
Abstract
We herein report a case of Childhood Primary Central Nervous System (CNS) Angiitis. This case consisted of a 14-year-old girl who presented with right-sided weakness, aphasia, and a fever. A Magnetic Resonance Imaging of the brain showed multifocal areas of ischemia. Magnetic Resonance Angiography of the head and neck showed narrowing and irregularities of the left middle cerebral artery and right posterior cerebral artery. Cerebrospinal Fluid studies showed a lymphocytic pleocytosis and brain biopsy revealed leptomeningeal and perivascular inflammation. The epidemiology, presenting symptoms, work-up, pathophysiology, diagnostic criteria, and treatment of Childhood Primary CNS angiitis are discussed. This case serves as a reminder that when pediatric patients present with stroke-like symptoms inflammatory etiologies including Primary CNS Angiitis must be considered and treated appropriately in a time sensitive manner.
Introduction
Acute ischemic stroke in the pediatric population is rare but extremely important to recognize and treat appropriately. Estimated incidence of strokes in children ranges anywhere from 2.5–13 per 100,000 per year.1,2 Stroke-like symptoms in the pediatric population has an extremely broad differential including inflammatory and metabolic etiologies that are rarely seen in adults. We present a case of a 14–year-old girl who presented with right-sided weakness and aphasia. She was ultimately diagnosed and treated for large-medium vessel angiography-positive nonprogressive subtype of Childhood Primary Central Nervous System Angiitis (PACNS).
Case Description
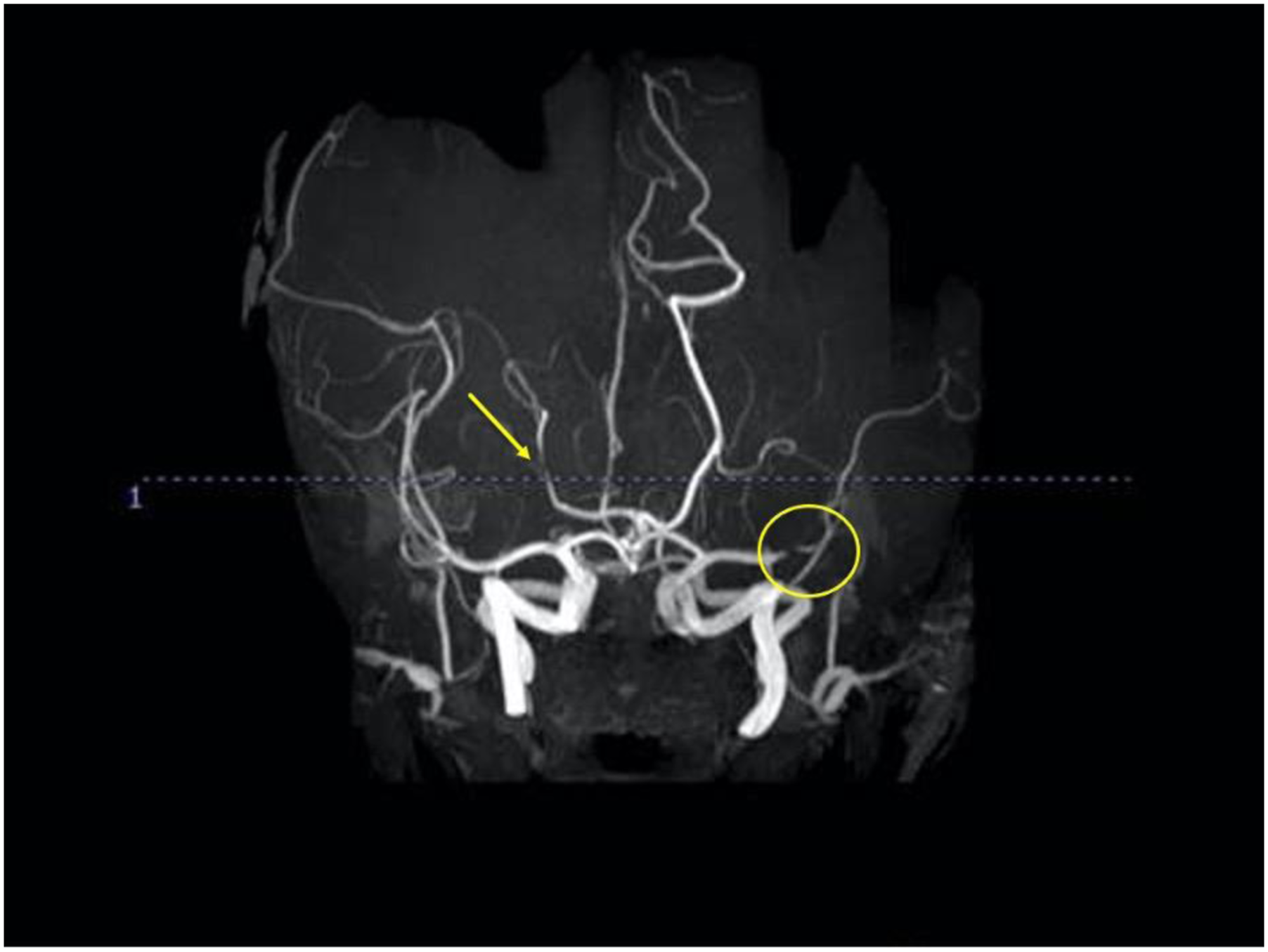
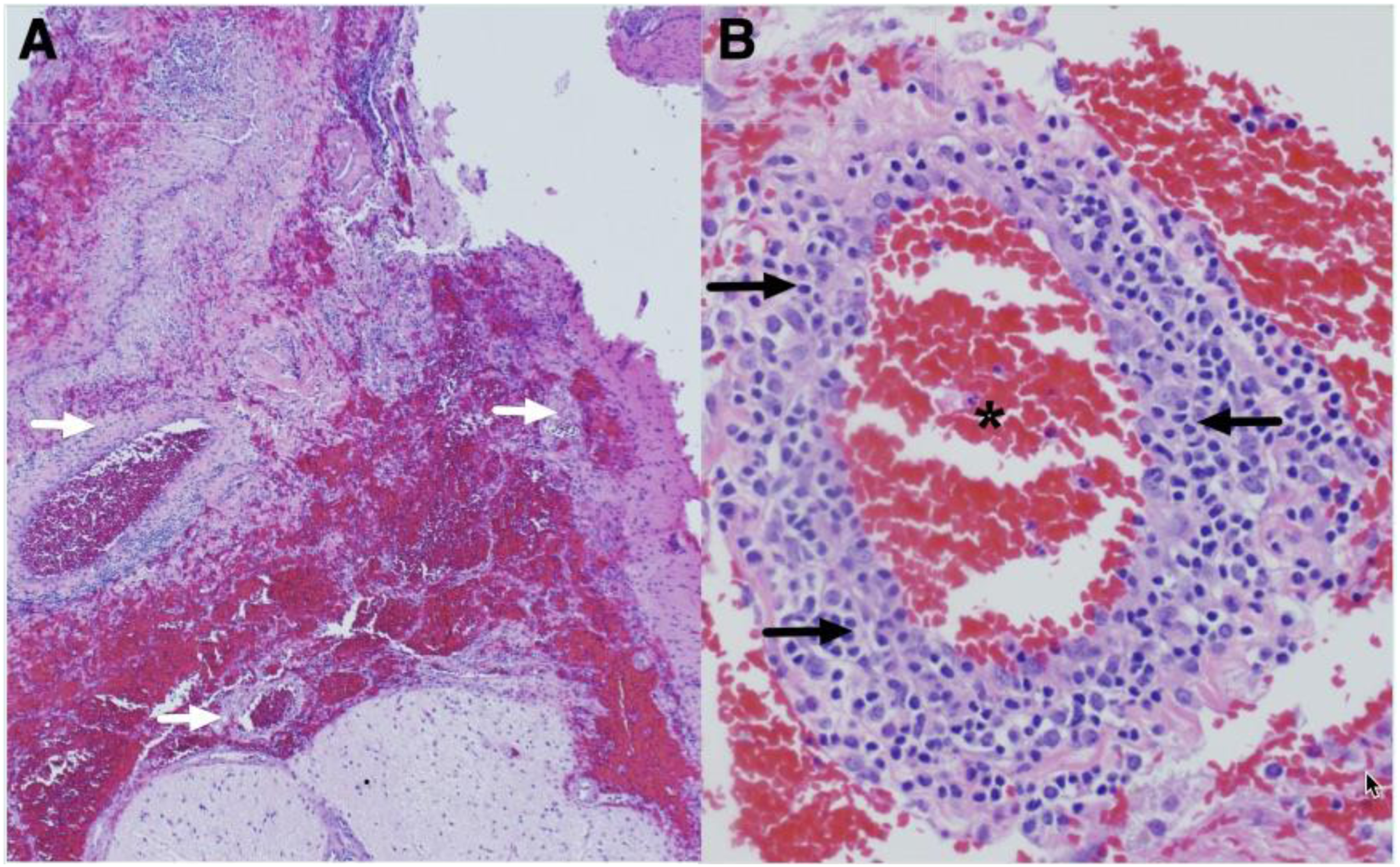
