
Abstract
Background
Morbidity and Mortality (M&M) conferences are widespread but vary in goals and methodology. Some focus on clinical enigmas while an increasing number utilize quality improvement (QI) tools to effect systems change. Little is known about the current state of US Neurology M&Ms.
Methods
We surveyed 56 US academic neurology departments regarding their M&Ms to understand the use of QI tools and assess variability. Additionally, we reviewed the evolution of M&Ms in our department.
Results
The survey was completed by 44 (80%) departments; 68% reported quarterly frequency with 61% discussing 1–2 safety events per conference. The number of written guidelines or protocols resulting from M&Ms in 2 years varied from 0 (14% of departments), 1–2 (45%), to >5 (5%). Institutional culture regarding quality and safety and conference timing were cited by 71% as important in improving participation. In our own department, the M&M format changed in 2014 based on a sentinel patient event combined with improving safety culture across the hospital: neurology M&Ms transformed into thematic quarterly conferences utilizing QI tools. Attendance increased 3-fold, and in 7 years, we have generated 26 guidelines or pathways with corresponding decision-support tools, among other improvement efforts, resulting in specific systems changes. Based on survey results and our experience, suggested M&M “best practices” include the use of just culture, peer review protection, safety event analysis with QI methodology, trainee involvement, and logistical optimization.
Conclusion
Structured M&Ms incorporating suggested QI-informed “best practices” can be highly effective in driving system change within neurology.
Introduction
Morbidity and mortality conferences (M&Ms) have been widely adopted across the United States (US) since their inception in the mid-1900s.1,2 Despite their ubiquity, there has been considerable variability in terms of structure, content, and aims over time and across specialties. Some M&Ms have focused on clinical education, some on critiquing medical management, while others have increasingly had a quality improvement (QI) focus. 3 There has also more recently been a recognition of the conferences as a potential tool for QI education.4-6 In 2012, Josephson and Engstrom suggested M&Ms could be one of several tools harnessed within neurology for clinical and QI education for residents. 7 Given the shift in medicine over the last 2 decades toward safety culture and more rigorous implementation of improvement science, M&M conferences, with their roots in error analysis, represent a natural vehicle for identifying systems vulnerabilities and driving systems change.
National surveys in surgery8,9 and internal medicine 1 have detailed the frequency and characteristics of M&M conferences within those fields. Such surveys have also identified gaps in the traditional M&M format with Orlander and Fincke showing that internal medicine departments tended to have limited follow-up on action items after M&Ms such that change would be difficult to achieve. 1 Similarly, in reviewing the M&Ms across 12 departments at a large academic medical center, Aboumater et al found little adherence to medical incident analysis, with only 8% utilizing modern tools such as root cause analysis to investigate system factors. 3 Pieurluissi et al, in a prospective review of internal medicine and surgical M&Ms at 4 academic medical centers, found that discussion of error, even when the error directly led to an adverse event, was often lacking in M&Ms, more so in internal medicine than surgery departments. 10 Despite this growing literature in other specialties, little is known about the current state of neurology M&Ms in the US.
Here we present results of a national survey, the objectives of which were to evaluate use of QI tools, their impact on system changes, and to assess variability across academic neurology M&Ms. We also describe the evolution of the neurology M&M conference at our institution, including more recent changes incorporating QI tools. Based on the above, we propose a list of concrete and practical Neurology M&M best practices rooted in the literature and quality improvement methodology.
Methods
National Survey
We conducted an online, self-report survey of academic neurology departments in the US (Supplemental Appendix 1). In collaboration with a survey design expert, we developed an 18-question instrument through which we sought to understand the frequency, structure, content, aims and outcomes of neurology M&Ms, as well as the extent of incorporation of QI methodology5,11 (e.g., use of the just culture algorithm). Prior surveys done within other specialties, as well as the literature served as a guide.1,3,5,8-12 Prior to distribution, the survey was beta tested for clarity and face validity by individuals who were not otherwise involved in its development. A total of 56 medical centers were surveyed based on membership of their departmental leaders in the Association of University Professors of Neurology (AUPN; www.aupn.org). The AUPN members were emailed the survey, requesting completion within 8 weeks by the department chair or delegate most familiar with the departmental M&M conference (quality and safety chair, vice chair, residency training program director or other identified individual). Two reminders were sent prior to the deadline.
