
Abstract
Carotid artery web is an underrecognized source and is found in about 1-2% of patients with acute ischemic stroke. Although, first described four decades ago, optimal therapy for carotid web is not yet known. Carotid stenting and endarterectomy are increasingly used for carotid web treatment, given its definitive treatment and avoiding the complications associated with anticoagulation. The case reported here is of an ischemic stroke secondary to a mobile thrombus on a carotid web evident on CT angiography and successful definitive treatment with delayed carotid wall stent placement. In young patients who have a diagnosis of ischemic stroke, the carotid web should be on the differential and adequate neuroimaging with either CTA or DSA should be pursued.
Keywords
Introduction
The carotid artery web also known as atypical fibromuscular dysplasia (AFMD) is a triangular-like shelf of tissue extending from the wall of the carotid artery into the lumen with stagnation and turbulence of blood flow distal to the lesion. 1 Sajedi et al has reported carotid web prevalence of 21.2% in the cryptogenic stroke population as opposed to 1.6% in the control group, a 10-fold increased risk. 2 African Americans and females were found to have higher incidence of carotid webs in a single-institution study. 3 Similarly, Coutinho et al also reported an association between ischemic stroke and the carotid web in cryptogenic stroke patients. They reported an association 8 times more common than the control group. In a single-center study of consecutive patients with anterior circulation ischemic stroke referred for mechanical thrombectomy, there were about 12% of patients who had an embolic stroke of undetermined source. Ipsilateral carotid artery web was detected in 1.9% of these patients. 4 No optimal treatment strategies have been defined for the management of carotid webs in patients with cryptogenic ischemic stroke in terms of medical and interventional treatment. 5
Case Description
We report a case of a 55-year-old right-handed Caucasian woman with no significant past medical history who presented with acute onset of aphasia and right-sided hemiparesis. She was treated with IV tissue plasminogen activator followed by mechanical thrombectomy for an acute left-middle cerebral artery occlusion. Transesophageal echocardiography and prothrombic workup were done as part of the initial stroke workup. They were unremarkable for etiology of the stroke. A vascular web at the carotid bulb was seen on computed tomography angiogram (CTA), but without any critical stenosis (Figure 1A). She was discharged home on aspirin 81 mg daily. After 6 months, a CTA of the neck was done to evaluate the carotid web and showed a large thrombus adhering to the carotid web (Figure 1B). She was started on the anticoagulation with apixaban 5 mg twice daily in addition to aspirin 81 mg daily. A month later, follow-up CTA showed clot resolution. She was continued on apixaban 5 mg twice daily for 6 months and was then admitted for elective stenting of the carotid web. She tolerated the procedure well with no evidence of proximal left ICA web after placement of endovascular carotid stent. She was then placed on aspirin 81 mg daily and Plavix 75 mg daily for the first 3 months after the stent placement. Three-month follow-up CTA scan showed the stent in appropriate position, with no evidence of a carotid web (Figure 1C). Following the CTA scan, the patient was continued on aspirin 81 mg daily for secondary stroke prevention.
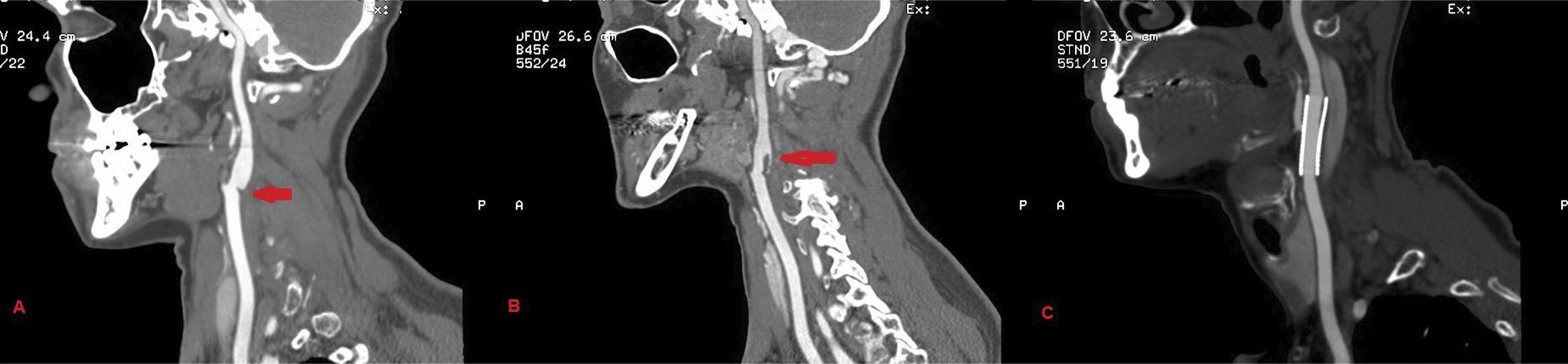
(A) Left ICA carotid web. (B) Left ICA carotid web and in-situ thrombus. (C) Left ICA carotid web treatment with endovascular wall stent.