A 14-year-old right-handed girl presented with right-sided weakness and aphasia. She was in her usual state of health until she developed tingling and numbness in a circumferential pattern in her right hand. The following day she could not move her right hand and developed difficulty walking. On the third day she developed complete paralysis of her right arm and leg. She was unable to walk and was only able to say a few words with decreased fluency. Patient denied headache. She had no preceding trauma or infectious symptoms. Her past medical history was notable for a diagnosis of bilateral vitritis ten months ago that self-resolved. She had also been referred to rheumatology six months prior to presentation for neck, hand, and knee pain. She also had swelling in her right fifth distal interphalangeal joint. X-rays of her neck, hand, and knee were normal at this time. Magnetic Resonance Imaging (MRI) of her right hand was normal at this time. Erythrocyte Sedimentation Rate (ESR), C-reactive protein (CRP), Antinuclear Antibody (ANA), Human Leukocyte Antigen B27, Rheumatoid Factor, and Cyclic Citrullinated Peptide were all normal at this time. Her family history was notable for a brother with juvenile idiopathic arthritis. The patient presented to the emergency room where she was found to have a temperature of 38.3°C and pulse of 112. She was alert and able to follow commands. No clear encephalopathy. She was a well-developed female in no acute distress. Respirations were clear and unlabored. No rashes or lymphadenopathy were noted. She had severe expressive aphasia, intermittently able to say only one or two words and unable to name or repeat. She had a right lower facial droop with weakness in her right arm and right leg graded at 1/5 on the Medical Research Council scale for muscle strength. She had decreased sensation to light touch throughout her right face, right arm, and right leg. Reflexes were 3+ in the right biceps, brachioradialis, and patella with extensor plantar reflex on the right. The remainder of her neurologic exam was normal. Basic laboratory testing including complete blood count, comprehensive metabolic panel, ESR, and CRP were within normal limits. An ANA titer returned positive at a titer