The survey was developed through Google Forms, designed to take 5–7 minutes to complete and, in addition to structured questions, offered an option to provide additional free-text comments. Survey respondents were requested to provide their names, e-mail addresses and hospital affiliations in the event follow-up clarification was needed. Respondents were informed that their names would not be revealed; however, if permission was granted, hospital names would be acknowledged in the event of publication. Survey results are presented as means (continuous variables) or frequencies and percentages (categorical variables).
Evolution of M&Ms in Our Department
A descriptive history of M&Ms in our department along with the evolution in the last decade was compiled through informal query of faculty present at our institution for several decades as well as the records kept by current quality chair (AS) who led recent revisions to the conference.
Standard Protocol Approvals, Registrations, and Patient Consents
The manuscript conforms to SQUIRE 2.0 guidelines. The survey was undertaken as a QI initiative at the Massachusetts General Hospital to understand the format of M&M conferences in the US and inform our own practices, and as such was not formally supervised by our Institutional Review Board per their policies.
Results
National Survey Results
Neurology M&M survey results: demographics of responding departments and basic M&M characteristics.
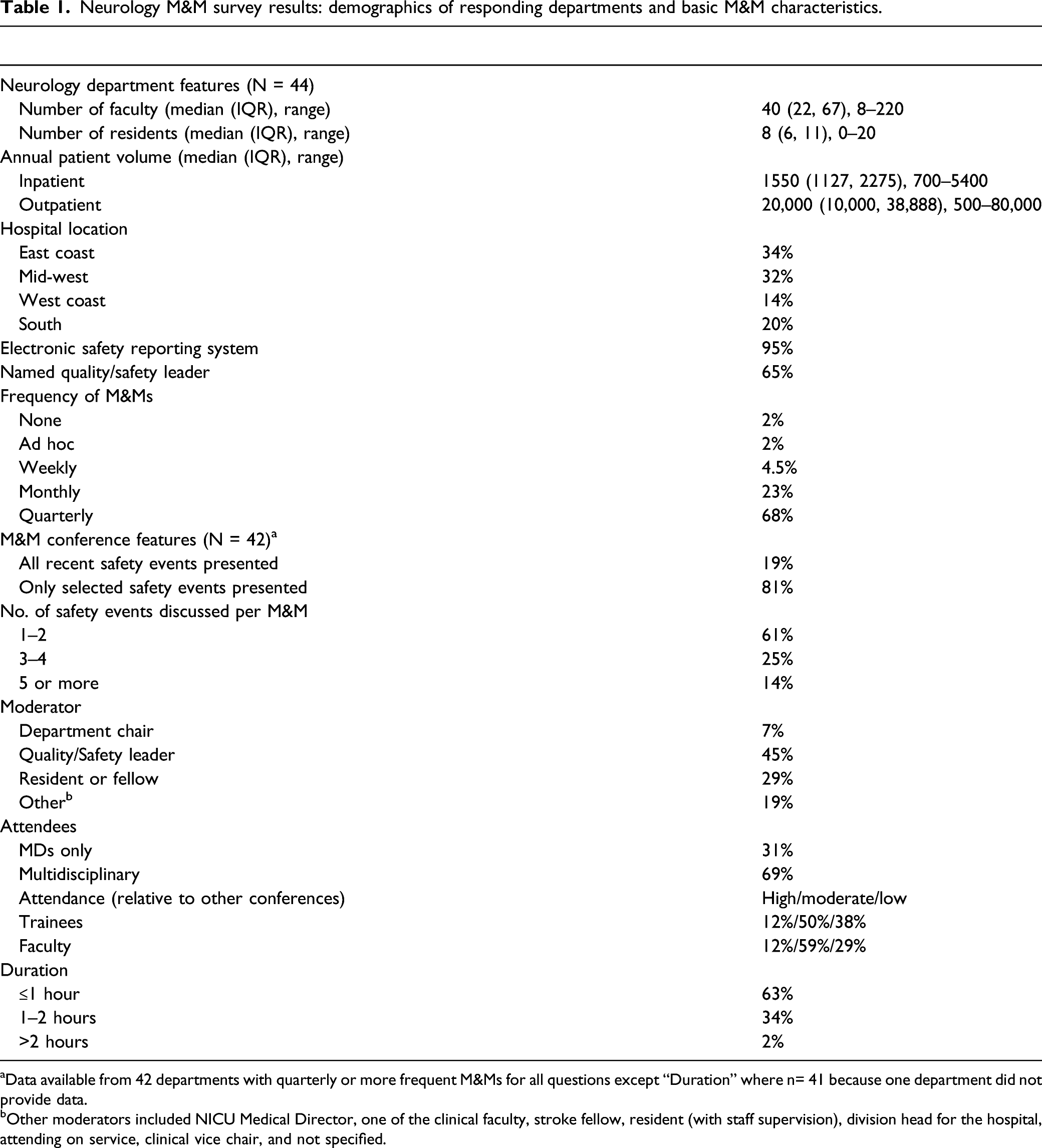
aData available from 42 departments with quarterly or more frequent M&Ms for all questions except “Duration” where n= 41 because one department did not provide data.
