
Abstract
5 fluorouracil (5-FU)-related neurotoxicity is a rare and severe complication of 5-FU administration. Dihydropyrimidine dehydrogenase (DPD) deficiency is associated with an increased risk of serious adverse reactions due to its role in 5-FU metabolism. We report a case of acute reversible neurotoxicity with global areas of diffusion restriction in a patient with colorectal adenocarcinoma being treated with leucovorin calcium, 5-fluorouracil, and oxaliplatin (FOLFOX) without DPD deficiency following uridine triacetate administration.
Introduction
5-fluorouracil (5-FU) is a pyrimidine metabolite commonly used to treat solid malignancies including gastrointestinal, breast, head, and neck cancers. 5-FU-related neurotoxicity is rare and often presents with confusion, agitation, ataxia, seizure, and coma.1-3 Treatment regimens incorporating 5-FU may be given intravenously as a bolus or as a continuous infusion. While intravenous medication is rapidly metabolized by the liver in 15–20 minutes, continuous infusion may increase the risk of 5-FU toxicity and in particular, neurotoxicity, due to errors in device programming and device malfunction. 1 Dihydropyrimidine dehydrogenase (DPD) deficiency has also been associated with an increased risk of serious adverse reactions following 5-FU administration as the enzyme is responsible for metabolizing the drug.4,5 Characteristic brain MRI findings in 5-FU neurotoxicity include diffuse high-intensity T2 lesions that exhibit diffusion restriction in the deep cerebral white matter and corpus callosum. 6 Herein, we report a case of acute reversible neurotoxicity with global areas of diffusion restriction in a patient with colorectal adenocarcinoma being treated with leucovorin calcium, 5-fluorouracil, and oxaliplatin (FOLFOX) in the absence of DPD deficiency. We obtained informed consent from the patient’s surrogate decision-maker for this case report.
Results
A 67-year-old woman with stage III chronic kidney disease and newly diagnosed stage III colorectal cancer presented to the emergency department (ED) with generalized tonic-clonic (GTC) seizures. One day before admission, she started FOLFOX, a chemotherapy regimen containing oxaliplatin (98 mg), leucovorin (600 mg), and 5-FU (400 mg/m2). She was prescribed a 48 hour continuous 5-FU home infusion (total dose 3600 mg). Within 24 hours of the infusion, she became restless and complained of chest pressure and a headache. Shortly after the onset of symptoms, she developed generalized convulsions and her husband brought her to the ED.
Emergency Department Course and Admission
On presentation to the ED, our patient was normotensive, normoxic, tachycardic with a heart rate of 147, and tachypneic with a respiratory rate of 29. On physical exam, her eyes opened spontaneously and exhibited a left gaze deviation. She made incomprehensible noises and her level of responsiveness fluctuated between a Glasgow coma scale 3 and 10. There was no ataxia present on her exam. She otherwise had no focal neurological deficits. Shortly after her initial exam, her tachypnea worsened, she became hypoxic, and experienced a GTC seizure. She received 4 mg of intravenous midazolam and was intubated for airway protection. Subsequently, she was given 2 g of levetiracetam and started on continuous infusions of midazolam and propofol. Initial labs showed mild anemia with a hemoglobin of 11.7 g/dL, metabolic acidosis with a bicarbonate 13 mmol/L, worsening kidney function with blood urea nitrogen of 37 mg/dL and creatinine 2.21 mg/dL (patient’s baseline 2.00 mg/dL). The remainder of the metabolic panel, liver function tests, cardiac enzymes, procalcitonin, and coagulation studies were unremarkable. A non-contrast computed tomography (CT) scan of her head revealed no acute intracranial abnormalities. Her chest X-ray showed multifocal infiltrates; therefore, she was started on vancomycin, cefepime, and metronidazole out of concern for aspiration pneumonia. She was admitted to the intensive care unit for further management for further work-up for seizures.
