
Abstract
Introduction
There is a complex interplay between systemic autoimmunity, immunosuppression, and infections. Any or all of these can result in neurologic manifestations, requiring diligence on the part of neurologists.
Case report
We herein report a case of a patient on immunosuppressive treatment for a vasculitis that resulted in zoster meningoencephalitis. This was further complicated by the development of anti-NMDAr encephalitis, the etiology of which is undetermined and further discussed in this paper. The patient eventually developed COVID-19 during hospitalization, succumbing to the respiratory infection.
Conclusion
This case emphasizes that post-infectious autoimmune disorders are becoming increasingly recognized and that they should still be considered in patients who are on immunosuppression. Practitioners should be aware of the complex relationship between autoimmunity and immunosuppression and consider both throughout the disease course.
Case Description
A 76-year-old man, with past medical history of right parietal stroke in 2014, in the distal branches of the medial cerebral artery (MCA), and acute ischemic cardiopathy in June of 2016, was admitted in July of 2016 with a prolonged history of anorexia, fatigue, fever, nonproductive cough, and epistaxis accompanied by acute kidney injury, microcytic anemia (Hb 8.6 g/dL), eosinophilia (900–1500/μL), elevated erythrocyte sedimentation rate (ESR) (94 mm/h), and elevated IgG (3184 mg/dL) with positive pANCA (MPO) antibodies. A diagnosis of ANCA-associated vasculitis was assumed after exclusion of other causes and treatment with prednisolone 40 mg/day and cyclophosphamide 750 mg 3/3 weeks initiated and tapered in the outpatient clinic.
CSF analysis during different time-points of the clinical history.
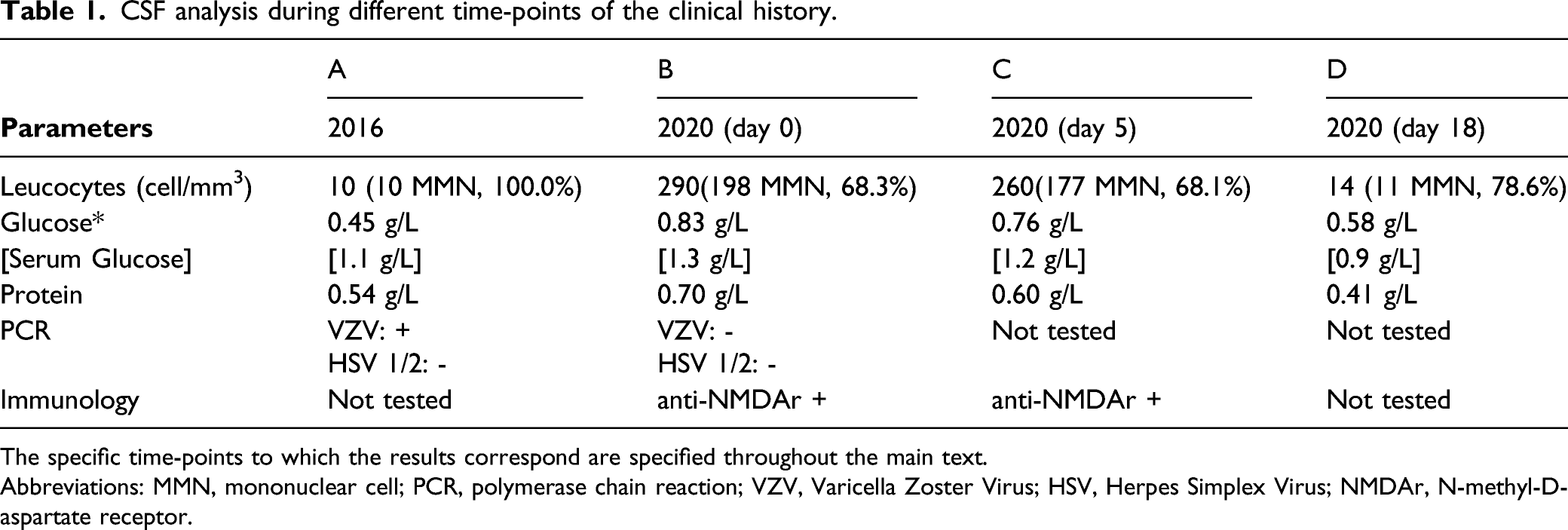
The specific time-points to which the results correspond are specified throughout the main text.
Abbreviations: MMN, mononuclear cell; PCR, polymerase chain reaction; VZV, Varicella Zoster Virus; HSV, Herpes Simplex Virus; NMDAr, N-methyl-D-aspartate receptor.