bOther moderators included NICU Medical Director, one of the clinical faculty, stroke fellow, resident (with staff supervision), division head for the hospital, attending on service, clinical vice chair, and not specified.
Institutional culture regarding quality and safety and conference timing were cited as important factors in improving M&M participation by 71% of departments. Another 57% identified regular attendance by departmental leaders as an important factor. Approximately 40% (15–20/42) of the departments identified the following factors as important for conference participation: mandatory attendance at a minimum number of annual conferences, just culture algorithm, time for discussion, location and provision of food/beverages. While only 28% of departments provided risk-management continuing medical education (CME) credits for faculty, the majority (72%) reported using M&Ms to meet the QI requirements for trainees established by the Accreditation Council for Graduate Medical Education (ACGME).
The majority of departments reported incorporation of some quality improvement tools (Figure 1). Many departments reported written guidelines or protocols resulting from M&M discussions over the last 2 years; however, the numbers varied widely (45% reported 1–2 guidelines or protocols; 19% reported 3–5; 5% reported >5; 14% reported none; 17% were uncertain). Only 38% of respondents consistently reviewed departmental or hospital performance on specific quality-safety metrics. The free-text comments highlighted challenges with safety culture, for example, skepticism about peer review protection and just culture. For example, one department reported that their conferences only permitted residents (with select faculty attendance by invitation) to preserve a “safe” environment for discussion. Percentage of Surveyed US Academic Neurology Departments Reporting the Inclusion of Certain Quality Improvement Practices into their M&M. Abbreviations: RCA—root cause analysis; Q&S—quality and safety; ACGME—Accreditation Council for Graduate Medical Education; CME—Continuing Medical Education.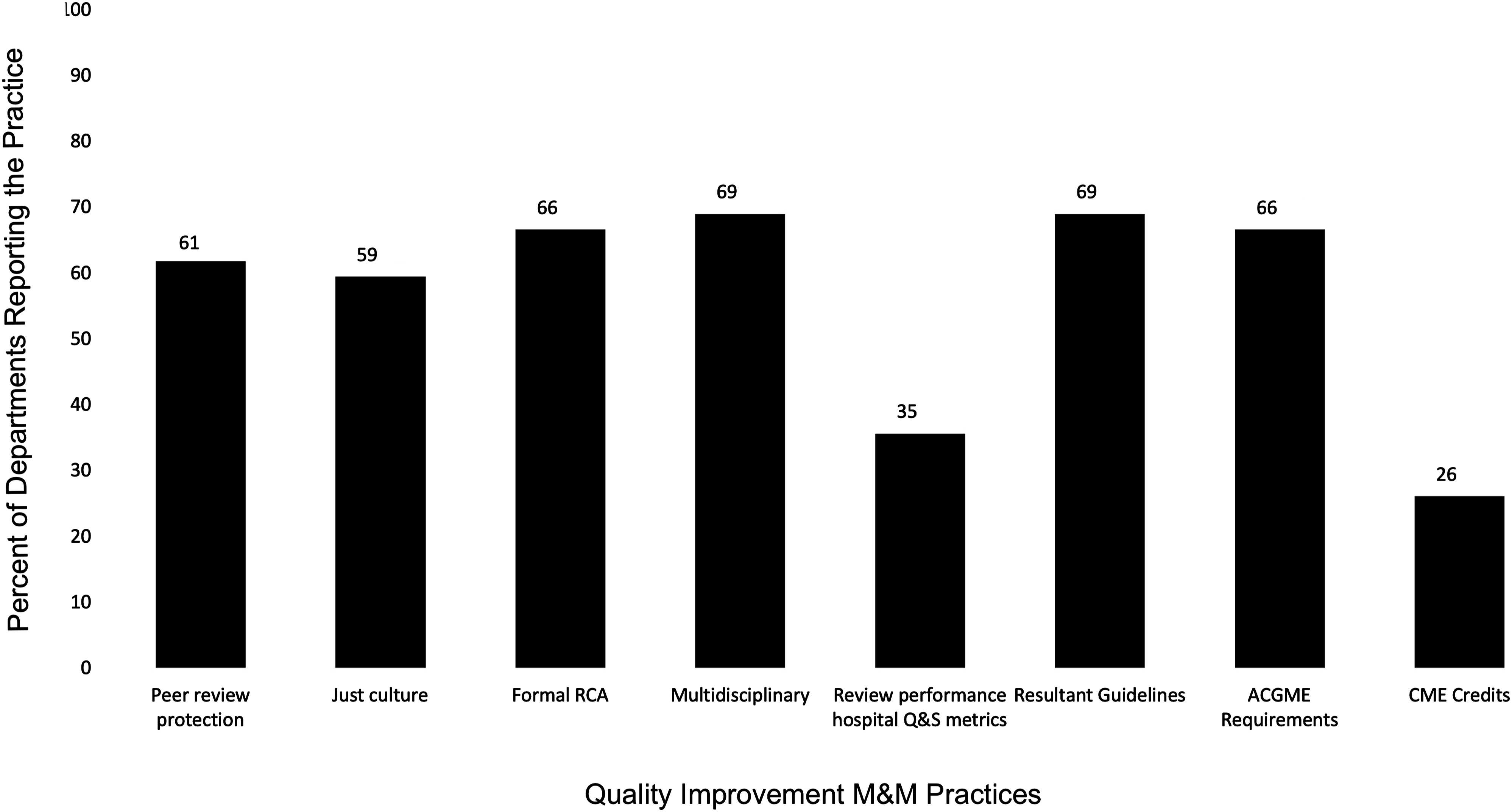
M&M Conferences in Our Department
History of the Conference
The Neurology Service at Massachusetts General Hospital (MGH) was established in 1872. Departmental M&Ms, which have always included both vascular and general neurology, have been held for over 4 decades and have gone through several iterations. Until 2003, conferences typically began in the early evening and ran for several hours with extensive literature reviews more often focused on interesting or challenging diagnoses than safety events. From 2004 to 2012, they were subsumed into senior residents’ noon conference reviews of their inpatient rotations with a primary focus on diagnostically challenging cases and only a brief review of major adverse events and mortalities. Additionally, our neurointensive care unit began its own M&M conferences run by fellows on a monthly basis. Outpatient and Consult service safety events were neither tracked nor reviewed, unless considered egregious. Faculty participation was voluntary; nurses and multidisciplinary team members participated rarely, and only if specifically invited. No formal incident analysis tools were utilized and there was little follow-up on safety events.