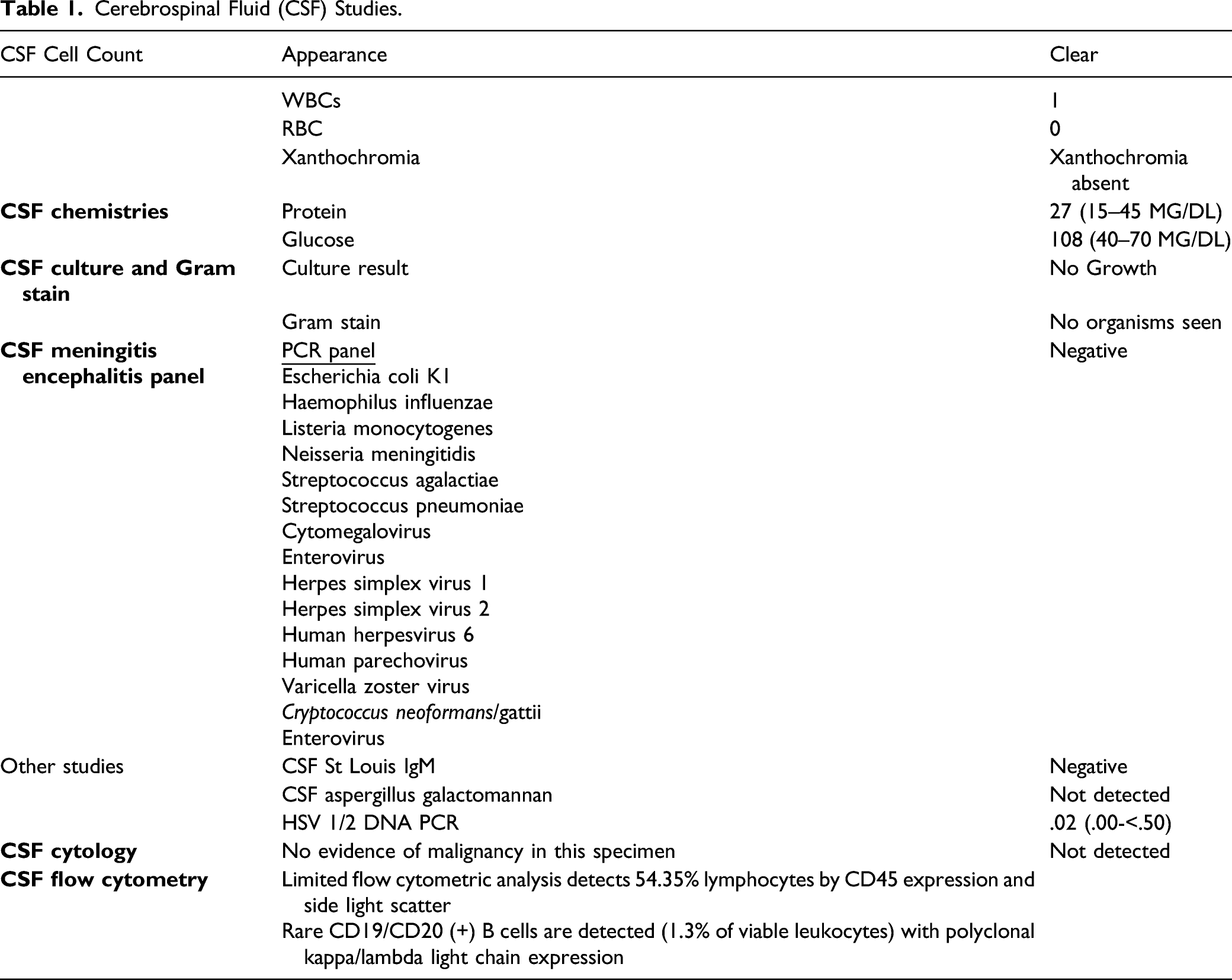
Cerebrospinal Fluid (CSF) Studies.
