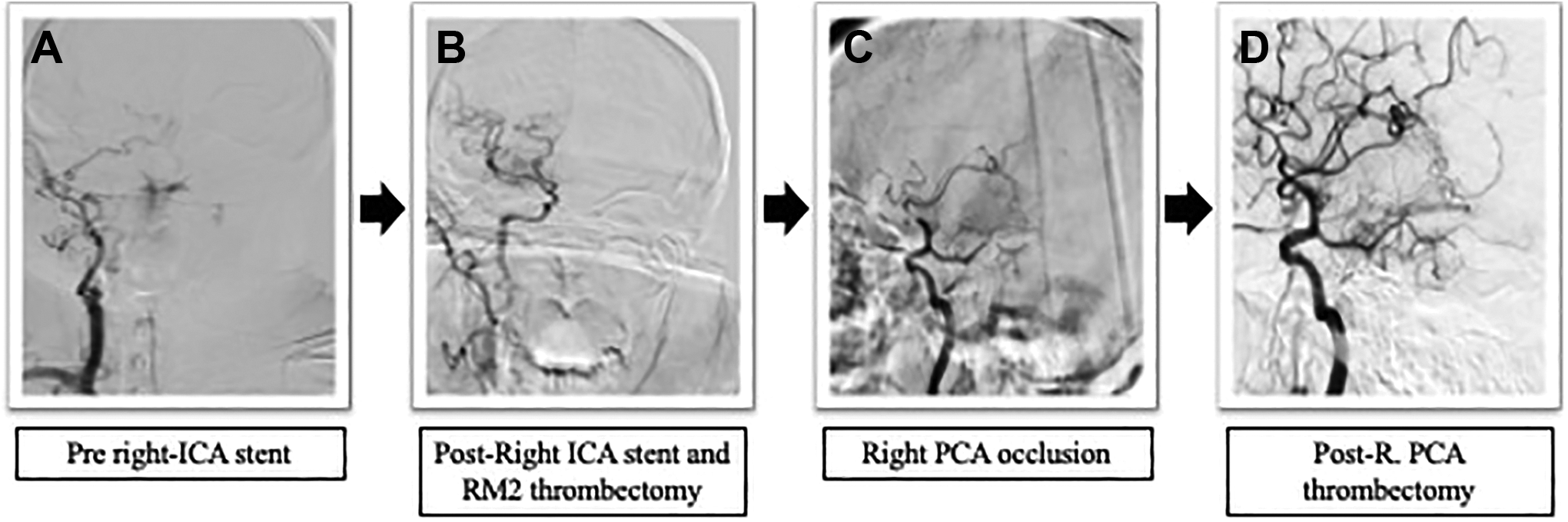
A. Right common carotid AP view demonstrating right internal carotid occlusion pre-thrombectomy. B. Right internal carotid AP view following right carotid stent and right M2 thrombectomy showing TICI2B reperfusion of the right MCA. C. Right internal carotid sagittal view demonstrating right PCA occlusion post- right MCA thrombectomy. D. Right internal carotid sagittal view showing TICI2B reperfusion following right PCA thrombectomy.
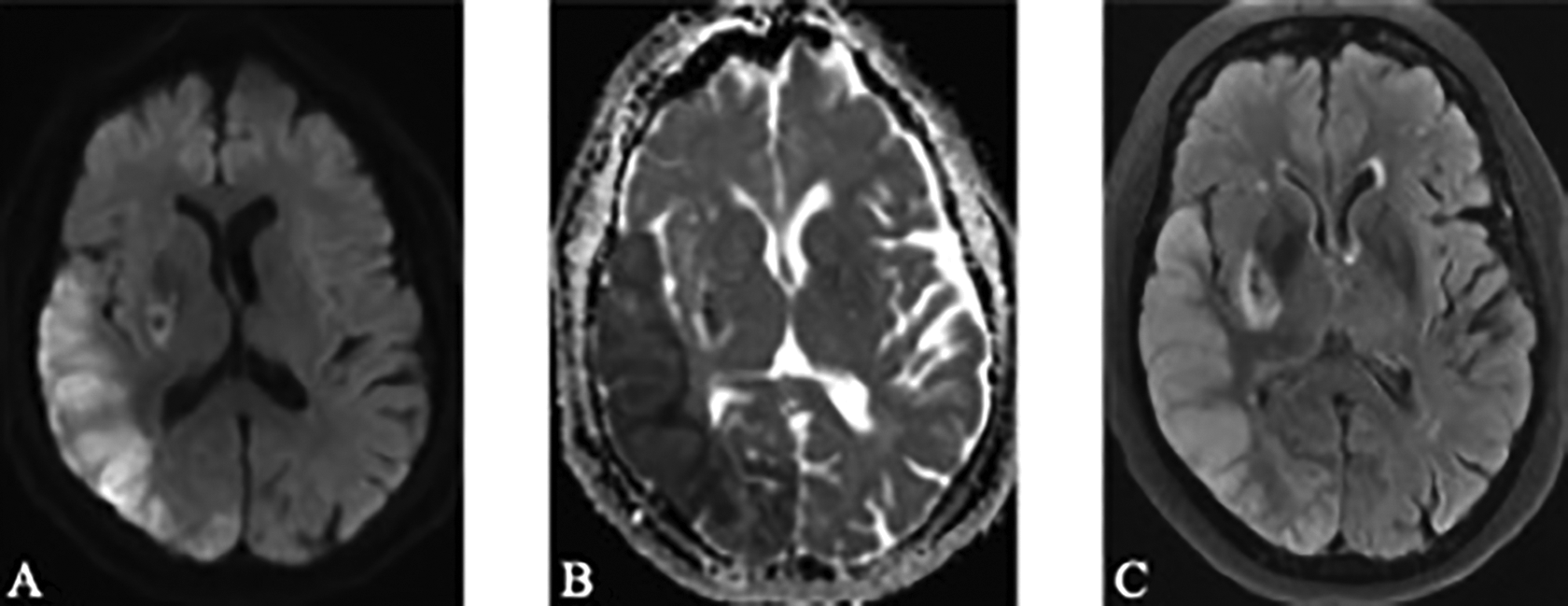
A. Diffusion weighted imaging showing right temporal and right occipital pole infarctions post-thrombectomy in the right MCA and right fetal PCA territory, respectively. B. Apparent Diffusion Coefficient post-thrombectomy. C. T2 FLAIR post-thrombectomy.
Discussion
The 2 cases described in this paper highlight unique instances of anterior to posterior circulation ENT. We show that successful recanalization can be achieved with aspiration thrombectomy by approaching the target lesion through an anterior or posterior circulation approach. ENT is a well-documented complication of endovascular intervention for acute ischemic stroke. 8
There have been many attempts to mitigate distal emboli in catheter-based angiography. In vitro studies have shown that rates of distal embolization are affected by catheterization technique, equipment, and the mechanics of emboli. 9 It has been shown that flow arrest secondary to balloon catheters leads to less clot fragmentation, distal emboli, and improved reperfusion.10,11
This is corroborated in clinical practice as well. A meta-analysis by Brinjikji et al showed less clot fragmentation and distal embolization with balloon guided catheters during mechanical thrombectomy. 5 Stampfl et al found that in 31 patients with ICA occlusions, using a combination of balloon catheter and distal aspiration through an intermediate catheter avoided ENT. 6 The benefit of flow arrest is further supported by the increased prevalence of distal emboli with thrombectomy in the posterior circulation compared to the anterior circulation. This is hypothesized to be due to lack of flow arrest when performing thrombectomy of the posterior circulation. 4 In one study, proximal or distal protected stent retrieval prevented ENT during retraction of thrombus, but not to the immediate distal territory. 7
