
Abstract
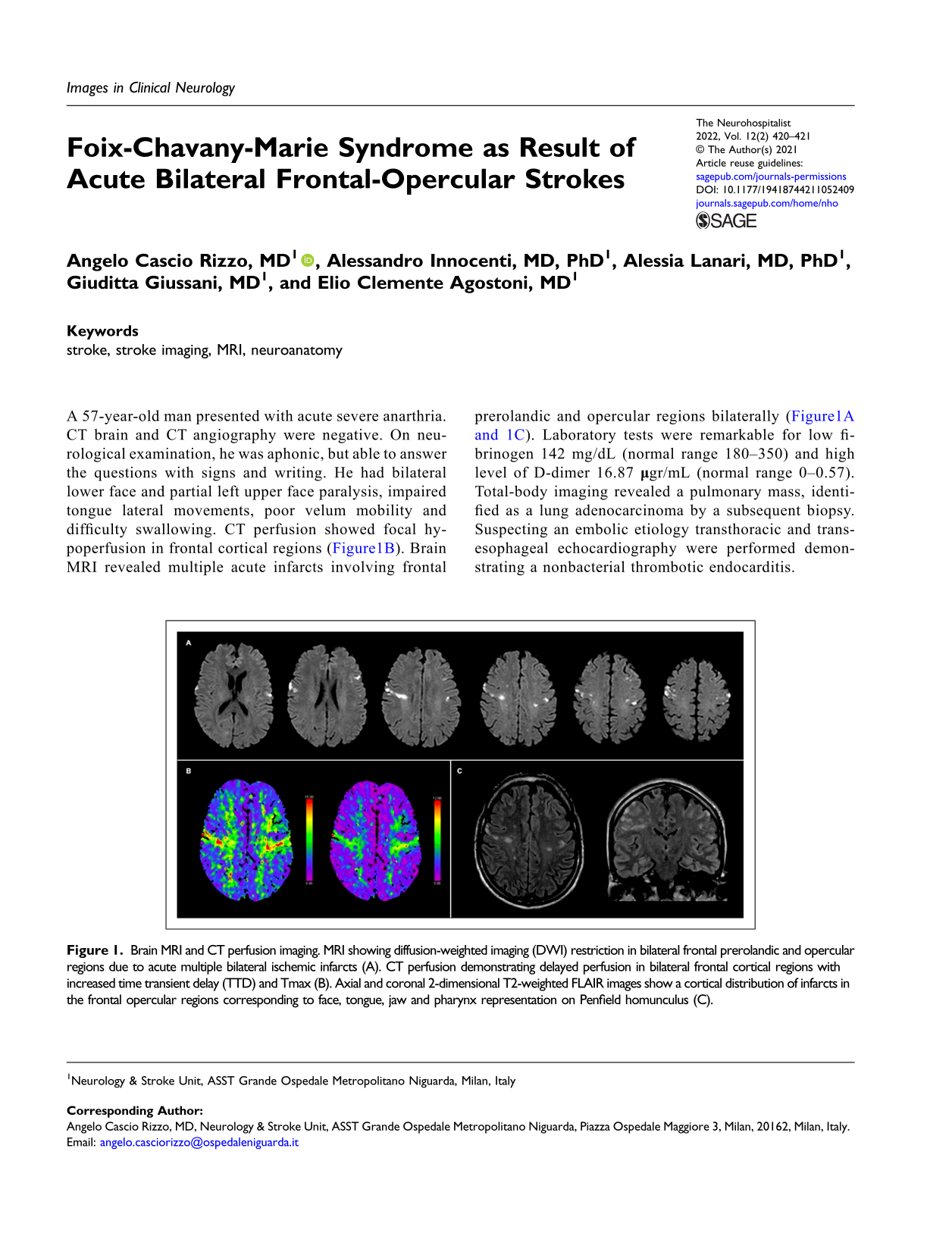
A 57-year-old man presented with acute severe anarthria. CT brain and CT angiography were negative. On neurological examination, he was aphonic, but able to answer the questions with signs and writing. He had bilateral lower face and partial left upper face paralysis, impaired tongue lateral movements, poor velum mobility and difficulty swallowing. CT perfusion showed focal hypoperfusion in frontal cortical regions (Figure1B). Brain MRI revealed multiple acute infarcts involving frontal prerolandic and opercular regions bilaterally (Figure1A and 1C). Laboratory tests were remarkable for low fibrinogen 142 mg/dL (normal range 180–350) and high level of D-dimer 16.87 Brain MRI and CT perfusion imaging. MRI showing diffusion-weighted imaging (DWI) restriction in bilateral frontal prerolandic and opercular regions due to acute multiple bilateral ischemic infarcts (A). CT perfusion demonstrating delayed perfusion in bilateral frontal cortical regions with increased time transient delay (TTD) and Tmax (B). Axial and coronal 2-dimensional T2-weighted FLAIR images show a cortical distribution of infarcts in the frontal opercular regions corresponding to face, tongue, jaw and pharynx representation on Penfield homunculus (C).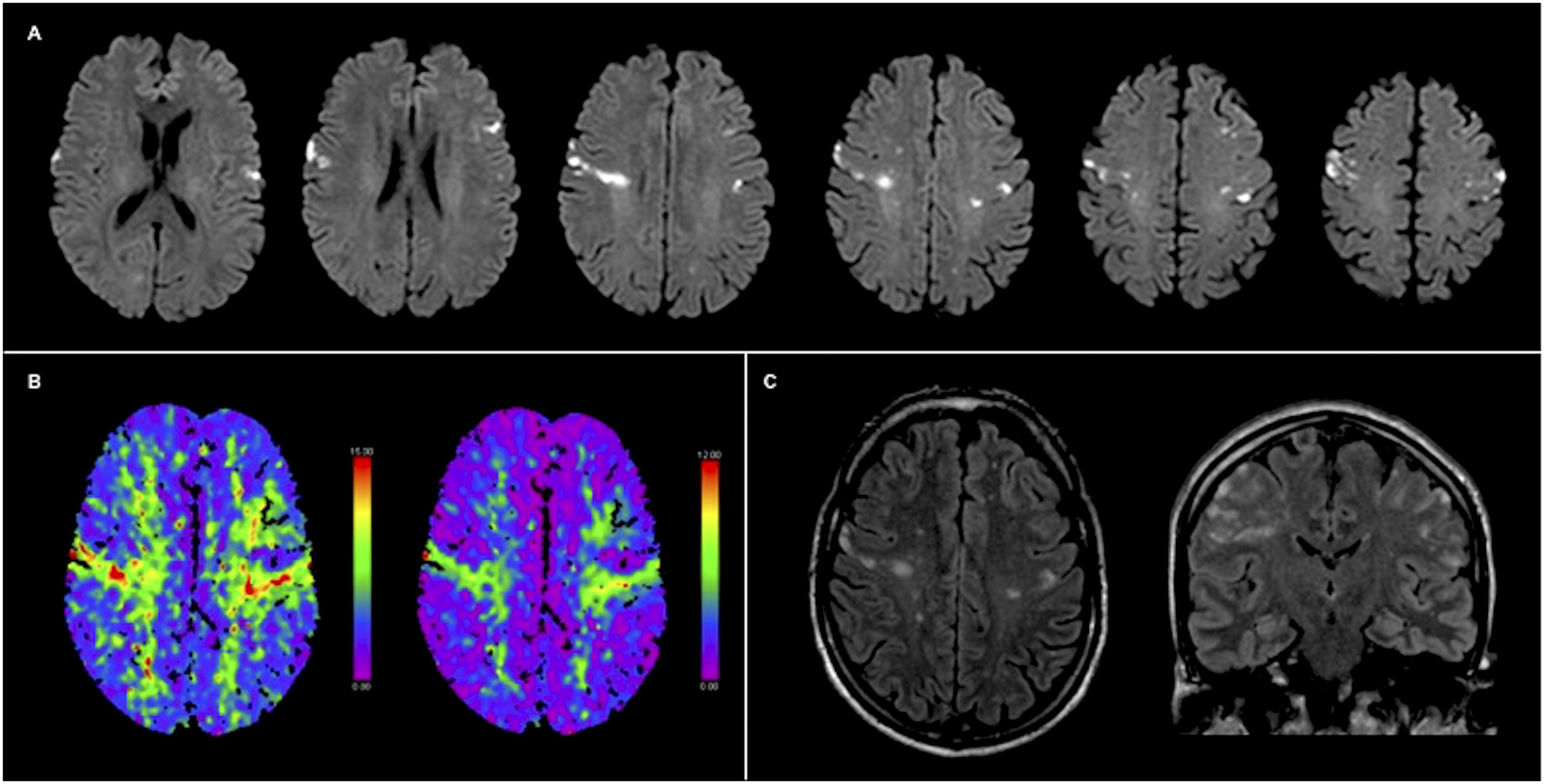