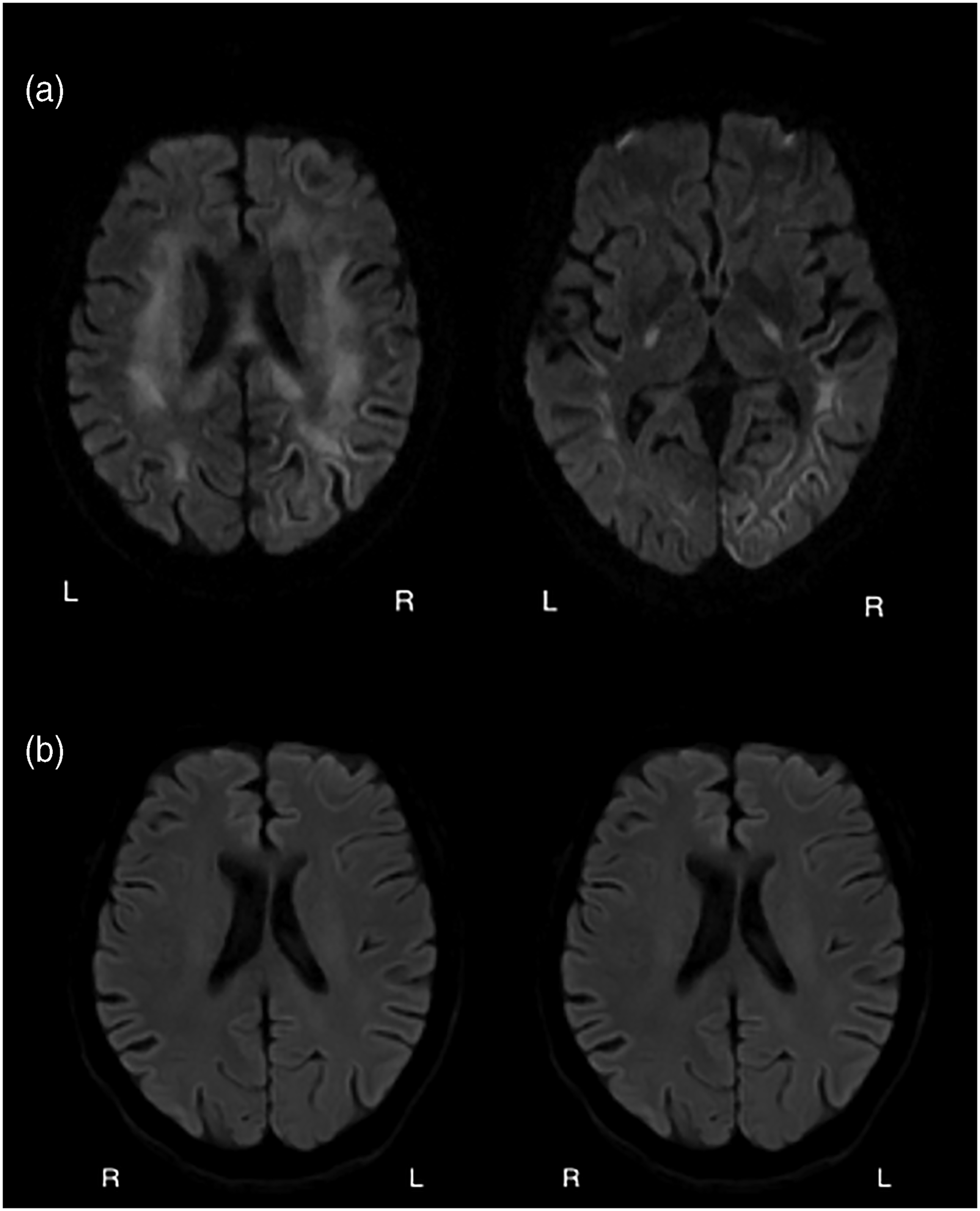
A. Diffusion-weighted imaging sequence showing areas of diffusion restriction in the centrum semiovale, thalami, and corpus callosum. B. Diffusion-weighted imaging sequence demonstrating resolution of diffusion restricting lesions.
Differential Diagnoses
Common causes of seizures include central nervous system infections, electrolyte abnormalities, alcohol withdrawal, and acute intracranial processes such as cerebral hemorrhage, ischemic strokes, posterior reversible encephalopathy syndrome, and medication toxicity. Uncommon etiologies include thrombotic events secondary to hypercoagulable disorders, such as cerebral venous sinus thrombosis, autoimmune conditions, such as systemic lupus erythematosus, or paraneoplastic processes. Given her history, MRI findings, and negative work-up for other etiologies, 5-FU neurotoxicity was determined the likeliest possibility.
