
Abstract
Paroxysmal hypothermia (PH) is a rare syndrome of stereotyped episodes of hypothermia, bradycardia, and altered mental status occurring in patients with hypothalamic lesions. Prior cases have mentioned bradykinesia, ataxia, and dysarthria, but parkinsonism has not been described as a specific feature of PH. We report two patients, an adult and a child, who developed PH after suprachiasmatic tumor resection, both with clinical presentations notable for prominent parkinsonian features despite no evidence of parkinsonism during the intervening months and years. We propose a diagnostic algorithm and scoring tool to aid in the clinical diagnosis of PH presenting as parkinsonism.
Keywords
Introduction
Paroxysmal hypothermia (PH) is a rare syndrome of stereotyped episodes of hypothermia, bradycardia, and altered mental status which has been previously reported in patients with hypothalamic lesions. We report two patients, an adult and a child, who developed PH after suprachiasmatic tumor resection, both with clinical presentations notable for parkinsonism.
Case Series
Case #1
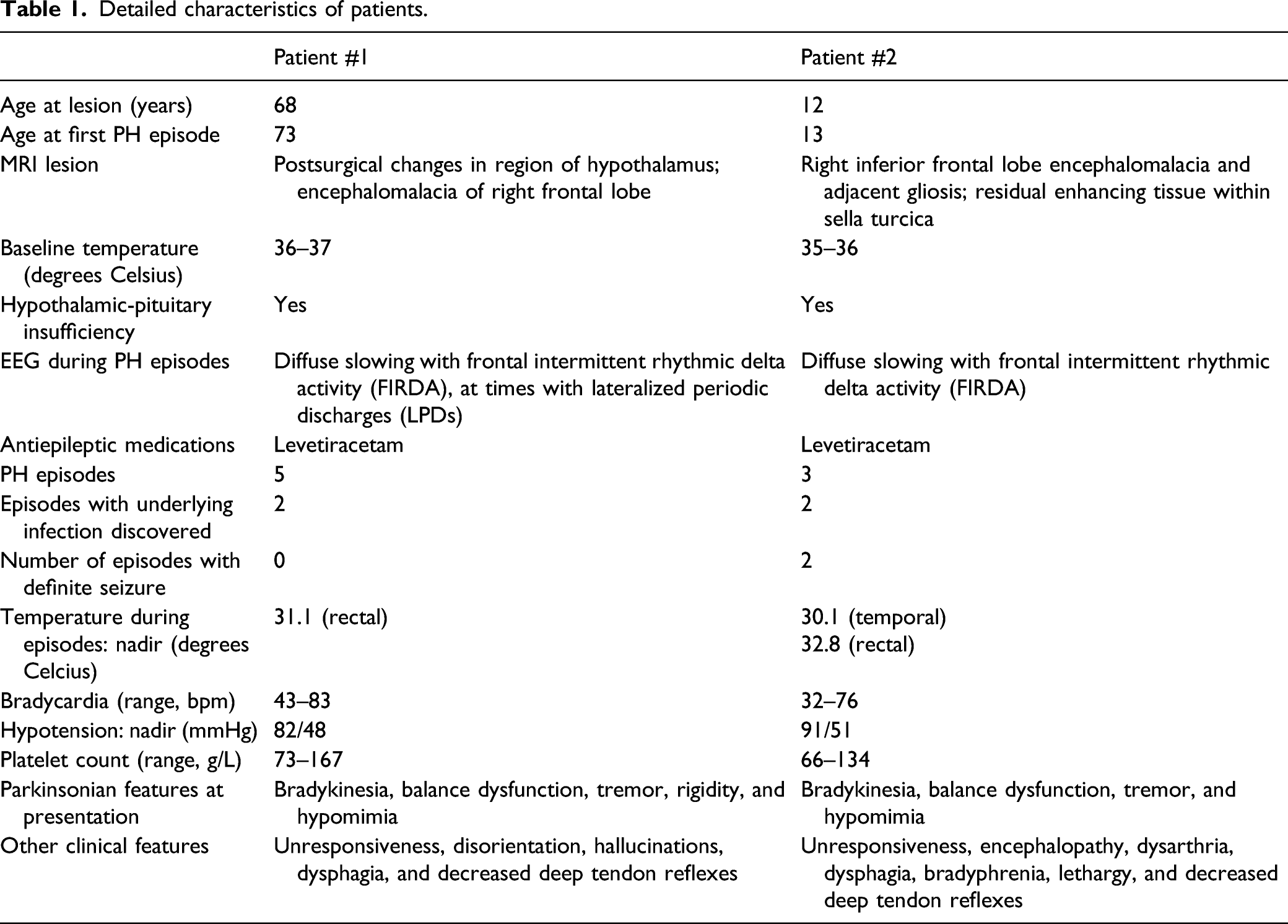
Detailed characteristics of patients.