Discussion
The carotid web has been described pathologically as an intimal variant of fibromuscular dysplasia in the internal carotid artery (ICA) and is defined radiographically as a translucent, shelf-like filling defect arising from the posterior aspect of the proximal ICA and projecting into the arterial lumen.6,7 It was first defined by Momose and New in 1973 and has since then been reported to be an underrecognized risk factor for cryptogenic ischemic strokes. 8 Doppler ultrasound combined with CTA or high-resolution magnetic resonance imaging (HRMRI) is an effective and reliable method to identify carotid webs. 9 In one of the largest case series of patients with carotid webs, the recurrent stroke risk was 30% (6 of 20 patients) in the antiplatelet therapy only group compared to 0% (0 of 7 patients) in the endarterectomy group after a mean follow-up of 2 years. 10 The most commonly reported treatments for the management of carotid webs are carotid endarterectomy and carotid artery stenting, given the prior case studies showing poor response to antiplatelet agents. 11 Given the imaging evidence of contrast stagnation, anticoagulation may constitute a reasonable choice of secondary stroke prevention; however, the evidence in this population is limited. Life-long commitment of anticoagulation also increases the risk of hemorrhagic complications and continues to be an important limitation. 12 Revascularization through endarterectomy or carotid stenting emerges as a viable treatment modality, given limitation with medical management. 12 Multon et al have reported in the Journal of vascular surgery on the sixteen patients who underwent treatment for carotid webs, in which thirteen were treated by carotid endarterectomy and 3 by carotid stenting. The follow-up at 30 days and 1 year was uneventful for all patients, without any deaths or stroke recurrences. 13 In one of the largest case series, Haussen et al, have reported data on carotid stent for webs showing effective strategy for secondary prevention with no periprocedural complications. After a 12-month follow-up of sixteen patients who underwent stenting, there were no recurrent strokes or TIA and no detectable carotid restenosis. 14
In our case, the patient was initially treated with aspirin 81 mg daily and then anticoagulation with apixaban 5 mg was added twice daily after the discovery of thrombus on the web. Follow-up imaging showed resolution of the thrombus with added anticoagulation. However, considering the increased risk of bleeding with anticoagulant therapy and lack of evidence for ideal management of the carotid web, a definite treatment approach was pursued with endovascular carotid stenting. No complications were reported from the procedure during the follow-up on 6 and 9 months.
By reporting this additional case of the carotid web, we aim to highlight its association with cryptogenic strokes. Carotid webs can not only cause strokes by focal stenosis from intimal hyperplasia but can also serve as a nidus for thrombus formation and subsequent artery-to-artery embolic stroke(s). Hence, immediate treatment is warranted in patients with symptomatic or incidentally identified carotid webs. Although no evidence-based management options exist at present for primary or secondary stroke prevention in such patients, our experience with anticoagulation (for bridging) and ultimate endovascular carotid stenting was a successful management strategy. In young patients with otherwise cryptogenic stroke, the carotid artery web should always be considered and ruled out with CTA as illustrated in the case report. Clinicians should be aware of this underappreciated stroke risk factor and a comprehensive approach to management with the help of different specialties.
Footnotes
Author’s Note
An informed consent for publication of this case report was provided by the patient’s legal representative.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.