Treatment
The patient remained in super-refractory non-convulsive status epilepticus for several days despite aggressive medical management with anesthetics and anti-seizure drugs (ASDs). She required 7 ASDs for seizure control including lacosamide, levetiracetam, oxcarbazepine, perampanel, pregabalin, and continuous midazolam and ketamine infusions (Figure 2). On hospital day 3, she received uridine triacetate, FDA approved antidote for 5-FU toxicity and received a total of 20 doses. On hospital day 9, she started a 5-day course of high-dose methylprednisolone empirically while the paraneoplastic panel was pending. Repeat brain MRI on day 10 revealed complete resolution of areas of diffusion restriction and high T2 signal (Figure 1(B)) and resolution of status epilepticus. She was gradually weaned off ketamine, midazolam, levetiracetam, and lacosamide over several weeks with gradual but significant improvement in her level of alertness and cognition. She was discharged on oxcarbazepine, perampanel, and pregabalin (Figure 2). Medications timeline during admission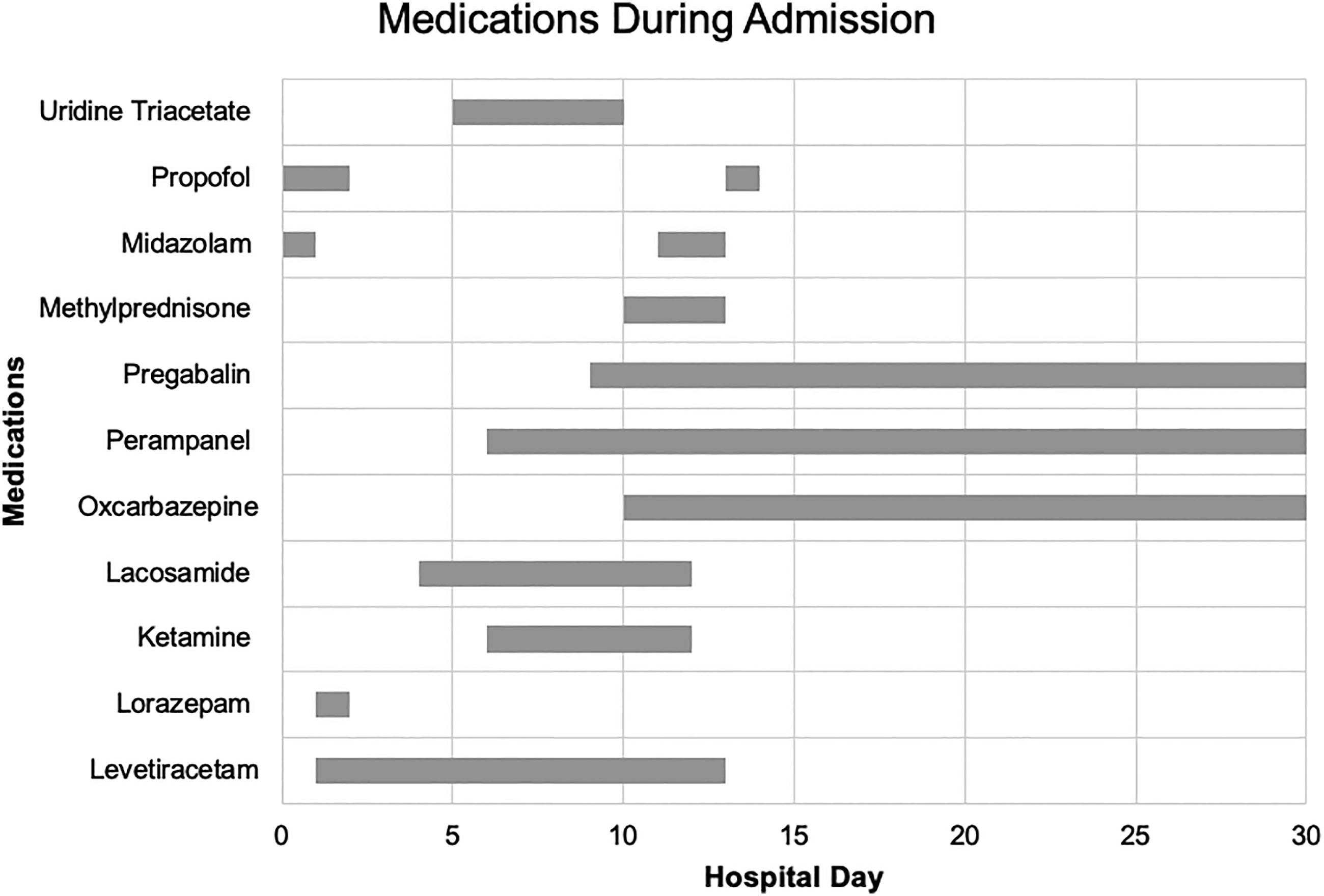
Outcome and Follow Up
At 29 days, she was discharged to a skilled nursing facility to continue her physical rehabilitation. Upon discharge, she was seizure-free, awake and alert, oriented to self, date, and location. She regained her ability to speak and followed simple commands. Two days following discharge, she required brief readmission for recurrent seizure activity due to transient hyponatremia attributed to oxcarbazepine. The medical team discontinued oxcarbazepine and pregabalin and transitioned her to a regimen of levetiracetam, phenytoin, and perampanel. She was discharged back to the prior skilled nursing facility after 6-day inpatient readmission to continue her recovery.