In concert with shifting national priorities, the MGH established its Lawrence Center for Quality and Safety in 2007, resulting in greater emphasis on safety culture and process improvement over the ensuing years. In that context, our department encountered a sentinel safety event concerning a missed opportunity for decompressive hemicraniectomy in large middle cerebral artery infarction. This case was analyzed using modern quality/safety methodology in 2011, resulting in a new guideline and implementation with evidence-based patient selection criteria for preventive neurosurgery.13,14 The goal of the guideline was to facilitate collaborative decision-making between neurologists and neurosurgeons; subsequent analysis showed a significant positive impact on patient outcomes and length of stay, and improved consensus between providers. 15 Motivated by this experience, we re-examined and later changed our M&M framework in 2014 to maximize safety culture and improvements in our systems of care.
New Format
The new M&M framework formally emphasizes just culture
16
and peer review protection.
17
Influenced by Lucian Leape’s teachings,
18
the conferences focus not on “who did it?” but rather “why did it happen?” Conferences are held quarterly. Faculty are expected to attend at least 2 of the 4 conferences annually. Departmental leadership is typically in attendance. To promote attendance, 1.0-hour risk-management CME credit is awarded, lunch is provided, and attention to the physical location, timing and duration (12:00–1:00
One or 2 similarly themed cases encountered over the prior 3 months warranting “systems change” are selected in advance by our multidisciplinary Neurology Quality and Safety Committee; most cases are selected from a review of consecutive safety events submitted via our secure electronic safety reporting system. Cases are formally analyzed using QI tools such as process maps and root cause analysis. The Mass General Brigham Joint Neurology Residency Program has developed a voluntary “QI certificate program” for residents interested in quality/safety. Participating residents are trained on QI methods and present the selected cases using aforementioned tools in a formal incident analysis during the M&M. Key questions are formulated in advance to frame the discussion, moderated by the departmental quality chair. The M&Ms end with consensus for a tangible action item with timeframes for systems improvement, delineation of responsibility, and clear accountability. Progress on prior projects is announced at each M&M providing a strong feedback loop and increasing engagement. Adherence is monitored, and feedback provided if warranted. This learning culture, together with explicit focus on just culture and a robust safety event reporting system, promote a strong safety culture related to our new M&M format. 19
Of note, these quarterly “themed” M&Ms supplement rather than replace the historic resident-run conferences and neurointensive care unit conferences where all mortalities, interesting cases and challenging diagnoses continue to be discussed.