of 1:80. A MRI of the brain showed multifocal areas of ischemia most prominent in the left superior frontal lobe in the anterior cerebral artery (ACA) and middle cerebral artery (MCA) territory (Figure 1). Magnetic Resonance Angiography of the head and neck showed narrowing and irregularity of the proximal left M2 MCA branch and a P3 branch of the right posterior cerebral artery (Figure 2). Susceptibility weighted images showed focal decreased signal in the left M2 branch and left A2 branch. Vessel wall imaging showed vessel wall enhancement of the left M2. Echocardiogram with bubble study was normal with no evidence of interatrial shunt. Hypercoagulability labs including Factor V Leiden mutation, lupus anticoagulant, anti-cardiolipin, and anti B2 glycoprotein were negative. SARS-CoV-2 IgG and IgM were negative. Cerebrospinal Fluid (CSF) studies showed 18 white blood cells (97% lymphocytes), glucose of 50 mg/dl, and protein of 25 mg/dl. Cerebrospinal Fluid panel testing for infectious and viral pathogens by PCR including Cytomegalovirus, Enterovirus, Herpes Simplex 1 and 2, Human Herpesvirus 6, Parechovirus, and Varicella Zoster Virus (VZV) were negative. Bacterial cultures were negative. Autoimmune/Paraneoplastic antibody panel was not sent. A left frontal brain biopsy was obtained which contained superficial cortex and white matter with superficial vein/artery. The biopsy revealed prominent leptomeningeal mononuclear cell inflammation and marked transmural and perivascular T-lymphocyte predominant inflammatory infiltrates without definitive evidence of vascular damage (Figure 3A and B). The biopsy was negative for evidence of embolism, viral infection, demyelination, or neoplasm. Additional rheumatologic serum testing was obtained including ANCA, complement levels, SSA/SSB, double stranded DNA antibody, centromere B antibody, SM antibody, angiotensin converting enzyme, lysozyme muramidase, and anti-Mullerian hormone, which were all