Foix-Chavany-Marie syndrome (FCMS) or bilateral anterior opercular syndrome is the cortical form of pseudobulbar paralysis, described as a facio-labio-glosso-pharyngo-laryngo-brachial paralysis with autonomic-voluntary dissociation. 1 The syndrome results from interruption of cortico-nuclear pathways from the frontal operculum cortex to the V, VII, IX, X, XII cranial nerve nuclei in both hemispheres. 2 The main etiology of FCMS is the vascular one. It is most frequently reported as the consequence of consecutive, multiple, separate vascular lesions (ischemic or hemorrhagic strokes) in anterior frontal opercula and subcortical insula regions of both hemispheres.2,3
Acute onset without a history of one or more contralateral strokes is unusual. Our case is a rare example of simultaneous bilateral opercular infarcts presenting with acute cortical form of pseudobulbar syndrome.4,5
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest concerning the research, authorship, and publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Informed Consent
The patient gave his consent to the publication of the data.
Disclosure
A. Cascio Rizzo, A. Innocenti, A. Lanari, G. Giussani, and E.C. Agostoni report no disclosures.
Contributorship
ACR concepted and drafted the manuscript and the figures, acquired data and worked up the clinical case as physician of care. AI concepted the manuscript and the figures and worked up the clinical case as physician of care. AL worked up the clinical case as physician of care and provided revision of the manuscript. GG provided revision of the manuscript. ECA concepted, supervised and planed the manuscript, and provided revision of the manuscript.