Selected examples: Massachusetts General Hospital M&Ms since 2014.
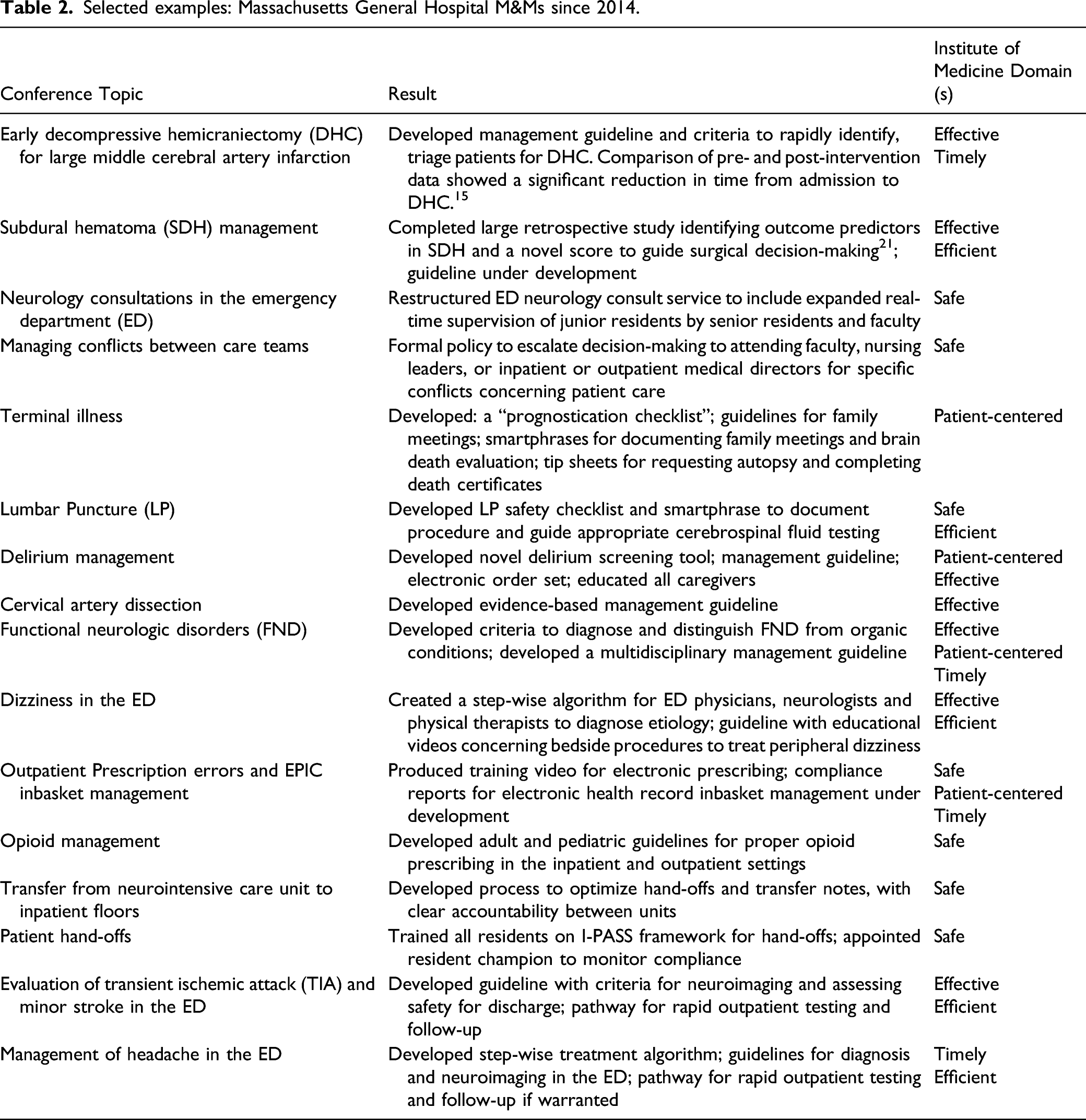
While data concerning M&M attendance and guideline creation prior to 2014 was not systematically recorded, the new-format M&Ms showed greater participation (on average, 40–60 faculty and trainees as compared to 15–20 previously), new guideline creation (26 in 5 years (Table 1), vs 4-6 over the prior several decades) and other systems changes. Our departmental QI projects complement the substantial hospital-wide QI initiatives developed by our hospital’s Center for Quality and Safety. At least one M&M related QI project led to reduced length of stay for neurology patients in the emergency department, among other systems outcomes. Feedback from faculty, residents, fellows, advance practice providers, nurses, other caregivers, and invited guests about our process has been overwhelmingly positive and recognized by hospital leadership. These conferences have become a key component of our resident QI certificate program, and QI education for our faculty and staff.