Case #2
A 12-year-old girl underwent near-complete resection of a suprachiasmatic pilocytic astrocytoma in 2018. Postoperatively, she developed diabetes insipidus, hypothyroidism, and hydrocephalus requiring desmopressin, levothyroxine, and external ventricular drain, respectively. In the following year, she was admitted twice for provoked seizures due to hyponatremia. One year postoperatively, surveillance MRI brain demonstrated two foci of enhancement in the hypothalamus, and she completed chemotherapy with vincristine and carboplatin. Beginning in January 2020 she had three separate hospitalizations for seizure or unresponsiveness, preceded by days to weeks of increased lethargy, balance dysfunction, psychomotor slowing, bilateral hand tremor, and dysarthria. She had no history of exposure to dopamine-blocking agents. She had hypothermia with nadir temperature range 30.1–34.7 Celsius, with rectal temperature, when measured, two degrees lower than the concurrent temporal reading. Additional findings included bradycardia, thrombocytopenia, and polyuria with large fluctuations in serum sodium levels, requiring frequent adjustments in vasopressin dose. Each hospitalization was marked by one to two days of severe encephalopathy, with no speech and minimal eye opening, attributed to prolonged post-ictal state. Continuous EEG monitoring during each hospitalization showed diffuse slowing with FIRDA. Levetiracetam was initiated on the first of these hospitalizations. MRI brain demonstrated no recurrence of hydrocephalus in all three hospitalizations, but on the second demonstrated bilaterally symmetric restricted diffusion with FLAIR/T2 hyperintensity involving external capsules and putamina, consistent with extrapontine myelinolysis in the setting of overly rapid correction of hyponatremia. Infectious workup revealed MSSA pneumonia on the first hospitalization and urinary tract infection with Citrobacter koseri on the third. Her neurological examination, after resolution of minimally responsive state, showed hypomimia, bradykinesia, inability to perform serial sevens, and trace deep tendon reflexes. Gait was slow and hesitant (Table 1) and described by examiners as parkinsonian.
Discussion
Paroxysmal hypothermia (PH) is a rare syndrome characterized by recurrent episodes of spontaneous hypothermia, confusion, and impaired arousal. Bradycardia is typically present and frequently accompanied by additional findings of thrombocytopenia, hyperhidrosis, and asterixis. This syndrome was first described in pediatric patients with agenesis of the corpus callosum, and in that setting is known as Shapiro syndrome. The adult-onset cases usually do not have a detectable structural abnormality and may be due to a channelopathy. 1 Those with an identifiable lesion typically involve the hypothalamus. Etiologies reported include stroke, traumatic brain injury, subarachnoid hemorrhage, and multiple sclerosis. 2 Previously reported cases have mentioned bradykinesia, ataxia, and dysarthria, but parkinsonism has not been described as a specific feature of PH. The prominent parkinsonian features of the patients in this report thus made the diagnosis of PH more difficult.