It has been proposed that intravenous thrombolysis pretreatment before mechanical thrombectomy may reduce the incidence of INT due to creation of a fibrinolytic state.1,12 A recent study by Goyal et al did not show an independent association of intravenous thrombolysis with INT. 13 It did suggest that posterior circulation occlusions are more likely to have INT following mechanical thrombectomy. In a separate study, pretreatment with intravenous thrombolysis again failed to show an association with rate of INT. 3 At this time, the association of pretreatment intravenous thrombolysis prior to mechanical thrombectomy and rates of ENT remains unclear.
There has been limited evidence that conscious sedation compared to general anesthesia led to a higher rate of ENT. 7 The theory is that patients under conscious sedation often move during the painful mobilization and retraction of the thrombus increasing the risk of embolization. A metanalysis incorporating the results of the AnStroke and GOLIATH trial failed to show a statistically significant correlation between type of anesthesia and rates of embolism to new territory. 14
Balloon guided catheters were not utilized for the cases we report in this paper. Perhaps utilization would have prevented ENT. In addition, perhaps utilization of pre-procedure imaging could be helpful. For example, patient 2 had a pre-procedure imaging CT angiogram of the head that revealed a large right Pcomm. This could alert the proceduralist to take greater care in preventing ENT or necessitating a higher degree of surveillance on post-procedure runs. Patient 2 had a fetal PCA while patient 1 had normal variation. It is uncertain at this time whether anatomical variation can affect the prevalence of ENT. Management of ENT or distal embolus is uncertain and depends on a proceduralists’ risk/benefit calculation. When a new embolus results, recanalization options include use of an aspiration catheter, stentriever as well as intra-arterial tPA. 15 In our case series, both patients with ENT were managed with aspiration mechanical thrombectomy of the ENT with excellent outcome. Future studies will be necessary to determine both mechanism of ENT and therapeutic approach to ENT.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.