Discussion
We aimed to understand the status of M&Ms across the US and, combined with our own experience, propose best practices with attention to contemporary QI methodology. Our study builds upon a single-center report describing the evolution of M&Ms after implementation of a novel quality improvement curriculum. 22 Our national survey results suggest that many other Neurology departments are beginning to use quality-improvement in M&Ms Our data shows that many neurology departments conduct M&Ms; however, there is variability in their structure, frequency, attendance, and adoption of quality/safety methodology. Between 50% and 70% of departments reported implementation of selected quality and safety “best practices” including peer review protection, just culture algorithm, root cause analysis, multidisciplinary participation and guideline creation. However, the total number of new guidelines created in each case was relatively limited. Nonetheless, the majority of departments’ focus on formal quality/safety analysis and systems change is encouraging. Identified opportunities for improvement include the provision of risk-management CME to encourage faculty participation, increased trainee engagement and review of performance on hospital quality and safety metrics.
In the years since the Institute of Medicine report To Err is Human, 23 there has been a trend toward a more rigorous focus on safety and improvement including utilization of QI methodology to improve the utility of M&M conferences in driving systems change.6,24,25 The value of the conferences in achieving this end has been demonstrated in various reports throughout the evolving M&M literature. For example, Calder et al created the Ottowa Model for the Departments of Emergency Medicine and Trauma Services that emphasized structured case analysis, interprofessional and multidisciplinary involvement and included a pathway for systems issues to be brought to the respective quality and safety committee for action. 24 In the post-intervention period, they found that 100% of the M&Ms identified systems issues as compared to only 56.5% in the pre-intervention period and correspondingly, concrete systems solutions were proposed in 64.3% of post-intervention compared with 21.7% of pre-intervention M&Ms. Similarly, Bechtold et al implemented an Internal Medicine Patient Safety M&M which resulted in increase in attendance, some change in attitudes and although they were not able to do a before/after comparison of systems changes implemented, they did demonstrate a large number of systems improvement implemented over the course of the study period. Tad-Y et al implemented a similar systems-based M&M in their Department of Medicine and also showed increased attendance and adverse event reporting, along with a large number of systems improvements. 6
Compared with the large surveys conducted in surgery (2017) 9 and internal medicine (2003), 1 it appears that neurology departments are ahead of other specialties in incorporating QI methodology. However, other specialties may have changed their practices since the publication of these large surveys, as with the departments described above.