Case #1 experienced the first episode of hypothermia nearly five years after pituitary adenoma resection, with the intervening years only notable for well-controlled epilepsy, hypothyroidism, and diabetes insipidus. Case #2, who also had epilepsy, hypothyroidism, and diabetes insipidus, consistently had mild hypothermia following her surgery, but the first episode of more pronounced hypothermia with accompanying bradycardia and thrombocytopenia occurred over a year after resection.
A series of four patients with post-lesional PH with lesions involving the diencephalon were clinically stable for years between the brain insult and the first hypothermic episode.
3
Similar to our cases, authors reported epilepsy, hypopituitarism, bradycardia, thrombocytopenia, and EEGs with diffuse slowing and FIRDA during episodes. Interestingly, hyperhidrosis, usually described as a key feature in PF was absent in our cases and in those described by Devic et al. All four of Case #1’s and two of Case #2’s episodes of hypothermia occurred in the winter months, an association previously reported.4,5 In Figure 1, we propose a diagnostic algorithm and scoring tool for patients presenting with these characteristics. Proposed diagnostic algorithm and scoring tool for paroxysmal hypothermia.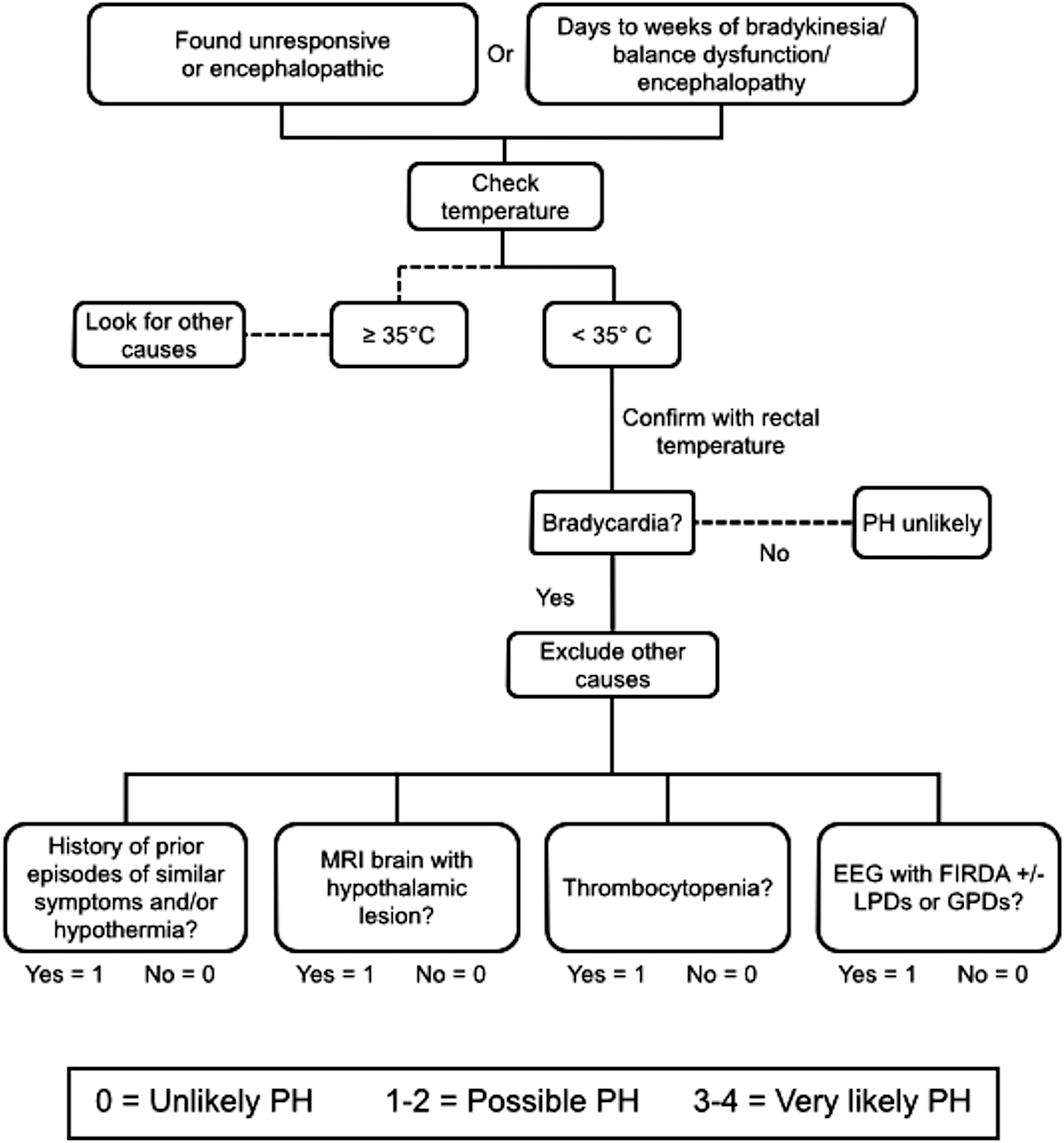
Many neurologic manifestations of acute hypothermia are well-established and progress in a fairly predictable manner. Psychomotor slowing, lethargy, and confusion are typically seen below rectal temperatures of 34°C, dysarthria below 33.5°C, with speech usually becoming completely absent below 28°C. Deep tendon reflexes become progressively diminished below 29.5°C. Increased muscle tone is frequently seen with mild hypothermia and ubiquitous at temperatures below 29.5°C. Some patients develop rigidity and flexion of all four limbs.2,6-8 Fay and Smith, in their experiments with the use of therapeutic hypothermia for various diseases, described “waxy stiffness,” a flexed position of the upper and lower extremities, increased muscular tone, and further described: “All volitional movements became progressively slower and incoordination gradually more pronounced as the temperature continued to fall. The slowed hypertonic movements of the Parkinsonian state are simulated, though the incoordination here was more pronounced.” 