Histology of sural nerve biopsy: Moderate axonal neuropathy, particularly affecting small, myelinated fibers and with a symmetric involvement of the different fascicles. There were rare degenerating fibers (arrow) and occasional small regenerating clusters. No inflammation. Toluidine blue, scale bar: 500 μm (A) and 50 μm (B).
In June of 2018, he was admitted in the emergency department with a 5-day history of left eye pain, redness, and blurred vision. He was diagnosed with ophthalmic herpes zoster based on clinical examination by the ophthalmologist who described edema and stromal infiltrates in the inferior half of the left eye. He was started on valaciclovir. Continued follow up by ophthalmology led to the diagnosis of refractory herpes ophtalmicus in April of 2019, and azathioprine suspended given the risk of permanent vision loss.
At this point, the ESR was 40 mm/h, lymphocyte count 900/μL and the glomerular filtration rate stabilized at 30 mL/min, with inactive urinary sediment. Prednisolone 5 mg was maintained and standing acyclovir was started.
In November of 2020, the patient was admitted to the emergency department with an isolated receptive aphasia and the CT scan revealed a left temporo-parietal stroke (NIHSS = 7). Recombinant tissue plasminogen activator (rTPA) was administrated around 3 hours after symptoms onset. CT angiography did not reveal any evidence of thrombosis, extracranial or intracranial stenosis.. Reevaluation after 24 hours showed persistence of the aphasia, and hemorrhagic transformation was confirmed via CT Scan, showing a cortico-subcortical hematoma rupturing to the ventricular system. He was admitted to the Stroke Unit, developing periods of agitation for which haloperidol 2 mg was administered. A negative SARS-CoV-2 test was provided before admission. He developed a fever and progressive deterioration of the level of consciousness in the following days, associated with rise of blood inflammatory markers (ESR at 85 mm/h and C reactive protein at 160 mg/L). An acute kidney injury was diagnosed (CrS 1.76 mg/dL) and acyclovir suspended given its nephrotoxic potential. Urinalysis revealed leukocyturia and nitrituria, for which piperacillin-tazobactam was initiated. On the eighth day of hospitalization, as the patient displayed neck stiffness and altered mental status and fever persisted, a lumbar puncture was performed for a possible meningoencephalitis. Based on cerebral spinal fluid marked lymphocytic pleocytosis (Table 1. B), the possibilities of a vasculitis flare vs zoster relapse (given the antiviral interruption) were