Proposed Neurology M&M Best Practices
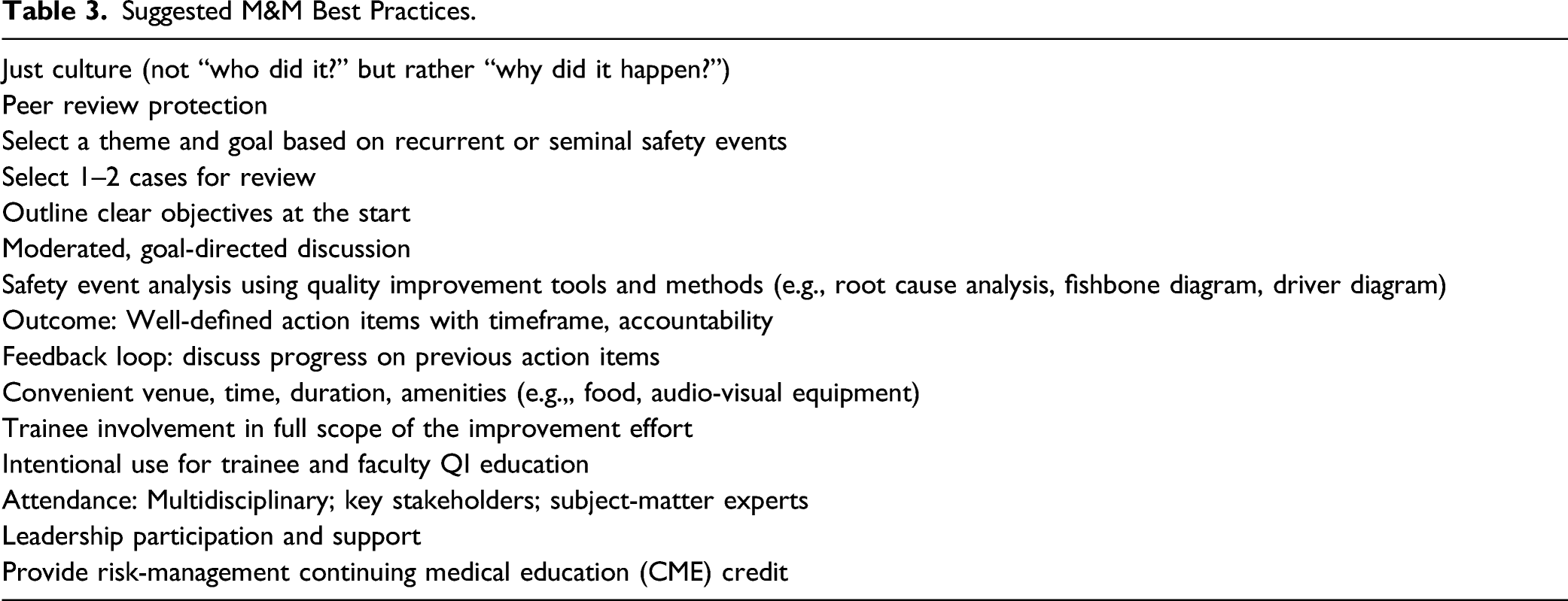
Suggested M&M Best Practices.
M&M as Tool for QI Education
While traditional M&Ms focus on clinical education they typically do not educate attendees on the tools necessary to implement evidence-based practices into routine workflow, nor do they specifically provide teaching about quality improvement or experiential learning across the full spectrum of the improvement process. In their 2018 Review, the Clinical Learning Environment Review (CLER) noted that while M&Ms were frequently used nationally for QI education and could be useful in providing foundational knowledge about safety issues, they often lacked critical components including a systems-based focus, timely response to safety events and interprofessional involvement. 26 At our own institution, we attempted to address these shortcomings by using a systems lens, involving a multidisciplinary group and involving residents in the “full scope of the improvement effort” from reviewing the event to implementing action items when possible via our QI certificate program.
The educational potential of M&Ms extends beyond trainees. The CLER report also noted that institutions “may lack a critical mass of faculty who are competent in performing and instructing QI activities, [such that] it is essential…to invest in faculty development in QI.” 26 Interestingly, most respondents to our survey utilized the conferences to meet ACGME requirements around quality and safety, but not for continuing medical education (CME) credits. This may be a reflection of the under-recognition of the need for faculty education on QI methodology.
Factors to Promote M&M Attendance and Engagement
Our experience provides insights into factors that can promote conference attendance and provider engagement, which are critical for the robust case reviews and discussions that help to drive meaningful quality improvement. Our rate of systems changes clearly accelerated after 2014 and is significantly higher than other centers. Further, feedback from our M&M participants suggest that changes such as guidelines with EHR reinforcement, care pathways and restructured inpatient services resulting from M&Ms are viewed as tangible ‘products’ and markers of progress, generating enthusiasm among front-line caregivers to report safety events and contribute to safety and QI initiatives. Also contributing to the success of our M&Ms are factors such as leadership support, involvement of subject-matter experts, convenient location, timing, limited duration, and provision of amenities. While attendance at M&Ms among the majority of survey respondents was reported as being low to moderate relative to other departmental conferences among both trainees and faculty (88% of departments), our M&Ms consistently generate high attendance compared to other educational conferences, presumably secondary to the above factors. Another likely contributor is the inclusion of nursing leadership and the entire multidisciplinary care team as well as medical students. Restricting individual case presentations to 1–2 events, and emphasizing just culture and peer review protection, additionally allow robust participation without concerns about blame or punitive action.
