
Abstract

A 59-year-old woman presented with a vesicular rash on her right hemiface (Figure 1A). She was treated with valaciclovir for presumed varicella-zoster virus (VZV) with resolution of her skin lesions. One month later, she returned with acute vision loss of the right eye. Slit-lamp examination revealed anterior uveitis involving the right eye. Cerebrospinal fluid analysis revealed a lymphocytic pleocytosis (10 total nucleated cells) with normal protein and glucose. MRI brain demonstrated T2 hyperintensity of the right spinal trigeminal nucleus (Figure 1B) and enhancement of the proximal optic nerve sheath suggestive of optic perineuritis (Figure 1C). Following primary infection, VZV may remain dormant in sensory ganglia and can reactivate in older adults in the setting of immunosenescence. Herpes zoster ophthalmicus (HZO) describes VZV reactivation within the ophthalmic division of the trigeminal nerve. Rarely, HZO causes inflammation of the optic nerve or sheath, requiring prompt treatment with antiviral and anti-inflammatory agents to preserve vision. The patient’s vision improved with intravenous acyclovir and methylprednisolone.
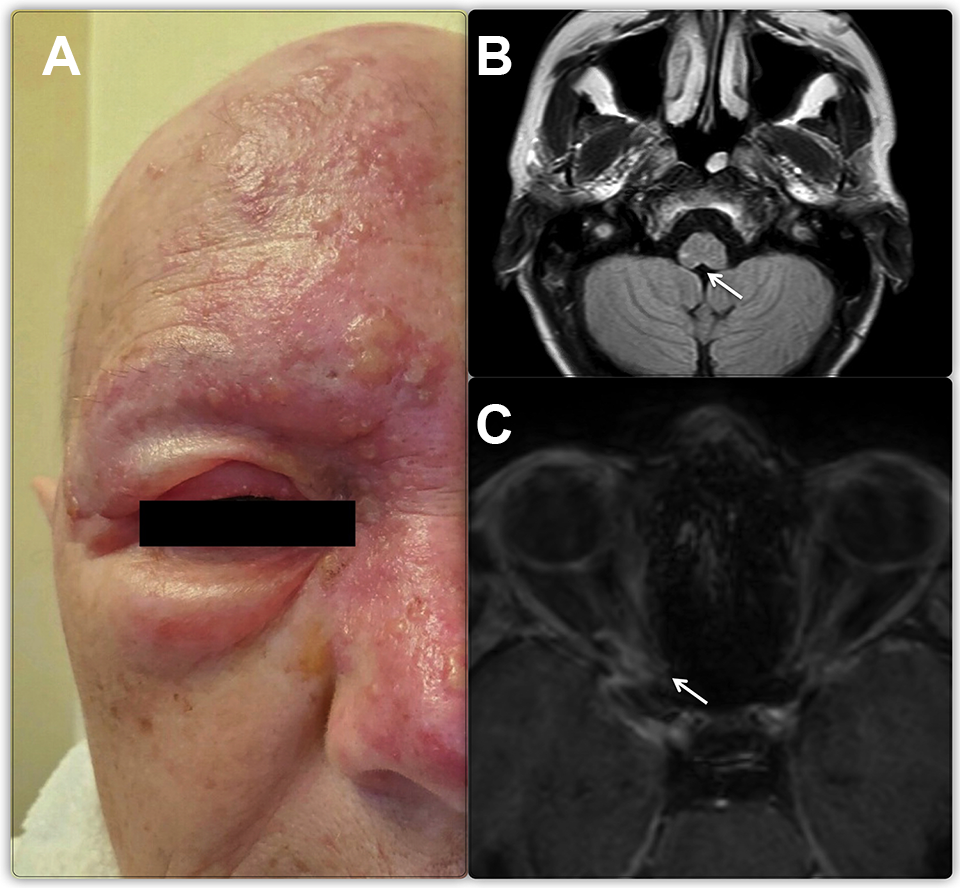
A, Vesiculo-papular rash in the distribution of the ophthalmic branch of trigeminal nerve. B, Axial FLAIR sequence of MRI brain showing hyperintensity of the right spinal trigeminal nucleus (white arrow). C, Axial T1 post-contrast MRI of orbits showing enhancement of the proximal optic nerve sheath suggestive of perioptic neuritis (white arrow).
Footnotes
Declaration of Conflicting Interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.