Discussion
5-FU-associated encephalopathy is a diagnosis of exclusion and requires a temporal relationship between drug administration and the onset of symptoms. The onset of encephalopathy varies from 10 to 30 hours from the start of high-dose 5-fluorouracil infusion. 7 Our patient’s symptoms started within the first 24 hours of the start of drug infusion. An extensive work-up was performed to rule out other causes of encephalopathy.
Dihydropyrimidine dehydrogenase (DPD) is responsible for breaking down over 80% of administered 5-FU. 8 Therefore, a deficiency in DPD increases the risk of fatal complications associated with 5-FU. Our patient tested negative for DPD mutations, but it remains possible she harbored a genetic variant not accounted for in the genetic testing panel. Other known risk factors include mutations in the orotate phosphoribosyltransferase and thymidylate synthase genes, high doses of 5-FU, renal failure, and concomitant use of leucovorin as it increases the intracellular concentration of 5-FU.9-11 Our patient received 400 mg/m2 of 5-FU and was discharged home on a 3600 mg infusion to be administered over the next 48 hours. We suspect her neurotoxicity resulted from concomitant leucovorin use and renal failure increasing her effective 5-FU dose.
Additionally, recognizing the imaging findings associated with 5-FU toxicity is imperative for early diagnosis and timely treatment. CT often shows symmetrical periventricular hypoattenuation. T2 weighted MRI is more sensitive, and findings include diffuse high-intensity signal in the white matter and corpus callosum, similar to this patient’s MRI findings. 6
The critical steps in managing 5-FU toxicity are prompt discontinuation of the drug and administration of uridine triacetate. Uridine triacetate inhibits fluorodeoxyuridine monophosphate, an active metabolite of 5-FU, which is responsible for inducing cellular apoptosis. Uridine triacetate has emerged as a highly efficacious treatment for 5-FU toxicity.12,13 The recommended dose is 10 g orally every 6 hours for a total of 20 doses. 13 Our patient was treated within 72 hours of exposure and received 20 doses. We noted clinical improvement on day 8 when she began to follow commands.
5-FU is one of the most widely used chemotherapeutic regimens to date, and clinicians must be aware of its neurotoxicity, clinical presentation, imaging findings, and management. DPD deficiency increases the risk of 5FU toxicity but it can occur even in the presence of normal DPD levels and activity such as in cases of renal failure and concomitant use of leucovorin. Uridine triacetate should be started immediately as prompt treatment is associated with rapid recovery.
Patient’s Perspective
Excerpt from phone call with patient: “This whole experience was a shock to my system! Never in a million years would I have thought this would have happened to me. I had to learn to walk again and slowly regained all my strength. It took about 6 months to get back to my full self again after the hospitalization. I am now walking, cleaning, cooking, shopping, and doing everything I used to do. I have not had any seizures since the hospitalizations and I have been driving small distances. I feel like I even have more energy now and new perspective; I do not sweat the small stuff. I was glad to hear I did not have the DPD mutation because I have a daughter. I am hoping writing about this can help others with my condition.”
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.