Complementary Formats: Theme-Based and Consecutive Safety Reviews
The new-format theme-based departmental M&Ms at our institution address the full spectrum of neurologic care: emergency department, ICU, inpatient and consult services, transitions of care and the outpatient setting. They complement the traditional inpatient service M&Ms that continue to be trainee-run and focused on reviewing mortalities, major safety events, and diagnostically challenging cases. Our experience suggests that resident engagement, “themed” conferences restricted to 1–2 events emblematic of a theme, with subsequent interventions informed by improvement science (e.g., accompanying decision-support and documentation tools), 27 results in prompt and sustained change. Efforts are ongoing to quantify impact on patient safety.
Despite the advantages in selecting a “theme,” we emphasize that it is equally important to review consecutive mortalities and safety events. Indeed, preventable events identified through service-based conferences often became the “theme” for our quarterly conferences. In addition, the key role of systematic case reviews required by regulatory bodies (e.g., stroke quality measure performance as required by the Joint Commission–approved Comprehensive Stroke Centers) cannot be over-stated. Ultimately, we believe a combination of processes is required to optimize patient safety and drive system change.
Limitations
As with other survey-based investigations, we acknowledge several limitations and biases that may influence our results and proposed “best practices.” Departments with an existing quality/safety leader, or those with existing financial or other commitments to quality and safety, may be more likely to respond to such surveys. Answers to the survey questions were based on self-report, and largely descriptive. Recall bias may have impacted answers. Large departments, or those with more frequent M&Ms or robust QI programs may heavily influence the overall result; we were unable to perform sensitivity analysis based on such factors due to the relatively low number of total respondents. Similarly, responses based on M&Ms conducted for regulatory reasons may have confounded our results. Since the survey was restricted to US academic neurology departments, our results and proposed “best practices” are not generalizable to community hospitals, or non-US hospitals. However, the overarching theme of utilizing a structured M&M format to drive systems change and QI education for all types of care providers may be generalizable.
In reviewing our own prior M&M topics as they linked to one or more of the 6 domains of quality care laid out by the Institute of Medicine 20 (Table 2) we noted that an M&M specifically advancing equity was lacking; indeed equity is the “theme” for our September 2021 M&M conference. In 2017 the IHI published a white paper entitled: Achieving Health Equity: A Guide for Healthcare Organizations. 28 The authors note great progress on all of the aims laid out in “Crossing the Quality Chasm” but admit that equity became the forgotten aim. There have been well-supported proposals that suggest that the key to transformational change around health equity, along with culture change, is to apply quality improvement tools to mitigating health disparities that occur based on identities. 29 The M&M conference represents a prime opportunity to put this suggestion into practice. Root cause analyses should consider whether patient or provider identities (race, class, sex, gender, sexual orientation, class, ability, language, and more) contributed to an error and propose actionable systems improvement. The very incorporation of these categories into error analysis will also effect culture change among resident and faculty, although may need to be supplemented with additional sessions directed specifically at culture change.
Conclusions
In summary, we believe that our experience is illustrative of the direction of academic neurology M&Ms across the country. Our proposed best practices provide practical and concrete steps for implementing QI methodology into M&Ms thereby harnessing these conferences to advance patient safety, QI education and systems change.
Supplemental Material
sj-pdf-1-nho-10.1177_19418744211067043 – Supplemental Material for Neurology Morbidity and Mortality Conferences and Quality Improvement: Single-Center Experience and National Survey
Supplemental Material, sj-pdf-1-nho-10.1177_19418744211067043 for Neurology Morbidity and Mortality Conferences and Quality Improvement: Single-Center Experience and National Survey by Sophia L. Ryan, Kathleen E. McKee, Lizbeth Londono-Sanche, Sarah Dougherty and Aneesh B. Singhal in The Neurohospitalist
Footnotes
Acknowledgments
We gratefully acknowledge Karen Lavoie for her expert guidance in survey creation, Professor Karen C. Johnston, MD, MSc, our Chief Merit Cudkowicz, MD, and the Association of University Professors of Neurology for assistance with survey distribution, all survey respondents, Ms Aayushee Jain for assistance with data analysis, the Massachusetts General Hospital Department of Neurology’s leadership, faculty, fellows, and residents (particularly those enrolled in our QI certificate program) for assistance via M&M participation, and Guideline creation and implementation.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Data Availability
All data used for analysis are presented in the tables and figures in this article. Anonymized data will be shared if requested by other investigators for purposes of replicating the results.
Supplemental Material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.