negative. There was no other systemic signs of vasculitis found and she was ultimately diagnosed with PACNS. MRI of the brain: Diffusion-weighted imaging (DWI). Imaging shows multifocal areas of ischemia, most prominent in the left superior frontal lobe in the ACA/MCA territory. Numerous smaller foci of restricted diffusion throughout the left MCA distribution. There are also DWI changes in the right thalamus. MRI, Magnetic Resonance Imaging; ACA, anterior cerebral artery; MCA, middle cerebral artery. Magnetic Resonance Angiography of the brain showed narrowing and irregularity of a proximal left M2 branch (yellow circle) and moderate focal narrowing of a right posterior cerebral artery segment in a P3 branch (yellow arrow). A. H&E stained section (40X) showing inflammation involving medium sized leptomeningeal vessels (white arrows). B. Higher magnification view (200x) showing a single vessel with predominantly lymphocytic inflammation in the vessel wall (black arrows). The vessel lumen with red blood cells is indicated by the asterisk.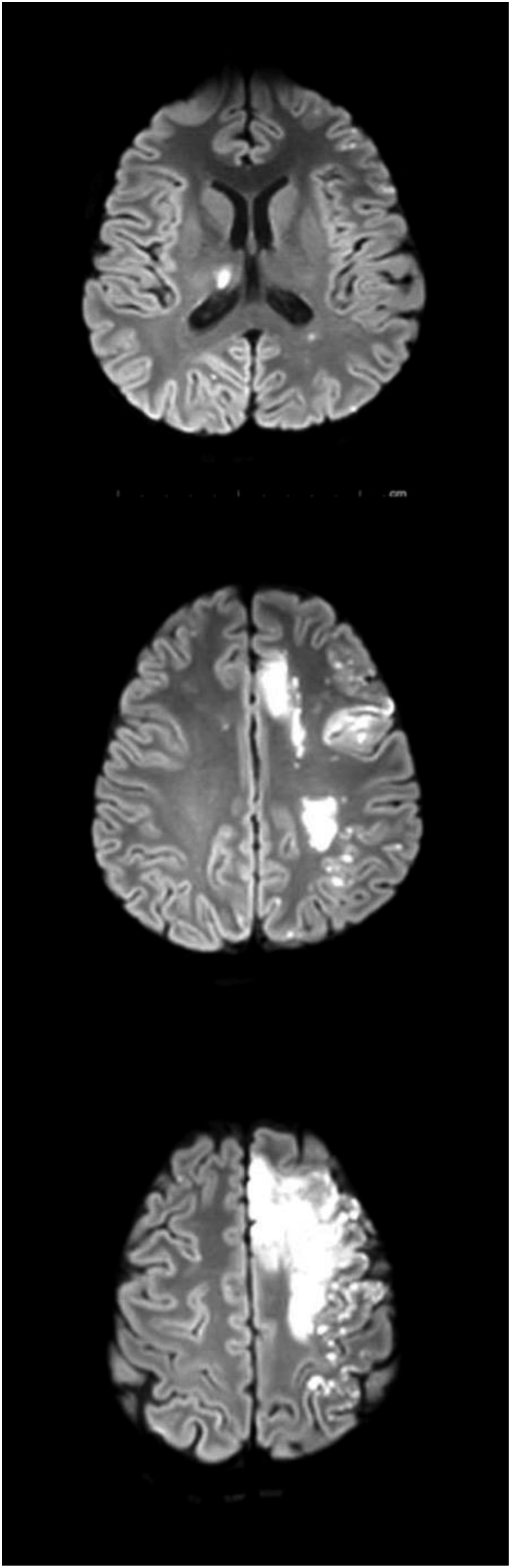
The patient was initially started on IV methylprednisolone 1 gram daily for 3 days, followed by oral prednisone 60 mg daily. Five days after the initial dose of IV methylprednisolone, our patient was given a loading dose of cyclophosphamide 500 mg/m2 with the plan for monthly maintenance infusion doses for at least 6 months. Daily aspirin was started for secondary stroke prevention.
The patient was transferred to inpatient rehab approximately 10 days after presentation. She gained back strength in her right arm and leg, measuring 4/5 on confrontational strength testing throughout her right side. Her speech including naming, repetition, and fluency greatly improved. Three weeks after her initial presentation, she was able to feed herself with her right hand and walk up and down stairs with stand-by assist. She maintained difficulty with reading and executive function.