considered. Treatment with acyclovir 10 mg/kg/day was started until further laboratory analysis was available. A brain MRI revealed no additional findings (Figure 2). Serum pANCA antibodies were negative. Viral PCR of CSF was negative for HSV1, HSV 2, and VZV. Strikingly, immunofluorescent staining of serum and CSF revealed marked positivity for anti-NMDAR autoantibodies in two separate occasions (Table 1. C). Treatment with IV methylprednisolone 1g for 5 days and IVIg 2 g/kg for 4 days was added. A CSF evaluation at the 18th day revealed improvement of the pleocytosis (Table 1. D), but without clinical response. Antiviral treatment was continued. A full-body CT and a testicular US were unremarkable, except for signs of chronic pulmonary embolism on the CT, for anticoagulation was initiated. Weaning of prednisolone was started and mensal cycles of intravenous Immunoglobulin (IVIg) programed. The patient remained unresponsive, with the eyes open, and symmetrically mobilizing the four limbs throughout the entire hospitalization. FLAIR MRI showing old ischemic lesions on the right temporal, parietal, and occipital topography. On the left occipitoparietal region, there are signs of a recent ischemic event with hemorrhagic transformation in the left middle cerebral artery territory, corresponding to the more recent stroke. This location is consistent with the clinical signs of expressive aphasia.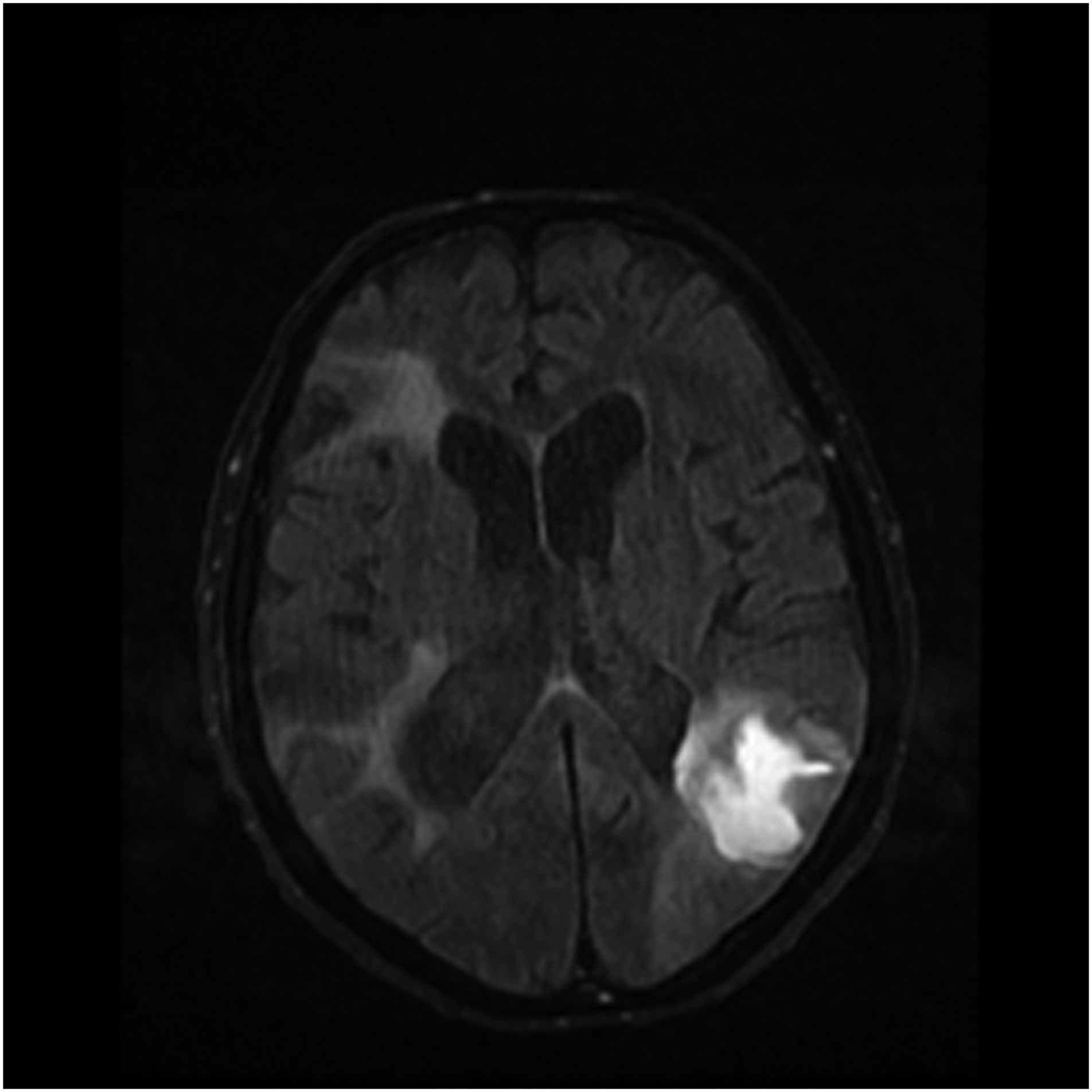
At the 42th day of his long stay, he developed a fever and nonproductive cough, and a SARS-CoV-2 PCR was ordered, which came positive. He was transferred to a COVID-19 dedicated infirmary where he died 16 days later from respiratory failure associated with viral pneumonia.
Discussion and Conclusions
This is an educational case of a patient with a rare systemic inflammatory condition, who developed both infectious and secondary autoimmune complications during his course of treatment.
The presence of eosinophilia and pANCA (MPO) antibodies gave rise to the diagnosis of eosinophilic granulomatosis with polyangiitis (EGPA), 1 previous Churg-Strauss syndrome, with cardiac, renal, lung, and suspected central and peripheral neurological involvements. Namely, in the absence of other cause, the previous ischemic stroke reflects a possible early involvement of the central nervous system. In fact, isolated cerebral infarction as the presenting symptom of ANCA-associated vasculitis has been reported. 2 The peripheral nervous system was also latter involved by a sensory-motor axonal neuropathy for which no other cause was identified.