9 According to the Human Phenotype Ontology, ataxia, fatigue, and gait dysfunction are experienced by 80 to 99% of patients with Shapiro syndrome, while confusion and tremor are present in 30 to 79% of patients. 10 In this context our patients’ motor examination findings are not surprising. Hallucinations and amnesia of the hypothermic episodes, observed in Case #1, have been reported previously in PH.4,8,11-13
The association between PH and bradykinesia, rigidity, and other parkinsonian features suggests a potential role of dopamine signaling pathways, either as cause or effect of hypothermia. Blockade of dopamine signaling via D2 receptors in the hypothalamus is implicated in neuroleptic malignant syndrome, while chlorpromazine, a D2 receptor blocker, has shown efficacy in PH. 1 Conversely, bromocriptine, a D2 receptor agonist, an experimental animal study also demonstrated that can induce hypothermia and selective D2 agonists had a temperature-lowering effect on rats in an animal model study. 14 Thus, hypothermia seems to be associated with increased dopaminergic states rather than decreased as seen in PD. Further supporting this association is the observation that methamphetamine, which has been shown to damage dopaminergic neurons in the striatum and even to predispose chronic users to developing PD, causes hyperthermia. 15 Interestingly, pretreatment with dopamine-blocking antipsychotics has been shown to attenuate the hyperthermia. 16
Parkinsonism in PH may result from involvement of other pathways. For instance, a study demonstrated an 11–35% reduction in the concentrations of glutamate, glutamine, GABA, and aspartate during hypothermia in neonates. 17 Another possibility is a negative-feedback mechanism involving an undetected abnormal increase in dopamine in hypothermia, which leads to dopamine receptor downregulation or internalization resulting in parkinsonism. In both patients, the presence of remote cerebral lesions involving the hypothalamus most likely played a role in PH, and the striatal lesions related to myelinolysis in the second case could have been a contributing factor to the observed parkinsonism.
Further research is needed to better understand the possible connection between PH and dopamine activity in the central nervous system.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.