Discussion
When assessing ischemic stroke and possible etiologies in the pediatric population, it is helpful to identify the patient's underlying risk factors as well as look at the location and focality of the patient’s stroke or strokes. Multifocal cortical infarcts raise suspicion for embolic etiology such as endocarditis and paradoxical emboli through a patent formane ovale similar to in adults. Infarcts isolated to a more distinct vascular territory raise suspicion for focal cerebral arteriopathy due to such things as infection (particularly VZV), sickle cell, Moya-moya, trauma/dissection, mitochondrial encephalopathy lactic acidosis and stroke-like episodes, and cerebral autosomal dominant arteriopathy and subcortical infarcts and leukoencephalopathy. Vasculitis including PACNS can present multifocal and involve multiple vascular territories both deep and cortical. Hypercoagulable disorders as well as autoimmune and paraneoplastic antibodies can present as both isolated infarcts and multifocal infarcts. If the MRI also has white matter hyperintensities, it is important to consider Fabry disease. Common causes of ischemic stroke in the adult population including hypertension and atrial fibrillation are less likely. In our case, a complete and thorough work-up including a left frontal brain biopsy confirmed an inflammatory etiology of stroke and lead to the diagnosis of Primary CNS angiitis.
Primary CNS angiitis, also known as Primary Cerebral Vasculitis, is a non-infectious, inflammatory disease that occurs in the central nervous system. The definition of Childhood Primary CNS angiitis (cPACNS) is based on the modified Calabrese criteria for adult PACNS: 1) Newly acquired, otherwise unexplained focal or diffuse neurologic deficits or psychiatric symptom in a patient less than 18 years of age. 2) Angiographic and/or histopathologic features of central nervous system angiitis. 3) Absence of an underlying or associated systemic disease.
3
The classification and subtypes of cPACNS are based upon the size of the cerebral vessels involved and the disease time course. The classification breaks cPACNS into small vessel, angiographic negative, large-medium-vessel, and angiography-positive. Large-medium vessel is further broken down into monophasic, nonprogressive, and progressive.3,4
The true incidence rate of cPACNS is relatively unknown. In one population cohort study with 97 childhood ischemic strokes, underlying cPACNS was identified in 24% of the cases. 5 In adult PACNS, the annual incidence rate has been reported as 2.4 cases per 1,000,000 person-years. 6
The symptoms of cPACNS vary greatly and depend on the size of the vessel affected and the area of the brain involved. Large vessel cPACNS usually presents with acute or subacute stroke and transient ischemic attack symptoms. These patients can also have headache and encephalopathy. The small vessel subtype can be more slowly progressive and present with seizure, headache, psychiatric symptoms, behavioral changes, and focal neurologic deficits. 7 When compared to Adult Primary CNS Angiitis children with cPACNS more often present with focal deficits. 3 The pathophysiology of cPACNS is an immune-mediated inflammatory process directed toward blood vessels in the CNS characterized by intramural and perivascular infiltration of immune cells resulting in edema, vessel stenosis, endothelial activation, and pro-thrombotic effects. 8 There have been studies showing increased levels of serum interleukin 6, interleukin 8, CRP, chemokines, matrix metalloproteinases, and tissue inhibitor of metalloprotease supporting the inflammatory nature of the disease.9,10
Definitive diagnosis of cPACNS is established by brain biopsy. If brain biopsy cannot be obtained the diagnosis is made by a combination of clinical symptoms, imaging including vessel imaging, CSF studies, and exclusion of other causes of CNS vasculopathy such as infection, systemic inflammatory disease, and malignancy. Imaging in medium-large vessel cPACNS can show arterial stenosis, vessel wall thickening, and contrast enhancement. In small vessel cPACNS, leptomeningeal enhancement can be seen. Although our patient had inflammatory CSF with lymphocytic pleocytosis, this is not seen in all cases. Inflammatory markers in serum and CSF are only abnormal in 30% of large-medium vessel type but more likely to be elevated in small vessel disease. 11 Treatment includes immediate steroid therapy followed by IV cyclophosphamide therapy for 6 months. After 6 months, maintenance therapy with mycophenolate mofetil/mycophenolic acid is recommended. Long-term antiplatelet therapy is also recommended. 12
In summary, this case represents an example of the large-medium vessel angiography-positive nonprogressive subtype of PACNS. It serves as a reminder that when patients in the pediatric population present with stroke-like symptoms, the differential is extremely broad and it is important to initiate a complete work-up and initiate treatment quickly.
Footnotes
Acknowledgments
The authors would like to thank the patient for allowing us to discuss her case. Written consent was obtained from a patient surrogate given her age.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.