Following the induction (prednisolone and cyclophosphamide) and maintenance (prednisolone and azathioprine) treatment for vasculitis, the patient developed VZV meningoradiculitis (with congruous herpetic rash) and herpes zoster ophthalmicus, respectively. These events were considered secondary to the immunosuppressive medication, in an elderly patient with chronic renal failure, both well-known factors associated with endogenous immune decline. In fact, both cyclophosphamide 3 and azathioprine 4 have been shown to directly correlate to the recrudescence of VZV and development of post-herpetic neuralgia. However, one must consider other factors as potentially predisposing for the recrudescence of the infection, not only related to the immune-senescence or systemic vasculitis, but also to an underlying malignancy, since both conditions are associated with immunosuppression. 5
This case highlights the intricate management of immunosuppression, since when the patient was kept only on prednisolone because of the multiple zoster recurrences he developed a probable flare of vasculitis. This in turn may have caused a second ischemic stroke with subsequent hemorrhagic transformation, for which vasculitis may have further contributed. 6 The etiology of this ischemic event was thoroughly explored, with exclusion of the most common causes of vascular disease by means of electrocardiography, electrocardiogram and angiography.
Clinical deterioration during hospitalization, associated with fever and meningeal signs, led to the investigation of a possible meningoencephalitis, unraveling marked positivity for anti-NMDAr in the CSF, with no evidence of VZV.
Based on the presence of altered mental status, CSF pleocytosis and seropositive for anti-NMDAr, an autoimmune encephalitis was considered. The brain MRI was normal, with no signs of increased signal on T2-weighted FLAIR imaging in the medial temporal lobes. As suggested by Graus et al, the diagnosis of autoimmune encephalitis can be made if antineural antibodies are detectable, even in the absence of imaging findings. 7 In this case, no better explanation for the clinical picture was present, with exclusion of infectious and other inflammatory conditions.
NMDA encephalitis is known to occur as a paraneoplastic disorder, post-infectious process or may be idiopathic. In our patient, a thorough investigation for malignancy was performed including full-body CT and testicular ultrasound, which were unremarkable. While the presence of pulmonary emboli could point toward malignancy-related hypercoagulability, this may have simply occurred in the setting of prolonged hospitalization.
Herpesviruses are a recognized trigger for anti-NMDAR antibodies. 8 Given their homology, we may speculate that the same mechanism of molecular mimicry proposed for HSV-1 may occur for VZV. 9 It has been suggested that other agents such as mycoplasma pneumoniae might also trigger anti-NMDAR antibodies, especially in younger patients. 10 With regard to the VZV associated anti-NMDAr encephalitis hypothesis, despite being rare, there have been several reported cases in the literature.11-12 Of these cases, two patients had underlying malignancy including a teratoma and non-teratomatous gynecologic malignancy, while one did not have any identified malignancy. This post-viral autoimmune encephalitis might progress into chronicity, with some reported cases of herpetic encephalitis associated with step-wise hippocampal sclerosis. 13
In this case, at the time of the diagnosis of the anti-NMDAr encephalitis, CSF PCR was negative for VZV. Unfortunately, VZV IgG was not tested in the CSF, which would have been useful in supporting the association.
We might argue that the last known manifestation of VZV activity occurred one year before, by means of herpes zoster ophthalmicus, which seems too long to consider the association. However, primarily with HSV, there have been reports of delayed diagnosis and persistent antibody presence farther out.14,15 Furthermore, VZV encephalitis might have been unnoticed at presentation.
Overall, taking into account the patients age and the diseases time course, post-herpetic anti-NMDAr seems a more plausible explanation. In the future, it would be interesting to study the immunogenic potential of clinically silent VZV infection and resulting autoimmune encephalitis. Immunosuppression is the mainstay of treatment, differing from the treatment of infectious causes, which highlights the importance of considering this etiology in clinical practice. 16
At the end, this patient with multiple processes of autoimmune, infectious and possibly neoplastic etiology, succumbed to hospital-acquired COVID-19, in the midst of the pandemic.
Our case highlights several points. Immunosuppression puts patients at risk for infections like VSV. Infections in turn can put patients at risk for autoimmune disorders, particularly in the increasingly recognized association between herpesviruses and anti-NMDAr encephalitis. Thus, it is important to always consider a wide differential diagnosis in complex patients with underlying or iatrogenic perturbations of the immune system.
Footnotes
Author contributions
JM collected the data and conceived the article. RT did the neuropathology study. SD, AS, JD, RT, PC, EN, AC and ES reviewed and critiqued the paper.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethics
This case report did not include any data that may identify the patient of its relatives. No approval from the ethics committee was needed.
Availability of Data and Materials
The information was obtained through from the electronical clinical records. No reference was made to any feature that may identify the patient or its relatives.